
Abstract
Patients with critical illness have disrupted circadian rhythms, which can lead to increased morbidity, mortality and length of intensive care unit stay. Light intensity within the intensive care unit influences the circadian rhythm and may therefore impact on patient outcome. We performed an observational single-centre pilot study monitoring nocturnal light exposure of intensive care unit patients between November and December 2016. As there are currently no medical guidance on recommended light levels, we audited our findings against building regulation standards. The median light intensity was 1.5 lux, which is below the 20 lux standards; however, there were significant outliers. There was positive correlation between patient illness severity based on SOFA score and maximum lux (R = 0.45, P = 0.026); however, there was no relationship between patient illness severity and median lux exposure (R = 0.23, P = 0.28). As illness severity increased so did the time spent greater than 20 lux (R = 0.59, P = 0.0021), and the individual occasions where lux breached the 20 lux limit (R = 0.52, P = 0.009). There was no relationship between illness severity of neighbouring patients and maximum lux (R = −0.11, P = 0.69) or neighbouring illness severity and median lux (R = −0.04, P = 0.87). This preliminary work will form the basis of future projects, including national guidance and evaluating the impact of environmental light on patient-centred outcomes.
Introduction
The focus of this pilot study is to quantify the nocturnal light intensity patients are exposed to in intensive care unit (ICU) with the aim of improving the clinical environment through improved awareness and guidelines. The circadian rhythm is the 24 h, autonomous “body clock” which is primarily responsible for sleep regulation but also has effects on body temperature, hormonal homeostasis, cell regeneration and glucose metabolism. 1 Light plays a major role in the control of the circadian rhythm.2–5 Light passes through the retina and is collected via intrinsically photosensitive retinal ganglion cells (ipRGCs) which use the photopigment melanopsin to absorb light.2–5 The ipRGCs are independent of the image-forming rods and cones. Information is then transmitted via the retinohypothalamic tract to the suprachiasmatic nucleus of the anterior hypothalamus.2–5 The suprachiasmatic nucleus then controls the amount of melatonin produced by the pineal gland via entraining or supressing melatonin release.2–5 Light thus has a major influence on the circadian rhythm with low levels of artificial light exposure for as little as 20 min proven to suppress melatonin production.6–9
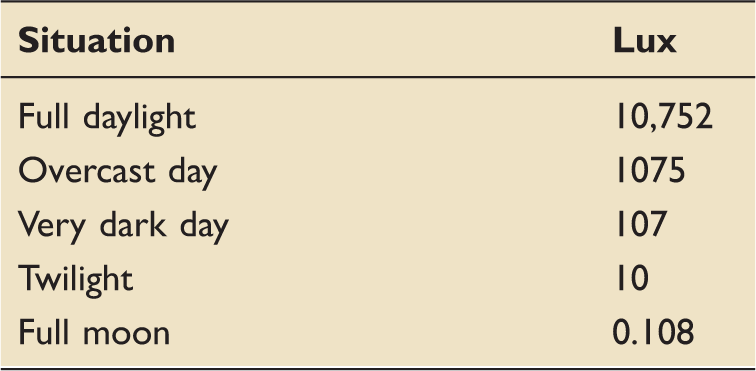
Naturally occurring lux values for comparison. 18
Methodology
In this single-centre prospective observational study, a digital luxometer (accuracy ±4% 0–10,000 Lx) Appendix 1)) recorded light levels at night in pre-determined bed spaces on ICU between November and December 2016. Permission to carry out the study was gained locally with the Portsmouth Hospitals NHS Trust R&D department and registered as an audit. Portsmouth ICU is a modern, 24-bedded general ICU in England, which admits around 1400 level 2/3 patients per year (Figure 1). The unit has been designed with maximal natural light in mind and has large floor to ceiling windows throughout, as well as ceiling lighting and desktop computers at each bed space. There are no local guidelines currently in place around light; however, nursing staff habitually decrease artificial lighting between 23:00 and 07:00.
