
Abstract
Objective
To investigate the clinical characteristics and long-term mortality of patients with ST-elevation myocardial infarction (STEMI) and non-ST-elevation myocardial infarction (NSTEMI) after orthopaedic surgery.
Methods
This retrospective, single-centre study enrolled patients that underwent inpatient orthopaedic surgery from 2009 to 2017 in Beijing Jishuitan Hospital. The patients were screened for a cardiac troponin I elevation and fulfilled the Fourth Universal Definition of Myocardial Infarction within 30 days of surgery.
Results
A total of 180 patients that developed perioperative myocardial infarction (MI) were included in the study. Among them, 14 patients (7.8%) were classified as STEMI, and 166 (92.2%) had NSTEMI. Compared with those with NSTEMI, STEMI patients had significantly higher 30-day and long-term mortality rates (50.0% versus 5.4%; 71.4% versus 22.3%; respectively). Multivariate Cox regression model analysis among the entire cohort demonstrated that STEMI (hazard ratio [HR] 5.78, 95% confidence interval [CI] 2.50, 13.38) and prior MI (HR 2.35, 95% CI 1.02, 5.38) were the most significant independent predictors of long-term mortality.
Conclusion
Perioperative MI after orthopaedic surgery was associated with a high mortality rate. STEMI was independently associated with a significant increase in short- and long-term mortality.
Introduction
Orthopaedic surgery is the most common non-cardiac surgical procedure, and as populations age, more orthopaedic procedures are performed worldwide. 1 Many orthopaedic patients are elderly and have multiple medical comorbidities. 2 Orthopaedic surgeries have been considered to carry an intermediate risk of death and nonfatal myocardial infarction (MI), 3 so a careful preoperative cardiac risk assessment can improve patient outcomes. 4 Although the efforts to prevent the occurrence of perioperative adverse events, cardiovascular complications are still the leading cause of morbidity and mortality in the perioperative period.5–7 The Fourth Universal Definition of Myocardial Infarction (UDMI) proposed a new definition of myocardial injury. 8 Myocardial injury was defined as an elevated troponin level above the 99th percentile. 8 Various causes had been suggested for myocardial injury, including myocardial ischaemic or nonischaemic conditions. 8 The diagnosis of acute MI highlighted the presence of acute myocardial injury detected by abnormal cardiac biomarkers in the setting of the evidence of acute myocardial ischaemia. 8 Large database analyses have reported that perioperative myocardial injury was associated with an increased mortality in a concentration-dependent manner.7,9–11 A recent study reported that in elderly patients with hip fracture, a troponin rise without MI was not associated with a significant increase in 6-month mortality. 12 While it is well understood that perioperative MI after non-cardiac surgery has substantial risks for both serious cardiovascular events and short- and long-term mortality.4,7,9,13
Perioperative MI that occurs after non-cardiac surgery is a unique disease entity with distinct epidemiology and outcomes compared with spontaneous MI. 8 According to the presenting electrocardiogram (ECG), acute MI has been classified into ST-elevation myocardial infarction (STEMI) and non-ST-elevation myocardial infarction (NSTEMI). 8 However, there are no data comparing the clinical characteristics and long-term mortality of patients with STEMI and NSTEMI after orthopaedic surgery. This current study investigated the clinical characteristics and long-term mortality of patients with STEMI and NSTEMI after orthopaedic surgery in a tertiary referral orthopaedic centre in China.
