
Abstract
Introduction
Both Scottish and UK standards guidelines recommend that intensive care units should hold regular, structured, multidisciplinary morbidity and mortality meetings. The aim of this survey was to ascertain the nature of current practice with regards to morbidity and mortality case reviews and meetings in all intensive care units in Scotland.
Methods
Semi-structured telephone interviews were conducted with a consultant from all Scottish intensive care units. A list of intensive care units in Scotland was obtained from the Scottish Intensive Care Society Audit Group annual report.
Results
All 24 intensive care units (100%) in Scotland were surveyed. The interviews took an average of 20 min. The three cardiac intensive care units were excluded from analysis. All other intensive care units had morbidity and mortality meetings and 18 units had a morbidity and mortality clinical lead. Nineteen intensive care units held joint morbidity and mortality meetings, eight of which were regular. In all intensive care units, meetings were attended by consultants and trainees. In 14 intensive care units, meetings were attended by nurses, seven by allied health professionals, 1 by a manager and 11 by other professionals. All mortality cases in intensive care unit were discussed in 19 intensive care units, in the other two intensive care units, 10–20% of mortality cases were discussed.
Conclusion
There is a wide variation in the processes of reviewing mortality cases and significant events in intensive care units across Scotland, and in the way morbidity and mortality meetings are organised and held. Based on this survey, there is scope for improving the consistency of approach to morbidity and mortality case reviews and meetings in order to improve education and facilitate shared learning.
Introduction
Morbidity and mortality (M&M) case reviews and meetings are considered a vital component of the hospital governance process.1–3 They provide a systematic approach for the health care team to learn lessons from clinical outcomes, drive improvement in service delivery and support services to achieve and maintain high standards of care. 4 The M&M process begins with the identification and initial review of cases, presentation of these cases at an M&M meeting, then the implementation of agreed action points. 5 There is limited evidence on the impact of the M&M case reviews and meetings specifically on patient outcome. 6 However, regular M&M meetings provide a powerful resource for assessing quality of care and have an increasing role in improving patient safety and enhancing team cohesion.7–9 Despite this, it is a governance tool that is widely underutilised. 10
It is inevitable that some patients will have an unsatisfactory event, or die, during the course of their intensive care unit (ICU) stay. With similar inevitability, it will be possible to identify areas of practice that could have been done differently in these instances. On occasion these areas will point to potential improvements in the delivery of care that is provided. It is essential to identify those factors that have, or could have, impacted on patient outcome. Proper scrutiny is therefore important so that system, team and individual learning can be achieved to the benefit of subsequent patients. Further, proper processes facilitate a full and transparent account of events and can contribute positively to the resolution of complaints. 4
Adverse events are identified more frequently in ICU than any other hospital setting and their consequences are often more severe. 7 While the opportunities for learning from M&M case reviews are vast, variation in the process limits operation and impact. Published papers report significant heterogeneity regarding M&M implementation, structure, delivery and educational goals.11–13 There are limited studies on the conduct of M&M case reviews and meetings in adult ICUs with no published reports covering all ICUs in any one country.
In its publication on minimum standards and quality indicators,
1
the Scottish Intensive Care Society Audit Group (SICSAG) recommended that:
All ICUs should hold regular, structured, multidisciplinary (MDT) meetings. All unit deaths and significant adverse event should be discussed at these meetings. A written record should be kept. A timely and reliable method for dissemination of shared learning should be in place.
We aimed to compare current practice of M&M case reviews and meetings in all ICUs in Scotland to the standards above.
Methods
Participation in this survey was voluntary and consent was obtained on preliminary contact with responding clinicians, and again at the start of the telephone interview, formal ethical approval was not sought. A literature search was conducted in order to identify publications outlining factors considered important for effective M&M case reviews and meetings. A semi-structured survey form was created on Google Forms™ (online Appendix 1) based on the literature review and the national guidelines published by SICSAG. These guidelines recommended that M&M meetings should be regular, open and blame free, as well as multi-disciplinary. In addition, all deaths, critical incidents and near misses should be reviewed and a written record should be kept. Learning points should be timely and reliably disseminated, and feedback provided to all involved parties. 1
The list of Scottish ICUs was obtained from the SICSAG annual report published in 2015. 3 Telephone interviews were carried out with a consultant from each ICU from 26 May 2016 to 9 September 2016 by the three consultant authors. The survey form was filled in during the telephone interviews. After all interviews were complete, data were exported to Microsoft Excel™ for analysis. Figures are presented as numbers or mean (SD).
