
Abstract
Clinical specialist physiotherapists from the five severe respiratory failure centres in England where respiratory extracorporeal membrane oxygenation (ECMO) is practiced have established this consensus agreement for physiotherapy best practice. The severe respiratory failure centres are Wythenshawe Hospital, Manchester; Glenfield Hospital, Leicester; Papworth Hospital, Cambridge; Guy’s and St Thomas’ Hospital, London and The Royal Brompton Hospital, London. Although research into physiotherapy and ECMO is increasing, there is not a sufficient amount to write evidence-based guidelines; hence the development of a consensus document, using knowledge and experience of the specialist physiotherapists working with patients receiving ECMO. The document outlines safety aspects, practicalities and additional treatment considerations for physiotherapists conducting respiratory care and physical rehabilitation.
Keywords
Introduction
Veno-venous extracorporeal membrane oxygenation (VV ECMO) support for patients with severe respiratory failure is commissioned by NHS England at five Trusts in England. The service manages patients throughout England and the wider United Kingdom (UK) if they have acute severe respiratory failure with an underlying reversible cause and a Murray score of 3 or more. The Murray score is used to characterise the severity of lung injury, scored on a range from 0 to 4 in each category, which are: number of quadrants with consolidation on chest X-ray, hypoxaemia (PaO2/FiO2), positive end expiratory pressure (PEEP) and lung compliance. 1 Patients are retrieved from other hospitals to the regional centre, either on conventional ventilation or on mobile ECMO and remain under the care of the ECMO specialist service for 48 h (or until stable) following decannulation from ECMO. Patients are subsequently repatriated to their referring hospitals, though the timing varies between patients and centres. 2
Whilst at the specialist severe respiratory failure centre for ECMO, patients may receive respiratory and rehabilitative physiotherapy. Whilst the provision of physiotherapy service is variable within the UK and worldwide, evidence supporting physiotherapy and ECMO is increasing,3,4 as is the awareness of the importance of physiotherapy and rehabilitation within ICU. 5 Respiratory physiotherapy can reduce ventilator-associated pneumonia, improve static lung compliance, enhance sputum clearance and address atelectasis and lobar collapse.6–9 However, it should be noted that these studies are not based on patients on ECMO. The timing of these treatments depends on the stage of acute respiratory distress syndrome (ARDS) and clinical indication. The evidence regarding respiratory physiotherapy during VV ECMO is limited to two case studies describing the use of ventilator hyperinflation and manual techniques in an ECMO patient with ultra-protective lung ventilation.3,10,11 There are also single centre studies reviewing the treatment options used in respiratory physiotherapy which highlights the variability between ECMO centres as to how respiratory physiotherapy is provided to ECMO patients.12,13
