
Abstract
Background
Enteral nutrition delivery in the critically ill is frequently interrupted for surgical and airway procedures to avoid aspiration of stomach contents. Recurrent fasting leads to under delivery of enteral nutrition and this underfeeding is associated with worse outcomes. International fasting recommendations do not provide guidance for intubated patients receiving enteral nutrition. This study aimed to gain a detailed perspective of UK critical care fasting practices.
Methods
A web-based survey was sent to 232 UK intensive care units consisting of questions relating to fasting practices, presence of guidelines, average fasting times for common procedures and dietitian time per intensive care unit bed.
Results
A total of 176 intensive care units responded. Only 20% of units had guidelines and respondents stated that they were not consistently adhered to (mean compliance 66%). Units with greater dietetic involvement were more likely to have guidelines (p = 0.04). Fasting times were shorter for abdominal surgery (p = 0.002), non-abdominal surgery (p = 0.016) and radiology (p = 0.015) if a guideline was present. Fasting for extubation and tracheostomy was similar irrespective of the presence of a guideline. Considerable variation in fasting times was reported, usually due to inconsistencies in clinical decision-making.
Conclusions
This survey of national practice demonstrates that fasting times are varied and inconsistent, which may lead to under-delivery of enteral nutrition. More dietetic input was associated with increased likelihood of a fasting guideline.
Introduction
Data from international multicentre trials1,2 demonstrate that intensive care unit (ICU) patients’ prescribed enteral nutrition (EN) targets are frequently unmet. On average, patients receive 60% of energy and protein targets as determined by predictive equations. 1 While achieving more than 80% of protein target is associated with a decrease in 60-day mortality and an increase in ventilator-free days, 2 underfeeding is associated with more infections and greater ICU and hospital stays.3,4
EN is considered the first choice of nutrition support as it is thought to maintain gut integrity, modulate the stress response, reduce mortality and infections. 5 The unpredictable nature of critical illness means that EN delivery is commonly interrupted with extended fasting times observed. 6 Frequently cited reasons include fasting for surgical and airway procedures (to avoid aspiration of stomach contents), loss of enteral access and gastrointestinal intolerance.7,8 While recommendations on fasting prior to procedures9–11 are intended for elective surgical patients eating food, they do not provide guidance for fasting of intubated patients receiving EN. This may be due to a dearth of research on fasting times for stopping EN in this patient population. Evidence suggests that ICU-specific guidelines increased the delivery of EN targets from 65% to 84%, 12 while extended fasting times is challenged by recent trials which suggest reducing fasting times before procedures resulted in significantly more EN delivered and with no increase in complications.13–16
Few data are available describing current practice or to guide fasting practice in ICU patients. Schneider et al. 17 surveyed anaesthesia and ICU departmental chiefs to determine current fasting practices across the United States. Based on a 26.9% response rate, the investigators found significant differences in the length of time EN was withheld before scheduled procedures such as extubation and tracheostomy. Fasting times differed for various procedures within units as well as between units, in that anaesthesia ICUs recommended 4 h for extubation and 6 h for tracheostomy, compared to 2 h for extubation and 4 h for tracheostomy in surgical ICUs. Given the low response rate, it is unclear if the results are representative of ICUs in the United States. Currently, no data are available on practice in the UK.
The primary aim of this survey was to gain a detailed perspective of fasting practices in UK ICUs. The objectives were to:
Describe national trends in ICU fasting prior to procedures. Identify the development and uptake of fasting guidelines in ICUs across the UK. Test for associations between fasting times before an intervention and the presence of a guideline. Determine whether direct dietitian involvement in patient care was associated with the presence of guidelines. Ascertain if there is an association between the presence of a guideline and allowing enteral clear fluids and enteral medications during fasting periods. To identify whether volume-based or catch up feeding was undertaken after EN interruptions.
