
Abstract
Introduction:
Lung ultrasound (LUS) is an emerging assessment tool for intensive care unit (ICU) therapists (physiotherapists, physical therapists and respiratory therapists) to aid pathology identification, intervention selection, clinical reasoning and as an outcome measure to assess intervention efficacy. However, the extent of LUS adoption and use by ICU therapists internationally has not been described in the literature.
Objectives:
This survey explored the interest in LUS amongst ICU therapists internationally. In addition, LUS training, use in clinical practice and barriers to implementation were also explored. The survey findings were used to facilitate recommendations for future adoption.
Methods:
International ICU therapists were invited to answer a 37 question cross-sectional open e-survey, distributed using the online survey tool REDCap®. The exact sample size of eligible ICU therapists from around the world is unknown, therefore the participant responses received were a representative convenience sample of the international ICU therapist population. Survey links were posted on the relevant web pages and social media forums utilised by various ICU therapist associations and professional organisations worldwide. A snowballing technique was used to encourage survey participants to forward the survey link within their professional networks. The survey was open on REDCap® for an 8-week period between March and May 2021.
Results:
Three hundred twenty ICU therapists from 30 countries responded with most respondents coming from either the United Kingdom (n = 94) or Australia (n = 87). Eighty-nine of the ICU therapist respondents (30%) reported being users of LUS, however, 40 of those 89 respondents reported having no formal accreditation. The top clinical indications to perform a LUS scan were changes on chest radiograph, altered findings on auscultation and a low partial pressure of arterial oxygen/fraction of inspired oxygen ratio. The 71% of LUS users reported that their ICU does not have a local policy in place to guide ICU therapists’ use of LUS. Most LUS users (82%) only document their LUS findings in the patient’s medical notes and (73%) only store the LUS clips on the ICU’s ultrasound machine. The 85% of respondents perceive LUS becoming an increasing part of their objective assessment in the future and 96% report that they have other ICU therapist colleagues interested in adopting LUS. Main reasons why respondents believe that ICU therapists are not adopting LUS in their ICU are a difficulty in access to appropriate training, mentorship, and a lack of local governance policy guiding their use of LUS.
Conclusions:
To the authors’ knowledge this is the first study to explore the international adoption and utility of LUS by ICU therapists. LUS is a growing technique with widespread interest from ICU therapists internationally with a desire to adopt LUS into their assessments and upskill their practice. ICU therapists’ use of LUS could allow more targetted and appropriate treatment for patients on ICU. Barriers to LUS adoption could be mitigated by having access to quality training programmes and mentorship. Development of profession specific guidance and policies within local infrastructure should facilitate growth and ensure robust quality assurance and governance processes.
Introduction
Lung ultrasound (LUS) is an emerging assessment tool for therapists (physiotherapists, physical therapists, and respiratory therapists) working in an intensive care unit (ICU) to aid pathology identification, intervention selection, clinical reasoning and as an outcome measure to assess intervention efficacy.1,2 Lung ultrasound has been proven to have significantly greater accuracy compared to chest radiograph (CXR) in identifying pleural effusion, consolidation, interstitial syndrome, and pneumothorax.3,4 The ability of ICU therapists to differentiate between the cause(s) of hypoxaemia or increased work of breathing in respiratory compromised patients should enhance patient care, reduce the adverse outcomes of prolonged mechanical ventilation and reduce ICU stay.5,6
Despite increasing evidence that LUS has the potential to improve patient care in many clinical areas,3–6 the extent of LUS uptake and use by ICU therapists internationally has not been described in the literature. Anecdotal experiences appear to vary widely between global regions, countries and individual intensive care units depending on local practice and the resources available. Beyond the United Kingdom (U.K.) and Australia,1,7,8 it is also unknown what barriers ICU therapists experience in the uptake of LUS.
The purpose of this survey is to explore how widespread the interest in LUS is amongst ICU therapists. The training, adoption and use in clinical practice was explored alongside the barriers to LUS implementation. The implications from the survey findings may assist to facilitate the recommendations for future adoption of LUS by ICU therapists.
Methods
Survey design and survey development
The authors formulated a 37-question cross-sectional open e-survey consisting of multiple-choice responses. The e-survey consisted of three main sections with 11–12 questions in each section, totalling four screens including the cover letter. There was no randomisation of the questions or surveyed items. Adaptive questioning was used; certain follow up questions would only appear if the respondents answered with a relevant response. Respondents had the ability to suggest additional comments by selecting ‘other’ which opened a free-text box.
The survey questions covered the following topics:
The demographics of the ICU therapists surveyed
The ICU therapist’s practice around the use of LUS
The ICU’s practice around the use of LUS
The ICU therapist’s implementation of LUS
Survey pilot
The usability, flow and technical functionality of the e-survey link was piloted by the ICU and Physiotherapy professionals which consisted of an ICU consultant, an ICU nurse unit manager, a physiotherapy head of department and one other senior physiotherapist who work in a general metropolitan hospital. They all had nil to novice knowledge of physiotherapy LUS. These functionalities were also supported by an IT technician. The e-survey was piloted on three occasions during the development phase.