Rehabilitation on ICU has been shown to be safe and that early intervention results in decreased episodes of delirium, decreased duration of mechanical ventilation, decreased ICU and hospital lengths of stay, improved functional ability and improved mortality.14–18 The growing use of ECMO for patients with severe respiratory failure raises challenges for physiotherapy and rehabilitation. 19 The ECMO patient cohort is a particularly difficult group with a mixed aetiology of respiratory failure including pre/post lung transplant, trauma and pneumonia. Historically, patients on ECMO are heavily sedated with prolonged bed rest, and exposure to muscle relaxants and corticosteroids, which puts them at high risk of physical disability. In addition to this, attachments such as ECMO cannulae may limit treatment options, dependent on insertion location. Despite this, it seems reasonable that the benefits of early rehabilitation seen in the general ICU population apply to patients receiving ECMO. However, it should be noted that even with early rehabilitation, patient who survive ARDS and those whose survive ARDS with ECMO support have a reduced health related quality of life at a one-year follow-up.20–21 There is an increasing number of patients awake on ECMO, therefore reducing the negative effects of sedation.3,22 This expedites the ability to participate in rehabilitation and liberation from ventilation, however the effect of increased work of breathing and patient anxiety needs to be considered.23–25
National care standards for rehabilitation within ICU are relevant and should be applied to patients receiving ECMO. Therefore, these patients should receive assessment for risk of physical and non-physical morbidity, assessment of rehabilitation needs within 24 h of admission, active therapy to enable them to achieve their goals, and the use of outcome measures.26–28 Rehabilitation on ECMO requires a careful, multi-disciplinary approach, including involvement of staff with experience of moving patients on ECMO.3,4,22
ECMO multi-disciplinary team
The ECMO team consists of senior staff from different specialities to provide input into operational planning, service development, peer review and specialist clinical support. The core team will differ between centres, but usually consists of:
Intensive care consultant/ ECMO consultant ECMO co-ordinator ECMO trained specialist nurse Perfusionist Senior nurse in charge Senior ICU specialist physiotherapist
Key consideration for safety during treatment
Patients on ECMO have one or more large cannulae in central veins (femoral or jugular) to allow the continuous flow of up to 6 L/min of blood per cannulae through the ECMO circuit. A disturbance to that flow or episode of unplanned decannulation is potentially life-threatening due to the risk of severe hypoxaemia. 3 Studies report mobilising patients receiving ECMO as a bridge to lung transplant or bridge to recovery. These studies have involved small patient numbers, however this process appears to be safe and show good functional outcome for patients.29–33 A systematic review of nine reports and 52 patients in total also found that although considered a high-risk procedure, passive and active physiotherapy was safe when undertaken with a highly specialised team. 3 There have been no reported significant adverse events during rehabilitation on ECMO, however it should be acknowledged that these reports are from highly expert teams.
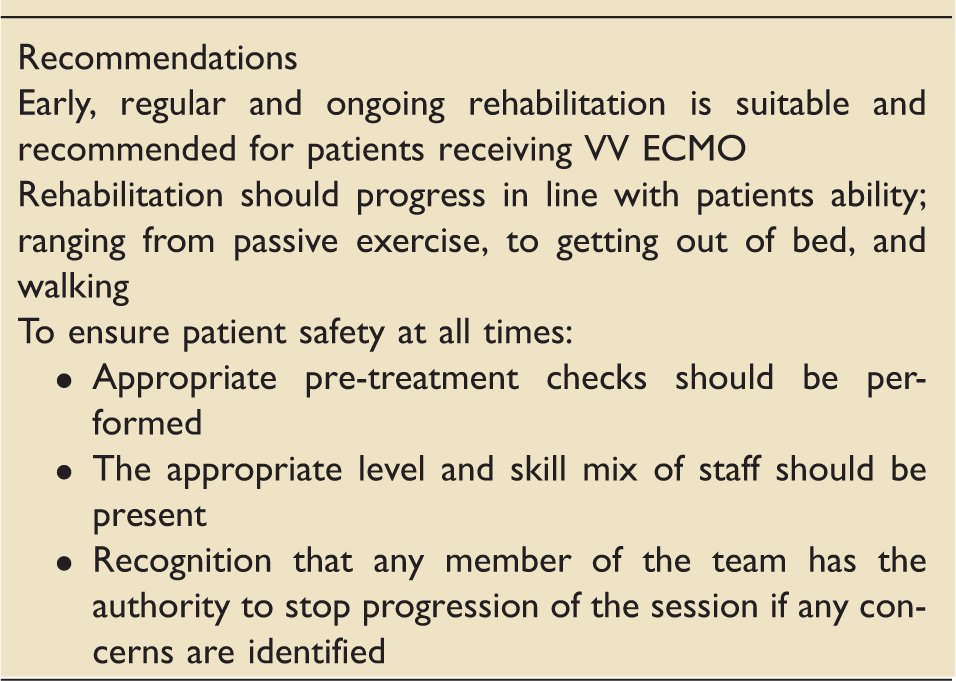
There are currently no national established guidelines or protocols for mobilising patients on ECMO, therefore practice regarding mobilisation and rehabilitation is likely to vary widely between institutions. There are also no national established guidelines or protocols for respiratory physiotherapy treatment for patients on ECMO. Given the relative lack of evidence, the severe respiratory failure centres who provide ECMO in England have formed a specialist physiotherapy group to provide expert consensus and recommendations for the physiotherapy treatment of VV ECMO patients within the ICU. The group present key recommendations within this document, but at present, evidence is lacking to provide standards of care.
