
Abstract
Objective
Intensive care for organ preservation (ICOP) is defined as the initiation or pursuit of intensive care not to save the patient's life, but to protect and optimize organs for transplantation.
Analysis
When a patient has devastating brain injury that might progress to organ donation this can be conceptualized as evolving through four consecutive stages: (1) instability, (2) stability, (3) futility and (4) finality. ICOP might be applied at any of these stages, raising different ethical issues. Only in the stage of finality is the switch from neurointensive care to ICOP ethically justified.
Conclusion
The difference between the stages is that during instability, stability and futility the focus must be neurointensive care which seeks the patient's recovery or an accurate neurological prognostication, while finality focuses on withdrawal of life-sustaining therapy and commencement of comfort care, which may include ICOP for deceased donation.
Introduction
In deceased organ donation, the ethical divide between intensive care treatment before and after death is not always clear. Many intensive care interventions and technologies are continued unchanged or even escalated after the declaration of death. This can make the transition from the therapeutic goal of saving the patient's life to the goal of facilitating organ donation ambiguous, leading to potential or perceived conflicts of interest.
We define the initiation or pursuit of intensive care not to save the life of the patient but to protect and optimize organs for transplantation, as intensive care for organ preservation (ICOP), which may occur before, during or after the determination of death. Every organ donor in the context of donation after brain death (DBD) is managed with ICOP at some point. At the very least, ICOP is continued after death to optimize organ perfusion until organ recovery occurs. 1 Sometimes, however, ICOP is initiated and pursued before death, to allow time for brain death to develop or be confirmed.2,3 In uncontrolled donation after circulatory death programs (DCD), donation would not be possible without the use of ICOP after death, for example in situ normothermic regional perfusion. 4 This procedure is based on extra-corporeal membrane oxygenation technology, an advanced type of resuscitation technology potentially only provided to the patient after death, which raises additional ethical issues. 5 In controlled DCD, like is practised in the UK, following consent for organ donation, life-sustaining therapy is not withdrawn until the surgical organ retrieval team is available and prepared in theatre, often resulting in the use of ICOP for several hours. 6 In situ normothermic regional perfusion after death in controlled DCD is also seeing an increase. 7
In this article, we conduct a detailed ethical analysis of ICOP and we suggest criteria under which ICOP is ethically acceptable.
Definitions and terms
Neurointensive care is defined as intensive care therapy specifically applied to patients with brain injury in order to achieve the best neurological outcome. Therapies are designed to support brain recovery and decrease intracranial pressure, and usually includes mechanical ventilation and blood pressure control, but can include increasing the salt concentration in the blood stream,8,9 deep sedation 10 and intracranial pressure and oxygen monitoring. Neurointensive care is best understood as a therapeutic goal, which is to support neurologic recovery, rather than a place of treatment, as it can occur in resuscitation areas of emergency departments or small hospitals, not just in neurointensive care units.
In contrast, ICOP involves efforts to optimize organs, other than the brain, for transplantation purposes. ICOP can include the initiation or pursuit of mechanical ventilation, the use of fluids, vasopressors, drugs such as hormonal therapy, cardio-pulmonary resuscitation in case of cardiac arrest 11 or extracorporeal membrane oxygenation in case of haemodynamic instability. 12 Importantly, just as neurointensive care is best understood as a therapeutic goal, ICOP is best understood not in terms of its treatment modalities but rather in terms of its intention. If the therapeutic goal is to optimize organs for transplantation, this is ICOP.
A change from neurointensive care to ICOP may or may not lead to immediate changes to the physical care of the patient. It will, however, always impact on the intentions and goals of treatment. This should, as we will detail, lead to altered communication within the multi-disciplinary team and with the patient's family.
ICOP would not include procedures that have the primary intention to hasten death, such as cranioplasty with bandaging 13 or euthanasia, where the primary goal is death and any possible benefit for organ donation a secondary outcome.
We have avoided wherever possible terminology such as elective or non-therapeutic ventilation/intensive care as these terms have often been understood as purely the initiation of mechanical ventilation for donation purposes2,14–18 and we regard the scope of ICOP as broader.