Methods
The study was considered a service improvement project by the research and development (R&D) service at Imperial College Healthcare NHS Trust and therefore ethical approval and R&D registration was not required. The survey was performed using a web-based provider (www.Surveymonkey.co.uk). To optimise content validity, the questionnaire was piloted by a group of 10 ICU dietitians and re-piloted once amendments were made prior to the survey launch. The survey was distributed in June 2016 to all UK ICUs via the British Dietetic Association critical care specialist group (BDA CCSG) and by email to non-member ICU dietitians. ICU dietitians were selected as respondents on the basis that in UK ICUs their role is well developed, 18 and these clinicians are closely involved in nutrition delivery and guideline development. As such, they represent the most reliable source of knowledge of actual practice.
Where no dietitian was identified, dietetic departments were telephoned to determine who was best placed to complete the survey. To maximise response rate, follow-up emails and telephone calls were made to non-responders between June and August 2016. Respondents were asked to complete one survey per hospital unless there was more than one ICU within a hospital and fasting practice varied between the different units, in which case one questionnaire was requested for each unit.
The questionnaire consisted of questions relating to local ICU fasting practices, including whether units had fasting guidelines and the average fasting times for a range of common procedures including extubation, tracheostomy insertion, diagnostic and surgical procedures. Respondents were asked to report whether the guidelines were routinely followed. Questions about factors influencing fasting, the use of catch up feeding, the influence of gastric residual volumes (GRVs) on fasting practices, and whether enteral clear fluids and enteral medications were allowed during fasting periods were included. Information was also collected on the whole time equivalent (WTE) of a dietitian per ICU bed. A copy of the survey can be found in the online supplementary appendix.
Volume or catch up feeding was defined as units that have a protocol for nursing staff to adjust the hourly infusion rate of EN after interruptions. This allows provision of a greater volume of EN, aiming to make up and achieve the 24-h volume target. 19
Dietitians who were unfamiliar with practice on their unit were asked to discuss fasting practices with their ICU team prior to completion of the survey. To inform the results, flexibility was built into the questionnaire to allow additional comments explaining variations in practice to be entered. Where fasting practices varied within units, respondents were asked to enter the most common fasting time and then add comments to explain the reasons for variation.
Qualitative analysis, guided by the research methods of Miles and Huberman, 20 was undertaken by two authors to assess any common themes within the free text comments. The comments were transcribed and explored using an inductive approach, where comments were split into three sections; those with guidelines, those without and any other comments. Data familiarization was undertaken where initial ideas, words and phrases were used to identify themes. The authors met to share work and to develop the final coding framework comprising 10 themes, which was further refined to provide 4 themes. There were no discrepancies between the two authors, and all authors confirmed agreement with the themes.
Data are presented as mean and standard deviation, median and interquartile ranges or counts and proportions. Where appropriate, data were tabulated to describe its distribution. To describe the data and answer the specified study questions, we tested for associations and trends between the presence of a fasting guideline (binary variable) and the various treatment interventions (categorical variables). Due to the low frequencies within some cells (less than five), a Fisher’s exact test was used to test for association between the type of intervention and the presence of a guideline. When the frequency of responses in most cells across categorical variables exceeded five, a Chi-squared test was used to test for associations between variables and trends. Data on work force availability were dichotomized using the minimum recommended guideline for amount of staffing per beds of 0.05 WTE per ICU bed. Logistic regression was used to test for an association between the presence of a guideline and the binary WTE variable. In all instances, statistical significance was defined at the 5% level. The analysis was performed using STATA MP 13.1 (STATA Corp., College Station, Texas, USA).
Results
A total of 167 ICU dietitians from 232 UK ICUs responded, representing 72% of all UK ICUs and 76% of ICUs with dietetic input. Among all responders, 111 (68%) were members of the BDA CCSG. Fourteen dietetic departments in UK hospitals with ICUs reported that they did not provide a service to the ICU.
The presence of fasting guidelines was reported by 20% (34 of 167), while 78% (131 of 167) of the respondents had no guideline and another 1.8% (2 of 167) was unsure. As both ‘don’t knows’ provided data for the without guideline questions, their responses were included in the ‘without guideline’ group. All 167 respondents provided responses regarding the presence or absence of a guideline; however, four responders did not fully complete the questions regarding fasting times for each procedure. As they contributed to other parts of the survey, their partially completed survey responses were included in the analysis.
