
Abstract
Background
Perioperative interventions, targeted to increase global blood flow defined by explicit measured goals, reduce postoperative complications. Consequently, reliable non-invasive estimation of the cardiac output could have far-reaching benefit.
Methods
This study compared a non-invasive Doppler device – the ultrasonic cardiac output monitor (USCOM) – with the oesophageal Doppler monitor (ODM), on 25 patients during major abdominal surgery. Stroke volume was determined by USCOM (SVUSCOM) and ODM (SVODM) pre and post fluid challenges.
Results
A ≥ 10% change (Δ) SVUSCOM had a sensitivity of 94% and specificity of 88% to detect a ≥ 10% Δ SVODM; the area under the receiver operating curve was 0.94 (95% CI 0.90–0.99). Concordance was 98%, using an exclusion zone of <10% Δ SVODM. 135 measurements gave median SVUSCOM 80 ml (interquartile range 65–93 ml) and SVODM 86 ml (69–100 ml); mean bias was 5.9 ml (limits of agreement −20 to +30 ml) and percentage error 30%.
Conclusions
Following fluid challenges SVUSCOM showed good concordance and accurately discriminated a change ≥10% in SVODM.
Introduction
Historically, clinical assessment of volume status has included measurement of basic haemodynamic parameters (such as blood pressure), examination, imaging (chest X-ray), functional measures of organ perfusion (such as urine output) and the central venous pressure (CVP). These measures are often used to guide therapy outside higher dependency areas, but do not accurately predict volume status or responsiveness.1–3 Given that volume overload is associated with increased morbidity and mortality4,5 then measures that may prevent this, such as titrating resuscitation, guided by stroke volume (SV) changes, should be explored.1,3,6
Since the first description of the pulmonary artery catheter (PAC) in 1970, 7 enthusiasm and evidence of benefit for goal directed therapy (GDT), including measurement of the cardiac output (CO), has ebbed and flowed in intensive care (ICU), perioperatively8–11 and in the emergency department.12,13 In the most recent Cochrane systematic review and meta-analysis of GDT perioperatively (31 randomized controlled trials (RCTs), 5292 patients), the authors concluded that GDT reduces complications and hospital length of stay (LOS). 10 Of note, more recent trials have questioned the use of GDT and, when compared to restrictive fluid protocols, outcomes have been comparable.14–16 In the most recent, large RCT, investigating use of a GDT algorithm, using a non-calibrated cardiac output device, (LiDCOrapid, LiDCO, Cambridge, UK), the primary outcome (a composite of 30-day complications and mortality), occurred in 36.6% of intervention and 43.4% of usual care participants (relative risk, 0.84 (95% confidence intervals, CI, 0.71–1.01); absolute risk reduction, 6.8% (−0.3%–13.9%); P = 0.07). 17 In the same paper, the authors provided an updated systematic review, concluding that complications remained less frequent among patients treated according to a GDT algorithm (intervention 31.5% vs. control 41.6%; RR, 0.77 (95% CI 0.71–0.83)) and LOS was shorter (mean reduction 0.79 days (95% CI 0.96–0.62)).
Much interest has recently been focused on non-invasive cardiac output (CO) devices that could have application beyond the operating room. 18 For such a device to be useful clinically it must be accurate, precise and detect significant directional changes, reflecting the response of the heart to an intervention – most commonly change (Δ) in SV. 18 The Ultrasonic Cardiac Output Monitor (USCOM 1A, Uscom Ltd., Sydney, NSW, Australia) is a non-invasive continuous wave (CW) Doppler ultrasound device. CW Doppler has an accuracy measured by Doppler string phantoms of ±2.3%. 19 The USCOM, temporarily placed in the suprasternal notch, measures Doppler flow at the aortic valve and determines this over a cardiac cycle (the velocity time integral, VTI). SV is calculated by multiplying the VTI by an estimate of valve cross-sectional area (CSA), determined by applying height-indexed regression equations. 20 USCOM has been compared positively with flow probes in animals21,22 and in externally driven artificial hearts in orthotopic transplantation, with the pulmonary artery catheter (PAC). 23 Two recently published studies, by one group, have suggested the USCOM, when compared to the oesophageal Doppler monitor ((ODM), CardioQ-ODM™ Deltex Medical, Chichester, UK) is able to track changes in SV.24,25 The aim of this study was to further investigate the ability of the USCOM to detect significant changes in SV as assessed by the ODM, in patients undergoing major abdominal surgery, when performing fluid optimisation manoeuvres.