Configuration of bed spaces on Portsmouth ICU with selected beds indicated with cross.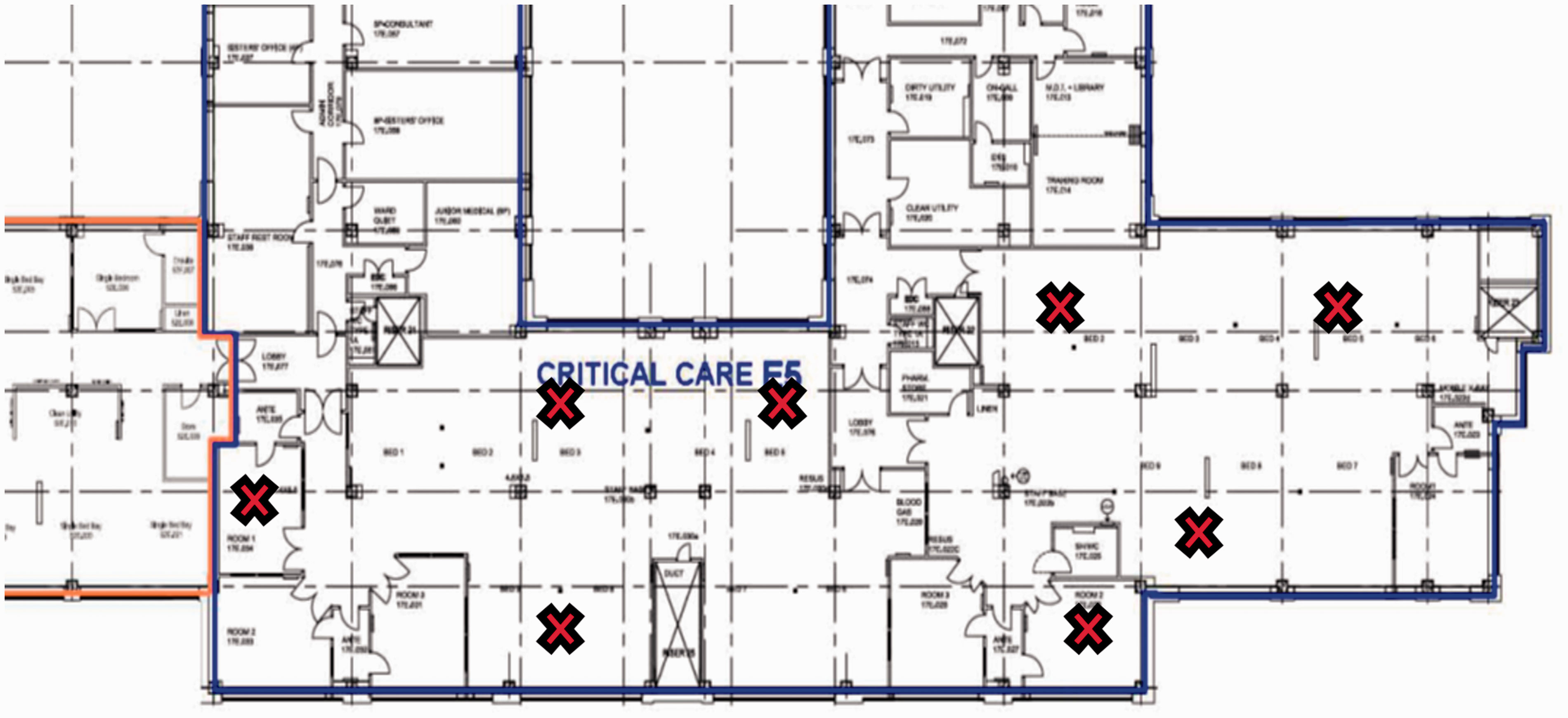
The Luxometer was only set up in bed spaces that already had patients admitted. It was positioned as close to the patient as possible (always within 1 m) with the level and angle of the sensor arranged in line with the patient’s eyes. In total, eight bed spaces were analysed to give a broad mix of areas around the unit. Each bed space was studied three times giving 24 nights’ data in total. The “night” period was defined as 23:00–07:00, with data recorded from November to December to avoid any seasonal variation during the recording period – we would expect a slight increase in the morning lux exposure during the summer months depending on unit design (amount/size of windows, etc.). The Luxometer was programmed to record data every 5 s giving 5760 data points per night. These data were downloaded to a Microsoft excel spreadsheet. In addition to lux, SOFA 19 score was calculated for the patient in the bed space monitored and the adjacent bed spaces. The purpose of recording SOFA scores was to evaluate if there were any association between illness severity and light exposure.