Patients and methods
Patient population
This single-centre retrospective study enrolled consecutive patients undergoing hip, knee, spine or orthopaedic trauma procedures at the Department of Orthopaedics, Beijing Jishuitan Hospital, Beijing, China, a 1500-bed tertiary referral orthopaedic centre, between January 2009 and December 2017. The hospital administrative database was screened to identify all perioperative patients with troponin I levels above the 99th percentile of the upper reference limit (>0.04 μg/l) within 30 days of surgery. Beginning with the UDMI as a case definition, 8 the initial list of patients was reviewed case by case in order to identify patients that fulfilled the criteria of MI. The inclusion criteria were as follows: (i) aged ≥50 years; (ii) underwent orthopaedic surgery under general or spinal anaesthesia; (iii) had an expected postoperative length of hospital stay of at least 24 h; (iv) fulfilled the criteria of MI. The exclusion criteria were as follows: (i) age <50 years; (ii) cardiac-related procedures (such as pacemaker insertion); (iii) surgery under local anaesthesia; (iv) cases with a rise and/or fall in serum troponin but without clinical evidence of ischaemia; (v) evidence of ischaemic myocardial injury but did not fulfil the criteria of MI (e.g. tachyarrhythmia); (vi) troponin I elevation attributed to nonischaemic reasons (e.g. pulmonary embolism, myocarditis, renal failure); (vii) cases with elevated serum troponin levels before surgery; (viii) cases with only one troponin value. Serum troponin assays were performed according to the decisions of clinicians. In most cases, the measurement of troponin I and an ECG were obtained due to changes in clinical status (e.g. hypotension, hypoxaemia and/or altered mental status) or in response to specific patient complaints (e.g. chest pain, dyspnoea or palpitations). In patients with troponin elevation, troponin I levels were assayed every 24 h for 72 h or until the troponin level fell below the level of 0.04 μg/l.
The study was approved by the Institutional Ethics Committee of Beijing Jishuitan Hospital, Beijing, China (no. 201905-05). All the patients participating in the study provided written or verbal informed consent.
Data collection
Data on demographic characteristics, medical history, procedural details, symptoms, cardiac biomarker concentrations, ECG changes, medications used and transfusion requirements were collected. All clinical details were adjudicated by two clinicians (W.H. & J.W.) and a third senior adjudicator (X.Z.) was consulted in case of disagreement. Perioperative MI was defined as a rise/fall of troponin I above the 99% upper reference limit (0.04 μg/l) in conjunction with ≥1 of the following: (i) symptoms of ischaemia; (ii) new ischaemic ECG changes; (iii) development of pathological Q waves on the ECG; (iv) imaging evidence of a new loss of viable myocardium or new regional wall motion abnormality. 8 Acute MI was categorized as STEMI or NSTEMI according to the universal definition of MI. 8 The primary endpoint of the study was all-cause mortality.
Patient conditions that possibly provoked or were associated with myocardial ischaemia were recorded. Postoperative anaemia was defined as haemoglobin <9.0 g/dl. Perioperative hypotension was defined as a mean arterial pressure < 65 mmHg. Severe arterial hypertension was defined as the presence of a systolic blood pressure ≥180 mmHg or a diastolic blood pressure ≥110 mmHg. Respiratory failure was defined as an arterial oxygen tension <8 kPa in conjunction with clinical signs of acute respiratory failure lasting 20 min. If the treating physician thought the myocardial ischaemia was attributable to dysrhythmia, then tachyarrhythmia or bradyarrhythmia was recorded as a provoking factor, but threshold heart rates for tachyarrhythmia or bradyarrhythmia were not defined.
Statistical analyses
All statistical analyses were performed using IBM SPSS Statistics for Windows, Version 20.0 (IBM Corp., Armonk, NY, USA). Continuous variables are presented as mean ± SD if normally distributed and median (inter-quartile range [IQR]) if not normally distributed. Differences in continuous variables were compared using a Student’s t-test for normally distributed continuous variables and a Mann–Whitney U-test for not normally distributed continuous variables. Categorical variables were shown as frequencies and percentages and compared using χ2-test and Fisher’s exact tests. Kaplan–Meier survival analyses were performed to compare survival probabilities between types of MI. A log-rank test was used to determine statistical significance. Multivariate logistic regression analysis was implemented to determine the predictors of 30-day and long-term mortality among the patients with perioperative MI. The cause-specific hazard ratio (HR) and corresponding 95% confidence interval (CI) for patients with STEMI versus NSTEMI were calculated by using univariate Cox regression models. Cox regression models were also adjusted for age, sex, prior MI and the Revised Cardiac Risk Index score. A P-value < 0.05 was considered statistically significant
Results
After screening 34 901 patients that underwent orthopaedic surgery during the study period, troponin I was detected in 5897 patients (16.9%); of these, 180 patients had elevated serum troponin I levels (>0.04 μg/l) and met the criteria of MI within 30 days of surgery (3.1% of patients that had a troponin measured and 0.5% of overall). The flow diagram for the study population is shown in Figure 1.