Methods
Data were collected prospectively from 25 patients undergoing major abdominal surgery, managed in accordance with established clinical guidelines, prepared according to the local enhanced recovery protocol. A favourable ethics opinion was received from the South Central Oxford A Ethics Committee (Reference 13/SC/0222). Informed written consent was obtained. Patients were excluded if under 18 years of age or if they presented with a history of heart failure, valvular disease, significant dysrhythmias, or contraindications to ODM (such as coagulopathy, oesophageal varices, or known aortic aneurysm).
Anaesthesia was induced to the discretion of the attending anaesthetist. Typically, patients received a short-acting opioid, propofol (2–3 mg kg−1) and a non-depolarizing neuromuscular blocking agent (rocuronium or atracurium) before endotracheal intubation. Anaesthesia was maintained with sevoflurane or desflurane at an age-corrected MAC value of 0.8–1.2. Additional short-acting opioids were administered as needed. After volume optimisation, metaraminol was administered as necessary to achieve a MAP of at least 60–70 mmHg. Patients were ventilated using tidal volumes of 6–8 ml kg−1, PEEP levels of 0–7 cm H2O, and a respiratory rate of 10–15 breaths per minute to maintain normocapnia through volume-controlled ventilation. Routine perioperative monitoring included electrocardiography, capnography, pulse oximetry, core temperature, airway pressure, invasive arterial pressure (AP) obtained from a radial arterial catheter and ODM. Patients were kept normothermic using a forced-air warming mattress.
Data collection
Simultaneous haemodynamic data from the two devices were recorded independently in a blinded fashion. The ODM (using an oesophageal Doppler probe OP6; Deltex Medical, Chichester, UK) has been well described elsewhere. 