
Abstract
Objective
Intensive care unit patients are at risk for catheter-associated urinary tract infection. Earlier removal of catheters may be possible with accurate measurement of bladder volume. The purpose was to compare measured bladder volumes with bedside ultrasound, bladder scanner, and urine volume.
Design
Prospective correlational descriptive study.
Setting
Surgical/trauma intensive care unit and medical intensive care unit.
Patients
Renal dialysis patients with less than 100 ml of urine in 24 h prior to urinary catheter removal and patients with suspected catheter obstruction.
Measurements and main results
A physician trained in ultrasound and an advanced practice registered nurse trained in bladder scanning measured bladder volume; each blinded to the other’s measurement. Device used first (ultrasound or bladder scanner) alternated daily. The intensive care unit team determined need for intermittent catheterization or treatment for suspected obstruction. Fifty-one measurements from 13 patients were obtained with results reported in milliliters. Ultrasound measurements were a mean volume of 72.1 ± 127 (range: 1.7–666) and the bladder scanner measurements were 117 ± 131 (0–529). On six occasions in five dialysis patients, urine volume measurement was available. The mean difference in ultrasound–urine volume mean difference was 0.5 ± 37.8 (range: −68 to 38.2) and the bladder scanner–urine volume was 132 ± 167 (−72 to 397). Two patients with suspected catheter obstructions had ultrasound, bladder scanner, urine volume measurements, respectively: (1) 539, 51, >300 (began voiding before catheter replaced); (2) 666, 68, 1000 with catheter replacement. Conditions leading to greatest differences were obesity, indwelling catheter and ascites.
Conclusions
These results demonstrate the inaccuracy of the bladder scanner. Ultrasound measurements appear more accurate. To remove urinary catheters in patients with minimal to low urine output, serial ultrasound measurements can be used to monitor bladder volumes and return of renal function.
Critically ill patients frequently require hourly monitoring of urine output with an indwelling urinary catheter placing them at risk for catheter-associated urinary tract infection (CAUTI). CAUTI remains an important healthcare-associated infection, despite national prevention guidelines and mandates for reduction. The daily risk of acquiring bacteriuria is 3%–7% with an indwelling urinary catheter. 1 Urinary catheter utilization rates are higher in the intensive care unit (ICU), 61% compared to 20% in non-ICU areas. 2 However, in recent studies with collaborative multi-institutional CAUTI reduction approaches, CAUTI rate in the ICUs failed to decrease.3,4 The use of bladder ultrasound is recommended in strategies to reduce indwelling urinary catheter days with a removal protocol and to verify urinary retention before catheterization. 5 There is very limited data assessing the diagnostic accuracy of ultrasound (US) bladder volume measurements in ICU patients, either with a bladder scanner (BS) or conventional bedside US. BS measurements are obtained with placement of scanner probe on the skin over landmarks of the expected bladder location. The BS does not allow the clinician to visualize the bladder. Point-of-care US allows clinicians to visualize the bladder and avoid measuring other abdominal fluid collections. Also, studies on BS and US bladder volume measurements have not been performed in patients with acute kidney injury and chronic kidney disease with low bladder volumes. Targeting patients with renal failure in the ICU for prompt catheter removal could reduce CAUTI.
The purpose of this pilot study was to compare the measured bladder volumes with a BS compared to US and urine volume (UVol) in ICU patients with low urine output receiving dialysis and in ICU patients with suspected urinary catheter obstruction.
Methods
This was a correlational descriptive study. Approval from the human subject committee was obtained. Patients or their legally authorized representative were consented prior to enrollment. Eligible patients were ≥18 years old, dialysis patients with less than 100 ml of urine in 24 h who had their catheters removed or ICU patients with suspected urinary catheter obstruction. Patients were excluded if consent was unable to be obtained.