Optimal light levels in healthcare environments are covered by guidance endorsed by the department of health and published by the Chartered Institute of Building Services Engineers. 16 These guidelines closely follow the British Standard EN 12464-1, which are used for Private Finance initiative hospitals. BS EN 12464-1 sets out the nocturnal lux limit for critical care units to be 20 lux.
Data were not normally distributed and therefore analysed using Spearman’s rank coefficient for monotonic correlation. Due to non-parametric data differences between open bay (OB) and side rooms (SRs), they were analysed using Mann-Whitney U Test. The significance was calculated via a two-tailed P test, with a P-value of 0.05 being used as cut-off.
Results
Data were recorded over 24 nights and from 24 different patients (12 medical patients and 12 surgical). The average age of patients was 62.2 years (SD: 19.89, range: 20–89) and average SOFA was 6.8 (SD: 4.1, range: 0–14). Twelve patients were exposed to greater than 20 lux during nocturnal hours, with an average exposure time of 32.7 min (range: 0–87 min). Real time lux levels between 23:00 and 07:00 are demonstrated in Figure 2 with a median of these demonstrated in Figure 3. It is important to appreciate both the raw and average values as short periods of high lux that are concealed by averages that can significantly affect melatonin production.6–9
Real time lux levels between 23:00 and 07:00 for each bed space studied. One data set not included for illustrative purposes. Median lux recorded across all bed spaces between 23:00 and 07:00.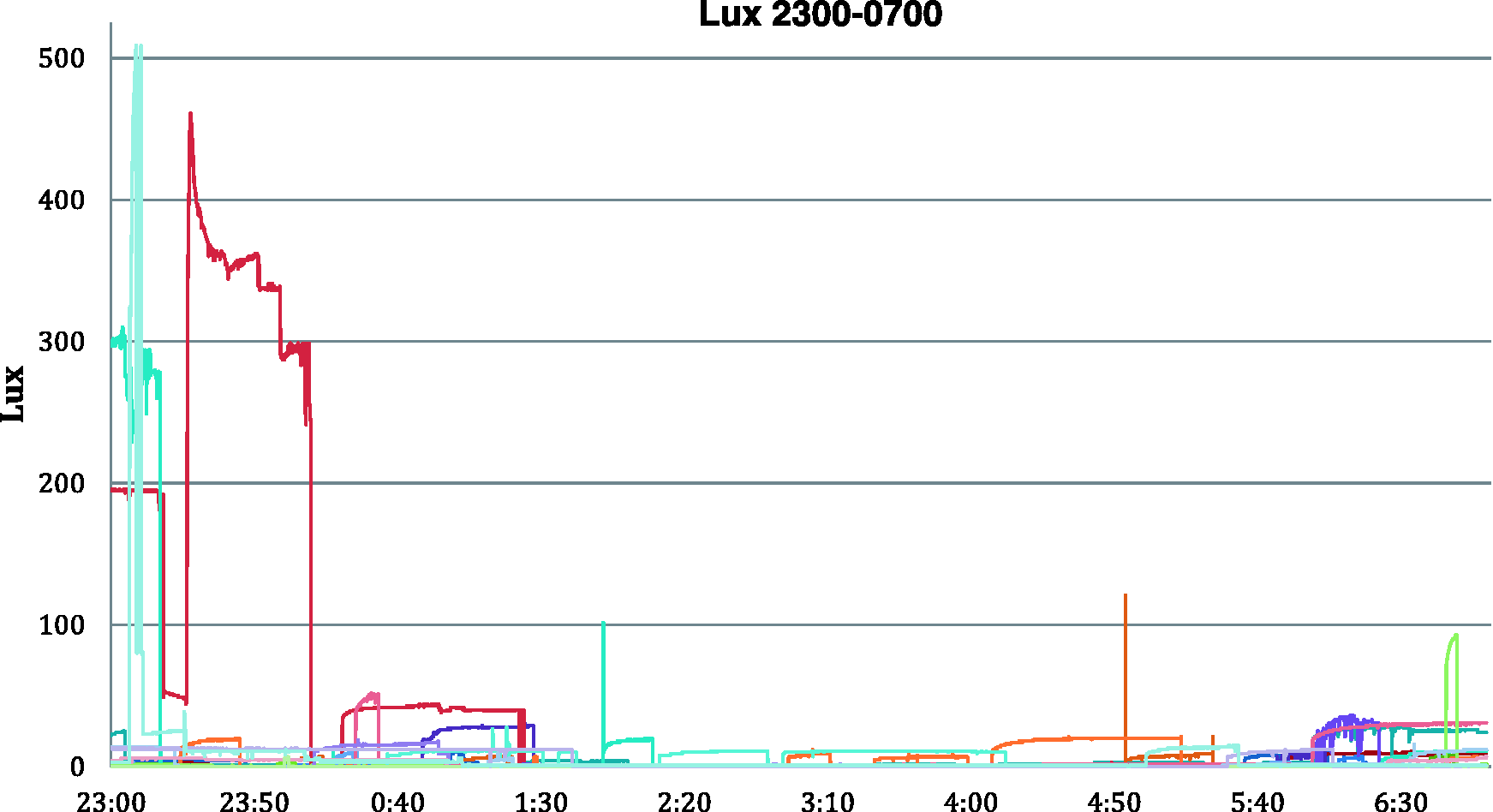
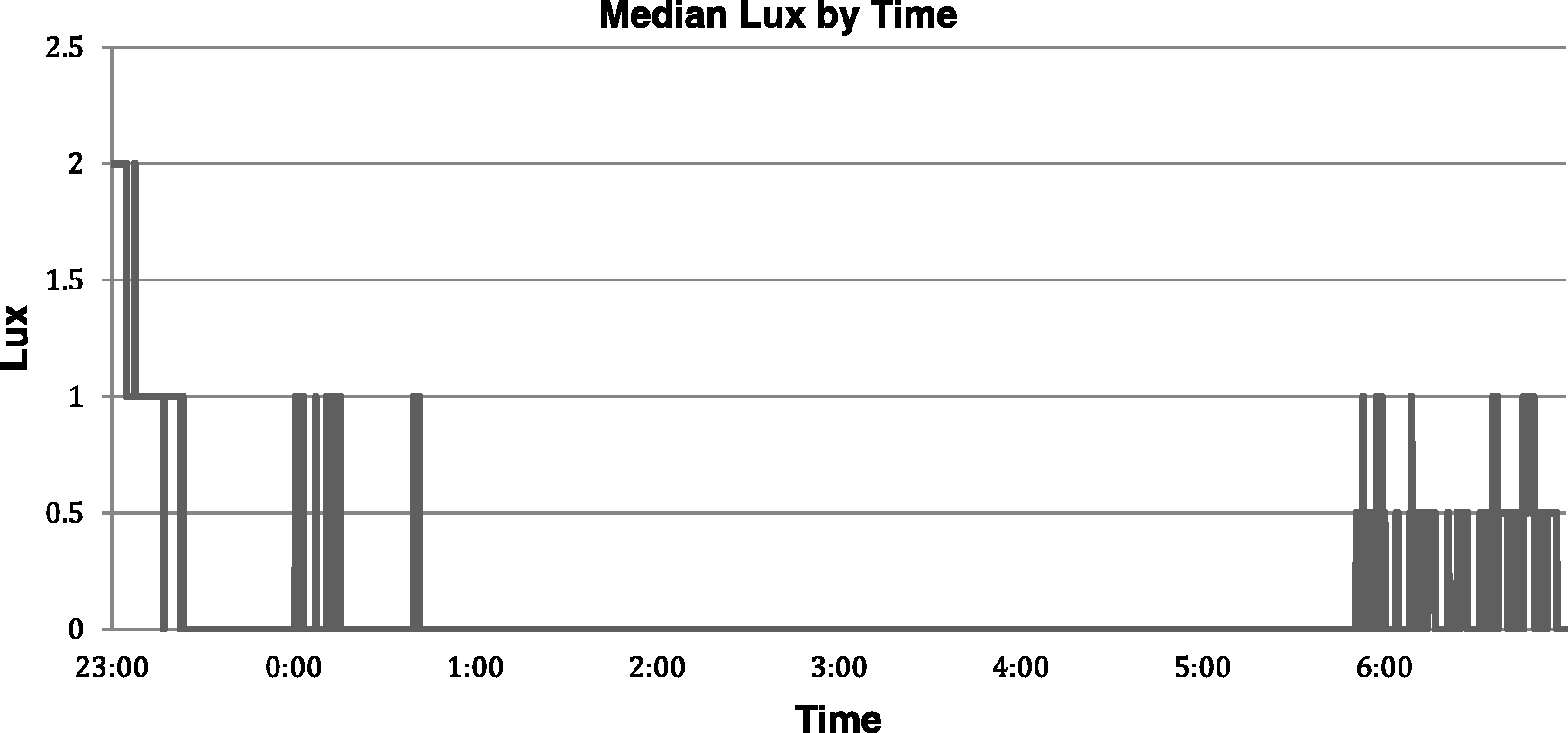
The median lux recorded across all bed spaces from 23:00 to 07:00 was 1.5 lux. There was positive correlation between patient illness severity and maximum lux (R = 0.45, P = 0.026); however, there was no relationship between illness severity and median lux exposure (R = 0.23, P = 0.28). As illness severity increased so did the time spent greater than 20 lux (R = 0.59, P = 0.0021), and the individual occasions where lux breached the 20 lux limit (R = 0.52, P = 0.009). There was no statistically significant relationship between neighbouring patient illness severity and maximum lux (R = − 0.11, P = 0.69) or neighbouring illness severity and median lux (R = −0.04, P = 0.87).