26 SV values were calculated as the average of 10 consecutive heart cycles, to minimise respiratory variability. Haemodynamic variables were registered manually and saved on the ODM software. Each USCOM reading was performed by one of the authors proficient in its’ use (experience with >200 scans) with the full focusing technique described by the company, by intermittently placing the probe in the suprasternal notch with the Doppler flow profile held steady, for a 7.5 second sweep. Aberrant flow profile outlines on visual inspection were rejected and scans scored according to the Freemantle criteria 27 (see supplementary file). ODM measurements were performed by the authors or a consultant anaesthetist experienced in ODM.
Patients
Patient characteristics.
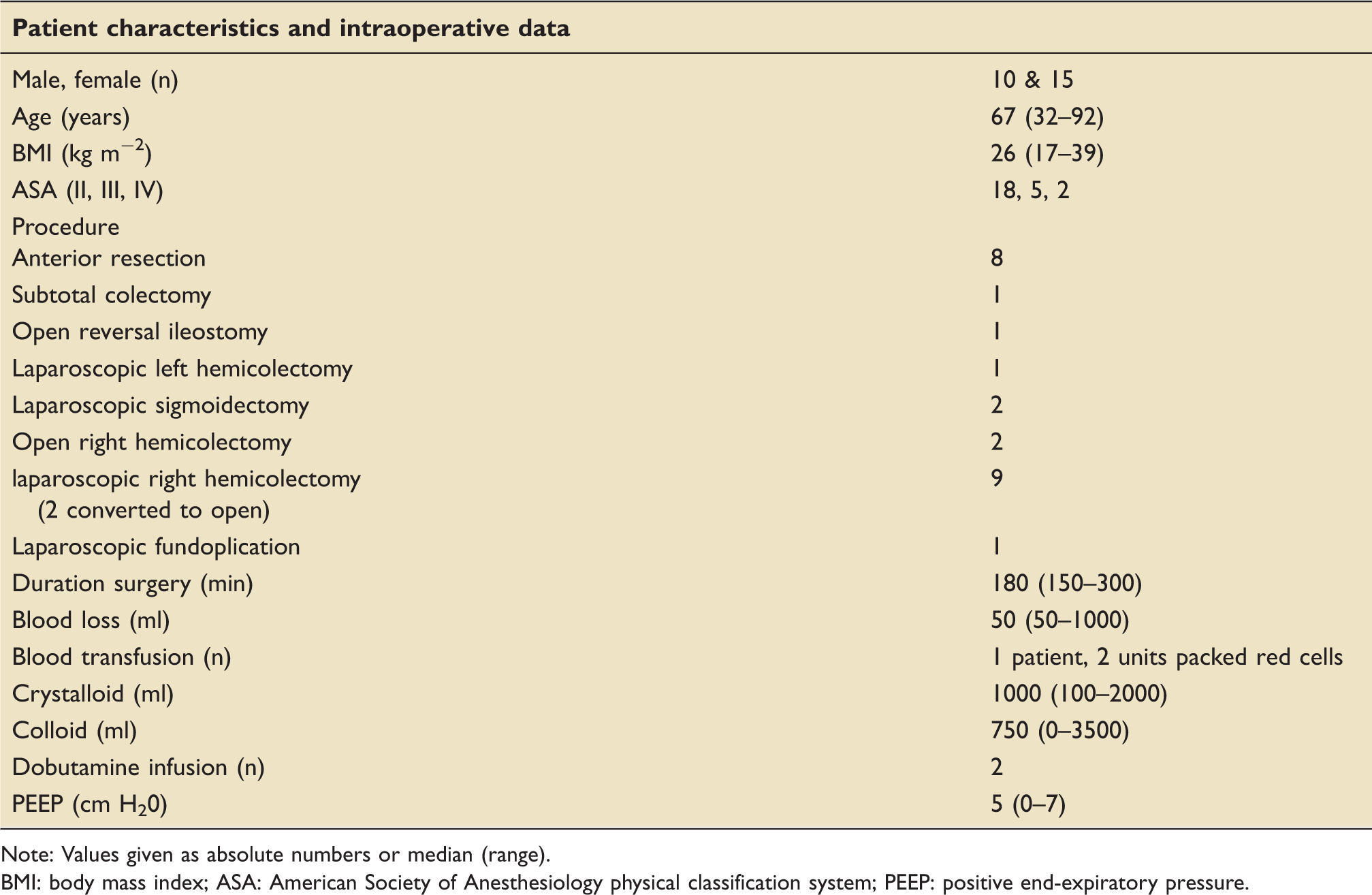
Note: Values given as absolute numbers or median (range).
BMI: body mass index; ASA: American Society Of Anesthesiology physical classification system; PEEP: positive end-expiratory pressure.
Study protocol
Prior to the start of surgery, when haemodynamic stability (<10% variation in SV and AP over a period of five minutes) was achieved, a standardised optimisation manoeuvre was conducted (with fluid loading performed using 250 ml of colloid or crystalloid administered over 3–5 min) with haemodynamic data (including ODM) recorded independently before and 5 min after, volume administration, as per normal practice. During the observation period, anaesthesia and ventilator settings were unchanged, no vasoactive drugs were administered and no postural changes to the patient were made.
If SV, as measured by ODM (SVODM), increased ≥10%, the fluid challenge was considered positive and an additional fluid bolus was immediately given. SV, rather than CO, was used to assess response to a fluid challenge, because an appropriate fall in heart rate in response to a fluid challenge may result in a decrease in CO, despite an increase in SV. After SV optimisation was achieved, surgery was commenced. During the course of surgery, optimisation manoeuvres were repeated at the discretion of the anaesthetist.
