
Abstract
Euglycaemic diabetic ketoacidosis is a term describing features of diabetic ketoacidosis but with normoglycaemia. We present a case of a perioperative diagnosis of euglycaemic ketoacidosis in a patient not known to be diabetic, and the subsequent management of the patient. A 65-year-old lady was scheduled for re-exploration of a giant paraoesophageal hernia, which had been initially repaired over six weeks previously. She developed dysphagia soon after the initial surgery and had low caloric intake. Arterial blood gases performed intraoperatively revealed metabolic acidosis with a normal lactate level. It did not respond to intravenous fluid therapy and sodium bicarbonate. Euglycaemic ketoacidosis was confirmed with raised serum ketone level. Insulin and dextrose infusions were commenced and she was managed in intensive care unit where the metabolic acidosis resolved over a 12-h period.
Introduction
Diabetic ketoacidosis (DKA) is a complex disordered metabolic state characterised by the triad of ketonaemia, hyperglycaemia and acidosis. 1 It is a well-known complication of diabetes. A less common presentation is euglycaemic diabetic ketoacidosis, with normoglycaemia, rather than hyperglycaemia. This could potentially lead to a delay in diagnosis. We present a case of a perioperative diagnosis of euglycaemic ketoacidosis due to starvation, in a patient who was not known to be diabetic.
Report
A 65-year-old lady was scheduled for re-exploration of a giant paraoesophageal hernia. Her background history included hypertension, hypothyroidism and osteoarthritis. She had had her initial laparoscopic paraoesophageal hernia repair and Nissen fundoplication performed over six weeks previously in another hospital which was reported uneventful and had been discharged home two days postoperatively. She had gradually developed progressive dysphagia one week postoperatively with worsening oral intake. After telephone consultation with the original surgical team, she was readmitted to the hospital, six weeks after her initial surgery. Her computed tomography (CT) scan showed a recurrence of giant paraoesophageal hernia with pooling of contrast in the mid to distal oesophagus. The body of the stomach was in the thoracic cavity. Her case was then discussed with the Upper Gastrointestinal surgeons at our hospital, and she was transferred for further management. She was systemically well with no evidence of sepsis or ischaemia. She underwent a laparoscopic reduction of the hernia on the following day. At laparoscopy, the hiatal sutures were divided and the stomach was reduced which was viable and not ischaemic. The hiatus was very fibrosed with no planes. Therefore, the decision was made to place a 16 Fr gastrostomy tube in the antrum to prevent further herniation. The previous wrap was undone. The greater curvature of the stomach was fixed to the lateral abdominal wall with a continuous V-lock vicryl suture.
ABG analysis intraoperative and immediate postoperative.
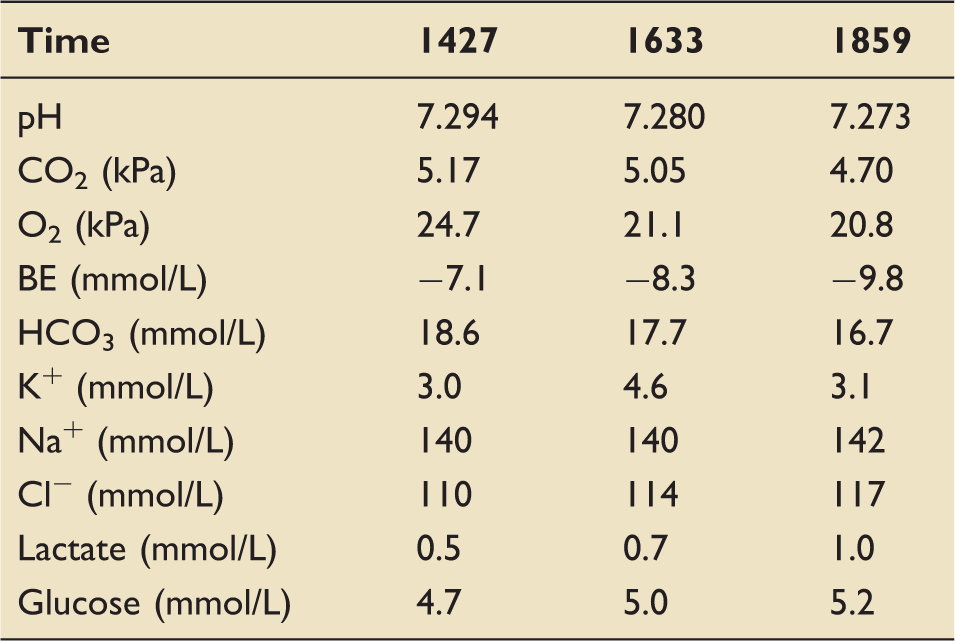
After arrival in recovery, a third ABG was obtained. The metabolic acidosis had worsened further. With the history of recent poor oral intake, euglycaemic ketoacidosis was suspected. The serum ketone level was checked using a point-of-care meter (Precision Xceed Pro, Abbott, Illinois, USA), which revealed significant ketonaemia (5.0 mmol/L). Insulin and dextrose infusions were commenced and she was managed on the ICU. The insulin was infused at a variable rate (between 0.5 and 2 units per hour) to keep the blood glucose level below 10 mmol/L. A 10% glucose infusion was infused at 100 ml/h (10 g/h). She also required 40 mmol potassium supplementation, twice, to keep the plasma concentration of potassium in the normal range.