Whole time equivalent of dietitian per ICU bed and likelihood of guidelines
Responses regarding the dietetic provision to the ICU were provided by 143 (86%); 24 respondents did not provide these data. We were unable to follow them up, as they did not leave contact details. The mean (SD) WTE per ICU bed was 0.04 (0.02), with a range from 0.01 to 0.11. The odds ratio (95% confidence interval) for having a guideline, based on UK WTE recommendation of ≥0.05 WTE per bed, was 2.4 (1.1–5.6; p = 0.04).
Comparisons between those with and without guidelines
Comparison of fasting times for those with and without fasting guidelines.
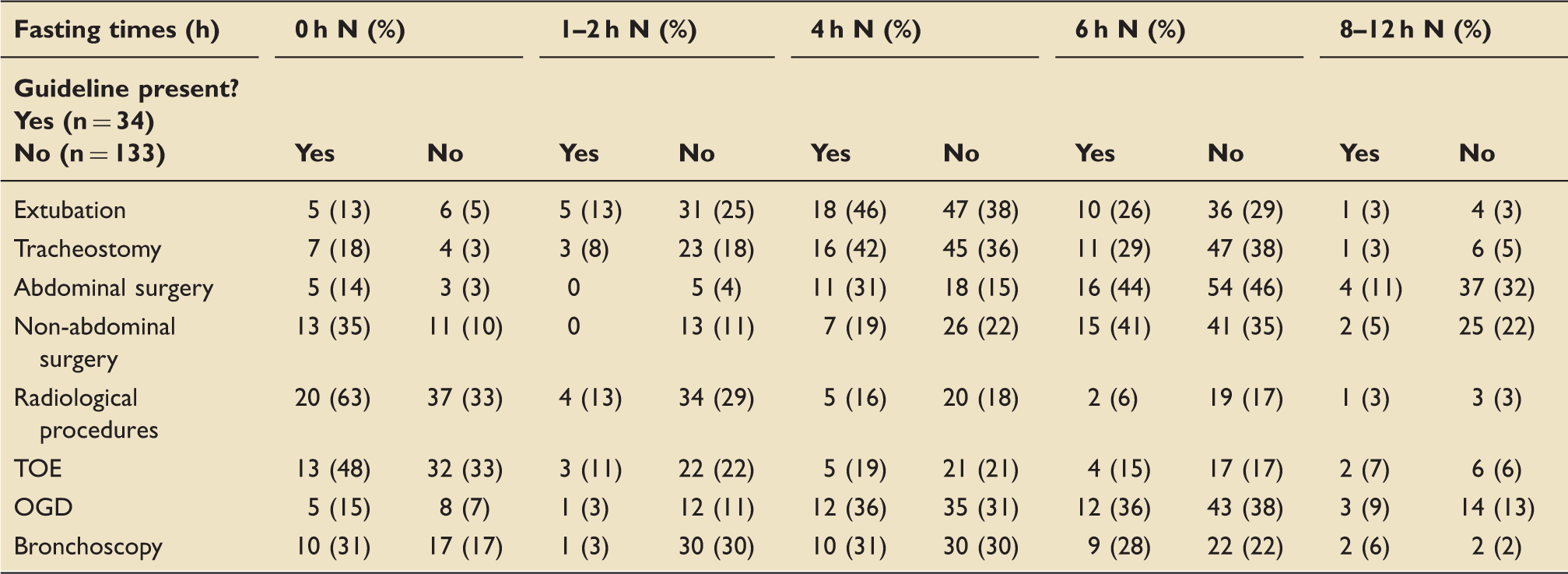
Bronchoscopy: rigid bronchoscopy; OGD: Oesophago-gastroduodenoscopy; TOE: Transoesophageal echocardiography.
