
Abstract
Chest drains are common on intensive care units for a wide variety of clinical conditions. Despite this, there are no published data on their use within the intensive care unit and minimal published literature to guide decision making regarding the timing of their removal. Therefore, we undertook an audit to review our experience over one year, as to the degree of variability in when chest drains were removed. Using our electronic observation records, we assessed the length of stay of our chest drains against their functionality by whether they remained swinging (i.e. in connection with the pleural space) and whether they had a pathological fluid output (>150 mL/24 h). We found that our drains had a mean duration of 5.89 days, and that one-quarter remained in place for three days despite being non-functional. To conclude, we have devised a three-stage assessment (using the acronym I-T-U), to help guide an intensivist in the safe and timely removal of a chest drain.
Introduction
Chest drains were first documented for the treatment of empyema by Hippocrates. He described the process of incising the chest and inserting a metal tube to allow drainage. 1 However, chest drains only became commonly used during the 1918 flu pandemic. The pandemic was complicated by a ‘haemolytic streptococci’ pneumonia (now known as a group-A streptococci) which was marked by an extensive haemolytic pleural effusion. This was treated by early surgical rib removal and insertion of pleural drain. This high-risk procedure had a very high mortality often occurring within 30 min. The mortality was probably in part due to the lack of appreciation at this time that the pleural space is at negative pressure, and therefore, there was no routine use of under-water seals.2,3 It was then only during the Second World War and Korean War that chest drains became commonly used in traumatic chest injuries. 4
Now of course chest drains are a common phenomenon throughout the hospital, regularly being used to treat empyema, pleural effusions, pneumothoracics, haemothorax and for post-surgical prophylaxis. Importantly, however, it is only within the intensive care unit (ICU) setting that this wide variety of clinical indications is seen in one location. To illustrate this, we audited our local one-year experience in chest drains, and as shown in Figure 1, the indications are indeed varied. The commonplace of chest drains is recognised by the ICU curriculum which insists trainees to learn techniques for their insertion. Yet, despite their prevalence, there is little guidance on when to remove them.
Indication for chest drain insertion.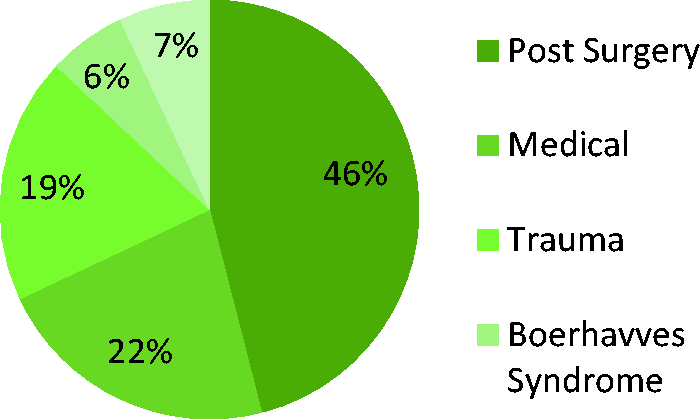
Reviewing both national guidelines and published literature, it is easy to find clear advice on how and when to consider inserting chest drains.5,6 However, there is little to no evidence about when their removal should be considered. For example, the British Thoracic Society provides the general statement that drains for pleural infection should be removed when there is radiological improvement and evidence of sepsis resolving. 5 A more recent review primarily looking at surgical chest drains states that there is no clear evidence as to when to remove chest drains, although their removal appears well tolerated even with flows of 500 mL per day. 7 However, the authors did conclude that there was moderate evidence to suggest the routine use of low-grade suction. Similarly, within the trauma literature there is some evidence that low-grade suction decreases repeat pneumothorax rates8–10 but again there is no specific guidance on when to remove the chest drains themselves. Finally, more general literature appears to suggest removal once drain output is between 100 and 300 mL/day. 11
Given the paucity of guidance regarding the removal of chest drains and their common occurrence within the ICU, we will review the rationale for their timely removal, the basic knowledge required to assess their removal and then put forward a generalisable approach that the intensivist can use when assessing whether or not to remove a chest drain. In this article, we will illustrate the current variation in the practice of removing chest drains by embedding data from our one-year retrospective audit of chest drain removal at the general adult ITU of the Oxford University Hospitals NHS Trust.
The rationale for timely removal of chest drains
Removing chest drains in a timely manner is important for four reasons. First, it is known from the vascular access device literature that if plastic remains in situ for a longer period of time (and particularly after 72 h), the risk of infection increases. 12 This is all the more significant for chest drains as infection in the pleural space confers a 15% one-year mortality. 5 This is due in part to the difficulty in antibiotic penetration to this privileged site. Second, chest drains provide ongoing morbidity for our patients as they are almost always uncomfortable and occasionally overtly painful. Third, having a chest drain in situ provides an additional physical restraint. Therefore, although the drains can be picked up, they add a further hurdle to ongoing effective physical rehabilitation. Finally, it would seem logical to assume that the presence of a foreign object in the thoracic cavity would have a deleterious effect on respiratory mechanics and potentially hinder weaning from ventilator support. Somewhat surprisingly, we could find no data in the world literature on the effects of chest drains on lung mechanics in either health or during positive pressure ventilation.
