
Abstract
A 59-year-old man was diagnosed with a massive pulmonary embolism. Despite thrombolysis there were two episodes of cardiac arrest and following recovery of spontaneous circulation profound cardiorespiratory failure ensued. An extracorporeal membrane oxygenation retrieval team initiated veno-venous extracorporeal membrane oxygenation on site to facilitate transfer to the extracorporeal membrane oxygenation centre. An excellent outcome is reported in the short term. This represents one of the few published cases of veno-venous extracorporeal membrane oxygenation for a massive pulmonary embolism following thrombolysis.
Introduction
Early mortality associated with pulmonary embolism (PE) ranges from 7 to 11%, which in Europe corresponds to over one million deaths/year. 1 Massive PE is defined as sustained hypotension (systolic blood pressure (SBP) <90 mmHg) for >15 min secondary to acute PE or a requirement of inotropes or signs of shock. 2 Registry data suggest a 90-day mortality rate of 52% in patients presenting with hypotension or circulatory arrest, 3 and it is thought many die within the first hours of presentation.4,5 Patients with massive PE often have acute right ventricular (RV) dysfunction and pulmonary arterial hypertension. A vicious spiral of hypoxaemia, hypercarbia (both potent pulmonary vasoconstrictors), RV failure and low cardiac output with further myocardial ischaemia may be fatal. Extracorporeal membrane oxygenation (ECMO) is a potential supportive treatment for massive PE. Veno-arterial (VA) ECMO can be used to support the patient haemodynamically (by returning oxygenated blood to the aorta under pressure in addition to the patients underlying cardiac output) or veno-venous (VV) ECMO can be used for severe respiratory failure.6,7 We present a case of VV-ECMO for severe respiratory failure following thrombolytic therapy for massive PE of which few previous cases have been described.
Case
A 59-year-old male presented to his GP with a two-week history of productive cough and progressive exertional dyspnoea, not responding to treatment for a presumed chest infection. A week-long history of polyuria and polydipsia was also elicited. Past medical history was unremarkable except for a possible PE following an orthopaedic procedure in 2002. On examination the patient was tachypnoeic and peripherally shut down with low oxygen saturations. Urgent transfer to hospital by ambulance was arranged. En route his respiratory rate was 40 breaths/min, saturations were 88–93% in air, his heart rate (HR) was 125 beats/min and blood pressure (BP) was 128/97 mmHg. In the emergency department (ED) he was noted to be peripherally vasoconstricted, with a respiratory rate of 36 breaths/min, oxygen saturations were 90% on a 15 l non-rebreather mask, HR was 106/min and an initial BP was 116/80 mmHg; his blood glucose was 31 mmol/l. An arterial blood gas revealed a pH 7.34, PaO2 10.9 kPa, PaCO2 4.3 kPa, base excess (BE) 8 mmol/l and a lactate 3.2 mmol/l. He received a ‘treatment dose’ of low-molecular-weight heparin – 18,000 units of subcutaneous Dalteparin. Over the course of the first half-hour in the ED he deteriorated and this resulted in a referral to the intensive care team. Continuous positive airway pressure (CPAP) of 10 mmHg was instituted, an arterial line sited, fluid resuscitation was initiated and an insulin sliding scale commenced. Laboratory blood results showed: Hb 172 g/l, WCC 23.4 × 109/l (neutrophils: 17.6), platelets 242 × 109/l, CRP 90 mg/l, bilirubin 16 µmol/l, ALT 65 IU/l, ALP 150 IU/l. Renal function, bone profile and clotting studies were within normal limits. Bedside ketones were 1.0 mmol/l. Arterial blood gas analysis on CPAP with 100% oxygen showed pH 7.04, PaO2 38 kPa, PaCO2 6.36 kPa, HCO3 11.3 mmol/l, BE 16.2 mmol/l, lactate 8.5 mmol/l and glucose 32 mmol/l. A portable AP chest X-ray showed no obvious abnormalities and was subsequently reported as normal.