For those procedures where a significant association was found between duration of fasting and the presence or absence of a fasting guideline, we tested for trend. A significant trend was found for abdominal surgery (p = 0.002), non-abdominal surgery (p = 0.016) and radiology (p = 0.015). Before abdominal surgery, most patients were fasted for 6 h or less (87%) in the presence of a guideline compared to most being fasted 6 h or more (79%) without a guideline. A similar pattern was observed for non-abdominal surgery where 82% were fasted up to 6 h if there was a guideline compared to just over half (58%) for 6 h or more. Finally, for radiological procedures, 72% of patients in the guidelines group were fasted for less than 1 h, compared to 80% being fasted for up to 4 h in the non-guideline group. Fasting prior to extubation was predominately for 4 to 6 h irrespective of whether the ICU had a guideline or not, 72% in the guideline group versus 67% without. A similar trend was observed with tracheostomy with 71% of fasting being within 4 to 6 h with a guideline versus 74% without. As guidelines for fasting of EN in critically ill patients do not exist, we can compare our findings to national guidelines for preoperative orally fed patients. 11 The number of units that stated following recommendation of 6 h was similar between those with guidelines and not and consistent for all procedures (Table 1). For example, for extubation, this was 26% with and 29% without guidelines, and for non-abdominal surgery, it was 41% with and 35% without.
