
Abstract
Background
Enteral nutrition is currently the route of choice for feeding critically ill patients with a functioning gut but delivery is commonly associated with disruptions. Common reasons for interruptions to enteral nutrition are fasting for diagnostic procedures, surgery and airway management. These interruptions result in significant calorie deficits that are associated with increased complications. We aimed to describe the specific interruptions in our patient group and the impact they have on nutrition delivery before and after implementation of a fasting guideline.
Methods
A service improvement project was undertaken over two different time points, 1 year apart, to evaluate the effectiveness of a fasting guideline in a general/trauma ICU in a London teaching hospital.
Results
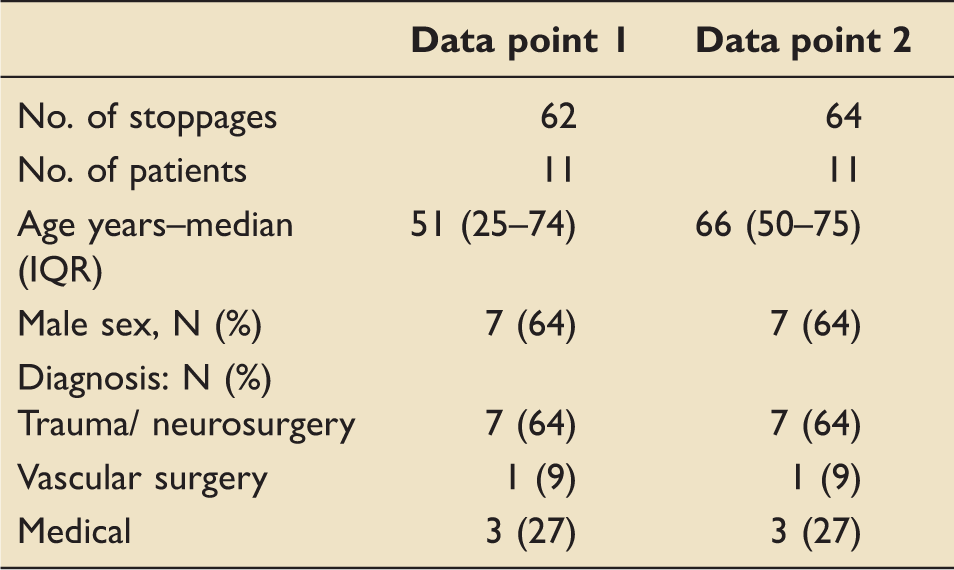
There were 62 interruptions to enteral nutrition delivery with the first data collection and 64 in the second. Prolonged fasting before and after surgery and airway procedures were initially identified as the two most important causes of delays. Implementation of the fasting guideline resulted in statistical and clinical improvements in reducing fasting for airways procedures. The calorie deficit also statistically and clinically decreased as a result of the guideline.
Conclusions
We conclude that the introduction of a simple guideline stipulating reduced fasting times before ICU procedures can result in less time lost in feed interruptions and improved enteral nutrition delivery.
Introduction
Enteral nutrition (EN) is currently the route of choice for feeding critically ill patients with a functioning gut1,2; however, due to the unpredictable nature of critical illness, the delivery of EN is frequently disrupted. In practice, it is rare for all the prescribed daily EN to be delivered. A large international multicentre study found that the critically ill patients were uniformly underfed calories, with an average of 59% of energy prescription being received. 3 This was also illustrated in the large English-based CALORIES trial, where target calories were not achieved for either EN or parenteral nutrition (PN) with EN delivering 62% and PN 73% of target. 4 Common reasons for the inadequate EN delivery are gastrointestinal intolerance, fasting for diagnostic procedures, surgery and airway management. 5 These interruptions to EN result in significant daily and cumulative calorie deficits, thus contributing to underfeeding and malnutrition. 3 Underfed patients have an increased risk of all-cause mortality, bloodstream infections and longer ICU and hospital stays.6–8
To reduce the risk of aspiration of gastric contents on induction of anaesthesia, the current practice is to withhold EN for 6 h before ICU procedures as per the UK and European guidance. 9 These recommendations, however, are intended for healthy elective surgical patients eating solid food and make no reference to fasting in critically ill intubated patients being enterally fed. MEDLINE, CINAHL and EMBASE databases were searched and demonstrated that there is a lack of research on gastric emptying times for EN in intubated critically ill patients, and as a consequence, there is no recognised guidance on the length of time that should elapse between stopping EN and commencing anaesthetic procedures. We therefore developed and implemented our own fasting guidelines in an attempt to address the specific interruptions to EN on our unit.