Preparation for physiotherapy
Refer Figure 1.
Preparation for physiotherapy: seven steps flow chart.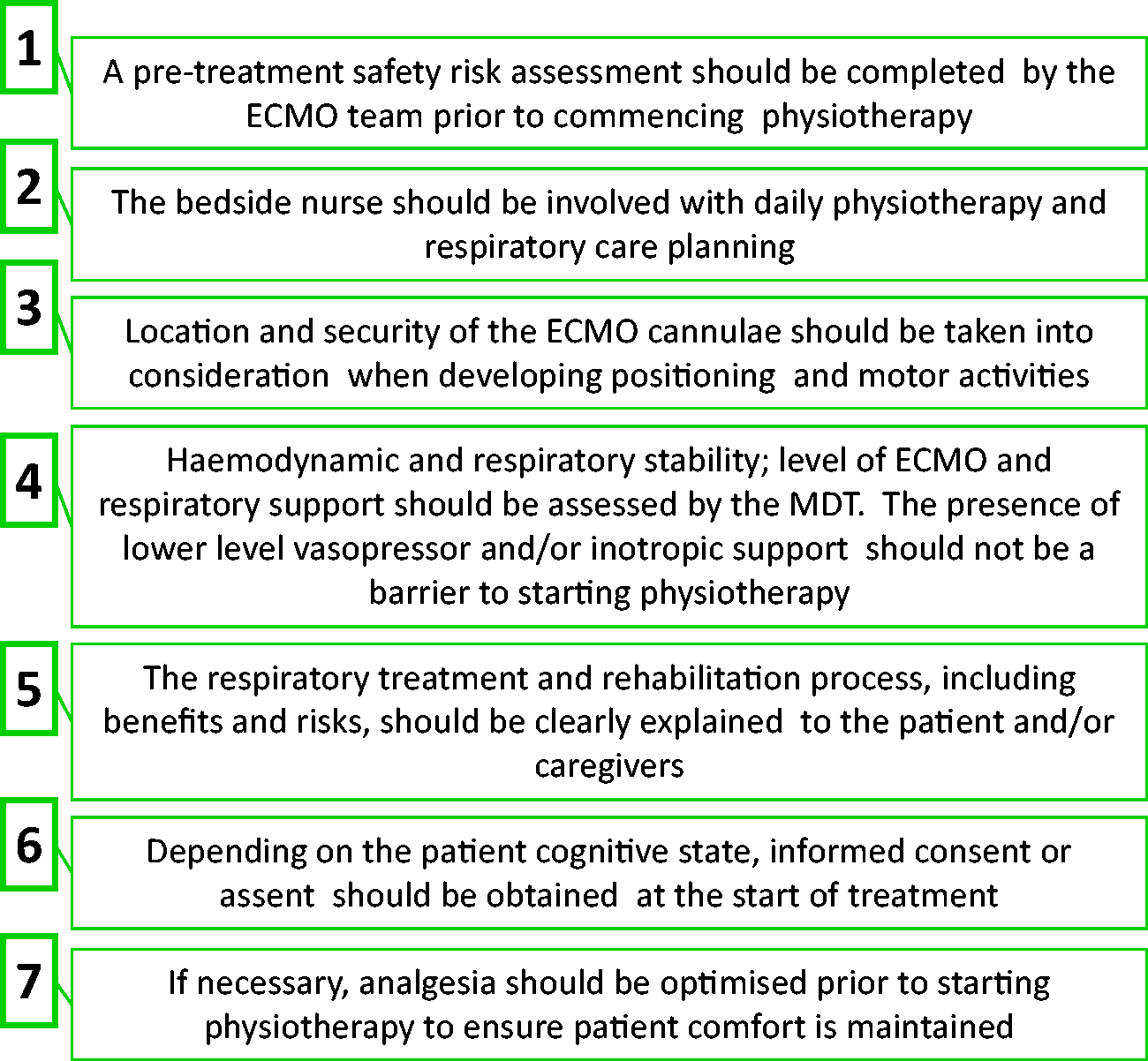
Physical rehabilitation
Rationale for rehabilitation:
Prevention of bed rest-related problems Optimise early recovery Improve functional ability as quickly as possible Improve mood and psychology with engagement in goal setting and attainment
Pre-treatment safety
Pre-treatment safety issues on VV ECMO patients.