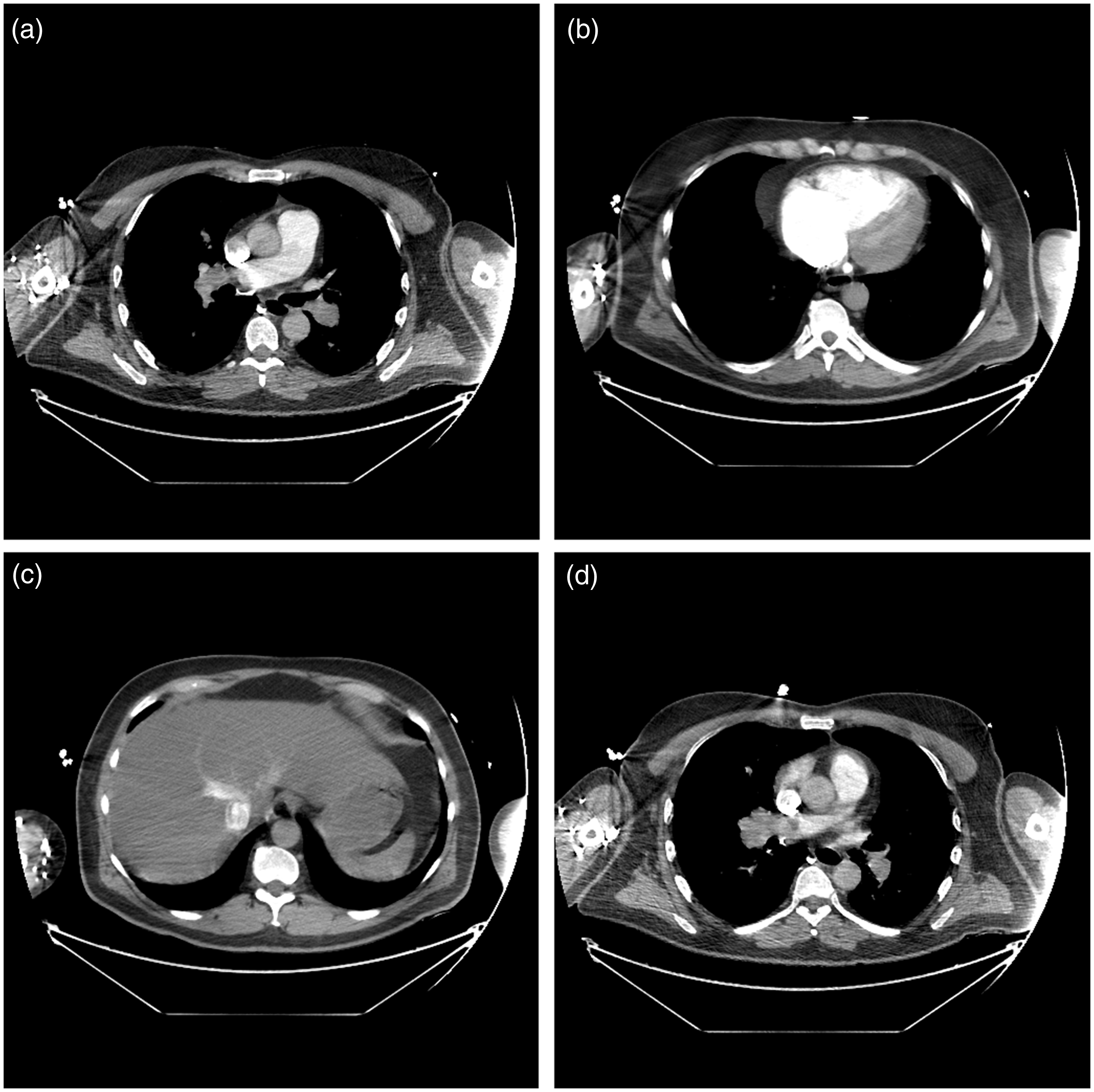
A bedside focussed echocardiogram revealed a dilated RV with septal bowing (Figure 1). A presumed diagnosis of massive PE was made. To confirm these suspicions a computerised tomography pulmonary angiography (CTPA) scan was performed, which confirmed a saddle PE; it also demonstrated the triad of radiological RV strain features with a main pulmonary artery (mPA):aorta ratio >1, septal bowing and reflux of contrast to the IVC (Figure 2(a) to (d)).