Patients were enrolled in a 36-bed surgical/burn/trauma ICU and a 34-bed medical ICU at an 1100-bed tertiary academic medical center. Data collection was performed by four physicians and three advanced practice registered nurses (APRN). Prospective data on bladder volume measurements were collected by two study team members, a physician skilled in US bladder volume measurement and an APRN skilled in the BS. Both the BS and the US were used to measure bladder volumes. BS measurements were repeated several times at each measurement time point in the attempt to obtain a signal in all four quadrants per manufacturer’s guidelines. Utilization of the first measuring device alternated, odd days started with the BS (BMI 9400,Verathon Inc., Bothell, WA) and even days started with the US (Zonare Ultra version 4.8, Mountain View, CA or Sonosite M-turbo, Bothell, WA). During data acquisition, the study team members were blinded to the other device’s bladder volume measurement result. The results of the two tests were reported to the clinical team and documented in the medical record. The decision to perform an intermittent straight catheterization (ISC) on the patient was performed at the ICU clinical team’s discretion. The patient’s nurse performed the ISC. UVol was documented in the medical record. BS and US measurements were conducted daily Monday through Friday by the study team for dialysis patients. The outcome of indwelling catheter-free days was measured by days in the study without an indwelling urinary catheter.
The desired sample size was 100 measurements comparing BS, US and UVol. Data were analyzed using descriptive statistics and repeated measures Bland-Altman analysis for agreement between two methods using SPSS 22 (IBM Corporation, Armonk, NY).
Results
The final sample included 13 patients with 51 paired measurements (BS and US) and 7 patients with 8 UVol measurements (ISC or void). On six occasions, in dialysis patients, UVol measurement was available from an ISC (five measurements) or void (one measurement). There were 49 measurements in patients with renal failure requiring dialysis and 2 measurements in patients with suspected urinary catheter obstruction. Figure 1 shows the difference between the US and BS methods against the average of the two measures. Points are labeled by the subject number. The mean difference between the US and BS methods (−39.0) and Bland-Altman limits of agreement are shown on the scatter plot as well. The limits appear to fit the data well. On average, the BS method resulted in a measurement approximately 39 ml higher than the US.
Bland-Altman plot of US to BS measurements.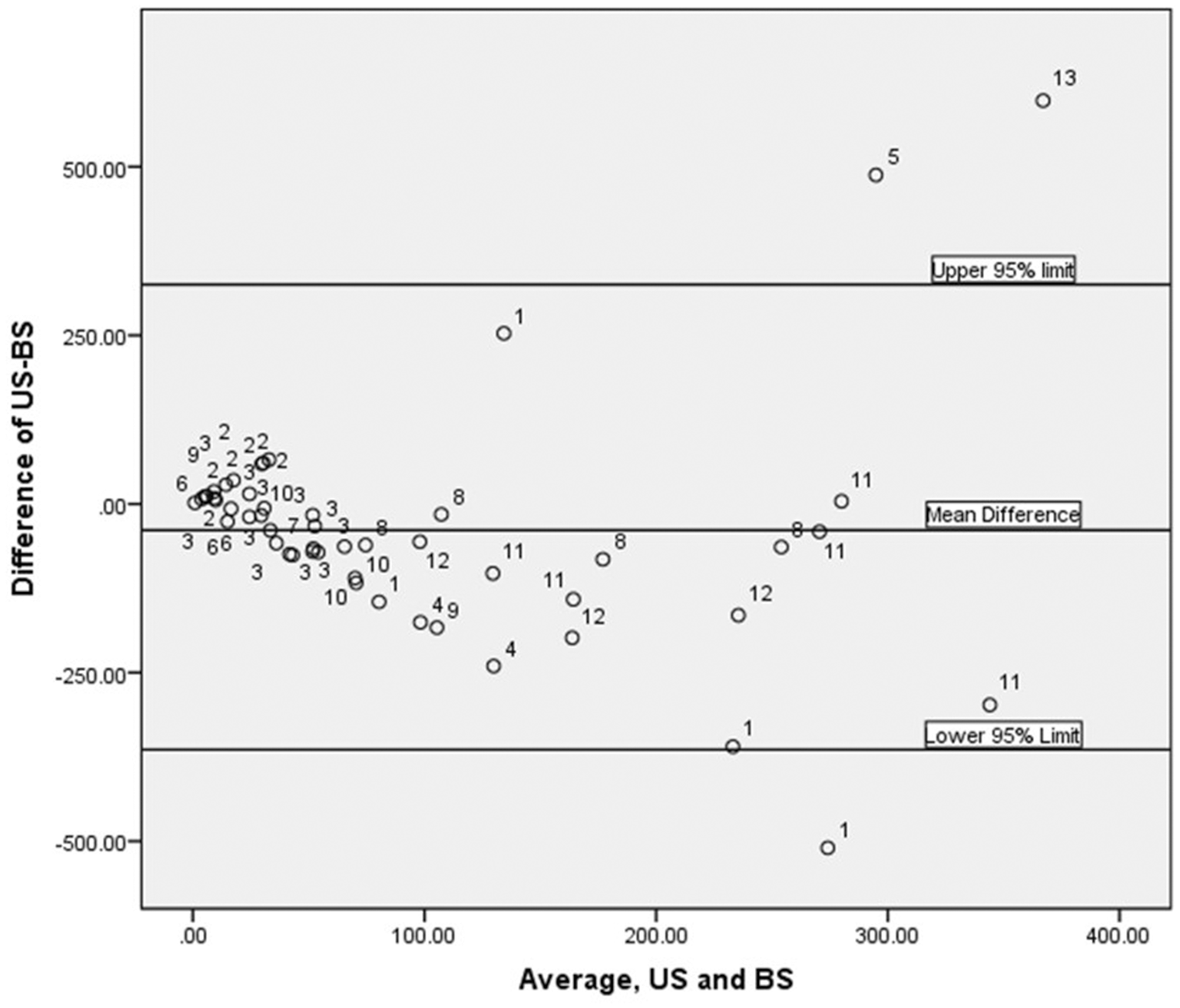
Summary of results.
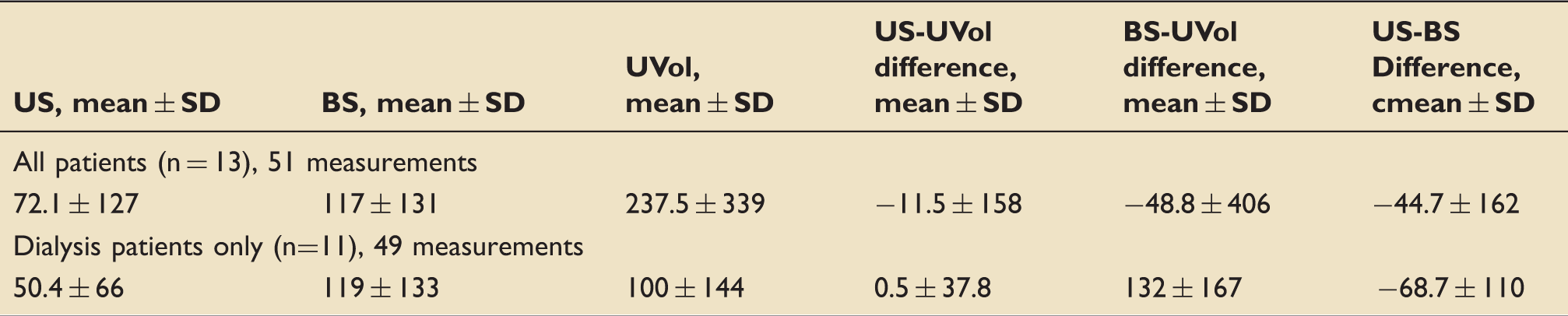
Note: all measurements reported in milliliters.
BS: bladder scanner; US: ultrasound; UVol: urine volume.
Bladder volume measurement comparisons with all three methods.