Patient monitoring
The patient should be connected to vital signs monitoring throughout the rehabilitation session. The level of monitoring required, including parameters, will be agreed at an institutional level by the ECMO team taking into consideration the individual patient. Baseline observations should be observed and documented prior to commencing exercise. Any changes in blood pressure, heart rate, peripheral haemoglobin oxygen saturation or ECMO flows should be noted and responded to appropriately. The rehabilitation session should be terminated and the patient returned to bed if there is an adverse change in observations that do not respond to basic intervention such as an increase in FiO2. Patients may require additional mechanical ventilation or ECMO support to perform rehabilitation due to increased cardiac output, oxygen consumption and carbon dioxide production during the physical activity. Patients with minimal native lung function (for example; tidal volumes <200 mL, or no change in PaO2 with an increase in Fio2 to 1.0 for 30 min to assess contribution of lungs to gas exchange) may require increased ECMO blood flow during the rehabilitation activity. Patients with recovering lung function (for example; tidal volumes >200 mL and incremental change in Pa02 following increase in Fio2 to 1.0) may require increased Fi02 via the ventilator and/or increased ECMO blood flow during the rehabilitation activity. Fluid boluses may be required to avoid complications related to changes to ECMO flow settings. Any and all changes to ECMO support required during rehabilitation should be performed by a qualified ECMO specialist. Patients should be monitored after exercise has finished for any delayed adverse response to exercise. During treatment, staff should be conscious of the risk of bleeding from cannulation sites, movement of cannulae and reduction in blood flow due to position changes. If patients complain of pain on movement following the removal of cannulae the site should be investigated as a haematoma may be present around the insertion point.
Roles and responsibilities
Minimum staffing:
^ At least two members of the physiotherapy team for rehabilitation session involving moving the patient. The lead physiotherapist should be senior, with ECMO rehabilitation experience and competence. The appropriate number of physiotherapy staff and skill mix may change dependent on the rehabilitation task planned. ^ ECMO specialist nurse; perfusionist or duty ECMO coordinator for ECMO cannulae safety. ^ Suitably trained staff for other lines and airway management. Additional members of staff may be required if the patient require more assistance with moving and handling or to monitor lines and equipment. Medical staff; ECMO specialist nurse; duty ECMO consultant or duty ECMO co-ordinator will be responsible for securing the ECMO cannulae prior to commencing rehabilitation. Adequate length of tubing to allow movement must be assessed prior to movement. They will also be responsible for monitoring the cannulae throughout the rehabilitation session and securing them on movement. The physiotherapists will be responsible for leading the rehabilitation session ensuring patient safety throughout the session. The therapy team involved must be deemed competent by the ICU physiotherapy lead according to locally agreed competencies and criteria. Suitably competent nursing staff or perfusionists will be responsible for monitoring ECMO flows and the circuit throughout the session and assisting with rehabilitation as required. The patient’s airway, observations and response to the treatment session will be monitored throughout the session with all team members being aware of alarms and airway safety. Any member of the team has the responsibility and authority to stop progression of the session if any concerns are identified. In the event of an adverse incident occurring during physiotherapy, if it is not possible to return the patient safely to bed, they should be safely lowered to the floor to allow any emergency care to be provided. Appropriate incident reporting should be completed in the event of an adverse incident.
Rehabilitation protocol
The following illustration provides a suggested progression for rehabilitation with patients who are awake on VV ECMO (Figure 2).