8
The patient was immediately transferred to the intensive care unit and received thrombolysis with recombinant tissue plasminogen activator (rtPA, 10 mg bolus) followed by an infusion (rtPA 90 mg). A femoral central venous cannula was inserted. Shortly after starting the infusion of rtPA the patient continued to deteriorate on increasing vasopressor (norepinephrine) support, developing ventricular tachycardia (VT) requiring DC cardioversion, followed by a pulseless electrical activity (PEA) cardiac arrest. Endotracheal intubation was performed uneventfully and a further rtPA bolus of 40 mg was given (bringing the total dose of rtPA at this time to 50 mg). Following 14 min of advanced life support (ALS) there was return of spontaneous circulation (ROSC). The patient remained critically unwell, with severe mixed acidosis (lactate 15 mmol/l), requiring high dose norepinephrine (∼1 µg/kg/min) and epinephrine (0.19 µg/kg/min). Prolonged periods of VT and atrial fibrillation with right bundle branch block followed for which 300 mg of amiodarone was given. A further PEA arrest required 2 min of ALS with subsequent ROSC. Although thrombolysis can be seen as a relative contraindication, a referral was made to the local ECMO centre for consideration of VA-ECMO due to persistent haemodynamic compromise and refractory hypercapnia. A dual-lumen left internal jugular cannula was inserted in anticipation of instituting haemodiafiltration to improve his metabolic acidosis.
Transthoracic ECHO images taken in A&E on presentation. (a) Parasternal short axis showing RV dilation with D-shaped LV is noted characteristic of high RV pressures and (b) apical four-chamber view showing dilated RV and bowing of the interventricular septal wall. LV: left ventricular; RV: right ventricular. CTPA. (a) Bilateral pulmonary emboli, (b) right ventricular dilatation with septal bowing, (c) retrograde contrast flow into the liver and (d) ratio of mPA to aorta >1. CTPA: computerised tomography pulmonary angiography.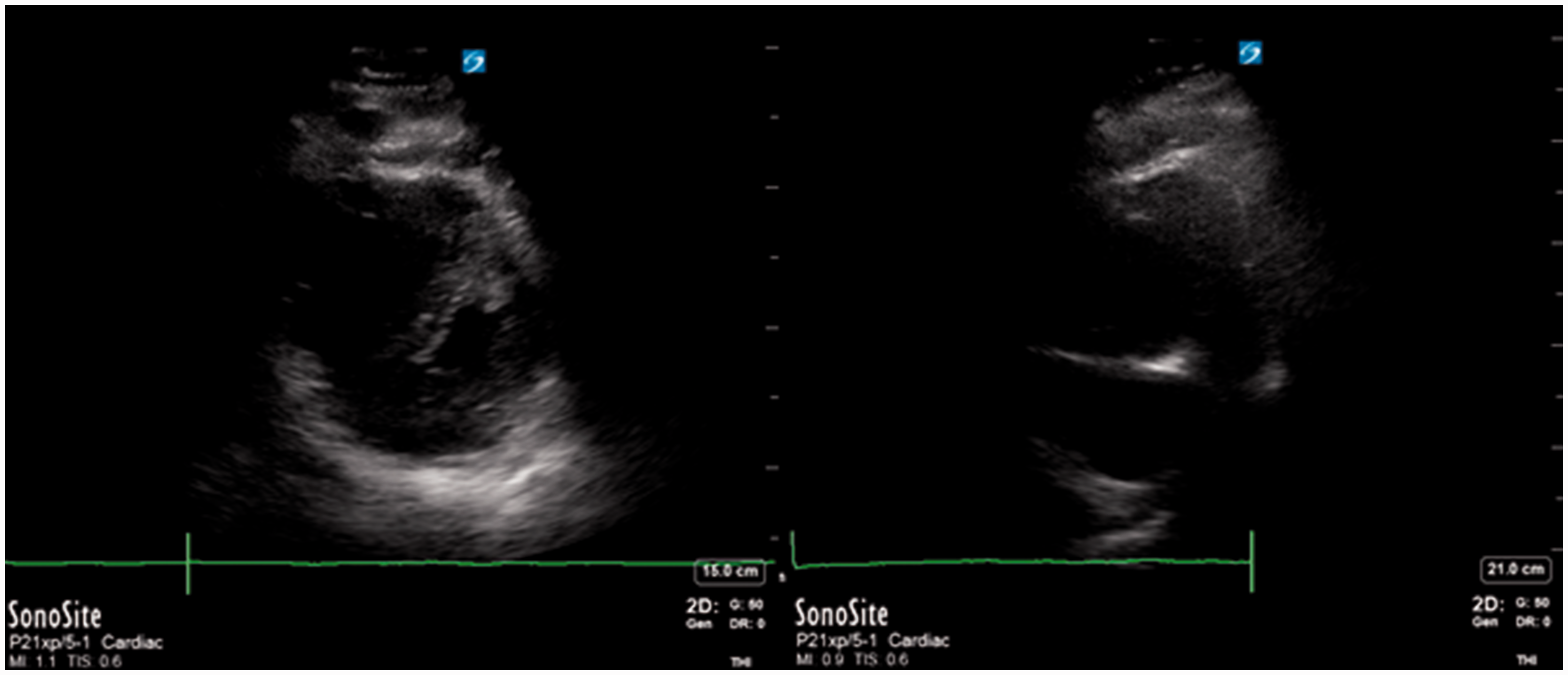
