
Abstract
Between 1 April 2012 and 31 March 2015, 263 of the 2244 families in the UK whose loved ones had registered to donate organs for transplantation after their death on the NHS Organ Donor Register chose to override this decision; an override rate of 11.7%. Multivariable logistic regression analysis was applied to data relating to various aspects of the family approach in order to identify factors associated with such overrides. The factors associated with family overrides were failure to involve the Specialist Nurse for Organ Donation in the family approach (odds ratio 3.0), donation after circulatory death (odds ratio 2.7) and Black, Asian or Minority Ethnicity (odds ratio 2.7). This highlights the need to further engage with these groups in exploring donation as an end of life choice, and suggests that there may be, from the perspective of the family, fundamental differences between donation after brainstem death and circulatory death. It further adds to the body of data linking involvement of the Specialist Nurse for Organ Donation in the family approach to improved UK consent rates.
Keywords
Introduction
There has been a 69% increase in deceased organ donation in the UK since the publication of the Organ Donation Taskforce report in January 2008. 1 However, deceased donor numbers continue to lag well behind those reported from many other countries, 2 with high rates of family refusals identified as a major obstacle to increasing the availability of organs for transplantation. 3
The NHS Organ Donor Register (ODR) was established in 1995. Since then, more than 20 million people have registered a decision to make their organs available after death for the purposes of transplantation. 1 Whilst families are much more likely to support organ donation when a loved one’s wishes are known, 4 a significant proportion continue to override such decisions.
The identification of avoidable or modifiable factors that prompt a family to withhold consent (authorisation in Scotland 5 ) for organ donation is considered to be an important means by which family refusal can be reduced.6,7 The purpose of this retrospective cohort study was to identify factors, particularly those that might be amenable to change, associated with refusals for organ donation made by families despite the knowledge that their relative had in life registered on the ODR their wish to donate their organs in the event of their death.
Methodology
NHS Blood and Transplant (NHSBT) continuously audits the potential for organ donation from patients who die in circumstances where donation is a possibility. 8 The audit comprises a data set that covers the donation pathway and records the reasons the potential for donation was lost. 9 This retrospective study included families approached for organ donation between 1 April 2012 to 31 March 2015 and where the potential donor was known to be registered on the ODR. Excluded from the study were those occasions where data collection was incomplete. The analysis was performed using commercially available software (SAS enterprise guide 6.4, SAS Institute, Carey, NC, USA).
Univariable and multivariable logistic regression were used to model the probability of the family overriding their relative’s wish to donate as recorded on the ODR. The factors investigated in these models were patient age, donation pathway (donation after brainstem death; DBD or donation after circulatory death; DCD), patient gender, cause of death, patient ethnicity, weekday time of donation, time of day of the family approach, number of family members present for the approach, involvement of a Specialist Nurse for Organ Donation (SNOD) in the approach and financial year.
Univariable (non-risk adjusted) logistic regression was used to investigate these factors in isolation and a multivariable (risk-adjusted) logistic regression model was then used to determine which of these factors were significant in the presence of other additional factors, i.e. which factors were significantly associated with a family override even after being adjusted for the influence of confounding factors.
Results
Audit data from 2244 approaches to families of patients registered as donors on the ODR were included in the study and a further 63 cases were excluded because of incomplete data. Of the 2244 family approaches analysed, 263 families chose to override their relative’s registered donation decision, an override rate of 11.7%.