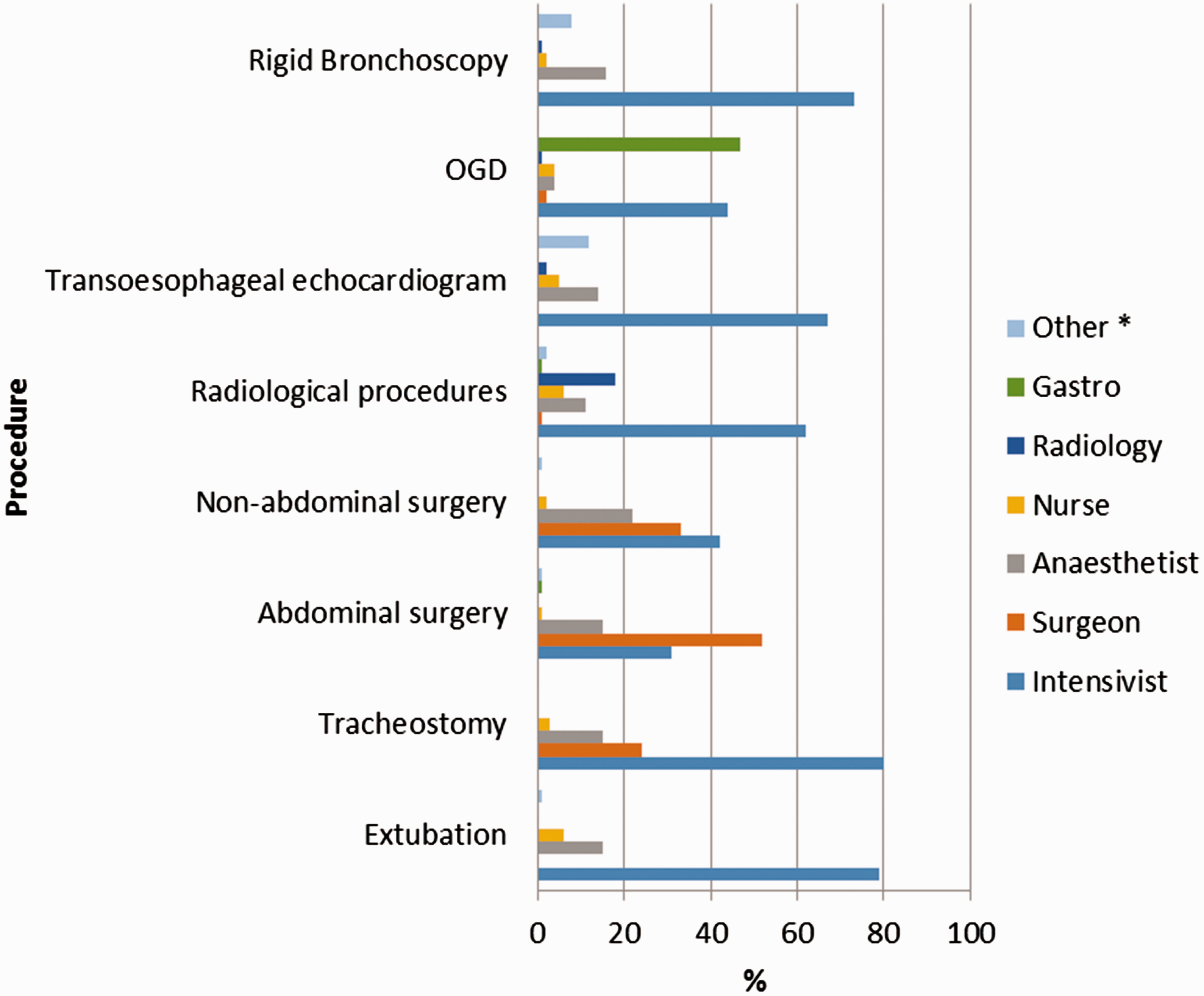
Despite having fasting guidelines, respondents reported that these were not always adhered to (Figure 1). The reported mean compliance for all procedures was 66%, and the noncompliance was reported for every procedure. Fasting for non-abdominal procedures had the lowest reported compliance, where set times were only followed 55% of the time. Where guidelines were not present, the intensivists (Figure 2) made most fasting decisions, for example, 79% of extubation and 80% of tracheostomy fasting decisions. Surgeons were most likely to set fasting times before abdominal surgery (52%), and gastroenterologists most likely to advise on fasting prior to OGD (47%).
Adherence to fasting guidelines. Surgery: non-abdominal surgery; Radiology: radiological procedures; TOE: Transoesophageal echocardiogram; OGD: Oesophago-gastroduodenoscopy. Decision makers in the absence of a guideline. Others: cardiology, respiratory, cardiothoracic.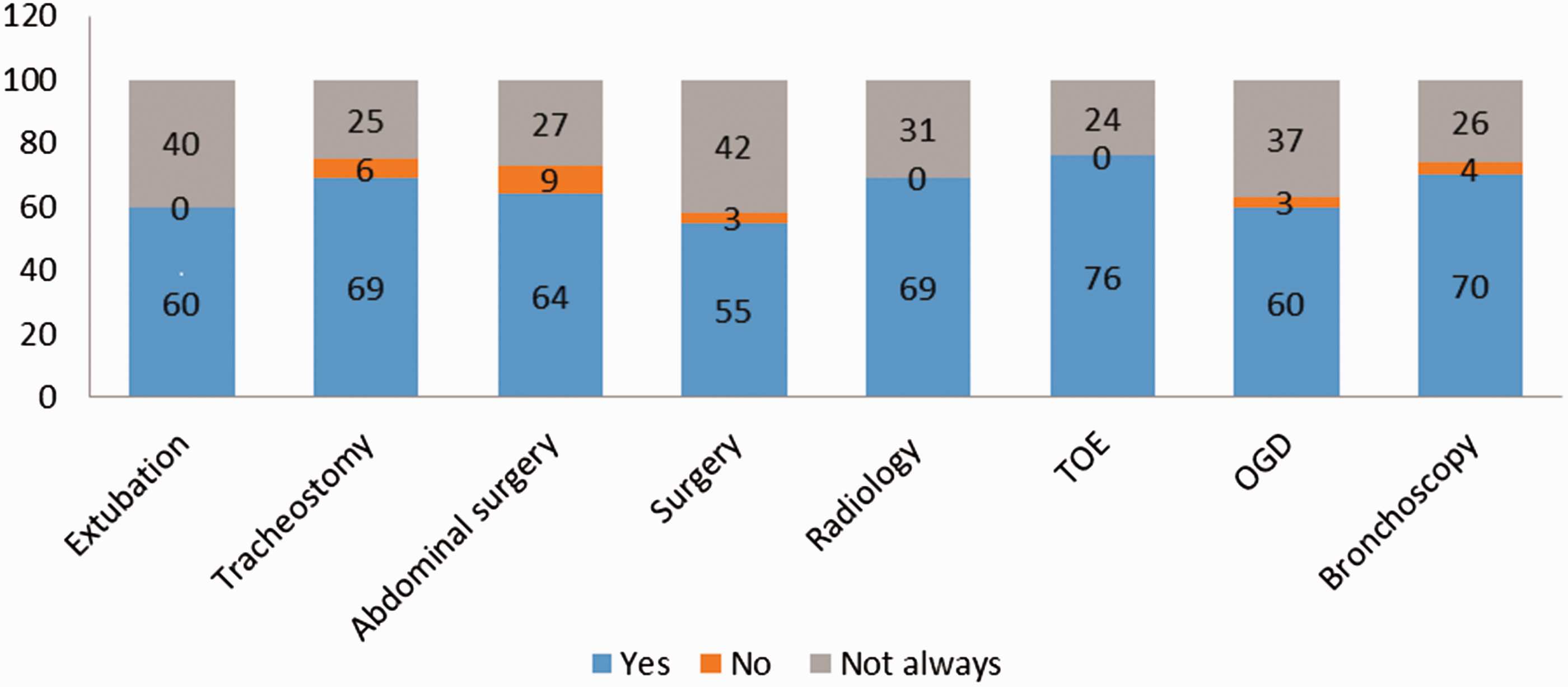
Factors influencing fasting
Participants were asked to state the maximum GRVs their unit used as a measure of gastric emptying. The size of GRV varied between units ranging from 200 to 500 ml. The most commonly reported volume was 400 ml, observed in 27%. When asked if the patients’ gastric emptying over the last 24 h influenced fasting practices, only 22 units (13%) affirmed, indicating that they would fast a patient with high GRVs for longer. There was no significant difference between those