On arrival of the ECMO retrieval team the patients’ haemodynamics had improved significantly, yet he had worsening Type 2 respiratory failure with a pH 6.95, PaO2 10.3 kPa, PaCO2 of 12.3 kPa on 100% FiO2. Repeat chest X-ray revealed findings consistent with acute respiratory distress syndrome and possible intrapulmonary haemorrhage. The decision was made to transfer to theatre to institute VV-ECMO using a bifemoral approach, prior to transfer to the ECMO centre. Heparin was not given due to recent thrombolysis. Establishment on ECMO fully controlled his PaCO2, allowed ultraprotective lung ventilation strategy and also further reduced the RV strain. The patient was established on ECMO approximately 6 h following his first cardiac arrest.
At the ECMO Centre his haemodynamics worsened again and he was started on vasopressin and hydrocortisone due to high norepinephrine requirements (>1 µg/kg/min). A repeat echocardiogram showed significantly improved RV function with mild dilatation and a hyperdynamic left ventricle and therefore he was not converted to VA ECMO. He had a complicated course including marked coagulopathy with significant bleeding over the first 24–36 h from the ECMO cannula sites and from his lungs, which was anticipated and aggressively managed with fresh frozen plasma, cryoprecipitate, platelets and tranexamic acid. When the bleeding settled a heparin infusion was commenced with a target activated partial thromboplastin time ratio of 1.5–2 on day 5 and 2–2.5 by day 6. He developed an acute liver injury with a peak ALT of 4000 IU/l and a period of renal replacement therapy (RRT) was required for an acute kidney injury (AKI).