Study flow chart showing the numbers of patients screened and the final study population. MI, myocardial infarction; STEMI, ST-elevation myocardial infarction; NSTEMI, non-ST-elevation myocardial infarction.
The median age of the180 patients was 71.0 years and 124 (68.9%) were female. A diagnosis of coronary artery disease was made in 84 patients (46.7%) and 31 (17.2%) had a prior history of angina within 6 months before surgery. Twenty patients (11.1%) had a troponin I measurement before surgery and the troponin I levels were in the normal range. On the basis of the UDMI, 14 patients (7.8%) were classified as STEMI and 166 patients (92.2%) were classified as NSTEMI. Table 1 presents the baseline demographic and clinical characteristics of the study population. Coronary artery disease and prior angina within 6 months were significantly more frequent among STEMI patients than NSTEMI patients (12 of 14 [85.7%] versus 72 of 166 [43.4%], P = 0.002; six of 14 [42.9%] versus 25 of 166 [15.1%], P =0.023; respectively). Patients in the STEMI group had a significantly lower proportion of females (5 of 14 [35.7%] versus 119 of 166 [71.7%], P = 0.013) and were more likely to have their antiplatelet medications discontinued on admission (six of 14 [42.9%] versus 21 of 166 [12.7%], P =0.008) than the NSTEMI group. Among patients with STEMI, the median peak postoperative troponin I was 6.30 μg/l (IQR 2.83–12.79 μg/l), which was significantly higher than that of the NSTEMI patients (0.36 μg/l; IQR 0.11–2.06 μg/l; P < 0.001).
Baseline demographic and clinical characteristics of patients (n = 180) that underwent orthopaedic surgery and experienced a perioperative myocardial infarction (MI) stratified according to the classification of the MI as ST-elevation myocardial infarction (STEMI) or non-ST-elevation myocardial infarction (NSTEMI).

Data presented as median (interquartile range) or n of patients (%).
aBetween-group differences in continuous variables were compared using Mann–Whitney U-test. Categorical variables were compared using χ2-test and Fisher’s exact tests; NS, no significant between-group difference (P ≥0.05).
In all patients with perioperative MI, only 24 of 180 (13.3%) reported chest pain and 79 of 180 (43.9%) presented with atypical clinical symptoms such as dyspnoea or shortness of breath (Table 2). A total of 31 of 180 (17.2%) patients experienced clinically silent events. ECG changes consistent with myocardial ischaemia were observed in 108 of 180 (60.0%) patients. Eight of 180 (4.4%) patients presented in cardiogenic shock. The majority of patients (143 of 180; 79.4%) developed perioperative MI within the first 3 postoperative days; 26 of 180 (14.4%) patients on the day of surgery; and two perioperative MIs occurred after hospital discharge.
Clinical presentation, electrocardiogram changes and mortality of patients (n = 180) that underwent orthopaedic surgery and experienced a perioperative myocardial infarction (MI) stratified according to the classification of the MI as ST-elevation myocardial infarction (STEMI) or non-ST-elevation myocardial infarction (NSTEMI).