Results
All 24 ICUs (100%) in Scotland were surveyed. The duration of the interviews was 20 (6) minutes. The three cardiac ICUs had M&M processes linked to cardiac services and were therefore excluded from analysis.
Standard 1. All ICUs should hold regular, structured, MDT meetings
Frequency of M&M meetings.
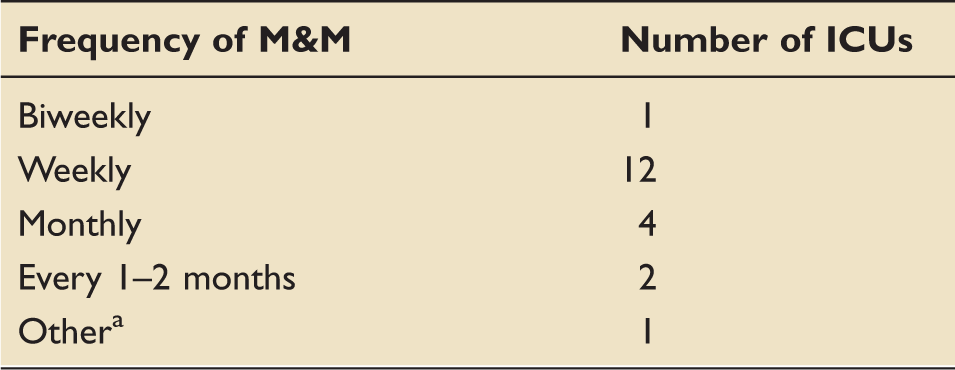
ICU: intensive care unit; M&M: morbidity and mortality.
Following every five deaths.
Professional groups attending M&M meetings.
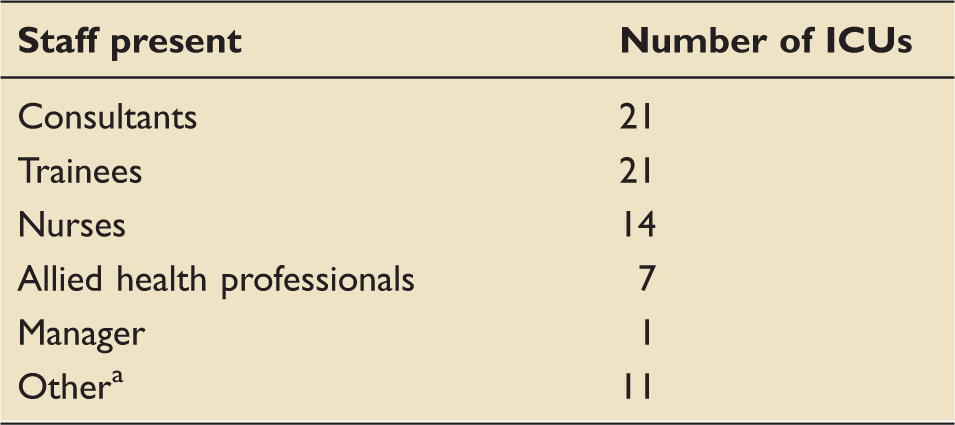
ICU: intensive care unit; M&M: morbidity and mortality.
Associate specialists, staff grades, critical care nurse practitioners and medical students.
A consultant was responsible for organising the meetings in 20 ICUs. Eighteen ICUs had an M&M lead, seven of whom had specific supporting professional activity (SPA) time allocated to the role.
Nine ICUs linked M&M case reviews and meetings to other hospital processes. Two ICUs presented cases at hospital M&M meetings, one ICU submitted cases using a hospital-wide M&M referral form, five ICUs linked cases to the electronic reporting system DATIX™ and were reviewed by the clinical risk team, and one ICU regularly reported to the hospital clinical governance group.