The authors hypothesised that the popularity of LUS among ICU therapists was higher in the U.K. or Australia, followed by the United States of America. Hence, the authors believed the demographics between the expected participants to be similar.
The pilot feedback from the ICU and physiotherapy management team was mainly around terminology used. They suggested changes to questions regarding the question flow and some definitions. The flow of the survey was improved and streamlined after the feedback was received until no further feedback was forthcoming.
A full copy of the survey can be found in Supplemental Appendix 1.
Survey administration
The East Metropolitan Health Service research governance unit (Perth, Australia) deemed this survey to be a service evaluation project and did not require research ethics or governance approval due to the survey participants being anonymous, not deemed to be vulnerable, were in the public domain and performed the questionnaire voluntarily.
The target population of respondents were physiotherapists, physical therapists and respiratory therapists who identified as an ‘ICU therapist’. The exact sample size of eligible ICU therapists from around the world was unknown, therefore the participant responses received were a representative convenience sample of a larger international ICU therapist population. Any responses from professions other than an ‘ICU therapist’ were excluded.
The survey was developed and distributed using the online survey tool REDCap®. 9 The REDCap® site created a web-based survey link, which was advertised and posted on the relevant web pages and social media forums (Facebook, Twitter and LinkedIn) utilised by various ICU therapist associations, professional organisations and ICU therapists special interest groups worldwide. The survey link was also emailed to relevant networks with whom the authors had connections. A snowballing technique was used to encourage survey participants to forward the e-survey link within their own networks. Follow up emails and posts to the social media forums were sent on five different occasions.
Participants could respond to the survey voluntarily without any incentives hence informed consent was not sought. At the end of the survey, participants had the option to provide contact details voluntarily if they chose to join the LUS networking group. The survey was open on REDCap® for an 8-week period between March and May 2021 after which further responses were not possible. REDCap® is Western Australia (WA) Health research data collection software, it requires password access and only WA Health employee (main author) had access to the survey responses. The survey responses were automatically captured, and results generated were de-identified.
Data analysis
Data were exported and analysed using the REDCap®’s export format function. For closed or multiple-choice questions, each question had a different denominator and percentage (%) was calculated against the total number of responses to that question. Partially completed entries or incomplete entries were analysed according to the questions answered. Inappropriate survey responses (i.e. a doctor responding to this survey) were eliminated from the analysis.
Free-text responses were analysed for common topics. The frequency of the free text responses were either included within existing options or reported separately. There was no completeness check nor non-response option in the survey. Respondents could simply not answer the question if they chose not to respond. Respondents could change their answers before submitting the survey or click submit before answering all the questions.
Results
Three hundred twenty ICU therapists completed the survey (either partially or fully).
Three hundred twenty participants responded to at least one survey question with 283 completing the survey in full. One respondent was excluded as they were not an ICU therapist.
The demographics of the ICU therapists surveyed
The geographical region of the respondents was presented according to the World Confederation for Physical Therapy (WCPT) five main regions. 10
Most of the ICU therapist respondents (89%; 270/304) reported being a physiotherapist. Close to half (47%; 147/315) reported their geographical region as Asia Western Pacific followed by 42% (133/315) in Europe. Many of the respondents worked in either a tertiary/teaching hospital (62%; 194/312) or a general/outer metropolitan (33%; 104/312) hospital (Figure 1).