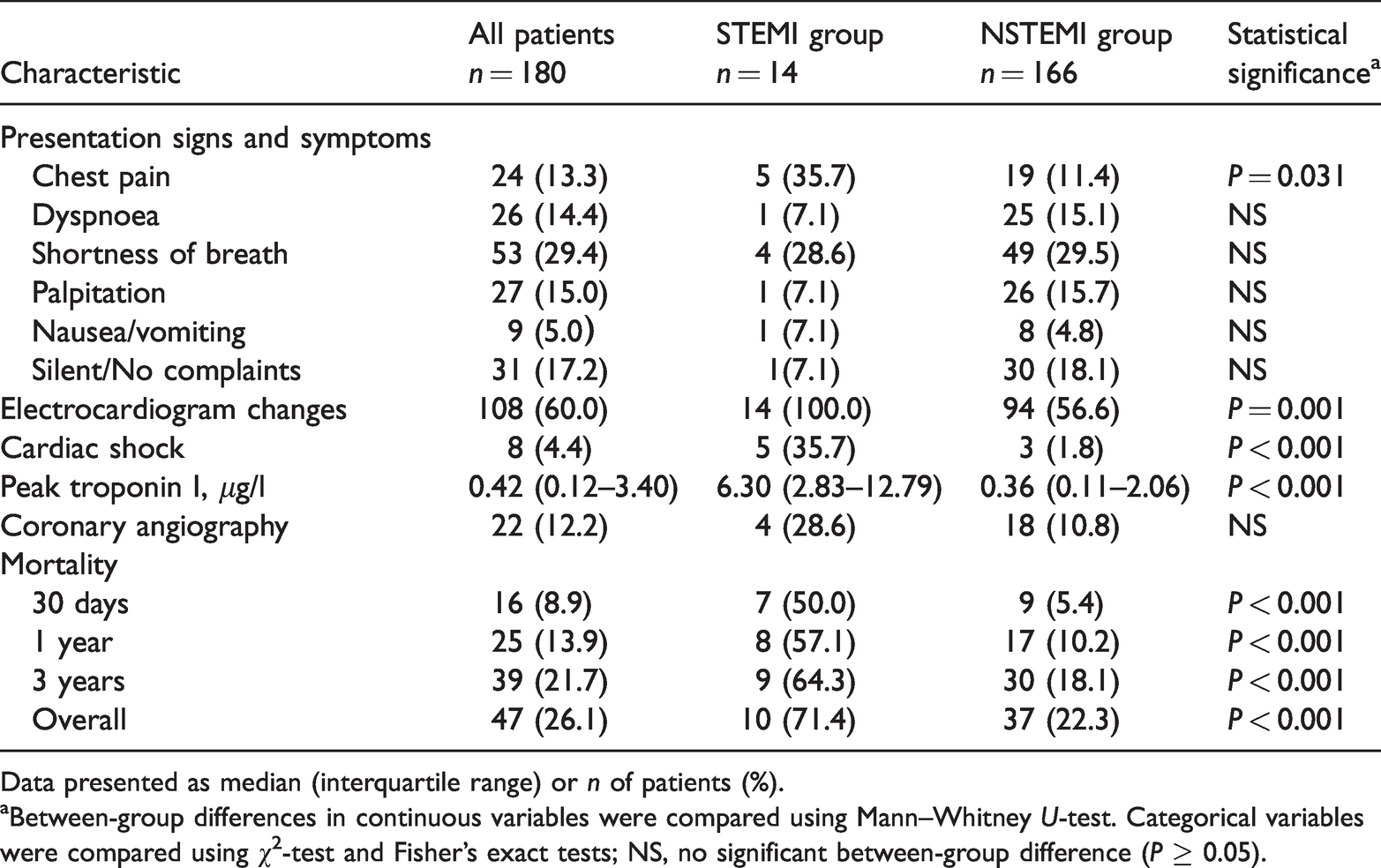
Data presented as median (interquartile range) or n of patients (%).
aBetween-group differences in continuous variables were compared using Mann–Whitney U-test. Categorical variables were compared using χ2-test and Fisher’s exact tests; NS, no significant between-group difference (P ≥ 0.05).
Postoperative complications or conditions that possibly provoked or were associated with myocardial ischaemia are shown in Table 3. The three most common complications underlying myocardial ischaemia were anaemia, heart failure and respiratory insufficiency. At least two different mechanisms were involved in some patients. Postoperative anaemia was present in 79 of 180 patients (43.9%); with haemoglobin < 9.0 g/dl and a median haemoglobin decrease of 4.3 ± 1.9 g/dl was observed prior to or within 24 h of the peak serum troponin.