Standard 2. All unit deaths and significant adverse events should be discussed at these meetings
All mortality cases in ICU were reviewed in 19 ICUs, while 10–20% of mortality cases were reviewed in the other two. Specific cases for presentation were selected in 16 ICUs. Seven ICUs selected cases where learning points were identified. Cases with patient safety issues were selected in two ICUs and one ICU used a low predicted mortality as a trigger for presentation of mortality cases.
Structure used to review deaths.
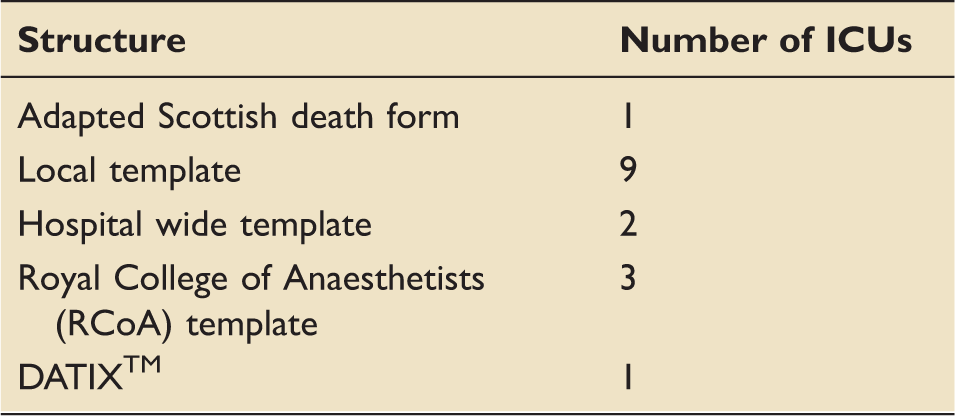
ICU: intensive care unit.
Significant events were reported in all ICUs. They were reviewed using DATIX™ in 17 and presented in 19 ICUs. Ten ICUs used a template for presenting significant events.
Standard 3. A written record should be kept
A written record of the meetings was kept in 13 ICUs.
Standard 4. A timely and reliable method for dissemination of shared learning should be in place
Learning points were disseminated in all ICUs. This was done by email following the meeting in 13 ICUs, stored on a database and disseminated at a later date in four ICUs, and documented on paper viewable by staff in two ICUs. One ICU had a weekly discussion of learning points and in one ICU, it was unclear how this information was disseminated.
There were mixed comments at the end of the survey. Two ICUs had seen significant recent improvements in their M&M process and one commented that they were keen to develop it further. One ICU reported successful establishment of a no blame culture and had witnessed significant improvement with the introduction of a structured process. Four ICUs described an absence of interdisciplinary involvement, difficulties in team engagement and lack of a robust reporting system leading to under identification of important clinical issues.
Discussion
This survey demonstrated that M&M case reviews and meetings in Scottish ICUs have reasonable compliance with the four standards set by SICSAG. However, there is considerable variation in practice.
The opportunity for clinicians, nurses and allied health professionals (AHPs) to discuss aspects of care where the outcome was not intended in an open and reflective manner is essential to support learning and promote patient safety. 14 However, organisational difficulties and impact on service provision may present obstacles to MDT involvement. Other obstacles to implementing M&M meetings are lack of a structured process, inexperience and physicians’ resistance. 15 Although medical professionals attended M&M meetings in all ICUs in our study, attendance was not as high for other professional groups. This finding is not dissimilar to a UK wide email survey of 429 (22% response rate) surgeons across five specialties, which revealed that nonmedical staff were invited to fewer than 50% of meetings. 16 Furthermore, Mehta found a significant reduction in patient safety incidents due to medical error, but not nursing error after introduction of a structured M&M process. This emphasises the importance of MDT involvement at M&M meetings. 17 This would not only enhance the quality of case reviews but would maximise the educational value and learning. 18 Participation is encouraged by effective feedback and review of action points thereby demonstrating the positive impact of the process. 14 Lack of MDT involvement will no doubt lead to missed opportunities to address some of the issues highlighted by the M&M process.