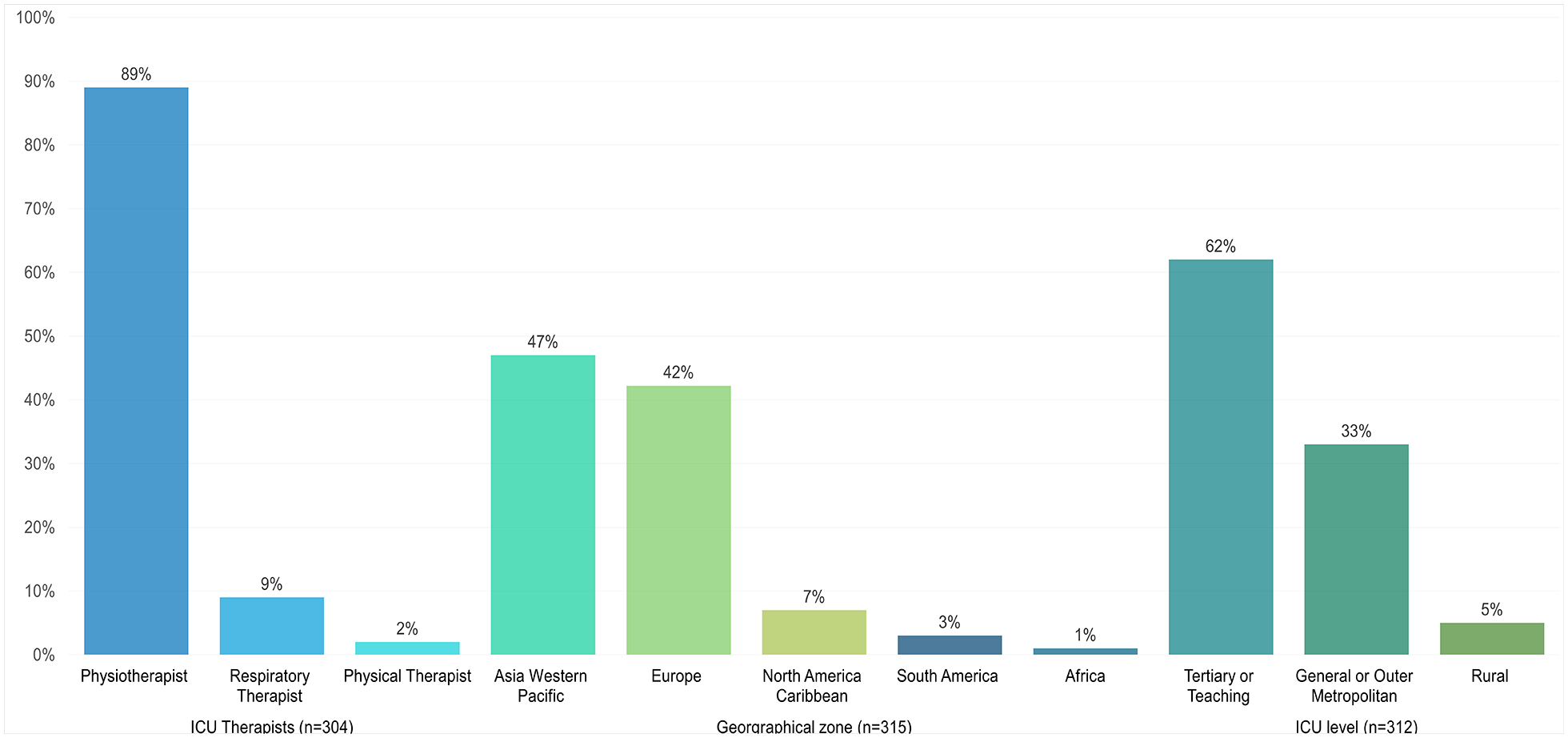
Respondent’s demographics.
Respondents reported coming from 30 different countries with most respondents coming from two countries, the United Kingdom (U.K.) (n = 94) or Australia (n = 87). A full list of the respondent’s countries of practice can be found in Supplemental Appendix 2.
The ICU therapist’s practice around the use of LUS
Eighty-nine (30%; 89/297) of the ICU therapist respondents reported being users of LUS (termed as ‘LUS users’). However, 40 of those 89 respondents (45%) reported having no formal accreditation in LUS, either through a relevant ICU/ultrasound society programme or university course (Figure 2).
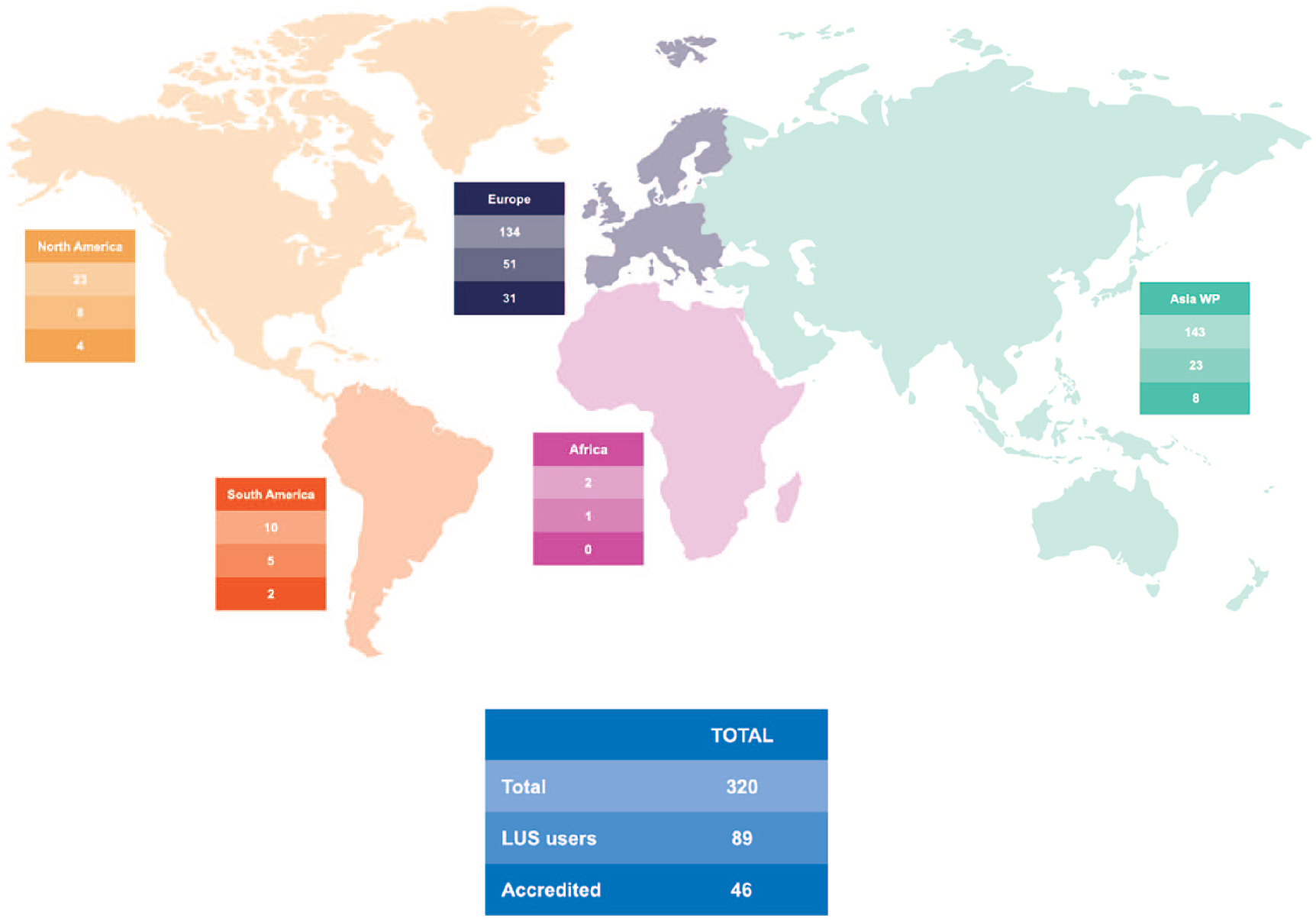
Number of LUS users and their accreditation status.