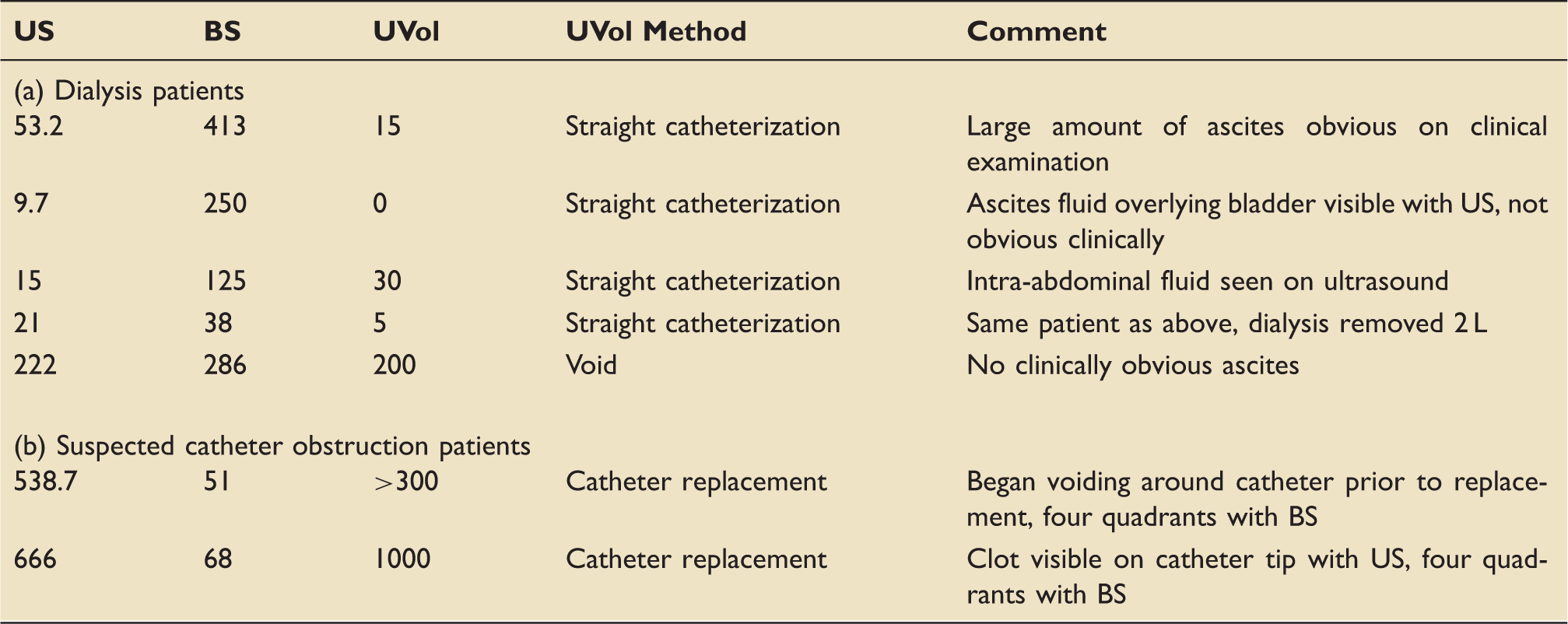
Note: All measurements reported in milliliters.
BS: bladder scanner; US: ultrasound; UVol: urine volume.
Discrepancy was also noted in a bariatric patient. Seven sets of measurements were obtained on one patient with a BMI of 52.6. The BS repeatedly interpreted bladder volume as zero with the inability to obtain any quadrants compared to the US showing a mean volume of 39.7 ml. The US was able to visualize the patient’s bladder to obtain measurements. For this patient, no UVol measurements were taken to compare with the BS and US.