This project first aimed to determine the reasons for and durations of EN interruptions and the impact of these on nutrition delivery. The second aim was to examine the effect of introducing ICU-specific fasting guidelines on the frequency of EN interruptions and nutrition delivery.
Methods
This service improvement project collected data at two different time points, one before and the other after the development of a fasting guideline in a general/trauma ICU in a London teaching hospital. The unit takes approximately 700 admissions a year, with 30–50% of admissions being trauma. There are eight intensive care medicine consultants, 100 nursing staff (50% band 5, 38% band 6, 10% band 7 and 2% band 8) and full-time critical care specialist dietitian, pharmacist and physiotherapists. The inclusion criteria were older than 18 years, receiving EN, experienced an interruption to EN over the duration of the data collection period. Data were collected at the bedside and from electronic patient records over a 4-week period and repeated 1 year later after the creation, implementation and adoption of guidelines. Data were collected on the reason for stopping EN, length of time EN was stopped prior to the procedure, length of procedure, the time it took post procedure for EN to be restarted and any reasons for delay in restarting EN. Nutritional data were collected daily for the project periods. Calorie requirements were calculated using the validated Penn State equations.10,11 Nutritional intake data were collected on the calorie target per day, the calories received per day, the cumulative calorie deficit (total calories prescribed for the project period minus the amount delivered) and percentage of energy target delivered over the 4-week period. Fasting times are presented as time before and after procedure. We observed for incidents of major pulmonary aspiration at the time of the procedures, surgery and airway management. Descriptive statistics are presented as median and inter-quartile range. Mann–Whitney U test was used to detect significant differences between variables.
The aim was to provide standardised guidelines to optimise nutrition support, minimising fasting times, whilst also maintaining patient safety. The guidelines were applicable to all ICU patients receiving EN with a protected airway, defined as a cuffed endotracheal or tracheostomy tube (Appendix 1). Before non-airway surgery (e.g. plastic surgery, orthopaedics and neurosurgery) or transfers for imaging, the EN was continued until the patient left the ICU. The nasogastric tube (NGT) was then aspirated and gastric contents discarded. EN was stopped 4 h before airway procedures (tracheostomy, airway change, extubation). After tracheostomy, the EN was restarted once the NGT tube position has been confirmed at the last hourly rate. After theatre (non-abdominal surgery) and off-unit scans with a protected airway, the EN was restarted immediately on return from theatre, at the last hourly rate, as long as there were no concerns over tube movement. After extubation, if after 4 h, the patient was stable, then EN was restarted at the same rate.
The guideline took 6 months to develop and get officially agreed by all stakeholders. Once ready for launch, the ICU dietitian provided focused education to all nursing and medical staff on the new guidelines, and this was re-enforced on the daily ward rounds. The guidelines were endorsed by all of the ICU consultants and actively promoted. Communication was also provided to all ICU staff from the lead ICU Clinician. This outlined the importance the unit placed on provision of optimal nutrition and stipulation that the guidelines must be followed irrespective of requests made by other teams and that the suggested AICU fasting times must be complied with. The anaesthetic department were also consulted with and provided ratification. The team of nurse educators were on the unit daily working with junior nursing staff and key in ensuring the guidelines were followed. The combination of approaches resulted in a good uptake of the guidelines. Six months was allocated as sufficient time for the guidelines to be implemented and adopted into the unit practice before repeating the data collection. There were no other protocol changes for other ICU treatments that could impact on fasting times or the uptake of the guideline.
Results
Demographics.
Average cessation times.