with and without a guideline in terms of allowing enteral clear fluids and enteral medications during fasting periods. Enteral clear fluids were not regularly given during fasting (30%), whereas enteral medications were given in 68% of units. Most units (over 80%) did not undertake catch up or volume-based feeding. If it was performed, it was more likely to occur following non-abdominal surgery (19%) and tracheostomy (19%) and least likely to occur after abdominal surgery (11%). There was no significant difference in whether catch up feeding was undertaken between those with and without a guideline.
Qualitative analysis of respondent’s comments
Coding framework for qualitative analysis and responses.
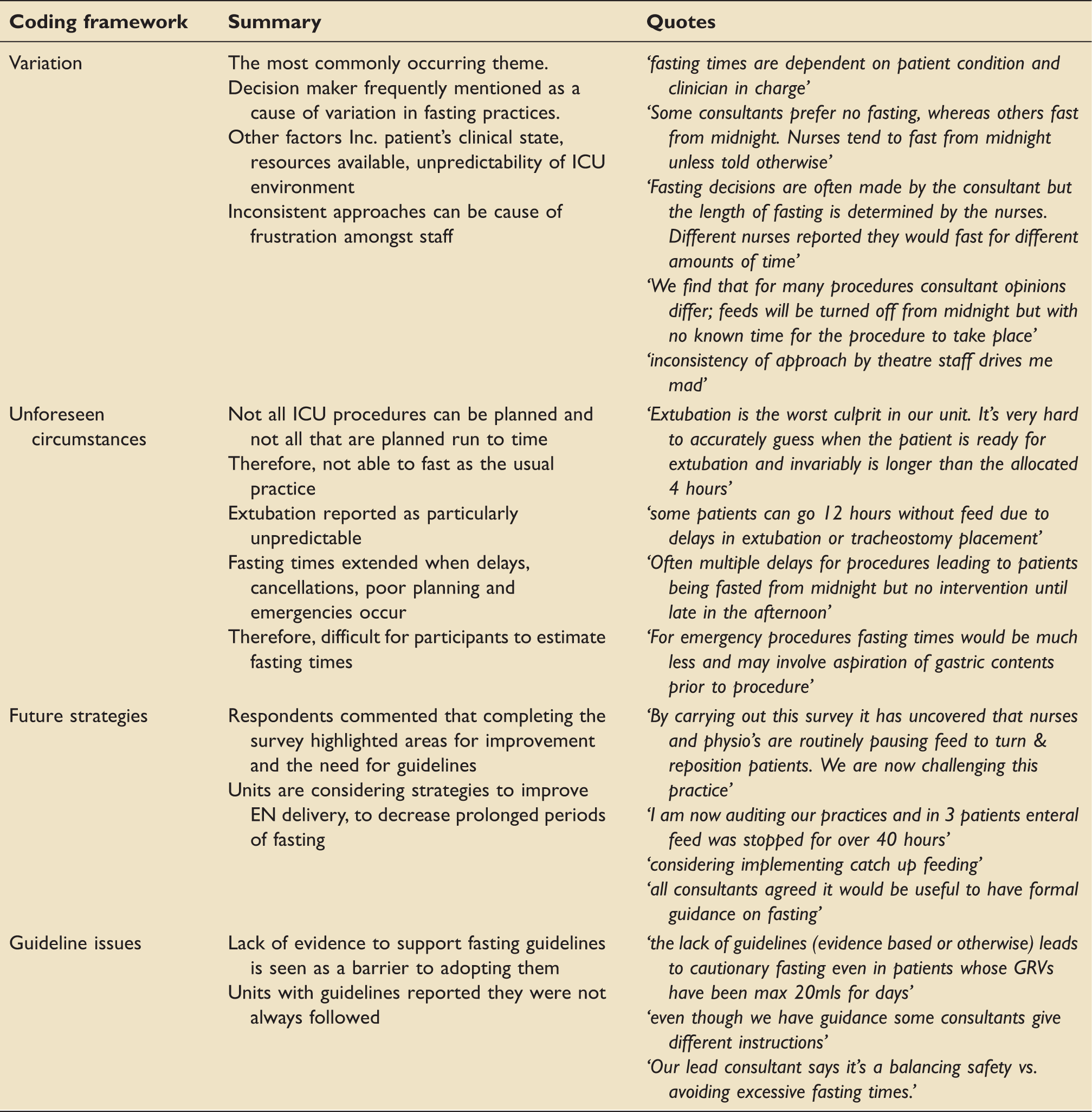
Variation was the most commonly occurring theme with decision makers frequently reported as the reason. This inconsistent approach caused frustration amongst staff. The patient’s clinical state, resources available and unpredictability of ICU environment were also described as causes.
Unforeseen circumstances were reported since unplanned procedures frequently occurred and planned procedures did not always run to time. Extubation was commonly stated as being particularly unpredictable and consequently the usual fasting practice was not always possible.
Future strategies were planned by respondents following completion of the survey. Teams had highlighted areas for improvement and the need for specific fasting guidelines. Units reported considering future strategies to help improve EN delivery and to decrease unnecessary long periods of fasting.
Guideline issues were observed in the units that had their own fasting guidelines, for example, problems with non-compliance and barriers to adoption.
Discussion
We report the most detailed description of fasting practices in adult UK ICUs to date. One of the strengths of this survey is its combination of quantitative data and descriptive responses, which enhance the results providing useful insights in to real fasting practices. Respondents described that fasting times are highly varied for a number of different scheduled procedures as also reported by Schneider et al. 17 However, the low response rate in the American study means the results are highly prone to selection bias. Conversely, our survey, which was completed by 72% of all UK ICUs, has low bias and is representative of UK practice. The high response rate observed is likely a result of the robust methods used, which included the questionnaire being emailed to a named person, easy online access and follow-up emails and telephone calls made. However, Schneider et al. used a paper-based questionnaire that was sent out which required respondents to return via mail and no follow-up undertaken.
Dietetic workforce
The mean dietetic staffing level was below the national recommendations for 0.05–0.10 WTE per bed. 18 The results suggest that the greater the involvement of the dietitian (equal to or greater than 0.05 WTE) on the ICU, the more influence they may have on the presence of a guideline.