Statistics
To address the objective of the study – the ability of USCOM SV measurements (SVUSCOM) to reflect significant change (Δ) in SVODM following intraoperative fluid optimisation manoeuvres – a number of methods were employed. Concordance was assessed by plotting ΔSV between the two devices on a 4-quadrant scatter plot following fluid challenges, as according to the method used by Biancofiore et al.28,29 Studies have used zones of exclusion (Δ < 10% or <15%) to remove statistical noise from small inconsequential changes.30,31 When this is applied concordance should be >90–95%.30,31 A <10% change in SVODM was used as ODM is the more established method, as previously described. 29 Percentage clinical agreement (PCA) – the number of paired measurements within clinically acceptable limits of agreement (±15% of mean bias) – was also calculated. 32 PCA indicates what percentage of paired measurements can be considered clinically interchangeable. Sensitivity, specificity, and likelihood ratios were all calculated at the Δ10% cut-off for both devices. A receiver operating curve was plotted to compare the ability of the SVUSCOM to reflect a ≥ 10% Δ in SVODM with a fluid challenge.
The method of Bland and Altman to estimate bias, 95% limits of agreement and percentage error was also employed, 33 with a percentage error of <30% previously quoted for validation studies between reference method and new device. This has limitations extensively discussed in the literature largely due to the difficulty comparing two methods that are not true gold standards.31,34 Secondly, with relatively limited data points available in the context