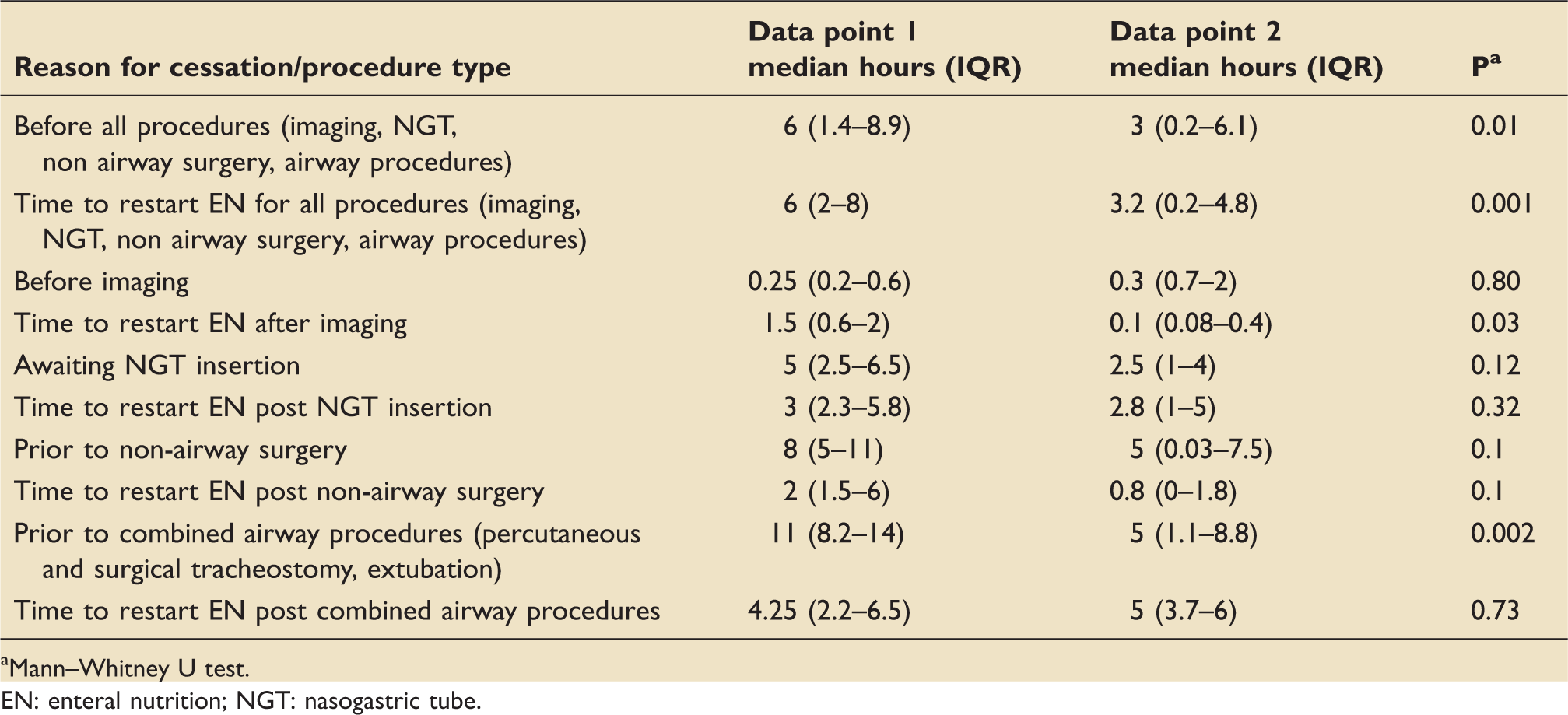
Mann–Whitney U test.
EN: enteral nutrition; NGT: nasogastric tube.
Nutritional data.
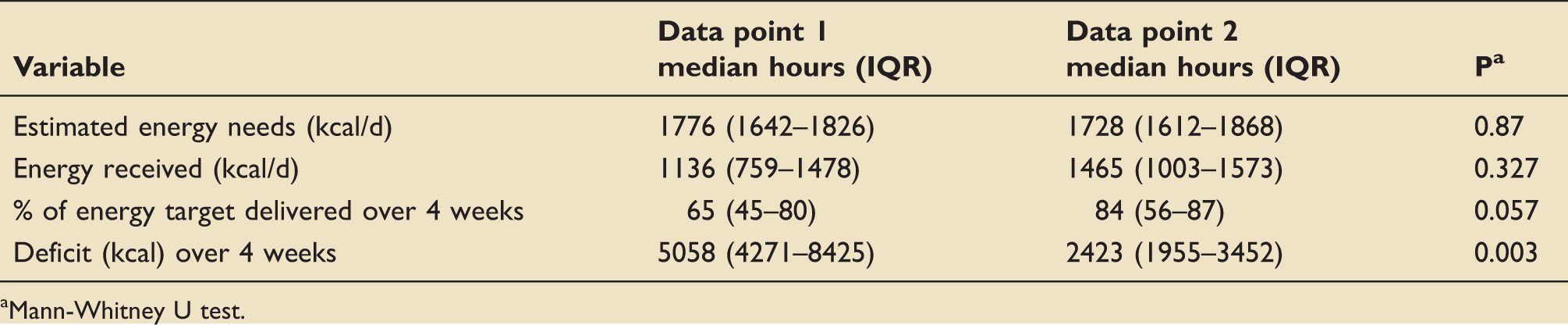
Mann-Whitney U test.