Differences between guideline and no guideline
Reported fasting times were shorter for abdominal surgery, non-abdominal surgery and radiological procedures if a guideline was present. Two of the most frequently stated reasons for fasting, namely extubation and tracheostomy, 12 saw no differences in fasting times between the guidelines group and non-guidelines. It is possible that these procedures are perceived as higher risk for aspiration and therefore intensivists are more reluctant to decrease fasting times, preferring to stick to the national recommendation of 6 h. 11 In contrast procedures that do not involve manipulation of the airway, in an already intubated patient, such as surgery and radiological procedures may be viewed as lower risk and therefore clinicians are more likely to allow a shorter fast. Also the longer fasting times seen both with and without a guideline for airway management could be attributed to the nature of these procedures in that they are comparatively less predictable and are not given the same allocated timeslots as surgical and radiological procedures more frequently are. This could result in airway management procedures being more difficult to set specified fasting times for, making them more susceptible to variation in fasting practices as highlighted in Table 2.
Factors influencing fasting
Considerable variation in fasting practices was described in those units without fasting guidelines. Respondents reported that individual ICU consultants were requesting that patients were fasted based on individual opinion and clinical experience. Comments provided describe ICU fasting advice conflicting with recommendations from theatre staff, causing frustration among ICU staff. Responders from units with guidelines stated that emergencies and unplanned procedures took place, causing delays, extending fasting times and contributing to nutritional deficits. Due to the lack of evidence and guidelines, there was considerable interest expressed in developing some degree of national standardisation.
Although recent guidelines question the appropriateness of GRVs as a measure of gastric emptying, 5 99% of units still use it. Only 13% of units consider GRVs when deciding on fasting times. Some described it not making a difference as the nasogastric tube is routinely aspirated prior to the procedure, while others had not considered it before. The majority of units continue with enteral medications during fasting but do not allow enteral clear fluids despite guidelines advocating clear fluids up until 2 h before anaesthesia. 11 Catch up feeding was uncommon despite being advocated for improving EN delivery.5,19,21 Many described wanting to implement it.
Three aspects require further work. First, we need to understand reasons for variation in fasting decision making, including whether the presence of guidelines reduces variation. Second, there is a need to develop expert consensus statements on fasting for ICUs to guide clinical practice. This could focus on creating a pragmatic approach considering the risks and benefits of continuing EN right up until procedures commence. Third, more research is needed to ascertain if different procedures and patient conditions necessitate different fasting times.
Limitations
There are limitations of this study. First, although the overall response rate of 72% is high, the fasting practices for 28% of units are unaccounted for. This may limit the generalisability of our results despite the relatively low risk of reporting bias. Second, we asked respondents to state and comment on compliance of guidelines rather than measuring it. This can open up the results to reporter bias. In ICUs where dietitians were not so familiar with unit fasting practices, and those units with no guidelines, the dietitian completing the survey discussed fasting practices with their intensivists and lead nurses. These respondents reported average figures, because standardised fasting approaches were not used on these units and therefore these represent an estimate.
Conclusions
In this comprehensive survey of national practice, we demonstrate that fasting times are varied and inconsistent, often leading to reported frustration for staff and long fasting times for patients, which may lead to under-delivery of EN. Where guidelines were present, fasting was significantly shorter for surgery and radiological procedures. However, for airway procedures such as extubation and tracheostomy, fasting times were similar between all units irrespective of the presence of a guideline. More dietetic input was associated with increased likelihood of the unit having a fasting guideline.
Footnotes
Authors contributions
ES conceived and designed the study. MT informed the study design, performed the statistical analysis and interpretation, provided supervision and critically revised the manuscript for publication. ES, CP, RJ, WB, TL, BJ, EON and SH conducted the study, undertook data acquisition and prepared the manuscript. RJ and WB performed the qualitative analysis. All authors read and approved the final manuscript.
Acknowledgments
The authors would like to thank all the UK critical care dietitians and their teams who completed the survey and participated in the study.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: ES has received honoraria for lectures and reimbursement of travel expenses from Fresenius Kabi and Baxter. BJ has received sponsorship from Nestle to support conference attendance. CP has received honoraria for lectures from Fresenius Kabi. EON received sponsorship from Nestle and Fresenius Kabi to support conference attendance. WB has received sponsorship from BBraun to support conference attendance.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study was considered a service improvement project and therefore ethical approval was not required nor approval by the local research and development service at Imperial College Healthcare NHS Trust.
Patient consent
No consent was required, as this study did not include patients. By completing the survey, participants agreed to take place and for their responses to be used.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.