of an acute clinical setting, this study was not designed as a validation study. All data were imported into an Excel™ spreadsheet (Microsoft, Redmond, WA, USA) used to calculate concordance. All other statistical analyses were performed using the open source statistical package R (GNU project, R Foundation for Statistical Computing, Vienna, Austria).
Results
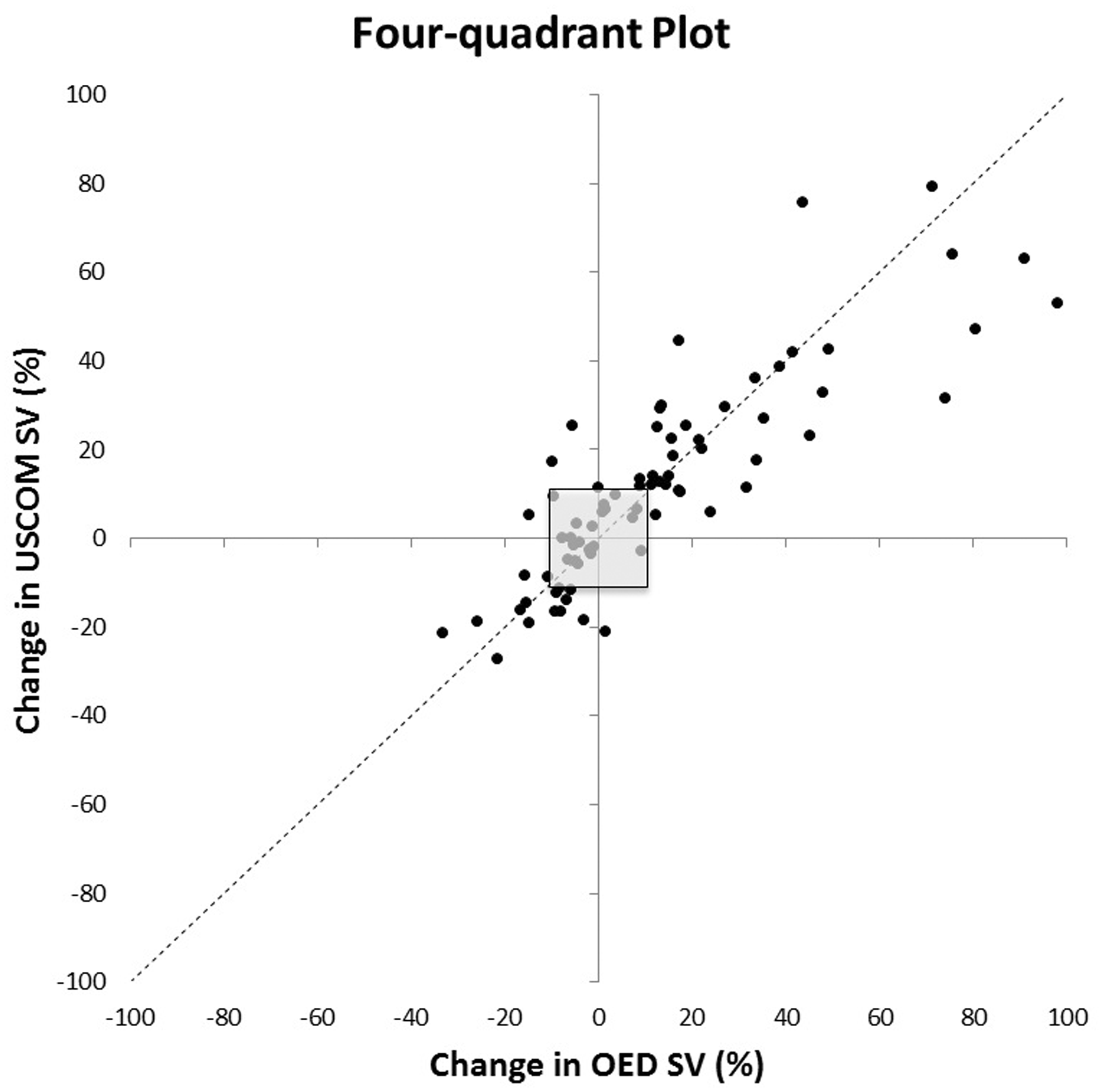
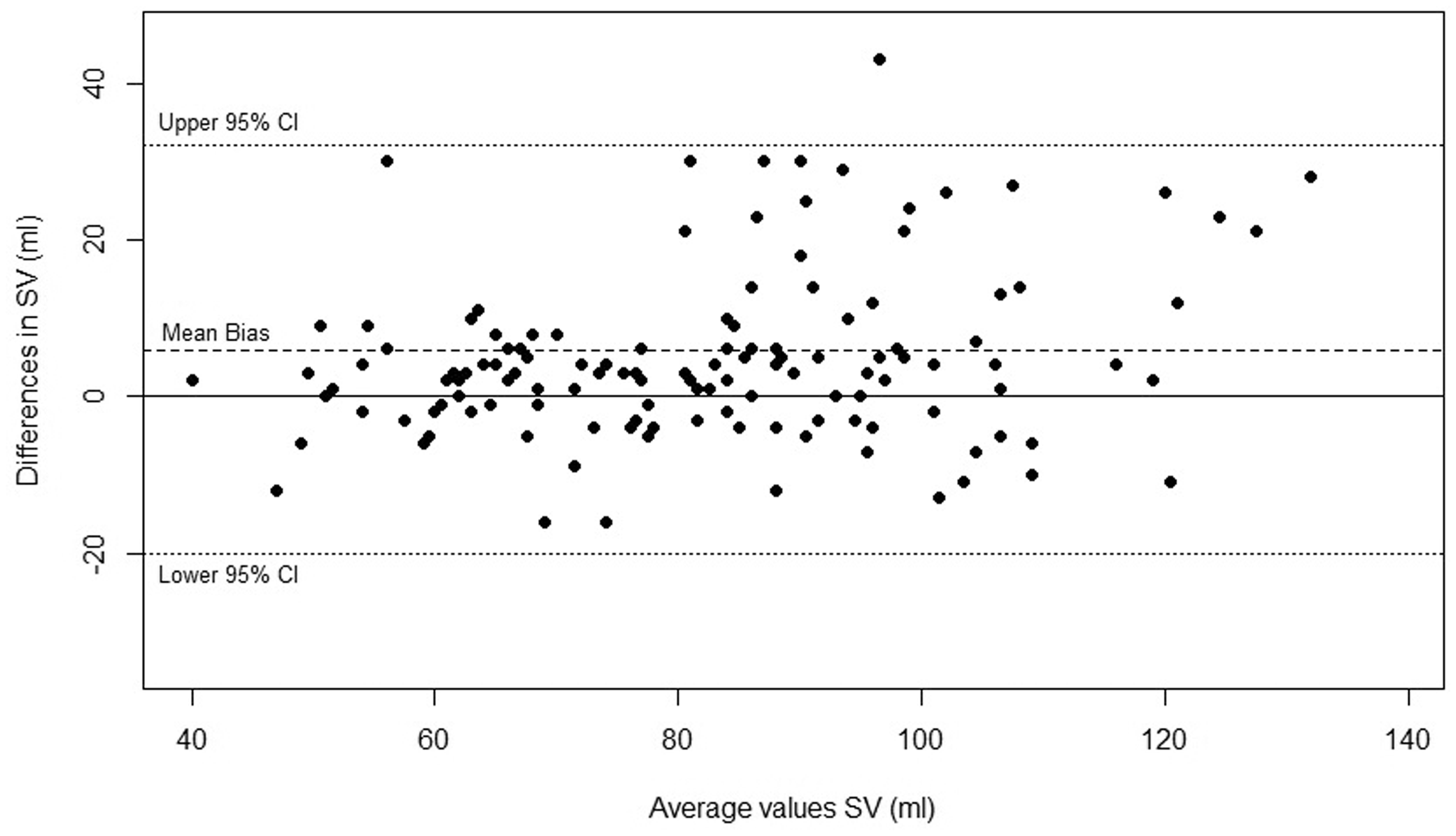
Overall 135 paired observations were obtained and 77 fluid challenges delivered. Median SV values were SVUSCOM 80 (IQR 65–93) and SVODM 86 (69–100). For all paired readings correlation coefficient was R2 = 0.68. 45% of the fluid challenges led to an increase in SVODM ≥ 10%. For SVUSCOM to predict a ≥ 10% increase in SVODM sensitivity was 94% (95% CI 81–99), specificity 88% (74–96)), positive likelihood ratio 7.9 (3.5–18.1) and negative likelihood ratio 0.06 (0.02–0.25). Using SVODM ≥ 10%, the area under the receiver operating curve (AUC) for SVUSCOM was 0.94 (0.90–0.99) (see Figure 1). Concordance following 77 fluid challenges was 91%, and 98% when applying an exclusion zone of ΔSVODM < 10% (Figure 2). Overall percentage of clinical agreement was 87%. Bland-Altman analysis demonstrated an SV mean bias of 5.9 mls (95% limits of agreement −20 to +32) and percentage error 30% (see Figure 3).
Receiver operating curve for SVUSCOM to discriminate a change ≥ 10% in SVODM. Area under the receiver operating curve was 0.94 (95% CI 0.90–0.99). 