While uncontrolled DCD can have ICOP elements as stated above, the patient population is sufficiently different (cardiac rather than brain injured) that we have not explored this issue further in this paper.
Choosing between neurointensive care and ICOP
Recommendations.
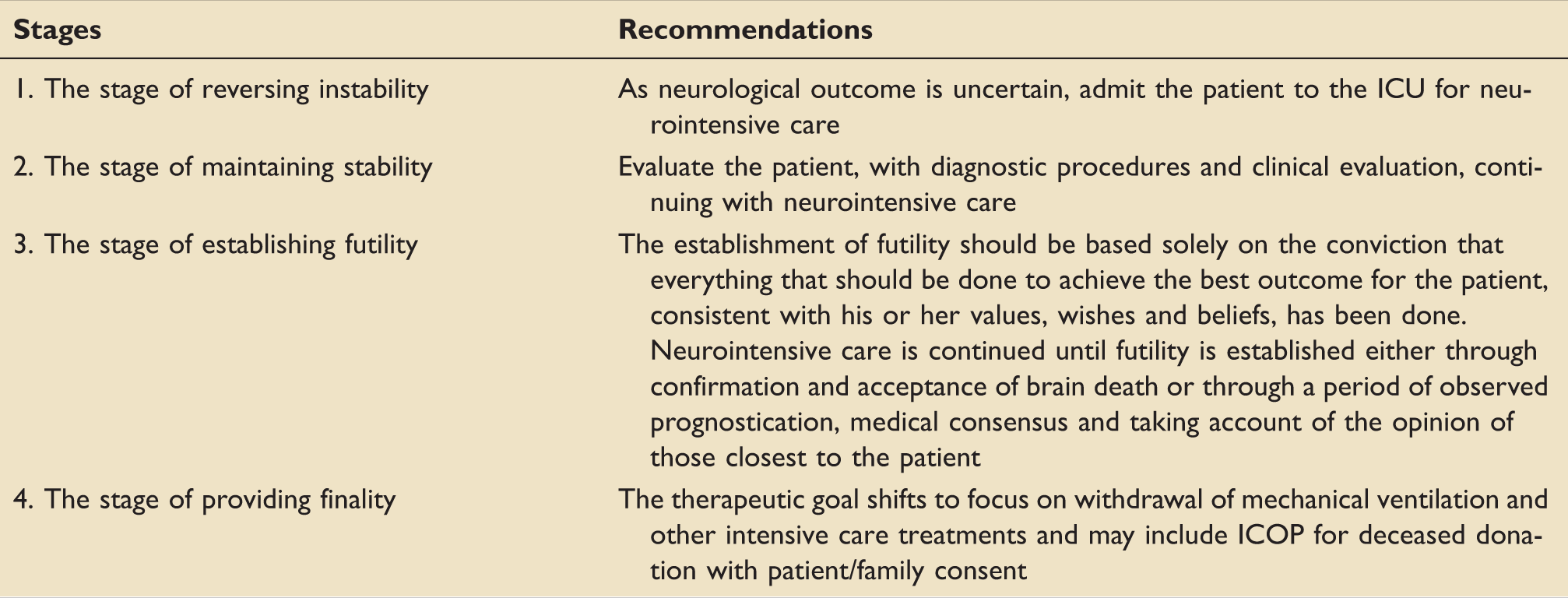
Instability
During the first stage of instability, the patient is usually unconscious, unable to breathe independently, and in dire need of life-saving procedures in order to stabilize and allow further observation over time and/or appropriate diagnostic tests or treatments. During the stage of instability, the cause of coma and prognosis may not be fully known. While initiation of ICOP during the stage of instability might be technically possible the patient's own need for survival should remain the exclusive concern for the medical team. It would be difficult for the medical team to claim that the patient could not be saved without having performed appropriate diagnostic tests and without having devoted enough time to evaluating the patient. 19
Stability
Once the patient has been stabilized by neurointensive care, often (but not always) a period of stability follows; this is usually characterized by prognostic uncertainty, with ongoing clinical investigations and observation. 20 Neurointensive care efforts at this stage will support neurological recovery, if any is possible, and simultaneously maintain organ function.