The postoperative complications or clinical conditions that might have provoked myocardial ischaemia in patients (n = 180) that underwent orthopaedic surgery and experienced a perioperative myocardial infarction.

Data presented as n of patients (%).
COPD, chronic obstructive pulmonary disease.
Most patients that developed a perioperative MI were asymptomatic or experienced atypical ischaemic symptoms (Table 2). As a result, perioperative MI was recognized late or not recognized at all. A cardiologist was consulted in 98 of 180 patients (54.4%). Among the 166 adjudicated as NSTEMI, only 63 (38.0%) were clinically diagnosed and treated by the clinical teams; and the remaining 103 patients (62.0%) were neglected.
Coronary angiography was performed in 22 of 180 patients (12.2%), including three patients with STEMI and 19 patients with NSTEMI. One patient suffered cardiac arrest in the catheterization laboratory and died within 24 h of percutaneous coronary intervention (PCI). Four patients did not have obstructive lesions (<50% stenosis in the left main artery or <70% stenosis for all other arteries). Acute coronary thrombosis was adjudicated in two patients with STEMI. Fifteen patients had obstructive lesions (≥50% stenosis in the left main artery or ≥70% stenosis for all other arteries), among them left main disease (≥50% stenosis) was present in three patients and totally occluded lesions were present in six patients.
In patients with STEMI, the most common reason for not being referred for cardiac catheterization was excessive comorbidities and critical condition. One patient died during transportation to the cardiac catheterization laboratory. While in patients with NSTEMI, the main reason for not pursuing a cardiac catheterization was that it was against the family and/or the patient’s wishes (53 of 166; 31.9%). Other reasons included excessive comorbidities, critical primary condition, active or excessive risk of bleeding and high risk of kidney injury.
Overall, a total of 163 patients (90.6%) survived to hospital discharge. At the time of hospital discharge, aspirin was prescribed in 73 of 163 patients (44.8%), clopidogrel in 62 of 163 patients (38.0%), a statin in 78 of 163 patients (47.9%), a beta-blocker in 58 of 163 patients (35.6%) and an angiotensin-converting enzyme inhibitor (ACEI) or angiotensin receptor blocker (ARB) in 43 of 163 patients (26.4%) (Table 4). Only 70 of 163 patients (42.9%) were discharged on a combination of aspirin and a statin. Twenty-five of 163 patients (15.3%) received prescriptions for aspirin, a statin, a beta-blocker and ACEI therapy at discharge.
Drug therapy at discharge in patients (n = 163) that underwent orthopaedic surgery and experienced a perioperative myocardial infarction.

Data presented as n of patients (%).
ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker; DAPT, dual antiplatelet therapy (aspirin + P2Y12 inhibitor).
The median follow-up duration was 3.7 years and a total of 47 deaths from any cause (26.1%) were observed. Patients with STEMI had worse outcomes than patients with NSTEMI. The 30-day death rate in the STEMI cohort was 50% (seven of 14 patients; 95% CI 20%, 80%) and 5.4% (nine of 166 patients; 95% CI 1.9%, 8.9%) in the NSTEMI cohort (Table 2). The overall long-term mortality rate was also significantly higher for patients with STEMI compared with those with NSTEMI (10 of 14 patients [71.4% ; 95% CI 44.4%, 98.5%] versus 37 of 166 patients [22.3%; 95% CI 15.9%, 28.7%] respectively, P < 0.001).
Stepwise logistic regression model analysis revealed STEMI (odds ratio [OR] 15.78; 95% CI 4.20, 59.21; P < 0.001) and prior MI (OR 7.58; 95% CI 1.75, 32.81; P =0.007) were independent predictors of all-cause mortality at 30 days. STEMI (OR 7.18; 95% CI 1.88, 27.45; P = 0.004), male (OR 2.43; 95% CI 1.07, 5.53; P = 0.034), age ≥70 years (OR 3.82; 95% CI 1.52, 9.62; P = 0.004) and orthopaedic trauma (reference) were associated with an increased risk of long-term mortality.