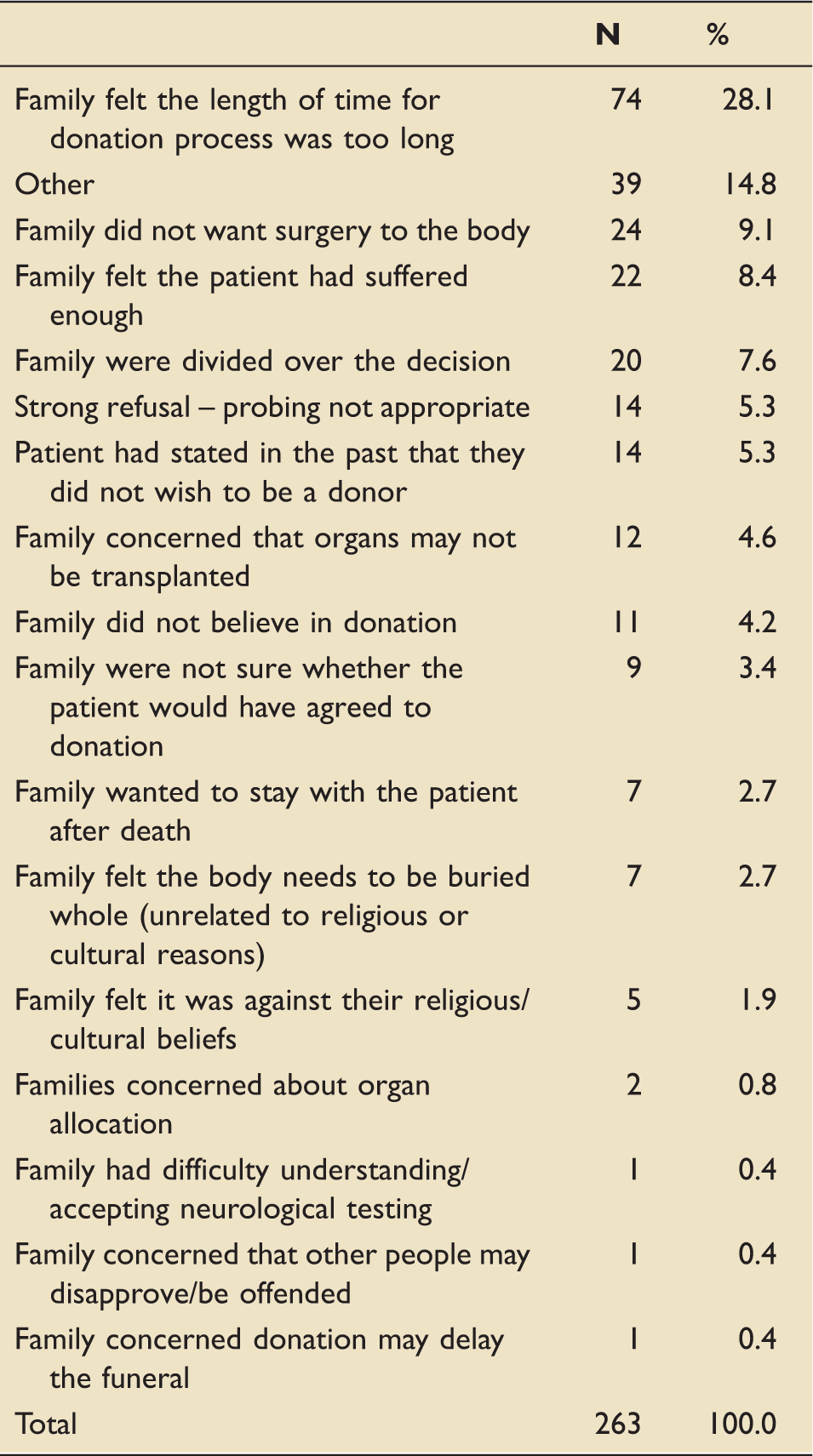
Reasons for a family’s decision to override the registered wish of a loved one to donate their organs for transplantation after death.
Univariable logistic models.