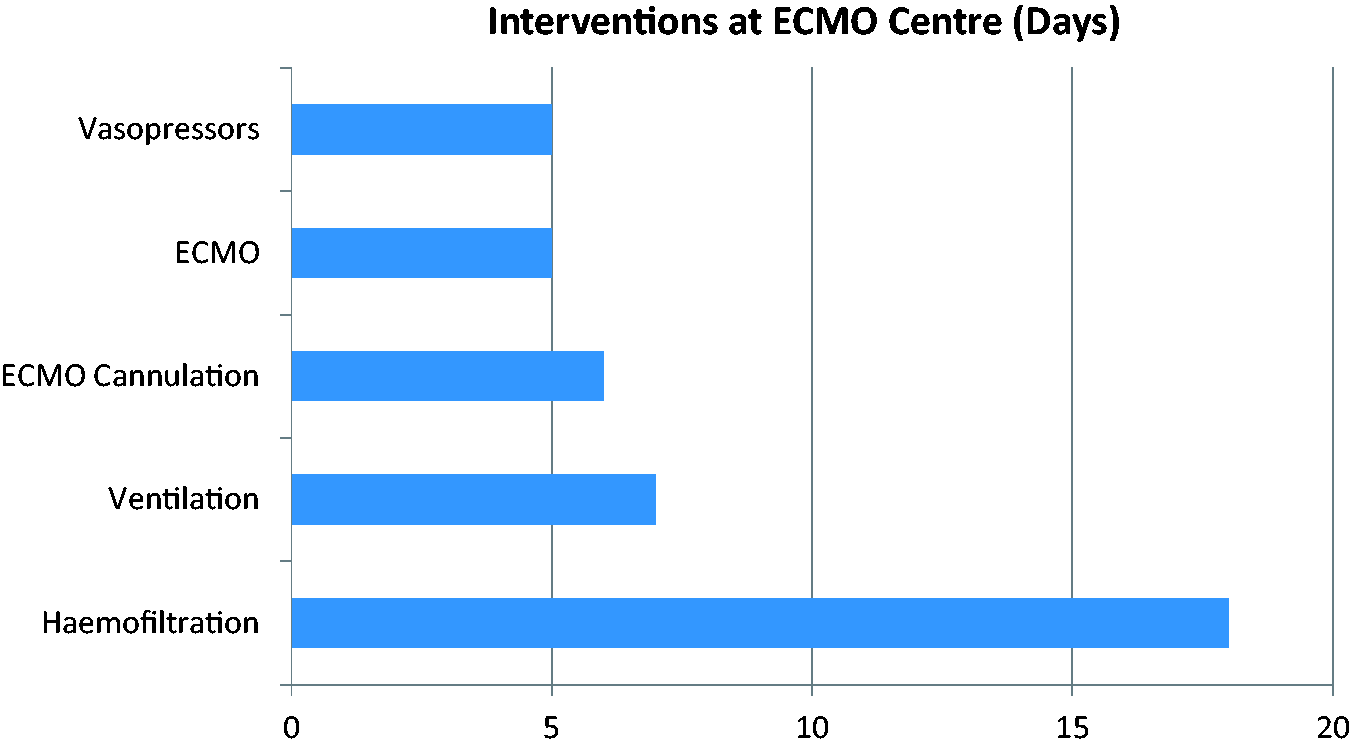
His haemodynamics improved during the first 48 h and vasopressors were weaned off by day 5. Respiratory function also improved, allowing a successful trial off ECMO support on day 5, decannulation on day 6 and extubation on day 7; the liver injury also resolved. The AKI persisted with ongoing need for RRT. Repatriation to the initial referring centre occurred on day 18. A repeat echocardiogram showed much improved biventricular function with a normal right atrial and ventricular size (Figure 3). There was no significant tricuspid regurgitation to quantify pulmonary artery systolic pressure. No further RRT was required. A degree of delirium gradually improved and he was stepped down to the ward on day 22 (Figure 4).