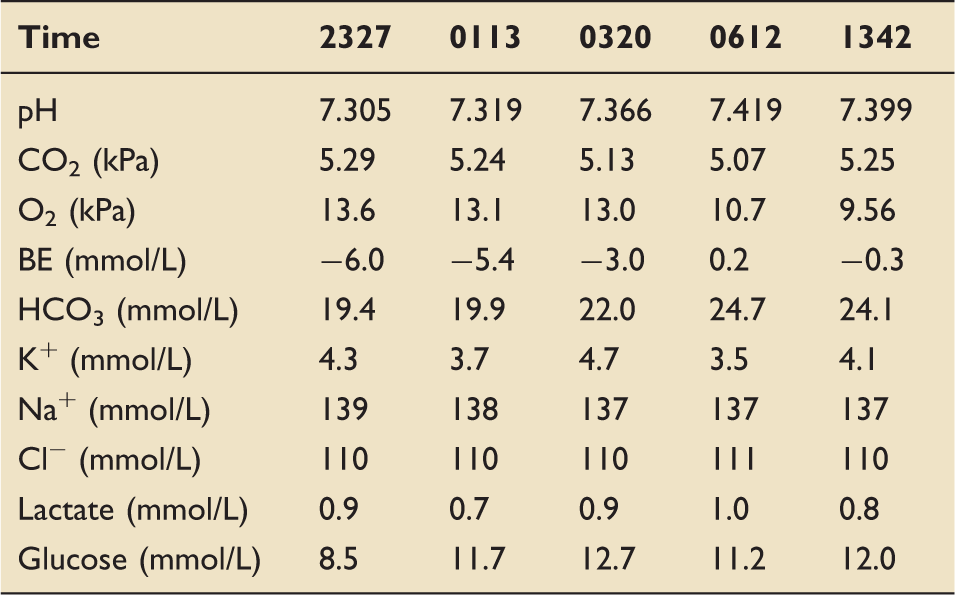
ABG analysis from commencing of insulin and dextrose infusions.
Discussion
The diagnostic criteria for DKA are a ketonaemia of 3 mmol/L or more, blood glucose over 11 mmol/L and acidaemia with a plasma pH less than 7.3, or plasma bicarbonate of less than 15 mmol/L. 1
DKA can also occur where both ketonaemia and acidosis are present but with only modest elevation of blood glucose. This condition is called euglycaemic diabetic ketoacidosis. It was first termed by Munro et al., who described a group of young diabetic patients with severe ketoacidaemia (plasma bicarbonate less than 10 mmol/L) but with blood glucose levels of 16.7 mmol/L or less. 2 The explanation for this condition was that insulin-dependent diabetic patients subjected to a ketogenic state reduced their caloric intake but continued to take insulin. The insulin reduces gluconeogenesis, and increases the cellular utilisation of the limited amount of glucose available. In addition, in patients with adequate renal perfusion, renal glucose excretion may be adequate to maintain normoglycaemia. 3 Lower glucose levels result in fatty acid oxidisation in the liver as an alternate energy source; metabolism of the fatty acids results in ketone bodies. Subsequently, the ketoacidosis and the increase in free fatty acids cause resistance to insulin, 4 which prevents the patient developing hypoglycaemia despite the reduced carbohydrate ingestion. 2 More recently, it has been suggested that the term ‘euglycaemic diabetic ketoacidosis’ be reserved for blood glucose levels less than 11 mmol/L, in line with the current WHO criteria for diagnosing diabetes. 5
Poor nutrition and depletion of carbohydrate reserves over a longer period may also contribute. Joseph et al. 6 described a case of starvation-induced euglycaemic ketoacidosis in a diabetic patient whose depression was severe enough to reduce his appetite and carbohydrate intake sufficiently to cause glycogen depletion and therefore prevent hyperglycaemia.
Euglycaemic ketoacidosis in non-diabetic patients, however, is very rarely reported. Prater and Chaiban 7 described a case of euglycaemic ketoacidosis not known to have diabetes, during an acute admission with pancreatitis. However, the insult to the pancreas may have caused hormonal glycaemic dysregulation.
Causes of euglycaemic ketoacidosis. 6
In our case, euglycaemic ketoacidosis was diagnosed immediately postoperative with raised ketone levels and acidosis but normoglycaemia. Our patient had no history of diabetes and had previously been tested negative. However, she had had low caloric intake for at least six weeks since her first surgery and had developed dysphagia soon after her surgery. Glycogen depletion and lipolysis were therefore perhaps not unexpected. As she was relatively stable in the immediate preoperative phase, an ABG was not performed as part of her anaesthetic assessment. She was kept nil by mouth and received only IV fluid supplementation. It was only from her first ABG results taken intraoperatively that her metabolic acidosis was recognised. Patients can appear well, which may delay the diagnosis and treatment.
We were unable to find specific treatment guidelines for non-diabetic starvation ketoacidosis. Current national guidelines for managing euglycaemic DKA recommend a 10% glucose infusion at 125 ml/h1, above the recommended amount of 50–150 g carbohydrate per day to prevent ketosis.10,11 Fluid replacement may be required but may be less so than in hyperglycaemic states. Fixed rate intravenous insulin infusion (FRIII), at a rate of 0.1 units per kilogram body weight per hour, rather than the variable rate intravenous insulin infusion (VRIII) is recommended in DKA and also in euglycaemic DKA, to suppress ketogenesis. 1 Ketoacidosis probably confers a degree of insulin resistance. 4 In this case, the ketoacidosis resolved over a period of 12 h from initiation of treatment.
We wanted to raise awareness of starvation ketoacidosis as a cause of metabolic acidosis in the perioperative period. Euglycaemic ketoacidosis should be suspected in patients who have recent poor oral intake with unexplained metabolic acidosis despite a normal glucose level. Measuring blood ketone levels with an unexplained acidaemia is important. It can occur within just a few days of a reduced carbohydrate intake. In the absence of specific guidelines, the current recommendations for managing euglycaemic DKA seem prudent for managing starvation ketoacidosis.
Footnotes
Consent
Written consent to publish this article was obtained from the patient.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.