Multivariate Cox regression model analysis among the entire cohort demonstrated that STEMI (HR 5.78, 95% CI 2.50, 13.38; P < 0.001) and prior MI (HR 2.35, 95% CI 1.02, 5.38; P = 0.044) were the most significant independent predictors of long-term mortality (Table 5). Kaplan–Meier curves of long-term survival among patients with STEMI or NSTEMI are shown in Figure 2.
Cox proportional hazard model* for long-term mortality among patients with ST-elevation myocardial infarction (STEMI) and non-ST-elevation myocardial infarction.

*Adjusted for all significant variables in the univariate analysis.

Kaplan‒Meier survival curves illustrating the risk of long-term death from any cause shown for patients (n = 180) that underwent orthopaedic surgery and experienced a perioperative myocardial infarction (MI) stratified according to the classification of the MI as ST-elevation myocardial infarction (STEMI) or non-ST-elevation myocardial infarction (NSTEMI).
Discussion
This current retrospective study of patients that developed perioperative MI within 30 days after orthopaedic surgery demonstrated the following results: (i) > 90% perioperative MI presented as NSTEMI; (ii) the most common triggering factors associated with perioperative MI were anaemia, heart failure and respiratory insufficiency; (iii) STEMI was associated with significantly higher short- and long-term mortality (50% 30-day mortality and 71% long-term mortality); (iv) STEMI was a strong independent predictor of long-term mortality in the general cohort.
The pathophysiological mechanism of perioperative MI after noncardiac surgery involves two potential mechanisms. One is caused by plaque destabilization, rupture and thrombosis within the coronary artery (type 1 MI); and the other is a consequence of an imbalance between myocardial oxygen supply and demand (type 2 MI). Postoperative tachycardia, anaemia, hypoxaemia and haemodynamic instability may initiate pathways causing more type 2 MI. 8 In contrast, the complex pathophysiology associated with operative interventions including volume overload, an increased prothrombotic state and surgical stress may also exacerbate a ‘supply and demand’ mismatch. 5
The current data showed perioperative MI occurred in 3.1% of patients with troponin I measured and in 0.5% of the whole population. Several previous studies have investigated the incidence of perioperative MI after orthopaedic surgery. For example, a previous study reported a 13.8% incidence of MI in a cohort of 1212 elderly patients undergoing hip fracture surgery. 14 In another study, the rate of clinically verified MI during the first 7 days following surgical repair of a hip fracture was 10.4%. 15 Both these studies investigated an older population undergoing hip fracture surgery.14,15 In a study of 3050 patients undergoing hip, knee or spine surgery, the incidence of perioperative MI was 0.7%. 13 A review of 1098 elective orthopaedic surgeries demonstrated that the combined incidence of perioperative MI, death and cardiac arrest was 0.9%. 16 These previous results were similar to those of the current study.14–16 Another study reported a postoperative MI incidence of 1.2% in patients with cardiac risk factors and 0.09% in all patients undergoing major orthopaedic surgery. 17 This was slightly lower than the incidence of 0.5% for a perioperative MI in the current study. In this study, a value of troponin I ≥ 0.1 μg/l (five-times the reference levels) was used to diagnose MI, which may have underestimated the incidence of MI.
These current results also confirmed previous findings that perioperative MI occurred mainly within the first 3 days of the procedure. Most of the events were NSTEMI and the majority were asymptomatic or were associated with a lack of typical chest pain.7,10,18–20 Previous studies have shown that more than 80% of perioperative myocardial injury or MI would have gone undetected without routine troponin screening.7,11,21,22 In the current study, even with postoperative troponin I elevation, most of the patients adjudicated as NSTEMI were still ignored in routine clinical practice.