Just over a third of LUS users (36%; 32/89) reported having a local competency assessment for ICU therapists using LUS. Almost all (99%; 84/85) of the ICU therapists’ who did report having a formal LUS accreditation, had their competency assessed by either an appropriately trained medical professional, sonographer, or equivalently recognised professional.
The 13% (11/82) of the LUS users routinely scan every patient as part of their objective examination. The 70% (57/81) of the LUS users continue to use lung auscultation as part of their routine objective examination.
The 90% (64/71) of the LUS users scan patients at their own discretion while 25% (18/71) will scan at the direction of the treating intensivist or senior medical physician and 21% (15/71) will scan at the direction of the multidisciplinary team (MDT).
A full list of the LUS users’ indications to perform a LUS scan can be found in Figure 3.
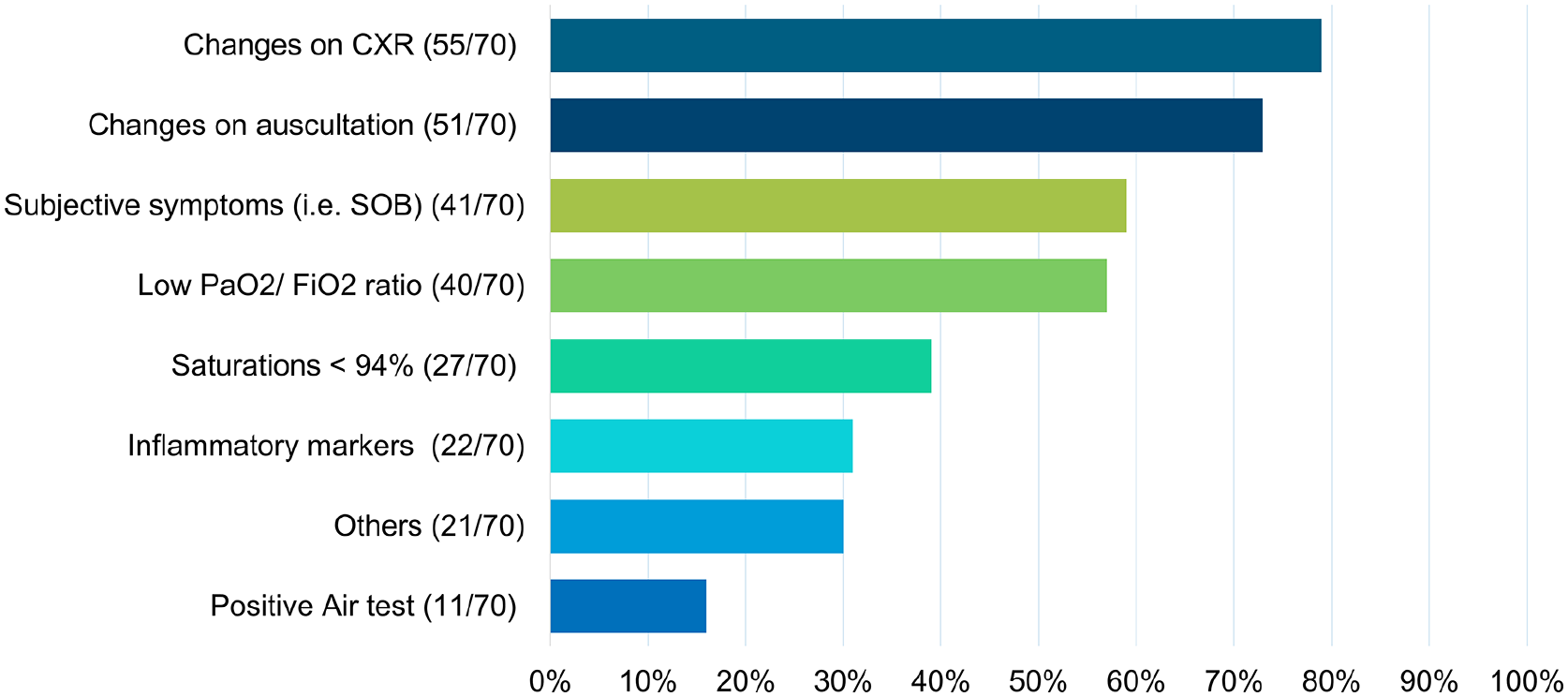
ICU therapists’ indications to use LUS.
The ICU’s practice around the use of LUS
Around 85% (248/293) of respondents reported their ICU does not routinely use LUS as an alternative to CXR. Almost half of all the respondents (46%; 146/318) reported that their ICU continues to do routine CXRs on patients with respiratory problems, regardless of their clinical state. However, 26% (75/296) reported that they had seen an increase in the use of LUS in their ICU since the SARS-CoV-2 pandemic.
Of the LUS users, 71% (63/89) of them reported that their ICU does not have a local policy in place to guide ICU therapists’ use of LUS.
Figure 4 Showed LUS users’ methods of scan feedback, reporting and storing.
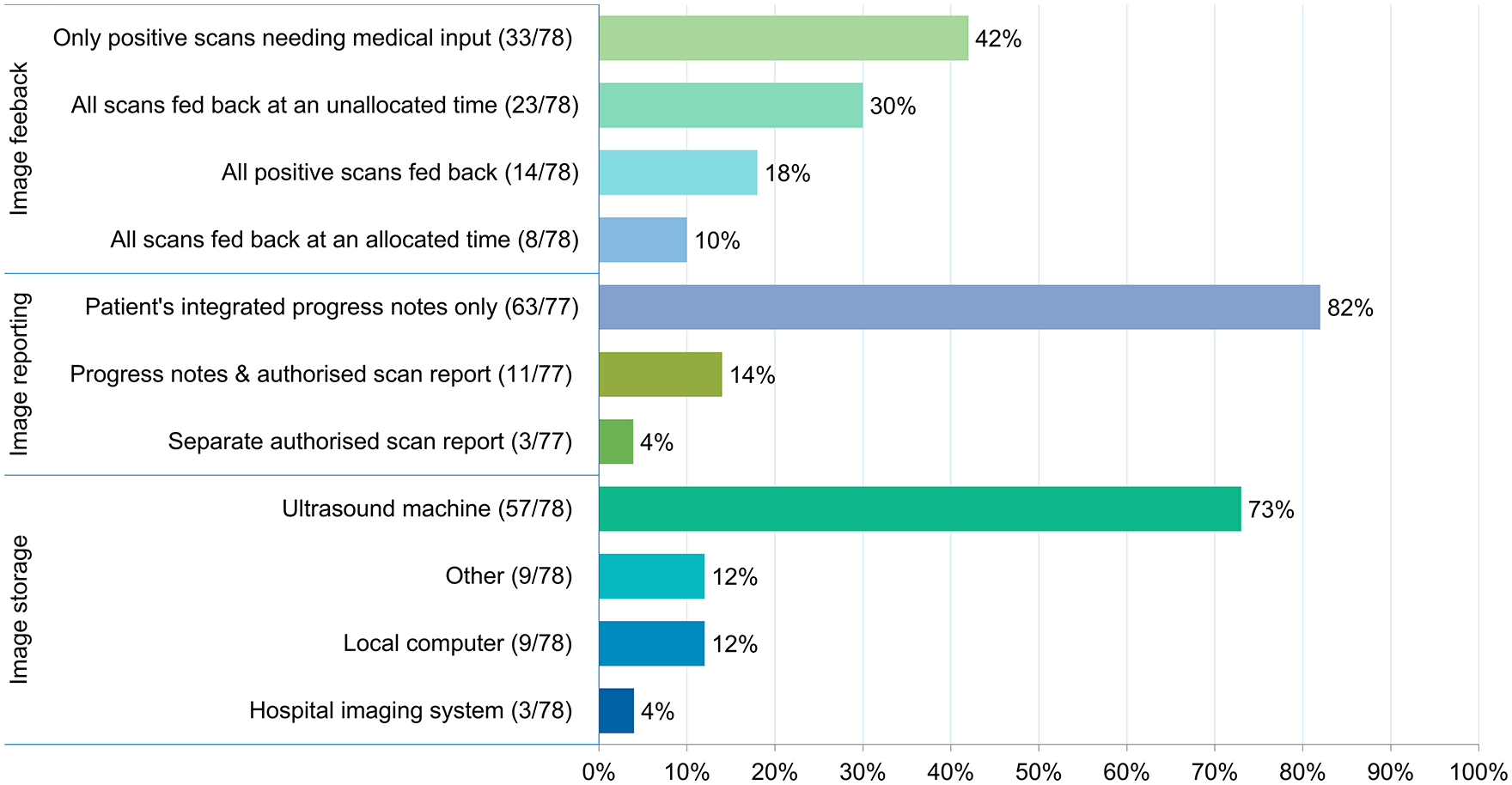
LUS users’ methods of scan feedback, reporting and storing.