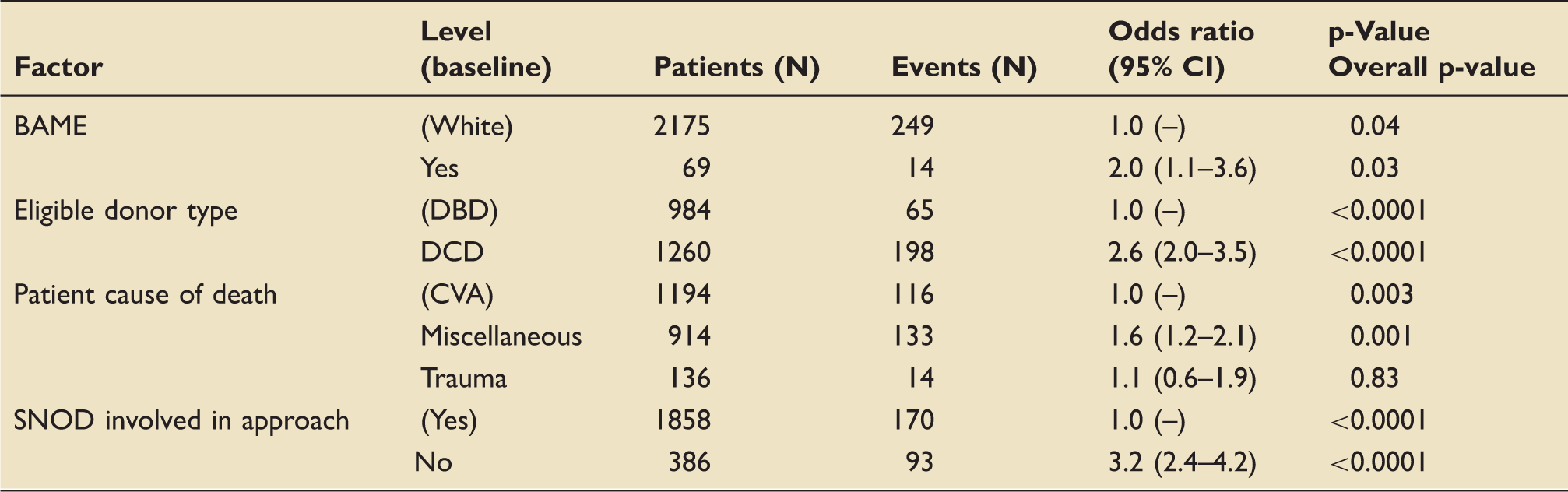
Note: Factors that were not significant: patient gender, patient age group (0–17, 18–24, 25–34, 35–49, 50–59, 60+), working hours (7am–7 pm and 9am–9 pm), number of family members present (1–2, 3–4, 5+ and 1, 2, 3, 4, 5+), weekends, financial year. Miscellaneous causes of death included patients who died from cardiovascular causes, brain damage, organ failure, drug-related causes, infections and cancer including brain tumours.
BAME: Black, Asian or Minority Ethnic; CVA: Cerebrovascular accident/Stroke; DBD: donation after brainstem death; DCD: donation after circulatory death; SNOD: Specialist Nurse for Organ Donation.
Multivariable logistic models.
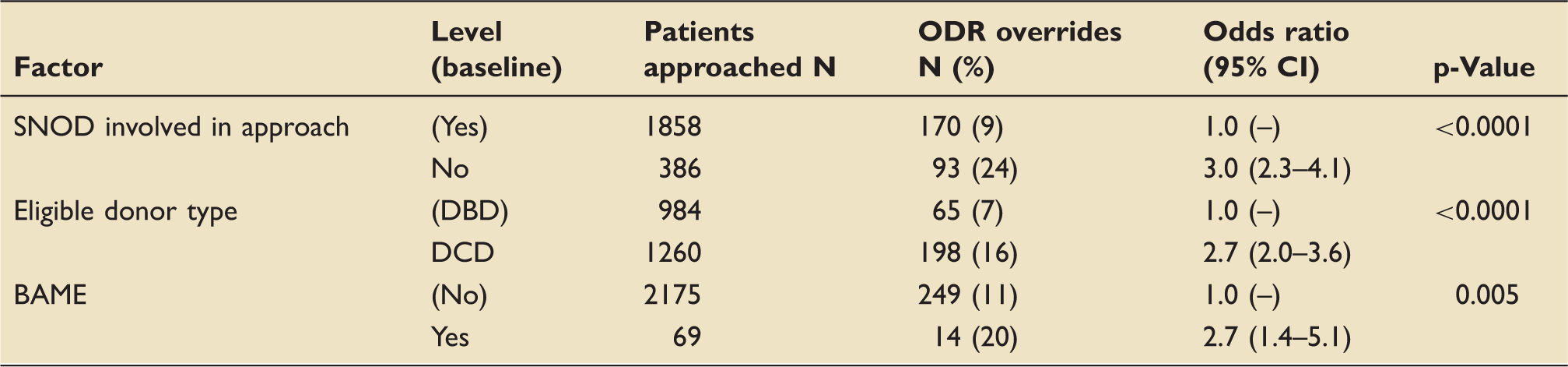
Note: Factors that were not significant: patient gender, patient age group (0–17, 18–24, 25–34, 35–49, 50–59, 60+), working hours (7am–7 pm and 9am–9 pm), number of family members present (1–2, 3–4, 5+ and 1, 2, 3, 4, 5+), time of the week (weekday or weekends), financial year and patient cause of death (CVA, miscellaneous, trauma).