There are certain scenarios in distinguishing type 1 from type 2 MI particularly in the setting of MI after non-cardiac surgery. Angiographic characteristics in patients with perioperative MI are not yet fully understood. Some angiographic investigations have identified coronary plaque rupture and acute coronary thrombosis in 50–60% of patients with perioperative MI (type 1 MI).23,24 However, more studies advocated that most perioperative MI events were adjudicated as demand ischaemia (type 2 MI).18,19 A previous study that explored 281 patients undergoing diagnostic coronary angiography for MI after noncardiac surgery showed a 22% PCI rate due to acute coronary thrombosis among 1093 patients with acute coronary syndrome after noncardiac surgery. 18 Another study also found a 73% rate due to demand ischaemia in 146 patients with acute coronary syndrome after screening 215 077 patients undergoing noncardiac surgery. 19 In this current study, only 22 (12%) patients received coronary angiography; while demand ischaemia was seen more often, a thrombotic event (type 1 MI) was adjudicated in only two patients. In contrast, these current results also suggested that anaemia, heart failure and respiratory insufficiency were the most prevalent mechanisms underlying myocardial ischaemia. Anaemia was associated with increased morbidity and mortality in several clinical contexts such as MI, heart failure and noncardiac surgery. 20 In the present study nearly a half of perioperative MIs experienced postoperative anaemia. A previous study found that postoperative anaemia (<8.0 g/dl) among elderly patients was associated with a 3.5-fold increase in hospital mortality after hip fracture. 14 The current data supported that in most cases of perioperative MI as myocardial necrosis seemed to be triggered by a supply-demand mismatch attributable to anaemia, heart failure and respiratory failure rather than plaque rupture.5,24,25 This also indicated that the dominant underlying pathophysiological mechanisms and the associated optimal management of patients with perioperative MI are presumably fundamentally different from that of patients with spontaneous MI.
In the current cohort, the patients had a high mortality rate (8.9% 30-day mortality and 13.9% 1-year mortality). This mortality rate was comparable with previous published reports for patients undergoing noncardiac surgery.7,13,18,19 The Perioperative Ischemic Evaluation (POISE) trial demonstrated a 30-day mortality rate of 11.6% among patients with a perioperative MI after noncardiac surgery and 2.2% among patients who did not, but long-term outcomes were not reported. 7 Findings from two studies in patients undergoing coronary angiography after perioperative MI showed that 30-day mortality was 5.2–7.0% and 1-year mortality was 14–15%.18,19 But another study described a 30-day mortality of 17.4% and 1-year mortality of 39.5% in an elderly patients (mean age, 85.3 years) with MI undergoing hip fracture surgery. 14 A 1-year mortality rate of 35.8% was reported in elderly patients with clinically verified MI after surgical repair of a hip fracture. 15 The high degree of mortality in the hip fracture population may be partially because of an older age and a higher burden of cardiovascular risk factors. All these data suggested that perioperative MI increases the risk of all-cause death ≤1 year.7,13,14,18,19 A previous study described a long-term (3 years) mortality rate of 16.8% in patients with myocardial necrosis and 5.8% in those with a troponin level in the normal range. 13 This previous study enrolled all patients with perioperative troponin elevation, including those with isolated troponin elevation and perioperative MI. 13
In the present study, perioperative MI after orthopaedic surgery had a high long-term (median follow-up of 3.7 years) mortality rate of 26% and STEMI was the most significant independent predictor of long-term mortality (HR 5.78, 95% CI 2.50, 13.38). The 30-day mortality rate with STEMI was 50%, approximately 10-fold higher than with NSTEMI. STEMI was also associated with a 3.2-fold increased risk of long-term mortality compared with NSTEMI, which was consistent with previous studies showing that mortality is much higher in patients that experienced STEMI compared with NSTEMI.18,19 A previous study reported a 30-day mortality rate of 31.2% in a STEMI cohort and 8.5% in a NSTEMI cohort in patients undergoing PCI for MI after noncardiac surgery. 18 In-hospital mortality for patients that developed in-hospital STEMI was between 8% and 66%. 26