VV ECMO rehabilitation protocol: five steps flow chart.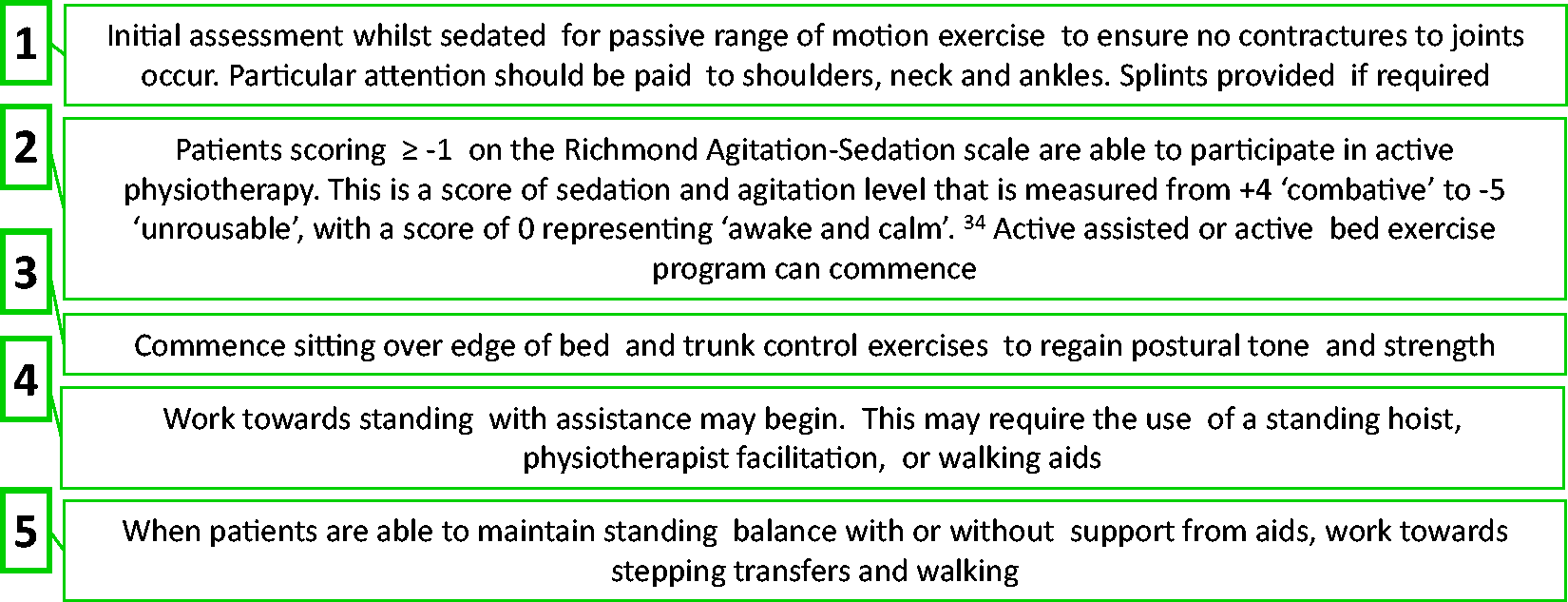
Throughout this process, patient progress will be continually monitored and treatment sessions adapted accordingly. If there are periods of medical instability during the rehabilitation phase it may be necessary to halt rehabilitation sessions for a period of time, or to return to earlier stages of the rehabilitation pathway as required.
Rehabilitation treatment options and equipment
In addition to rehabilitation treatment techniques’ outlines above (limb exercises, sitting over edge of bed, standing, and stepping transfers) other rehabilitation techniques and equipment can be used.
Rehabilitation equipment for moving and handling safety for both patients and staff should be used as appropriate, e.g. standing frames, zimmer frames, tilt table. For more debilitated patients with poor lower limb function, a bed bike can be used, with progression onto chair pedals for patients able to sit out of bed. The bed and chair pedals treatment modalities can be passive, or involve active participation and can be used as an adjunct for specific lower limbs muscle strengthen and general range of movement. If patients are able to sit out of bed, a chair with an appropriate level of support for the patient’s trunk strength and pressure care needs must be provided. Appropriate seating must be used to allow reclining, or patient transfer board/hoisting back to bed in an emergency. For physically able patients, upright cycle and walking around ICU is possible with appropriately trained staff.