Repeat transthoracic ECHO images taken on day 20. (a) Apical four-chamber view and (b) subcostal view both show normal RV and LV chamber sizes via visual estimation. LV: left ventricular; RV: right ventricular. Organ support at ECMO centre. ECMO: extracorporeal membrane oxygenation.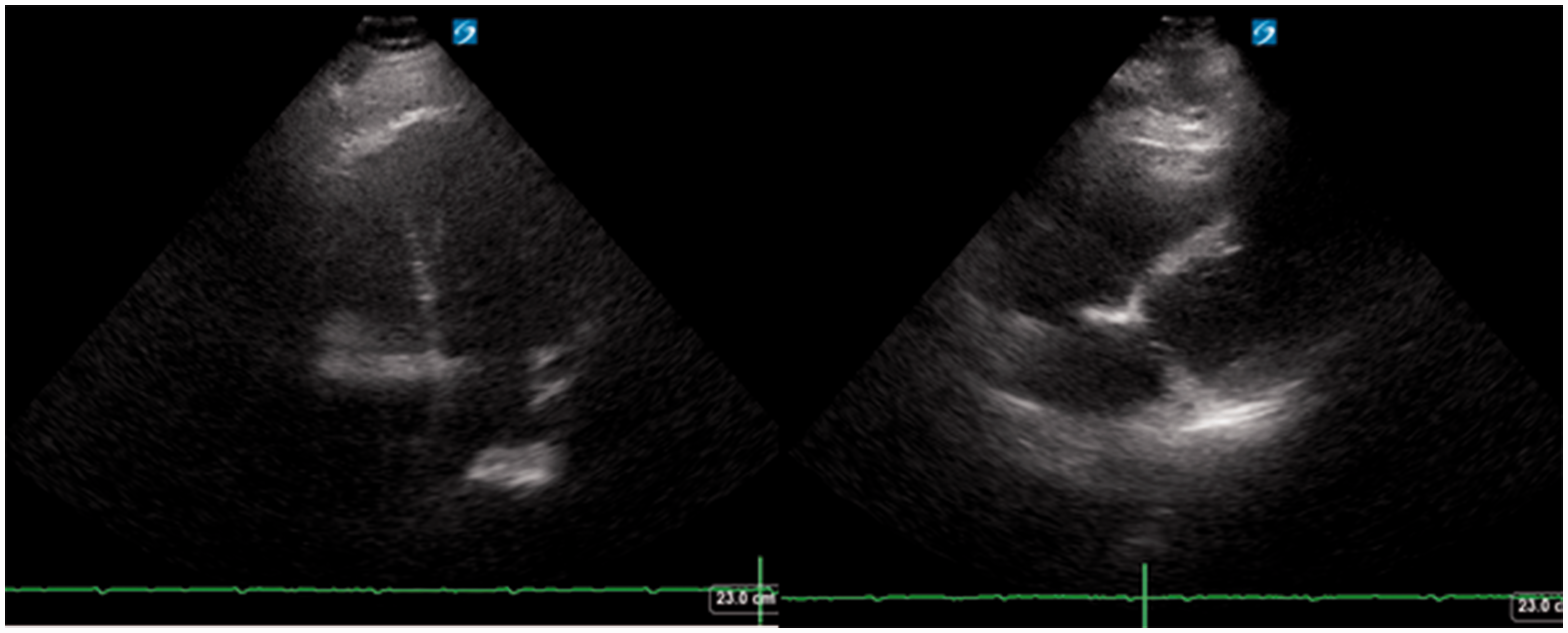
Discussion
The management of patients with massive PE complicated by acute cor pulmonale is challenging. From data derived largely from animal studies, the pathophysiology of circulatory failure and shock is thought to be primarily caused by a reduced cross-sectional area of the pulmonary vascular bed due to the mechanical effect of the embolus and secondary effects, including hypoxic/acidotic vasoconstriction and release of vasoactive substances. 9 Acute haemodynamic changes can induce a lethal spiral of obstruction to RV outflow with RV failure, reduced pulmonary blood flow and inadequate LV filling, leading to decreased cardiac output and systemic hypotension. The combination of elevated RV end-diastolic pressure with systemic hypotension results in decreased RV coronary perfusion pressure (CPP) and subsequent RV ischaemia. Additionally, in severe pulmonary hypertension the RV distends, resulting in a shift of the interventricular septum, compressing the LV, further inhibiting LV filling (ventricular interdependence) contributing to LV failure and systemic hypotension.10,11
It may be helpful to employ tools to risk stratify patients presenting with PE. One commonly used risk score is the simplified pulmonary embolism severity index, combining age, co-morbidities and physiological parameters, with mortality 1% in a low-risk group and 9–11% in those considered high risk. 12 This patient fell into the high-risk group based on initial ambulance parameters despite being normotensive. On echocardiography RV dysfunction incidence ranges from 40% in the normotensive to 70% in massive PE, though this may be influenced by selection bias (i.e. the acutely unwell are more likely to have an echocardiogram performed). A systematic review found RV dysfunction (usually defined as hypokinesis by a qualitative evaluation of RV wall motion) to be associated with at least a two-fold increased risk of mortality, though in patients who were normotensive, positive predictive value was poor. 13 The addition of N-terminal pro-brain natriuretic peptide and troponin has further prognostic value in the normotensive group. 14 Interestingly, one CT study noted that ventricular septal bowing was predictive of short-term mortality (and was specific but not sensitive) whilst the ratio of RV diameter to LV diameter and embolic burden were not. 15
John Gibbon in the 1930s, whilst looking after a patient with a massive PE, considered the possibility of an extracorporeal machine to provide oxygenation and later with his wife Mary pioneered the use of cardiopulmonary bypass. 16 In a 2009 review of Japanese experience with ECMO (n = 193), the modality was combined with surgical embolectomy (35%), thrombolytic therapy (62%), catheter therapy (24%) or heparin alone. 6 Overall survival rate was 73%, dropping to 65% in cases of cardiac arrest. A more recent systematic review (n = 78) outside Japan reported an overall survival of 70%. 7 Few studies have reported on the use of VV-ECMO in PE, with only two in the 2015 systematic review from the Maggio series (n = 21). 