Almost all ICUs surveyed organised M&M meetings with other departments in the hospital. The value of this hospital wide involvement is that it may facilitate understanding of broader system challenges less visible at the departmental level. 19 Formal reporting of meeting outcomes to the hospital clinical governance structure improves sharing of learning and helps aid quality assurance. 10 Only one ICU in our study reported to the clinical governance team. It is every health care professional’s responsibility to be open, honest and tell patients and their families when there is an unintended outcome. 20 The duty of candour states patients and relatives should be informed of any outcomes of the M&M process. 21 On this basis, it is prudent that meeting outcomes reach beyond the individual ICU into the wider hospital governance structure.
Our survey demonstrated variation in how cases are selected for review and presentation. All deaths were discussed in 19 units, which is concordant with standard 2 from SICSAG. Significant events were reviewed in all units. In 2013, Kuteifan and colleagues published a national survey of M&M meeting implementation in 293 ICUs in France. The response rate was 170 (58%). All deaths were analysed in 38%, unexpected deaths in 42% and severe adverse events in 56% of all ICUs. 18 Moreover, the recent Scottish Morbidity and Mortality (SMMP) report emphasised the opportunity for learning from cases of excellence. Discussion of these cases can increase educational opportunities further and improve resilience and staff morale.14,22 Although we did not specifically ask about this, no ICU offered evidence that this is currently ongoing within Scottish ICUs.
Only 13 ICUs kept a written record of the M&M meetings. Written records of discussions are valuable and evidence of M&M discussions relating to individual patients has been requested by the Procurator Fiscal and during cases of litigation. 23 There was significant variability in the way learning was disseminated.
Variability in practice was also demonstrated in a recent American survey of 75 PICUs, which reported a lack of M&M conference structure and consistency, 24 and in a recent survey of 15 general surgical units in the West of Scotland which found a large diversity in structure and frequency of meetings as well as the participants. 25
To address such problems, the Safe Anaesthesia Liaison Group published a document in 2013 with the aim of facilitating effective meetings, improving the quality of presentations and increasing their educational value. 26 The use of the situation, background, assessment and recommendation (SBAR) communication format when reviewing cases has been shown to improve assessment and analysis of cases, and assist effective learning for both junior and senior attendees. 26 In May 2017, Health Improvement Scotland released a practice guide which emphasised the role of the M&M process in collective learning and improving the quality and safety of care. 14 Higginson and colleagues demonstrated that a structured approach increases the official nature of meetings; whilst a greater focus on accountability does not compromise educational and learning opportunities. A standardised process provides reassurance that all cases are reviewed in the same way and can guide questioning making it easier to extract the relevant information from the case notes. 10
Despite the limited evidence that M&M meetings improve patient safety, a large proportion of participants perceive this to be positive. 27 Lecoanet and colleagues conducted a survey of professionals involved in M&M conferences in three French teaching hospitals. There were 698 participants of whom 91% were satisfied with the conduct of the meetings with the main benefit perceived to be improvements in health care quality and patient safety. 27
Our study is the first comprehensive nationwide survey of the structure and conduct of M&M case reviews and meetings in ICUs. The results show a wide variation in the processes of reviewing mortality cases and significant events in ICUs, as well as the way M&M meetings are organised.
One of the limitations of this survey was that it was a reported rather than an observed account of the M&M case reviews and meeting in the ICUs. Despite a 100% response rate, the interviews were conducted with one consultant per unit; this meant that the opinions expressed and documented in the free text of the form were those of the interviewee.
Some plurality of processes is no doubt appropriate, but based on this survey, and taking into account the recent publication by SMMP, there is scope for better aligning practices. This may lead to higher compliance rates with SICSAG standards with the aim of enhancing the delivery of safe and effective care, and demonstrating equity of care across the country.
Footnotes
Acknowledgements
Many thanks to the Greater Glasgow and Clyde library network for assisting with our literature search and all the clinicians who took part in the interviews. This article was presented as a poster at the Scottish Intensive Care Society Annual Scientific Meeting, St. Andrews, UK on 26 January 2017.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.