Assessing outcome
In adherence with D16 standards
27
and NICE guidance CG83
28
a short clinical assessment should be undertaken on admission to identify patients at risk of physical and non-physical morbidity. A comprehensive clinical assessment should then be performed on admission and before discharge. Once patients commence rehabilitation, appropriate goals should be set with patients and their family in order to target therapy to the individual. These goals can then be used to assess achievement of rehabilitation targets. Patient’s progress and response to rehabilitation should be regularly assessed by a qualified practitioner; this is often the physiotherapist. Progress should be assessed at least weekly, but more often if the patient’s status changes significantly. Using a multi-disciplinary approach, patients should be assessed using a validated rehabilitation outcome measure on commencement of rehabilitation and discharge from the ICU.
26
The following are used within the UK ECMO centres: The Chelsea Critical Care Physical Assessment Tool,
35
Functional Independence Measure/Functional Assessment Measure,
36
Physical Function ICU Test
37
and Manchester mobility score.
38
Variability exists with the use of outcome measures, as at present there is not a ‘gold standard’ outcome measure to assess physical ability within ICU.
39
The rehabilitation plan and outcome measure should be provided as part of the handover to other hospitals following repatriation or on ward transfer.
Other therapy input
Involvement of occupational therapy, speech and language therapy, psychological support and dieticians should be considered early, dependent on resources within the centre. Post discharge support from ECMO follow-up clinics is also required to address physical impairment, psychological stress and emotional support for the patient and their families and carers. 40
Respiratory treatment
Rationale for respiratory treatment:
To optimise clearance of secretions from airways Improve ventilation in the presence of atelectasis/ collapse Maximise ventilation/perfusion potential
Dependent on local policy ECMO patients may be assessed for respiratory treatment on admission or on referral. If assessment is required, this should be performed by a suitably qualified physiotherapist in a timely fashion. Local protocol and clinical need will dictate frequency of further intervention. The majority of ECMO patients will be ventilated; however, some may be self-ventilating via a tracheostomy or without an artificial airway.
Prior to respiratory treatment
A full respiratory assessment should be conducted, this should include: ECMO settings, ventilation mode, flow curves and compliance, arterial blood gases, oxygenation saturation, auscultation, observation and palpation of the chest wall movement and fremitus, review of chest X-ray or CT scan. In cases of significantly reduced tidal volumes due to ultra-protective ventilation or poor compliance some assessment techniques will be of limited use, however this will become more useful with lung recovery and an increase in lung volume.
In addition to a respiratory assessment and review of the preparation for physiotherapy flow chart (Figure 1) the following should also be considered in more depth:
Assessment of lung compliance should be performed if appropriate for patients who are ventilated. Lung compliance is often calculated by the ventilator and can be read off the monitor screen, or calculated using the following formulas: ^ Dynamic compliance:
Exhaled tidal volume
cm H2O peak inspiration pressure – PEEP
^ Static compliance:
Exhaled tidal volume
cm H20 plateau pressure – PEEP
Recent radiological imaging should be reviewed prior to treatment to assess for changes within the lung fields and position of the ECMO cannulae. The level of sedation/ neuromuscular blocking agents should be considered as part of the assessment/ treatment planning. Locally agreed respiratory personal protective equipment precautions should be adhered to during respiratory treatment due to the generation of aerosolised particles.