Recent guidance from the US Neurocritical Care Society has recommended maintaining physiologic stability in the early stages of patients with devastating brain injury, even when early limitation of aggressive care is being considered. The use of neurointensive care prevents unwarranted deterioration and allows for sufficient opportunity for prognostic evaluation. 21 If this recommendation is accepted, this would in and of itself preclude ICOP at the stability stage. 19 Other medical societies have made similar recommendations, for example in hypoxic cardiac arrest, 22 strongly recommending that enough time of neurointensive care is given to allow better and safer prognostication.
However, the Neurocritical Care Society also suggested that the achievement of physiologic stability at this point also allows for care planning and consideration of organ donation. This consideration of organ donation could involve ICOP.23,24
We believe that ICOP should not be commenced at this stage if there is any chance of the patient surviving in a state that would be compatible with their values, wishes and beliefs. Instead, efforts should remain focused on attempting to save the patient's life and improving future neurological functioning by use of appropriate neurointensive care. To achieve such prognostic certainty a period of stability allowing observed prognostication over time will be required. This should be the default therapy of choice, unless the patient has additional co-morbidities that make intensive care non-beneficial or therapy is against the patient's wishes.
Futility
We are aware there is a movement away from the use of the term futility. 25 However, it is a commonly used word in intensive care to describe a patient's journey. When there is a belief that continuing neurointensive care may offer no prognostic benefit for the patient, we consider that the stage of futility has commenced. Establishing futility is usually part of a process rather than an event and remains one of the hardest areas in neurointensive care. After a careful medical evaluation, futility can be established based on neurological prognosis and family input on the patient's values wishes and beliefs. The establishment and acceptance of futility is the final end point of this stage.
Futility should be based solely on the conviction that everything that should be done to achieve the best outcome for the patient, consistent with his or her values, wishes and beliefs, has been done. 26 When necessary, multiple disciplines can be brought to bear to assist the intensive care physicians, including neurologists, neurosurgeons and radiologists and, if making any decision regarding quality of future life, involve any advanced expressed wishes and those family and friends closest to the patient.
In patients with devastating brain injury, the establishment of futility may occur either by confirmation of brain death or through a period of observed prognostication, medical consensus and taking account of the opinion of those closest to the patient. During this stage, clinicians may stop some neurointensive care therapies but continue standard intensive care. For example, cessation of sedation and the acceptance that physiological targets typically pursued during neurointensive care (e.g. intrancranial pressure control) may not be achievable. This is done to allow clinicians to accurately establish the neurological prognosis and confirm or refute futility.
Diagnosing death using neurological criteria (brain death) can be considered the gold standard for futility. Establishing if a patient is alive or dead is of benefit to the family, hospital staff and society, because it eradicates doubt.27,28 We do not consider the use of neurointensive care to achieve the diagnostic certainty of brain death as ICOP, if it is done to confirm prognostication.
Scenarios related to brain death diagnosis and confirmation.