Despite some reservations and concerns over the risk of aspiration of gastric contents with the new reduced fasting guidelines, no incidents of major pulmonary aspiration were observed.
Discussion
There is currently no consensus on the appropriate length of fasting time enterally fed patients should undergo prior to ICU procedures, i.e. theatre, tracheostomy insertion and extubation. Set fasting times vary from unit to unit and are usually between 4 and 8 h. 12 As there are no data available to guide our practice, we have tried to reach a sensible balance between practices used on other units, limited literature in the area, the risks associated with underfeeding and risk of pulmonary aspiration. The evidence to support the 6h fast originates from avoiding the major risk of asphyxiation from solid food matter.9 We reached a pragmatic decision for patients with a protected airways based on the premise that liquid enteral feed does not pose the same asphyxiation risk, plus the presence of an NGT that can be used for aspiration of any remaining gastric contents.
This was agreed both in the departments of anaesthesia and intensive care medicine.
In this service improvement project, we have shown on our unit that although EN is routinely stopped in excess of the UK recommended 6 h in critically ill patients prior to surgical and airway procedures, we were able to successfully develop and implement a reduced-hours fasting guideline. In our case, the practice of reducing the fasting times was not associated with any major pulmonary aspiration. We are adding to the limited body of knowledge available and also supporting a reduction in fasting times.
We were effective at reducing the time EN was discontinued before airway procedures and non-airway surgery although it was not possible to eliminate total fasting for the non-airway surgery as intended. This was indeed the most controversial aspect of the new guidance despite agreement from the ICU consultant team and anaesthetic department. Fasting practices are based on existing deep-rooted traditional practices, making changing practice difficult. The overriding aim of any reduced fasting guidance is to improve nutritional delivery to critically ill patients; we were able to successfully demonstrate this. Patients who experienced frequent EN interruptions have been shown to be at significant higher risk of prolonged ICU and hospital stay compared to those who did not experience interruptions to feeding. 13 The safety and effectiveness of reduced hours fasting guidance has been demonstrated in critically ill patients who have a protected airway.14–16 In a study by Pousman et al., 15 trauma patients were randomised to undergo either an 8-h fast or to follow the new guidelines of 45 min for selected operative procedures. No differences were seen between the groups in terms of vomiting or pneumonia, with a trend towards improving nutrition delivery. Interestingly, in 36% of patients in the reduced fasting group, the protocol was not followed, and they were inadvertently fasted prior to procedures. Ho and Culhane 14 implemented a fasting protocol for PEG insertions on the ICU. EN was given up until the time of procedure, and results were compared with a historical cohort who fasted for 8 h. The reduced fast patients received more calories that day, compared with those who fasted for 8 h. No peri-procedural vomiting or aspiration was observed. Jenkins et al. 16 took the fasting concept one step further by actually feeding during the surgical procedure in burns patients. This practice was not only successful at maximising nutritional intake, thus reducing wound infections, but also safe with no negative impact on the incidence of aspiration.
The limitations of our service improvement project need to be considered. No sample size calculation was performed. Data were collected over two set defined time points; therefore, the numbers are small. We also did not investigate whether the improvement in fasting times and nutrition delivery was also associated with an improvement in clinical outcomes such as length of stay and organ support. We did not assess for cases of micro-aspiration as a consequence of the reduced hours guideline. Several markers have been used to diagnose micro aspiration including technetium 99 m, blue dye, bile acids, pepsin and alpha amylase; 17 however, there are limitations on many that preclude their routine use for clinical practice and not indicated in a service review such as this. As a follow up to this study, we would like to determine if having a ‘protected airway’ with an ETT or tracheostomy does protect against micro aspiration of gastric contents with our reduced hours fasting guidelines.
Conclusions
The project identified excessive fasting times before and after ICU procedures, particularly airway procedures and surgery. ICU-specific guidelines were introduced, advising on no cessation prior to non-airway surgery and scans and fasting for 4 h for airway procedures (tracheostomy insertion, extubation). The safety of the changes was not measured scientifically. No incidents of major pulmonary aspiration were recorded during the data collection period. The introduction of clinical guidance both statistically and clinically improved delivery of nutrition for our patients. This practice may be safe, although we do not report improvements in clinically meaningful outcomes.
Footnotes
Disclaimer
This study was presented as an abstract by Ian Barker at the ESICM in 2014. This service evaluation was assessed and approved by the Imperial College Healthcare NHS trust ICU research and audit group.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Appendix 1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.