LUS implementation
The majority of respondents (85%; 248/293) see LUS becoming an increasing part of the objective assessment for ICU therapists in the future.
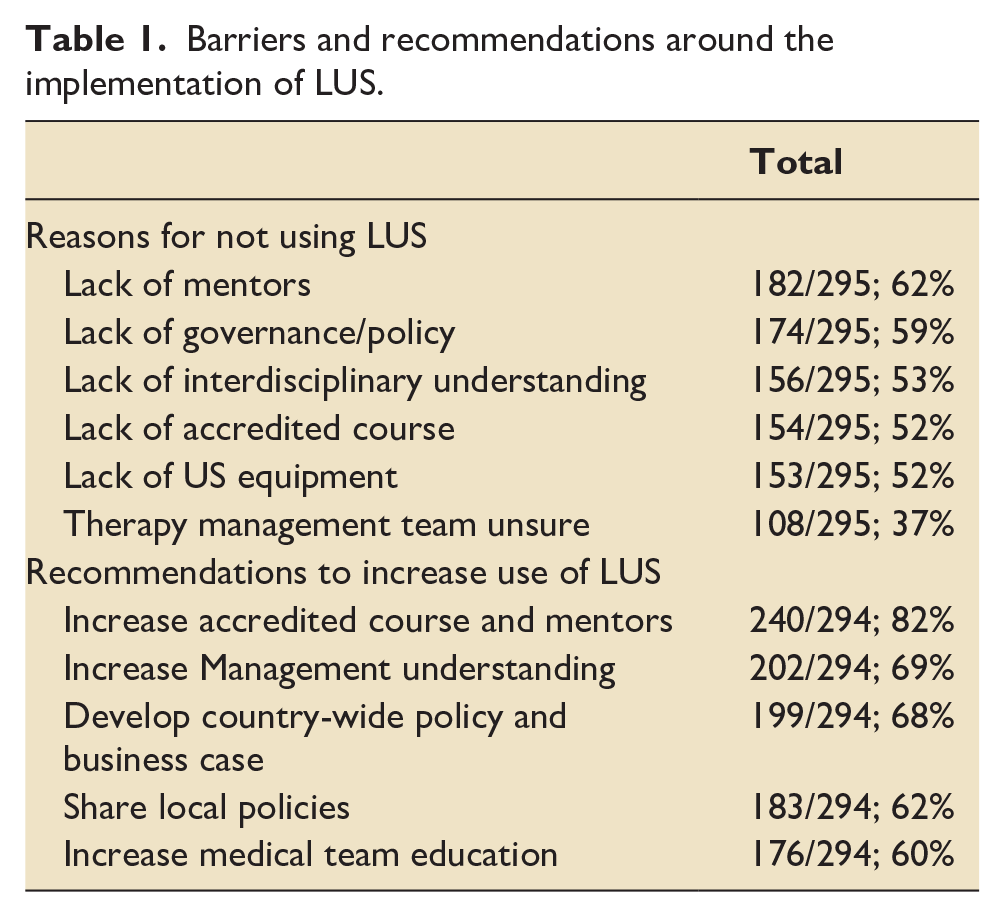
Most of the respondents (96%; 279/290) report that they have one or more therapists within their ICU who are interested in using LUS however barriers exist to the adoption of LUS. The main reasons why respondents believe that ICU therapists are not adopting LUS in their ICU and the possible solutions can be found in Table 1.
Barriers and recommendations around the implementation of LUS.