4-Quadrant scatter plot comparing change (Δ) in SVUSCOM and SVODM readings post fluid challenge (n = 77). A central exclusion zone is drawn to remove statistical noise (ΔSVODM < 10%). Concordance analysis is performed by counting the number of data points lying within the 2 quadrants of agreement (upper right and lower left). Overall concordance = 91% (70/77) and 98% after excluding ΔSVODM < 10%. Bland-Altman Analysis – paired ODM and USCOM stroke volume (SV) readings intra-operatively (n = 135). Mean bias for SV was 5.9 mls (95% limits of agreement−20 to +32) and percentage error 30%.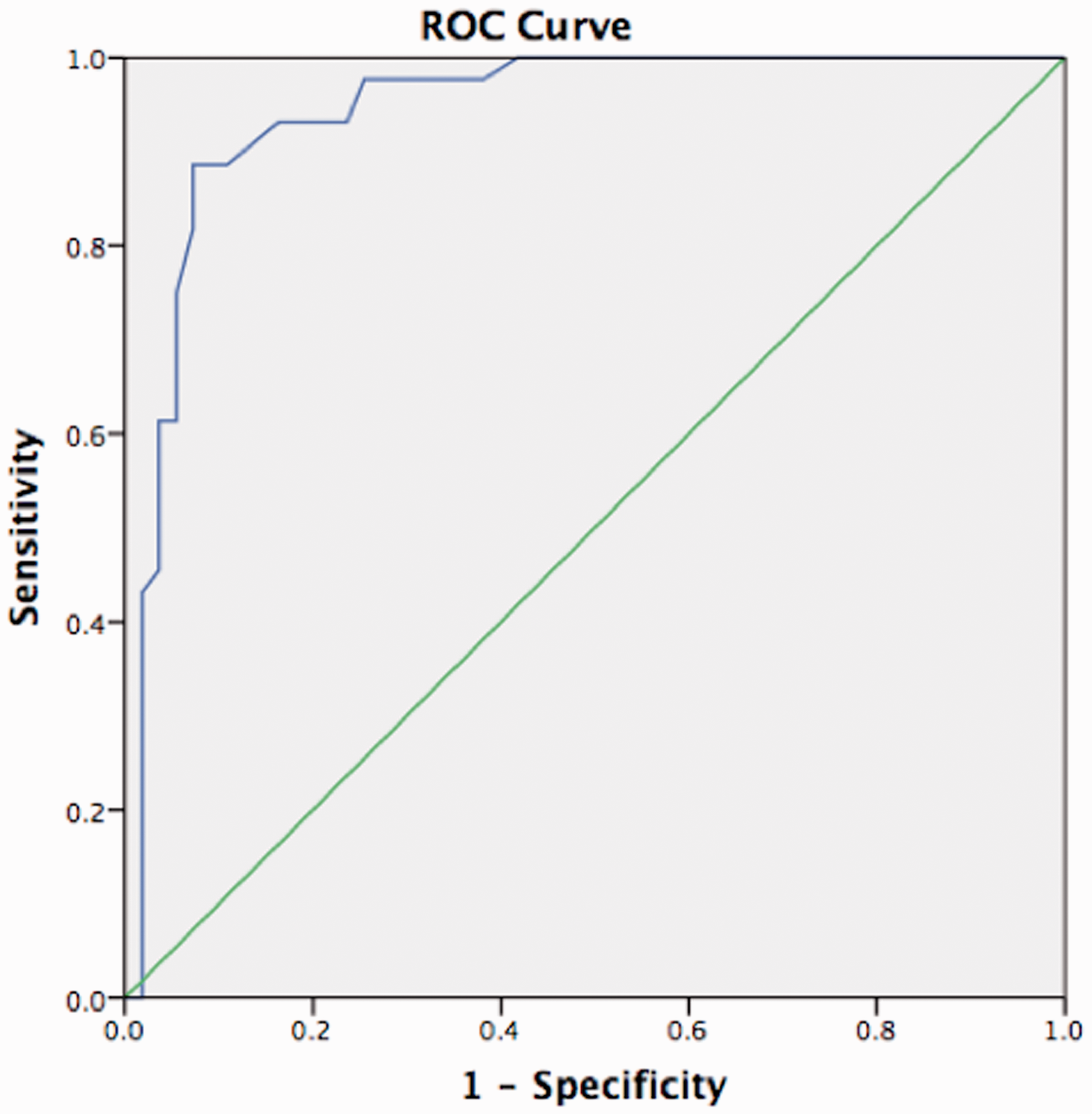
Discussion
During major abdominal surgery following fluid challenges SVUSCOM demonstrated good trending, with a concordance of 98% (using an exclusion zone ΔSVODM < 10%) following a fluid challenge, within the boundaries of acceptability recommended. 31 This replicates the findings of two other recent studies.24,25 The device reliably discriminated a significant change (Δ) in SVODM with an AUC of 0.94 (0.90–0.99). SVUSCOM was found to have a bias of 5.9 mls and percentage error of 30% compared to ODM. This percentage error is at the limit of acceptability often quoted, though this figure has been questioned when comparing two devices that are not gold standard.31,34 Furthermore, in the context of significant haemodynamic fluctuations, with a limited dataset, meant that the study was not primarily designed to drawn conclusions about accuracy of the two devices, though the percentage error is similar to other such studies between the USCOM and OED24,25 and the PICCO (in septic patients). 35