17 The modality was used because the patients had ‘adequate perfusion on vasoactive drugs and mild RV strain on echocardiogram’. 17 In a case report of a post-partum arrest, VA-ECMO was initially used but was switched to VV-ECMO once ventilator failure became the primary problem, as in the presented case. 18 In another case report a 51-year-old female required VV-ECMO in the presence of acute PE as a bridge to pulmonary thromboendarterectomy for (newly diagnosed) chronic thromboembolic pulmonary hypertension. 19 Finally, Aitchison et al. 20 reported the use of VV-ECMO in a patient who suffered a respiratory arrest secondary to multiple PEs and presumed reduced functional residual capacity after a large ventral hernia repair.
Other considerations
One key goal of management in massive PE is to optimise systemic BP. Norepinephrine may be the preferred agent from a number of animal PE models: α-mediated vasoconstriction increases mean arterial pressure which in turn increases RV CPP, β1-mediated inotropic effects may improve RV function and norepinephrine has minimal effect on pulmonary vascular pressures. 10 Epinephrine may be an option and was thought to be preferential in one case report. 9 Vasopressin in addition to systemic vasoconstriction does cause pulmonary vasodilation; however, a limitation is that at higher doses excessive systemic vasoconstriction may occur. There is little in the literature to guide such therapy. Positive pressure ventilation and induction/sedation may adversely affect haemodynamics and thus, if possible, intubation should be avoided. Indeed, in 1995, Davies et al. 21 reported a case of conscious VA-ECMO for PE.
The benefit of volume expansion is controversial with one study reporting an increase in cardiac index (CI) after fluid bolus in normotensive patients with low CI (n = 13). 22 However, in hypotensive patients with RV dysfunction, fluid administration may further increase RVEDP, decrease RV CPP, resulting in RV ischaemia and further deterioration in RV function. Experimental studies have confirmed this theory.11,23 In the Ghignone study norepinephrine was preferable to fluids. 23 Furthermore, a retrospective study of normotensive patients with PE and RV dilation suggested repeated boluses of furosemide (n = 40) were superior to fluid (n = 30) with decreased shock index, oxygen requirement and improved SBP at 24 h. 24 The role of diuretics is currently being investigated in a clinical trial. 25
Inhaled nitric oxide (iNO) has been proposed in cases in which hemodynamic compromise secondary to increased pulmonary vascular resistance, based on iNO’s selective dilation of the pulmonary vasculature (through smooth muscle relaxation by increasing cyclic guanosine monophosphate), improvement of
It is unclear in this case to what extent dehydration contributed to this patient’s risk and development of pulmonary emboli. He reported a history of polyuria and polydipsia, his blood glucose and ketones were significantly raised and he had biochemical features characteristic of dehydration. A consideration of a new diagnosis of type 2 diabetes mellitus was considered although he was euglycaemic off medication towards the end of his hospital stay.
Conclusions
We report a case of massive PE resulting in cardiac arrest and subsequent severe respiratory failure managed with VV-ECMO with an excellent recovery.
Footnotes
Author’s contributions
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.