BAME: Black, Asian or Minority Ethnic; DBD: donation after brainstem death; DCD: donation after circulatory death; SNOD: Specialist Nurse for Organ Donation.
Reasons for family refusals by factors associated with family override.
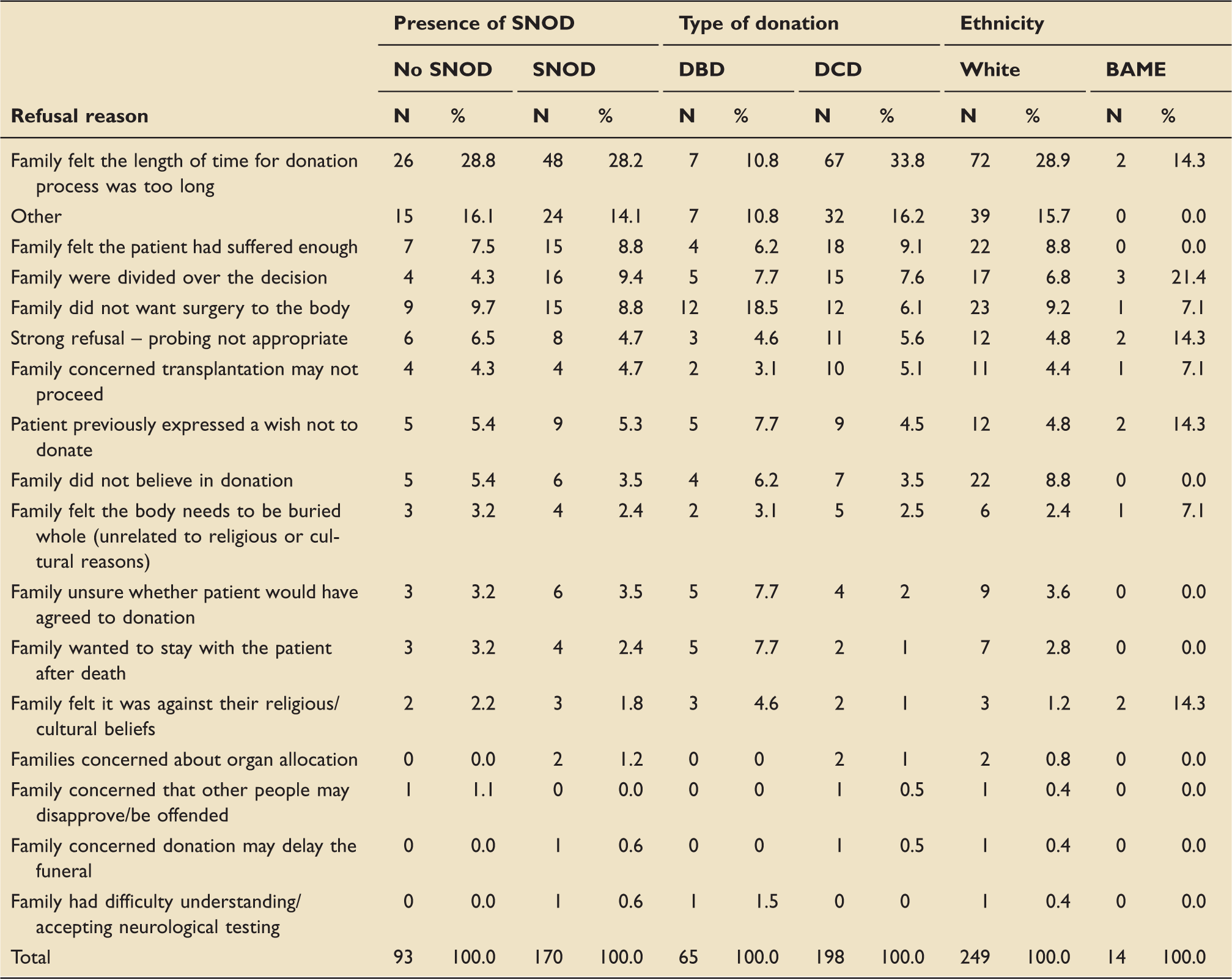
BAME: Black, Asian or Minority Ethnic; DBD: donation after brainstem death; DCD: donation after circulatory death; SNOD: Specialist Nurse for Organ Donation.