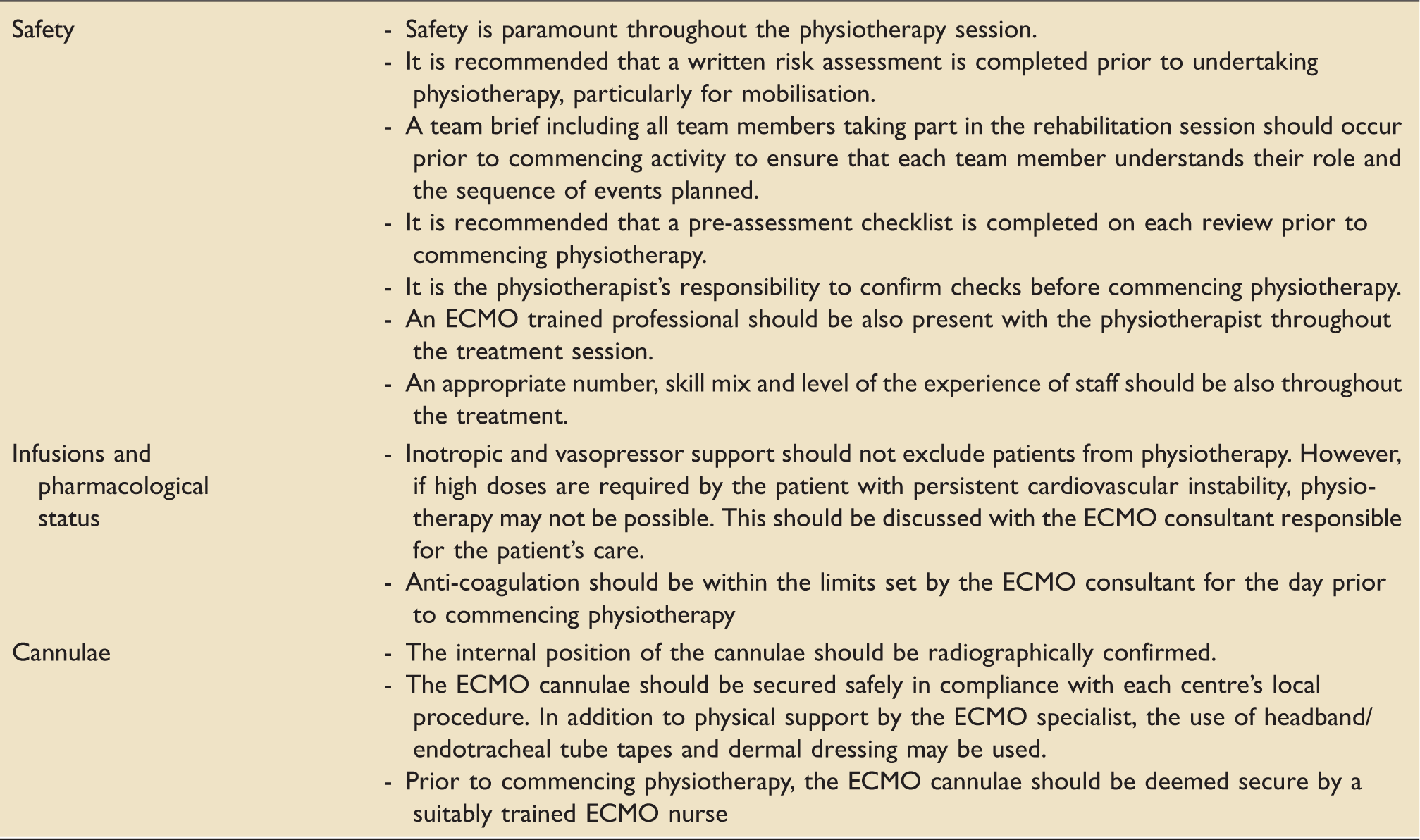
Safety
Safety considerations are outlined in Table 1.
Respiratory treatment options
The full range of treatment options should be considered for ECMO patients requiring respiratory intervention. However, additional consideration may be required due to cannulation sites, lung pathology, stage of lung recovery and compliance, anti-coagulation level and effect on ECMO flows.
Before breaking the ventilator circuit or aerosolising respiratory generated particles consider the risks to the patient and staff, and use infection control precautions required.
Precautions and recommendations for respiratory interventions on VV ECMO patients.