Validation and comparing CO devices is challenging, as no true clinical gold standard exists. The PAC overestimates CO compared to the FICK method in humans36–38 and animals (as measured by the aortic flow probe), in particular in the presence of low CO. 39 Of the 31 studies included in the latest systematic review of the use of GDT perioperatively, the majority used PAC (13) or the ODM (11). From 16 studies, Dark and Singer comparing PAC and ODM, found a pooled median bias of 0.19 l/min (range: −0.69 to 2.00 l/min) for CO. 32 The PAC is now less commonly used, following evidence of lack of benefit and its relatively invasive nature. 40 The ODM, though widely utilised in RCTs, 41 is generally limited to intubated patients and uses a normogram, as a calibration factor, to translate descending aortic stroke distance into an approximation of SV. Transthoracic echocardiography (TTE) requires considerable experience, particularly in the critically ill and lacks outcome studies of clinical benefit. Other non-invasive monitors have been shown to trend with MAP,26,42 with poor concordance compared to the PAC, 43 or are adversely affected by changes in peripheral resistance. 44
A passive leg raise (PLR), leads to an “auto-transfusion” into the central circulation and predicts, with excellent discrimination, whether a subsequent fluid challenge will result in a significant increase in SV. 45 As maximal hemodynamic effects of this manoeuvre occur rapidly, a CO device must likewise allow values to be obtained on a real-time basis. 46 Thiel et al.’s work 47 suggests that the USCOM could be used in this way. Furthermore, in certain cases the USCOM could be of use when the ODM is not employable because of contraindications or difficulty and it is more comfortable when the patient is awake.