Family ODR overrides of patients approached between 1 April 2012 and 31 March 2015, by donor type and presence of SNOD.
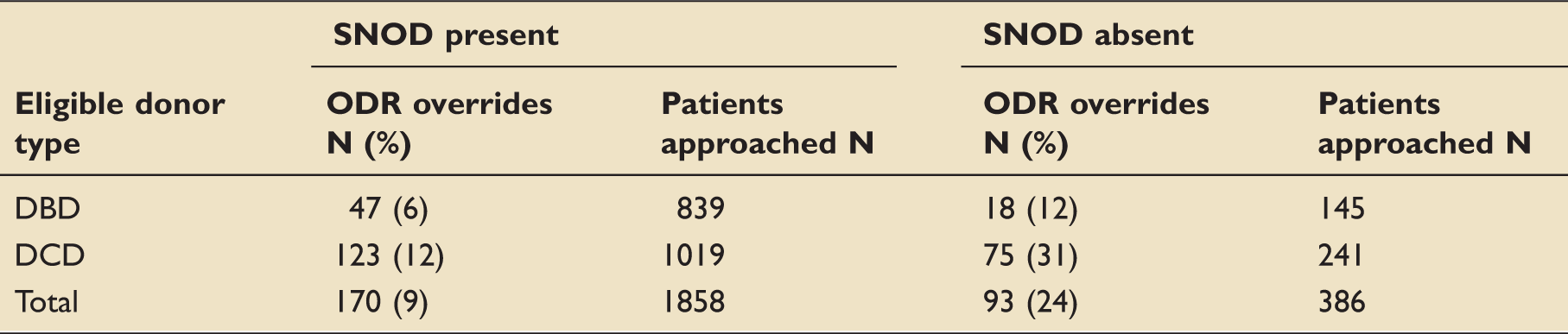
DBD: donation after brainstem death; DCD: donation after circulatory death; ODR: Organ Donor Register; SNOD: Specialist Nurse for Organ Donation.
Discussion
This study was carried out on data collected between April 2012 and March 2015 and at a time when opt-in systems of consent for organ donation were in force across the whole of the UK. In such systems, primacy is given to the views of the individual, however they might be recorded. The role of the family is to report the donation wishes of the patient to the extent they are known to them or to assume responsibility for decision-making when these views are not known. Whilst not meeting the standard of informed consent or that of an advance directive, registration on the ODR in the UK is recognised at law as legitimate first person consent. 10 Furthermore, it is of note that there is no legal provision for next of kin to override an individual’s wishes unless they can provide evidence that the individual had acted in error or had changed their views. 11 However, The Human Tissue Authority's Code of Practice does acknowledge that there may be rare circumstances where it would be inappropriate for donation to proceed. 11
Despite the apparent expectations of the law that override would be a rare event, the clinical reality as presented in this three-year analysis is somewhat different. From 1 April 2012 to 31 March 2015, 11.7% of potential donors who had registered their donation wish on the ODR had this wish overruled by their partner, relative(s) or close friend(s). Using the average conversion rates for consented deceased donors in the UK over this three-year period, 12 it is estimated that there would have been an extra 59 DBD donations and 95 DCD donations during this period. In turn, by applying the average rates of organ utilisation from these two groups of donors over this period, it is likely that more than 500 additional organ transplants could have been carried out over these three years had the individuals’ donation decisions been honoured.