Despite of the incidence and the associated worse outcomes of perioperative MI, it is unclear how to manage these patients with MI after noncardiac surgery. Some observational studies suggested that aspirin and statins might be beneficial in preventing death and major cardiac complications in patients with perioperative MI,7,27 but this has not been assessed in randomized clinical trials. In a sub-study of the POISE trial, the use of aspirin was associated with a 46% reduction in the risk for 30-day mortality and lipid-lowering therapy with statins was associated with a 76% reduction among patients with perioperative MI. 7 A small observational study demonstrated that patients with postoperative MI that did not receive intensive medical therapy (aspirin, statin, beta-blocker, ACEI) had higher rates of cardiovascular events at 1 year (HR 2.80, 95% CI 1.05, 24.2). 27 Thus, the Canadian Cardiovascular Society perioperative guidelines recommended initiating aspirin and statin therapy in patients that experience myocardial injury or MI after noncardiac surgery. 28 Recent clinical trials have evaluated novel approaches to the treatment of this patient population. For example, the MANAGE trial, which is an international, randomized, placebo-controlled trial, found that among patients aged ≥45 years with myocardial injury after noncardiac surgery, dabigatran 110 mg twice daily significantly reduced the risk of major vascular complications by approximately 25%. 22 Based on these findings, 22 it is reasonable to assume that patients may benefit from basic cardiac medication for the secondary prevention of MI after noncardiac surgery. However, the current results, consistent with a previous study, 29 showed that in clinical practice the proportion of patients with perioperative MI prescribed basic cardiac medical therapy remained low.
Although the role of revascularization in the setting of acute coronary syndrome is well established, performance of PCI and coronary artery bypass graft surgery in the setting of early postoperative MI is challenging due to patient comorbidities and relatively higher bleeding risk. Furthermore, the role of PCI as a treatment modality is unclear partly due to lack of quality data on outcomes in these patients.18,19 Thus, it is always difficult to weigh the risk/benefit ratio of making decisions of invasive strategy with early revascularization. Prior studies have shown that only 22–56% of in-hospital STEMI patients undergo PCI, a rate much less than seen with out-of-hospital STEMI.26,30 In-hospital mortality was equally high in both thrombotic and nonthrombotic groups given the different utilization rates of PCI (95% versus 29%); 30 and delays in treatment may partially account for the high mortality rate in patients with thrombotic in-hospital STEMI. Perioperative MI has a markedly high mortality rate even after PCI. 18 Additional efforts are warranted to determine the best treatment strategy in this population.
There were some limitations to the present study that need to be considered. First, it was a single-centre retrospective study. Although the sample size of 180 was collected from more than 34 000 orthopaedic surgeries at our hospital, it was still rather small and prone to bias. Secondly, the age criterion of ≥50 years in the study protocol may have resulted in potentially increased morbidity or mortality rate. Thirdly, the schedule for troponin I measurement was not standardized, which may increase the risk of measurement bias with any change in physician ordering patterns. The study may have also missed additional asymptomatic MIs. Fourthly, troponin I elevations may occur in patients with renal failure or other cardiovascular conditions such as takotsubo cardiomyopathy. As most of the perioperative MIs were adjudicated as type 2 MI, the lack of clear consensus regarding the exact diagnostic criteria of type 2 MI caused subjectivity in the diagnosis. Fifthly, patients with troponin I elevation before surgery were excluded, which may result in missing patients with preoperative MI.
In conclusion, this current study demonstrated that perioperative MI has a markedly high mortality rate. The development of STEMI after orthopaedic surgery was associated with worse short- and long-term survival compared with NSTEMI; being approximately 1 in 2 patients versus 1 in 20 patients that did not survive beyond 30 days after STEMI and NSTEMI, respectively. STEMI was also a significant and independent predictor of long-term mortality. Perioperative MI is a major healthcare problem, but there is no clear consensus regarding the exact definition of perioperative MI after noncardiac surgery and data are scant on how patients with perioperative MI are treated in clinical practice, therefore perioperative MI often remains unrecognized. Ultimately, this current study highlights the urgent need for additional efforts aimed at improving the clinical diagnosis and establishing strategies to prevent and treat this important complication of noncardiac surgery.