In the complex healthcare environment, providing evidence that a device is associated with clinical benefit, is challenging. Indeed, the very nature of fluid boluses and GDT following recent trials13,48 remains an active area of discussion in the field of haemodynamics. To date, the largest body of evidence for CO devices currently supports the use of the ODM. 10 It follows that a device like the USCOM, that can be used in awake patients, using Doppler technology, could potentially be used in further studies, to assess whether it can be used to develop novel evidence-based haemodynamic algorithms, for the benefit of perioperative and acutely unwell patients in critical care, or the emergency department environments. Adoption of such techniques could improve assessment of the circulation in our unstable patients, though whether an impact on outcome is achieved, will depend on how the additional information is used.
Weaknesses of the study and device
The USCOM normogram to predict CSA gives rise to a systematic error between patients that impacts upon accuracy when Bland-Altman comparisons are made against a reference method. 31 Like the ODM, this does not, however, affect information on trending and if valve area has been measured (by TTE) this can be entered into the device. Huang and Critchley 49 found the USCOM to have good repeatability but found increasing age led to difficulties obtaining good quality scans, possibly related to unfolding of the aortic arch and/or cardiomegaly. 50 In our experience, a proportion of elderly patients are more difficult to attain high-quality images that take longer to achieve. However, acceptable images, assessed by the Freemantle criteria 27 were achieved in this study, which included a number of elderly patients (24% aged > 80). Focusing of the probe (visual and acoustic) to obtain the optimal and maximum Doppler signal plays a critical role in all Doppler devices including the USCOM. 51 An improper technique and poor beam alignment with flow at the aortic outflow tract will lead to suboptimal VTI measurements and underestimation of SV.
The number of patients and data points were relatively small and although a number of the patients were high risk, undergoing interventions, they were a relatively stable group of patients. A similar investigation on critically unwell patients on ICU, could further add to the presented study. The USCOM readings were taken by one experienced operator and it must be noted that proper training using the device is crucial, as with any Doppler device. However, the device is more straightforward to use than echocardiography with a learning quoted of (at least) 20 scans. 27 Though good trending was found between the devices, absolute values in this and other studies between devices, demonstrated a degree of bias that should be borne in mind when interpreting, for instance, a low cardiac output state where the device may under, or overestimate a result. In addition, in such situations adequate flow profiles are crucial for correct interpretation of results. However, all other currently available non-invasive cardiac output devices have limitations.26,42–44
Conclusion
During major surgery the USCOM was able to accurately discriminate significant changes in SV as measured by the ODM and showed good concordance with the ODM. Future studies to assess impact on patient outcomes are desirable.
Footnotes
Authors’ contributions
LH: Study design, patient recruitment, data collection, data analysis and writing up of the paper. LF: Study design, data analysis and writing up of the paper.
RV: Study design, writing up of the paper.
TS: Study design, data analysis, writing up of the paper.
HW: Study design, patient recruitment, data collection, data analysis and writing up of the paper.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Wakeling declares receiving honoraria for lecturing and travel expenses to attend meetings from Deltex Medical, Chichester, UK.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.