Surveys of public opinion reveal some considerable resentment on the part of registered donors that families are allowed to defeat their wishes. 13 Furthermore, clinicians caring for dying patients who have made in life a decision to donate organs after their death can experience firsthand the frustration that follows on from the unwillingness of close family to support such a decision. However, and in contrast to what has occasionally occurred in other jurisdictions, 14 this has yet to result in recourse to the courts to allow a legally valid decision to be honoured. Rather, donation is stood down and the possibility of transplantation of organs and tissue lost.
It must be assumed that a donation decision recorded on the ODR is a genuine one. However, it is also fair to say that such a decision will not always be informed with personal experience of sudden and untimely loss in circumstances where donation becomes a possibility – the reality that the next of kin necessarily have to face. This brings into sharp relief the distinction between a personal decision that someone is prepared to make about their own organs and the willingness of that same person to make such a decision on behalf of a relative when the possibility is real and immediate; people are rather more likely to give in life first person consent for themselves than give consent on behalf of a dying close relative. 13 In the same way that the Human Tissue Act acknowledges that overrides may occasionally be justified, so too has the UK Donation Ethics Committee noted that there may well be occasions where the ethically correct decision is for donation not to proceed.15,16
The results of this analysis suggest that there may be more practical steps that can be taken to lessen the likelihood of family override. Families of a potential DCD donor are nearly three times more likely to obstruct first person consent than families of DBD donors and are much more likely to cite the length of the donation process as the reason for this. Concerningly, data from NHSBT reveal that the time interval between consent and treatment withdrawal in DCD has increased steadily over the last five years. 17 Whilst it may remain the case that the time to treatment withdrawal in DCD will always represent an obstacle to some families, this high rate of family override compared to DBD may also reflect the difficulties and conflicts that well-meaning families face when trying to support organ donation whilst concurrently awaiting treatment withdrawal and the death of a close relative. The perceived quality of the organs being donated and the greater certainty that donation will actually occur may further protect DBD from family overrides. There is a pressing need for all possible steps to be taken to shorten the DCD pathway and it is encouraging that NHSBT has already established interventions to address this problem.
This study also demonstrates a clear relationship between rates of family override and the involvement of SNODs when the possibility of organ donation is raised with families. SNODS – previously known as transplant co-ordinators – are employees of NHSBT and receive specific training in raising the possibility of donation with the next of kin of a potential donor. There is evidence that involvement of SNODs in the family approach is a powerful predictor of family consent 5 and this study demonstrates that their presence also reduces the likelihood of family overrides in both DBD and DCD donation. The National Institute for Clinical Excellence recommends that SNODs are involved in the family approach wherever possible, 17 although published data from NHSBT reveal that this best practice is not always the case, 18 particularly for DCD. The findings of this study show that clinicians should involve the SNOD whenever donation is being raised with a family and not conclude it unnecessary so to do when it is known that a patient has registered their wish on the ODR.
It is noted that families from BAME communities are 2.7 times more likely to override ODR registration as compared to White families. These new findings are consistent with overall rates of consent to organ donation in these groups and help to explain the problems they face when accessing transplantation. 19
Conclusion
This retrospective observational study identifies three factors significantly associated with a ‘three-fold’ increase in the likelihood of families overriding the donation decision of a relative: non-involvement of the SNOD, the type of donation being considered and the patients’ ethnicity.
It can be argued that all three factors are amenable to change, albeit from differing interventions. The evidence of relative under-representation of minority ethnic groups as organ donors highlights the need for those in a position to influence these communities to explore donation as an end of life choice. Secondly, the various agencies involved in the organ donation, retrieval and transplant pathway – surely one of the most complex healthcare pathways delivered by the NHS – need to recognise the role they have to play in shortening the duration of the DCD pathway in order to reduce the burden placed upon grieving families and the excess of family overrides that result. Finally and most readily addressed, clinical staff caring for potential donors should, in compliance with NICE guidance where this operates, make every effort to involve SNODs when donation is to be raised with families, and there is a similar responsibility for NHSBT to ensure that SNODs are readily accessible for this purpose.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.