Discussion
This international survey was the first to explore the adoption and utility of LUS by 320 ICU therapists from 30 countries across all five geographical regions. The 30% (89/297) of ICU therapists reported they actively use LUS. Concerningly, almost half of these ICU therapists reported having no formal LUS accreditation. This highlights a significant potential safety risk towards patients as the therapists in question have no meaningful evidence to demonstrate their capabilities against a recognised standard of training or practice. Most ICU therapists believe that LUS will eventually become part of their objective assessment. Specific indications and uses with consistent access to specific training and mentorship while being supported by departmental guidance and policies should be a priority for ICU therapists.
The demographics of the ICU therapists surveyed
As this is the first survey to explore where ICU therapists are attempting to adopt and/or use LUS in their practice, with respondents coming from 30 different countries, it shows the widespread international interest in LUS. Previous published work to compare with these findings is very limited.
Although the searches for the Hayward and Janssen 11 scoping review were performed in 2016, and the results were not all from ICU, the review reported 26 therapist-led LUS publications from all but one of the five geographical regions. Both ‘Asia Western Pacific’ and ‘South America’ were well represented by having 12 and 11 publications respectively. 11 When combined with this survey’s results, it hints at a potentially strong interest and use of LUS by therapists in both regions, particularly within the ‘Asia Western Pacific’ region.
The ICU therapist’s practice around the use of LUS
The 89 LUS users, comprising 30% (89/297) of all respondents, was a slightly higher proportion when compared to the 23% reported in the U.K. by Hayward et al. 1 However, with 40 of those 89 (45%) reporting to have no formal accreditation in LUS, this survey’s results do not compare favourably to other similar work. Yang et al. 12 reported only 30% of intensivists in Australasian ICUs were considered ‘untrained’ to use LUS, Hayward et al. 1 reported that only 13% of U.K. physiotherapists who use LUS are not accredited. In Australia, Hansell et al. 8 reported 90% of their respondents who use LUS to inform clinical decision-making are not accredited.
These findings raise concerns about the lack of training and governance oversight for ICU therapists in some countries. ICU therapists should seek guidance from their professional organisations on the adoption and utility of LUS in conjunction with the published literature. Two documents covering the use of point of care ultrasound (POCUS) by physiotherapists have recently been published by the Chartered Society of Physiotherapists (CSP) in the U.K. The first explains the context of physiotherapists’ using POCUS 13 while the second is a practice guidance. 14 In combination with these two documents, the proposed LUS framework for respiratory physiotherapists by Smith et al. 15 could form an initial foundation to address scope of practice, education, and governance issues for ICU therapists considering exploring the adoption and utility of LUS into their practice.
Reassuringly, the ICU therapists who had undergone a LUS competency assessment were almost always approved by an appropriately trained and recognised professional meaning robust training standards were possible to achieve.
With 90% (64/71) of LUS users scanning at their own discretion and 13% (11/82) scanning every patient they assess, having clear evidence-based guidance on the indications to perform a LUS scan for ICU therapists could reduce unnecessary scanning, target patient specific interventions and maintain ICU therapists’ autonomy. This survey’s respondents highlighted some of the possible indications that may prove useful to ICU therapists (Figure 3).
In conjunction with the potential indications found in the work by Kruisselbrink et al. 16 and Hayward et al., 1 a research study into ICU therapist specific indications could strengthen the understanding around which clinical presentations or findings require additional investigation with LUS. An increased and appropriate use of LUS by the whole MDT may also reduce the number of CXR patients are exposed to during their ICU admission. 17
The ICU’s practice around the use of LUS
The reported uptake of LUS at an ICU level appears to remain low with 85% (248/293) of respondents reported their ICU did not use LUS as an alternative to CXR. In contrast, Calamai et al. 18 reported that LUS was performed by intensivists in 94% of the Italian ICUs and Yang et al. 12 found that 83% of Australasian ICUs were using LUS. This highlights that the adoption of LUS varies across different regions and countries. However, with 26% (75/296) of ICU therapist respondents reporting that they had seen an increase in the use of LUS in their ICU since the beginning of the SARS-CoV-2 pandemic, opportunities for ICU therapists to adopt and use LUS should increase as well. There will need to be a major cultural change for LUS to become the new standard of care over CXR particularly in an ICU setting.
Of the 89 LUS users, 71% (63/89) of them reported that their ICU does not have a local policy in place to guide an ICU therapists’ use of LUS. These results are worse than those found by Ellis et al. 19 who reported that over half of their respondents (56%) believed there was no practice guideline for the use of musculoskeletal ultrasound by physiotherapists in their country of practice.
Guidance on how ICU therapists perform, report and store LUS images, as individuals or as part of a MDT, are paramount. Any variations from locally approved practises only increases the chances of miscommunication alongside lower levels of quality assurance which puts the patient at a potentially higher risk of mismanagement, harm, or both.