The maximum light exposure was highest in the SRs) compared to OBs (max SR 143.8 lux vs. max OB 101.98 lux) but not significant (U-test = 51, significance at P < 0.05 24). Median light exposure was higher outside of SRs (SR 0.33 lux vs. OB 30.66 lux) but possibly due to low sample size of SRs (6 data sets SR vs. 18 data sets OB), this was also not significant (U-test = 46, significance at P < 0.05 24).
Discussion
This prospective observational study shows that 50% of patients included in this pilot data were exposed to lux >20 at some point during the period of 23:00 and 07:00. This tended to be at the beginning and end of the recording period. There were delays in turning off lights; however, once lights were off, lux stayed generally low until the end of the recording period.
As would be predicted, as patient illness severity went up, maximum lux also increased, as did the absolute time spent >20 lux and the occasions >20 lux. This likely reflects the increasing workload and attention sicker patients demand. The average lux does not follow this trend, with those with higher illness severity being exposed to a lower median lux. This suggests that paradoxically while having higher spikes in lux, illness severity actually leads to lower average lux exposure. This may be due to staff being more aware of light when levels are very high (e.g. for a procedure) and then actively turning lights down low afterwards. The high spikes in lux may have acted as a prompt for action. In comparison, staff caring for less sick patients where very high levels of light were not required overnight may not have been aware of the amount of background lux their patients were exposed to. They may have therefore been less conscious of light as an issue and less likely to be light vigilant.
There were no correlations between adjacent patient SOFA and median or maximum lux; however, only 15 of the 24 patients studied had neighbouring patients on the data recording nights.
For one patient, very high median and max lux levels were recorded, despite a relatively low illness severity (Figure 4). These data were excluded from Figure 2 due to scale problems, which made visualisation of the remaining data difficult. After reviewing the notes of this patient, there were no clear reasons for these findings. It seems the staff caring for the patient overlooked the consequence of lux on outcomes, which highlights the importance of training and awareness of nocturnal light.