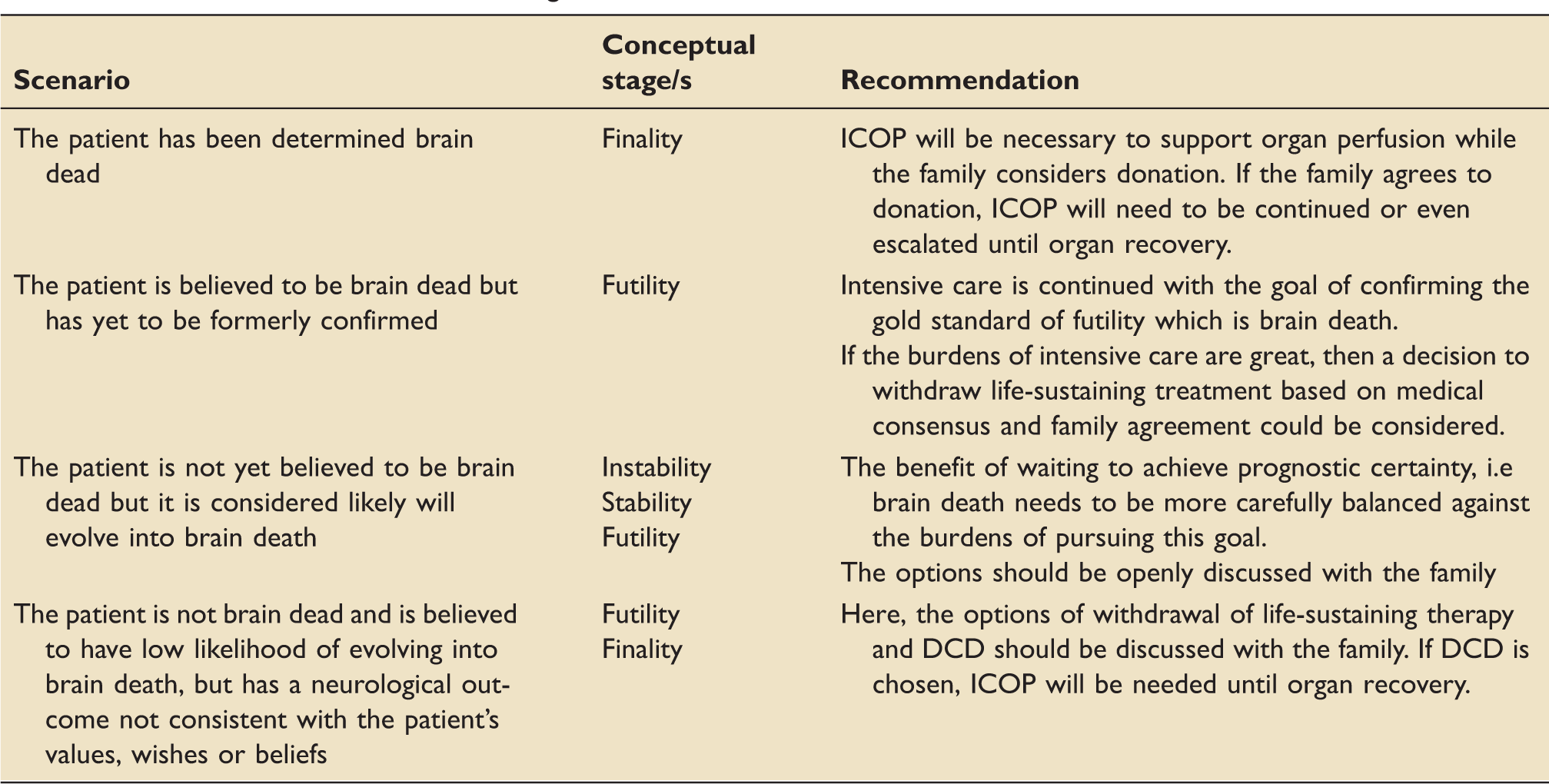
Without the specificity achieved through a diagnosis of brain death there is always an element of uncertainty in prognostication. It is well recognized that a small percentage of intensive care patients who have their life-sustaining treatment withdrawn will not die but will be discharged alive. 29 The risk of harm for the patient who is incorrectly assessed as futile is therefore considerable, as it may ‘deny patients with survivable injuries the chance of recovery’. 30 This risk can be exacerbated by prematurely declaring futility during the instability and stability phases. 31
If futility is established either through confirmation and acceptance of brain death or through a period of observed prognostication, medical consensus and taking account of the opinion of those closest to the patient, then the finality stage can be commenced.
Finality
The finality stage can include the care of a living or deceased patient. In living patients, this is the time for end of life care and for deceased patients the time for post-mortem care. This stage includes, but is not limited to, the options of withdrawal of life-sustaining therapy (WLST), DCD or DBD. 26
It is only now that ICOP, in the finality stage, can be appropriately considered and discussed with the patient's family. If the patient is a consented organ donor (e.g. is on an Organ Donor Register) and/or if the family agree to organ donation, ICOP has commenced.