There were instances when the BS and US showed comparable volumes. One patient with acute kidney injury had 14 paired measurements with mean US volume of 21.1 ml compared to the mean BS volume of 39.9 ml. No Uvol measurements were available for comparison. This patient had 17 catheter-free days. Of the 49 measurements on dialysis patients, only 5 had an ISC performed resulting in 51 completely catheter-free days. Based on these results, BS measurements may not be accurate in renal failure patients in the ICU. However, due to the low number of ISC volumes, additional data are needed.
Discussion
Overall, US was more accurate when UVol measurements were available. The ICU clinical team stopped ordering ISC due to the accuracy and confidence in US measurements. Clinicians lacked confidence in BS measurements. The blind nature of BS measurement does not allow differentiation of bladder from other fluid collections. Hence, patients with liver, renal or cardiac failure who have increased risk of developing ascites present a challenge to accurate BS measurement of UVol. The inability to find the bladder with the blind BS method also led to inaccuracy.
In addition, in patients with suspected obstructed indwelling urinary catheters, the US could differentiate the catheter balloon and clot around the tip of the catheter from the UVol in the bladder. US can promptly measure an accurate bladder volume and determine the need to replace the urinary catheter. Hence, unnecessary catheter exchanges may be eliminated.
Previous studies have demonstrated the role of BS to reduce catheter days and to assess the need for ISC.6–9 However, the majority of studies were conducted as post-void measurements or in surgical patients. Additionally, the majority of literature evaluating BS was conducted in non-ICU populations. In addition, no studies examined the accuracy of the BS in patients with renal dialysis. Of the 49 measurements on dialysis patients in our study, only 5 ISCs were performed resulting in 51 completely catheter-free days which included weekend days when BS and US measurements were not conducted. Hence, accurate US measurements can eliminate indwelling urinary catheter days.
Choe et al. 10 were the first to identify the potential inaccuracy of the BS due to the inability to distinguish UVol from other fluid collections in the pelvis or lower abdomen. In ICU patients, lack of direct visualization is a hindrance to accuracy in bariatric patients, patients with abdominal or pelvic fluid collections or suspected indwelling catheter obstruction. Abdominal and pelvic fluid collections are not always clinically apparent prior to bladder volume measurements with the BS but can be seen with US. Therefore, more research is needed using US measurement of UVol to eliminate catheter days with potential reduction in CAUTI. Research is also needed to examine the feasibility of bedside registered nurses conducting US measurement of the bladder volume to use in place of BS measurement in urinary catheter removal protocols. Newer models of the BS now allow for visualization of the bladder; however, no studies comparing BS measurement with these new models and US have been published.
Limitations of the study include small sample size and single center. Verification bias limited the number of actual UVol measurements. The small sample size, even with repeated measures for each person did not allow for Bland-Altman analysis of BS and UVol or US and UVol due to the low number of actual UVol measurements. In addition, the Bland-Altman analysis assumes the normality of differences between the two measurements (US and BS). However, the normality assumption does not hold for these data even with a log transformation due to the small sample size.
By allowing the clinicians to order ISC, real-world clinical practice was incorporated into the study protocol. Elimination of catheter days was sought which would reduce the risk for urinary tract infection from multiple ISCs. Stoppage of the study prematurely may overestimate the benefit of US due to the small sample size. No inter-rater reliability was conducted which is a potential limitation in accuracy. However, the clinicians performing the measurements were all experienced in the use of the devices.
Conclusion
Serial use of point-of-care US to monitor bladder volume is feasible and may reduce catheter days in patients with minimal to low urine output. Further research is needed on the ability of US to assess for return of renal function in critically ill dialysis patients and reduction of CAUTI rates. The results also support the use of US to measure UVol with suspected obstruction of indwelling catheter.
Footnotes
Acknowledgements
The authors would like to acknowledge Brad Bemiss MD and Jesse Meacham MD for their assistance with ultrasound measures and all of the nursing and medical staff in both ICUs for their support of the study. The study was conducted at Barnes-Jewish Hospital at Washington University.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Enyo A Ablordeppey was supported by Washington University School of Medicine Faculty Scholars grant and the Foundation for Barnes-Jewish Hospital grant.