Maximum lux levels compared to patient illness severity (SOFA).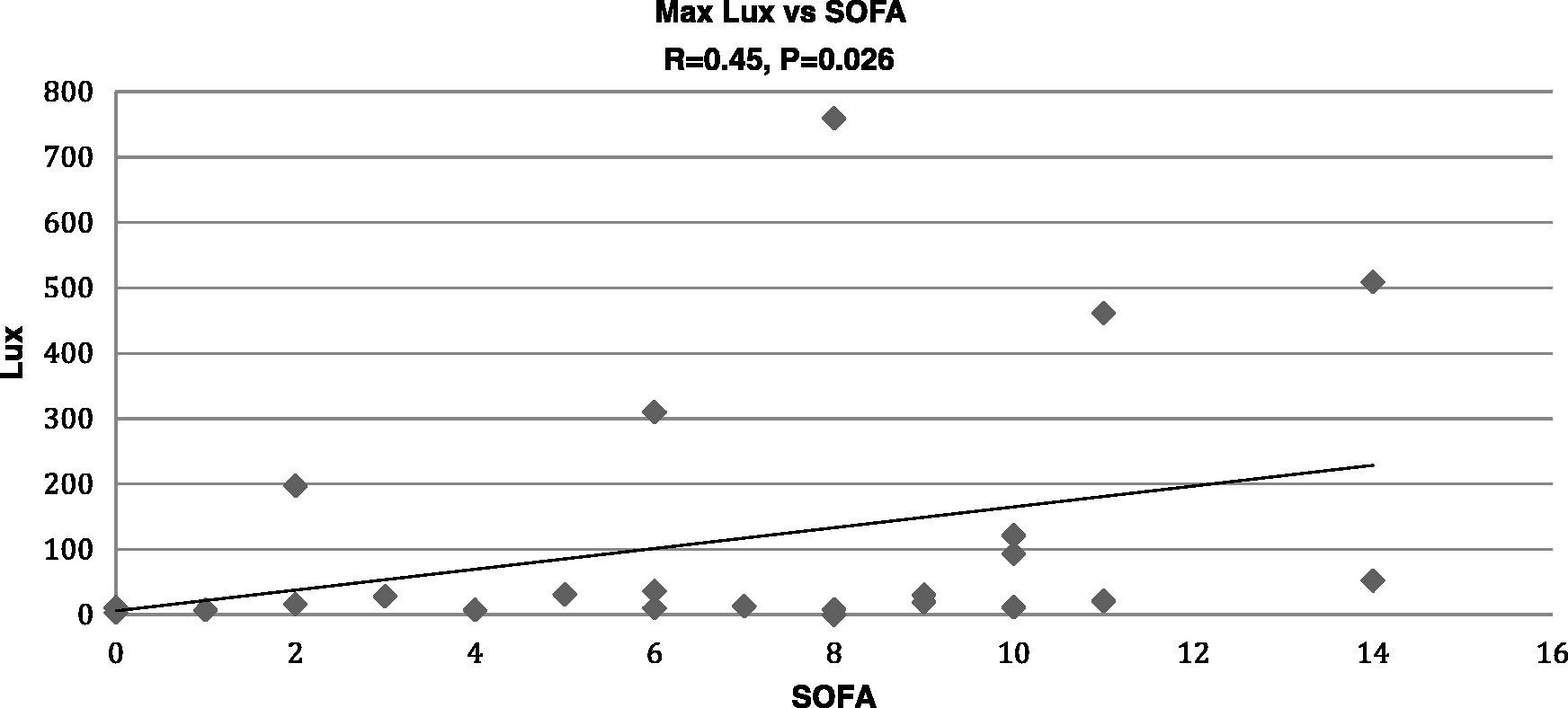
The building regulation of 20 lux limit appears to be overly lenient (roughly equating to a twilight evening) and potentially harmful to patients and needs further work to appraise its validity. It is not clear how much medical input has gone into this recommendation. We believe that this guidance is not robust enough for use in medical practice and needs a national medical body to review and advise on target nocturnal ICU lighting levels. The median recorded data were well below 20 lux and a reduction in nocturnal lux target below 20 would therefore be realistically achievable in modern ICUs.
This study has a number of limitations and confounders. It is a single-centre, observational study with recommended standards limited to building regulations rather than clinical guidelines. In addition, the Luxometer is not externally calibrated (however calibration at time of manufacture is completed). It also does not address patient-focussed outcomes.
However, as a pilot project, we have shown that it is feasible to measure lux in an intensive care environment and use this for education and a reminder of the importance of humanising the ICU setting. The cultural awareness this promulgates may assist with other areas such as addressing noise pollution and overall patient experience.
Moving forward, this study will be used as a framework for regional work to evaluate light levels and practice in other units within Wessex. This is soon to be adopted as a trainee-led project by SPARC-ICM, funded by a grant from the AAGBI. We intend to use these data to help produce national clinical guidance on optimal lighting levels and recommendations within the ICU. Future work needs to then concentrate on patient-centred outcomes, such as delirium, quality of sleep and patient experience.
Footnotes
Acknowledgements
Dr Jonathan Coates, Audit Lead, Portsmouth Critical Care department, Consultant in Critical Care and Emergency Medicine, Queen Alexandra Hospital, Portsmouth. Role: Assisted with registration as an audit and general study design.
Dr Thomas Pratt, Locum Consultant in Critical Care and Anaesthesia, Chichester Hospital. Role: Assisted with data collection.
Mr David Thom, Trainee Advanced Critical Care Practitioner, Queen Alexandra hospital, Portsmouth. Role: Assisted in devising name for the study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.