Switching from neurointensive care to ICOP without having first disclosed the reasons and implications of the switch to the family denies them the opportunity to bring information regarding the values, wishes and beliefs of the patient to the decision-making process. Communication and transparency is particularly crucial as the switch from neurointensive care to ICOP might not be noticeable by the family at the bedside. This period remains a delicate time of communication between the medical team and the family where end of life options have to be transparently discussed. 30
Discussion and recommendations
Notwithstanding issues of accurate prognostication, some patients may have ICOP initiated very early in their hospital admission, even before receiving any neurointensive care. One example is elective ventilation, where intubation and ventilation is performed for the express purpose of facilitating donation. After an intense debate on elective or non-therapeutic ventilation in the 1990s,2,3,14–16 the UK Department of Health guidance was that, ‘where the clinician's intention in referring the patient to intensive care is not for the patient's own benefit but is to ensure his or her organs can be retrieved for transplantation the practice would be unlawful’. 32 Recently, the UK Donation Ethics Committee has stated that, ‘the legal context has changed so dramatically since 1994 that the legal advice generated in that different era is no longer reliable’. 33 There is now some recognition in the UK that a desire to donate can give authority for clinicians to take actions to facilitate donation. While we do not reject this line of defence for elective ventilation, we see a potential risk that not enough will have been done to ensure accurate prognostication and would caution against policies encouraging elective ventilation before the stage of finality outside unique case by case circumstances. 34
In Switzerland, ICOP is acceptable if it has been established that the patient wanted to be an organ donor (either by first-person consent or surrogate consent), that a WLST has been decided and that there is a high probability that death will occur.
35
The Australian and New Zealand Intensive Care Society (ANZICS
20
) has stated that if the intensivist recommends that treatment be withdrawn and the family accepts and agrees with this, it may also be appropriate to discuss the possibility of maintaining physiological support for some hours, to provide time to discuss and consider organ donation (DCD or DBD), or to allow the patient to deteriorate to brain death. (p. 36)
We interpret these recommendations as saying that achieving agreement on futility is a process and that continuing neurointensive care at this stage is acceptable as this helps achieve this decision end point. This should not be considered ICOP. However, once the futility stage is concluded the finality stage commences. This transition can occur quite quickly and even be part of the same family discussion. ICOP is appropriate here while options in the finality stage are explored.
The key difference between the stages is that during the instability, stability and futility stages the focus must be neurointensive care which seeks the patient's recovery or achieving accurate neurological prognostication. Only in the finality stage should the therapeutic goal shift to focus on comfort care, the withdrawal of mechanical ventilation and other intensive care treatments for ICOP for deceased donation.
During the four stages, there is an additional risk of real or perceived conflicts of interest. This is a powerful reminder why a conclusion of futility should not be biased by organ donation considerations and why initiation of ICOP should not be considered during the instability, stability or futility stages but only in the finality stage, to avoid denying, or be perceived to be denying, neurointensive care to a saveable patient. By conceptualizing neurologically injured patient care using the four stages, as we have outlined in this paper, clinicians can better avoid real or perceived conflicts of interest. We consider that pursuing and maintaining trustworthiness, through transparent policies and shared decision making in each of the four stages, is the best way to mitigate these potential conflicts.
We would also recommend that a change in management, from neurointensive care to ICOP, should be documented in the patient's chart, after a discussion and an agreement with the family, in order for any healthcare professionals taking care of the patient to be fully aware of the goals and intentions of treatment.
Conclusion
The switch from neurointensive care to ICOP carries a risk of denying treatment to a patient that will benefit from it. We have suggested that the care of a patient with a devastating brain injury that eventuates in deceased donation can be conceptually understood as proceeding through four stages: instability, stability, futility and finality. During the first three stages, the focus must be neurointensive care which seeks the patient's recovery or achieving accurate neurological prognostication. Only in the finality stage should the therapeutic goal shift to ICOP if organ donation is consented.
Our hope is that clinicians who conceptualize neurologically injured patient care in the four stages, we have outlined in this paper, will be better able to navigate the ethical challenges in this fraught area of clinical practice, which may otherwise defeat the good intentions of all involved.
Footnotes
Disclaimer
The opinions expressed are the views of the authors and do not reflect the policy of their belonging institutions, NHS Blood and Transplant, the Swiss National Medical Associations or the Swiss Public Health Service.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dale Gardiner is national clinical lead for organ donation in the UK for NHS Blood and Transplant.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.