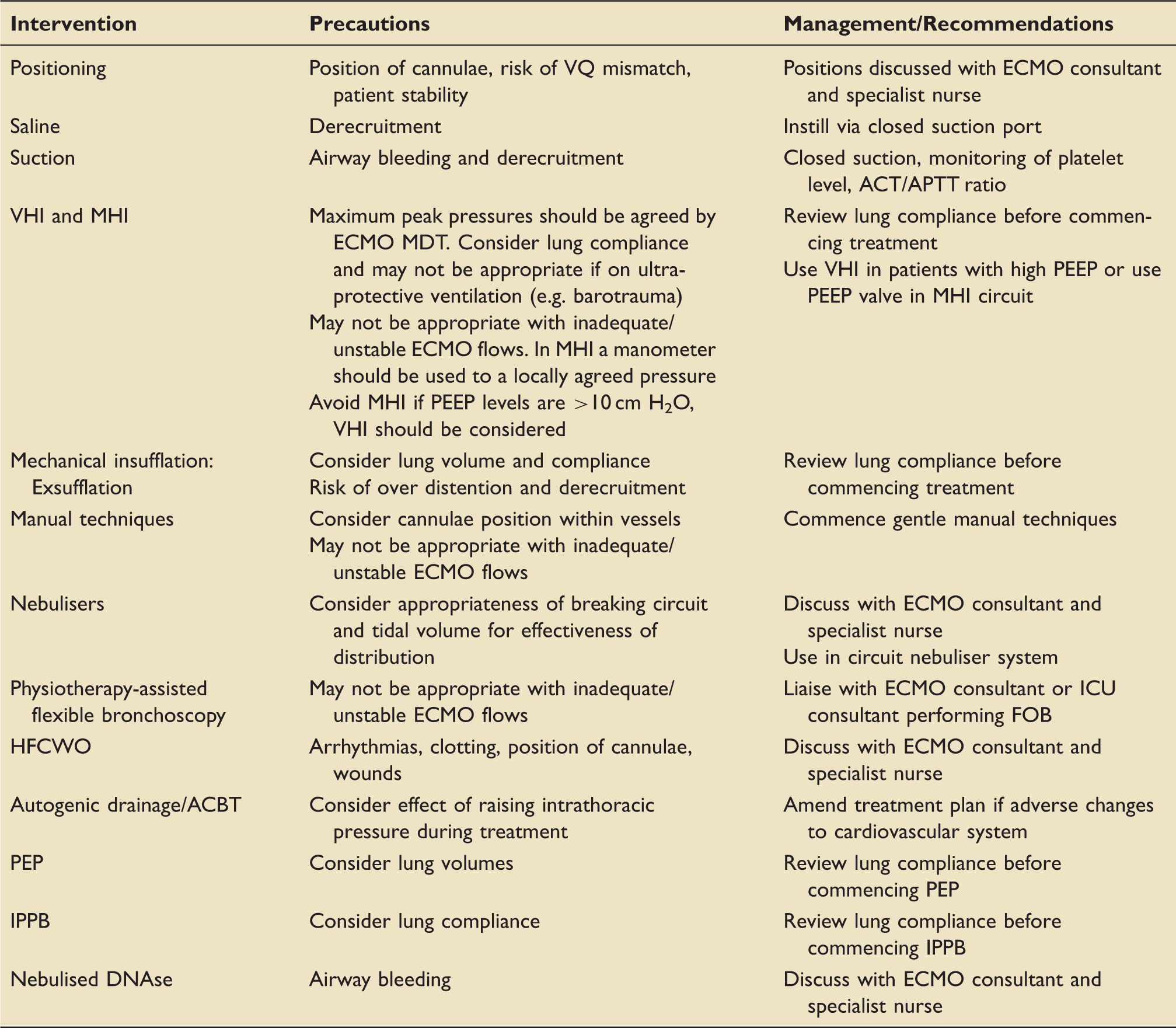
VQ: ventilation-perfusion; ACT/APTT: activated clotting time/activated partial thromboplastin time; VHI: ventilator hyperinflation; MHI: manual hyperinflation; MDT: multi-disciplinary team; PEEP: positive end-expiratory pressure; ICU: intensive care unit; FOB: fibreoptic bronchoscopy; HFCWO: high frequency chest wall oscillation; ACBT: active cycle of breathing techniques; PEP: positive expiratory pressure; IPPB: intermittent positive pressure breathing; DNase: deoxyribonuclease.
Keypoints
Physiotherapist should be involved with patients receiving ECMO from admission: for assessment, respiratory treatment and rehabilitation treatment. The likelihood of adverse events during treatment can be reduced by using a highly specialised team with each team member assigned specific roles. Safety during treatment is paramount; safety checks pre, during and post treatment are essential. Current evidence supports rehabilitation in awake patients on VV ECMO. There is limited evidence on respiratory intervention.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics
This consensus document has been approved and endorsed by the Association of Chartered Physiotherapists in Respiratory Care (ACPRC) committee.