The ICU therapist’s implementation of LUS
Almost all respondents (96%; 279/290) reported that they have one or more therapists in their ICU who are interested in adopting and using LUS. More importantly, most of the respondents (85%; 248/293) see LUS becoming part of their objective assessment on ICU in the future. Both findings show the degree of interest and desire amongst ICU therapists to learn and adopt LUS into their practice.
The top two reasons why ICU therapists are not using LUS are; a difficulty in accessing mentorship and a lack of a local governance policy. These findings echo some of the barriers identified by Hayward et al.1,7 and Hansell et al. 8 regarding a lack of mentorship and concerns around the governance for this novel technique, resulting in the potential delay of its adoption by ICU therapists.
When these reasons are combined with the other barriers found in Table 1 alongside those from previous work, it is reasonable to conclude that to adopt and implement the use of LUS by therapists in ICUs more widely, managers and policy makers need to consider providing practical support for ICU therapists to learn LUS. These may include clinical and non-clinical time for mentors to teach LUS, develop country-wide policy and business cases to increase awareness of the benefits of LUS and learning from countries where LUS use amongst ICU therapists is more established.
Strengths and limitations of the study:
This survey is the first study to explore the practicality of LUS uses among ICU therapists, at an international level. The survey received a relatively large numbers of responses from a more ‘focused’ represented group of therapists who have direct interest or knowledge of LUS, hence the generalisability of the results to this group is strong.
Survey pilot testing was performed by individuals from one hospital based in Australia and unlikely to be representative of the final sample of international respondents. The survey used a convenience sample and therefore, it may be biassed to those therapists that use technology and social media and unlikely to be representative of the entire population of ICU therapists globally. It is also not possible to know how many ICU therapists the survey reached; therefore, a response rate cannot be determined. This study used a snow-balling technique to all ICU therapists via social media and via the authors’ strong connections among U.K. or Australia thus the potential influence of significant selection bias cannot be ruled out. Furthermore, the respondents completed the survey voluntarily, which may suggest self-selection in terms of higher interest and awareness of LUS. Multiple responses, from a single site or respondent, may have biassed the results through inflated positive or negative responses from a site that has a particular interest in LUS.
Conclusion
To the authors’ knowledge this is the first study to explore the international adoption and utility of LUS by ICU therapists. LUS is a growing technique with widespread interest from ICU therapists internationally with a desire to adopt LUS into their assessments and upskill their practice. However, there are varying degrees of LUS adoption between geographical regions and countries. ICU therapists’ use of LUS could allow more targetted and appropriate treatment for patients on ICU thus avoiding deterioration and enhance recovery. Barriers to LUS adoption could be reduced through the education of ICU therapists’ management on the potential of LUS and thus facilitate access to quality training, supported by dedicated time to train.
Supplemental Material
sj-docx-1-inc-10.1177_17511437221148920 – Supplemental material for An international survey exploring the adoption and utility of diagnostic lung ultrasound by physiotherapists and respiratory therapists in intensive care
Supplemental material, sj-docx-1-inc-10.1177_17511437221148920 for An international survey exploring the adoption and utility of diagnostic lung ultrasound by physiotherapists and respiratory therapists in intensive care by Yin Hung Lau, Simon Hayward and George Ntoumenopoulos in Journal of the Intensive Care Society
Supplemental Material
sj-docx-2-inc-10.1177_17511437221148920 – Supplemental material for An international survey exploring the adoption and utility of diagnostic lung ultrasound by physiotherapists and respiratory therapists in intensive care
Supplemental material, sj-docx-2-inc-10.1177_17511437221148920 for An international survey exploring the adoption and utility of diagnostic lung ultrasound by physiotherapists and respiratory therapists in intensive care by Yin Hung Lau, Simon Hayward and George Ntoumenopoulos in Journal of the Intensive Care Society
Footnotes
Acknowledgements
The authors would like to thank the ICU therapists who responded to the survey. This survey was supported by the WA Health Translation Network.
Special thanks to
- The ICU medical, nursing and physiotherapy leadership group at Armadale Kalamunda Group (AKG) for supporting this seeding research activity to commence
- The Physiotherapy head of department Ms Carol Watson at Royal Perth Bentley Group (RPBG) for the full support of clinician’s time in the teaching and developing physiotherapy led LUS
- Dr Ashes Mukherjee (AKG Emergency physician) and Dr Adam Howard (RPBG Intensivist) for your dedicated transdisciplinary time in mentoring LUS
Contributors
Fion Lau, Simon Hayward and George Ntoumenopoulos all contributed to the development of the study design and were significantly involved in the drafting of the article and revising it. All have given final approval of the version to be published.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The survey was part-funded by the Western Australia Department of Health. The funder has no role in the survey’s design, implementation and analysis of the results.
Ethical approval
East Metropolitan Health Service Research hub (Perth, Australia) confirmed that this survey does not require research ethics and governance approval was provided on 9th December 2020.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.