Pleural fluid physiology
The first question most clinicians ask when considering removing a chest drain is what is the fluid output? To answer this, we need to revise some pleural physiology. Originally, it was hypothesised that pleural fluid turnover was merely a passive occurrence. That on the parietal side, pleural fluid is filtered as the high hydrostatic pressure of the systemic circulation overcomes the osmotic pressure and then on the visceral side the low pulmonary hydrostatic pressure allows the osmotic gradient to cause re-absorption of the fluid. Unfortunately, the reality of physiology is much more complex. Filtration of pleural fluid occurs from both visceral and parietal pleura, and in reality, re-absorption occurs predominantly via the lymphatic system which by its intrinsic smooth muscle is able to generate a sub-atmospheric pressure to ‘hoover’ out the fluid.
13
A complete review of the physiology of pleural fluid is beyond the scope of this article, but the following facts are worth revising. A normal person has approximately 21 mL (0.3 mLkg−1) of pleural fluid in each lung, whereas approximately 300 mL are required to become visible on a chest radiograph. However, the presence of a foreign body (e.g. a chest drain) in the pleural cavity will cause localised inflammation resulting in nearly 150–300 mL/day of pleural fluid to be formed. The lymphatic drainage of the pleurae in health is ∼34 mLday−1 (2% of the overall lymph flow) though this can increase with the presence of increased pleural fluid to ∼700 mLday−1 (40% of the overall lymph flow).
14
Finally, pleural effusions are classically determined as either transudative or exudative by the presence of one of Light’s Criteria
15
(see Figure 2).
Light’s criteria for exudative pleural effusion.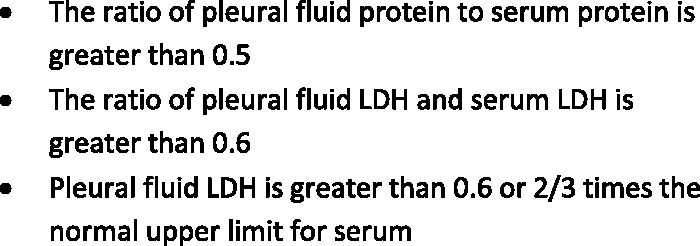
Terminology of chest drains
The second question most clinicians ask when considering removing a chest drain is whether the chest drain is active. To answer the second of these questions, we need to revise the terms ‘swinging’ and ‘bubbling’.
Swinging – The pleural space is intra-thoracic, and therefore, changes pressure during respiration. Thus, if a chest drain is in continuous connection with the pleural space, it will change pressure. This can be seen by a fluid level (either where the drain meets its under-water seal or within the piping) moving to-and-fro with respiration. Therefore, if a chest drain is not swinging, it is not in connection with the pleural space either through blockage, kinking or withdrawal to the thoracic wall. Bubbling – In a pneumothorax, air leaks into the pleural space. The chest drain provides a low resistance pathway for this trapped air to escape and the lung to expand and seal. Therefore, this escaping air will travel through the drain piping and bubble through the underwater seal (it is worth noting that a bubbling drain will also be swinging with water rising up the tubing during normal inspiration).
It may seem very simplistic to revise the above terms. However, when we reviewed our local practice covering over 500 drain days, over 25% of the drains we removed had not been swinging and therefore were non-functional for over three days (as shown in Figure 3). This equates to 144 days where non-functional plastic remained inside our patients.
Percentage of chest drains removed versus time.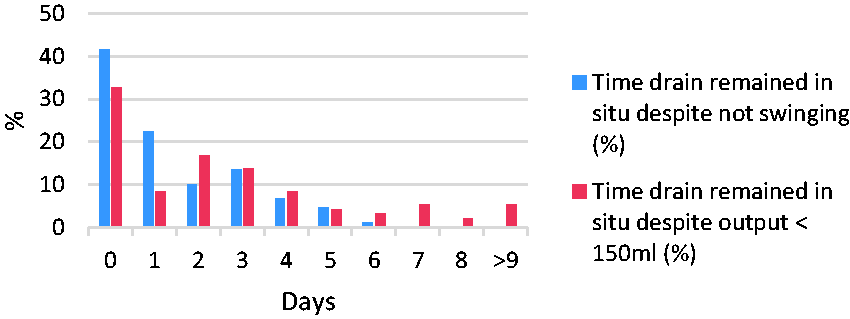
The I-T-U approach to removing chest drains
As explained above, the classical approach when removing chest drains is to first consider the fluid output – if it is less than 300 mL/day, it is unlikely to be actively treating any effusion. Then to question whether the drain is functional – if it is not swinging, action or re-imaging is required. However, Figure 1 demonstrates that the ICU has a myriad of reasons behind chest drain insertion, and it is therefore critical that the intensivist adds a further primary, key question namely what is the aim of the chest drain? Specifically, is the drain aiming to actively treat a problem; say removing pus or trapped air? Or is the drain prophylactic, placed to spot early leak post-surgery or catch a traumatic pneumothorax caused as a patient starts positive pressure ventilation? This provides the basis for our systematic approach to reviewing chest drains as shown in Figure 4.
ITU approach to removing chest drains.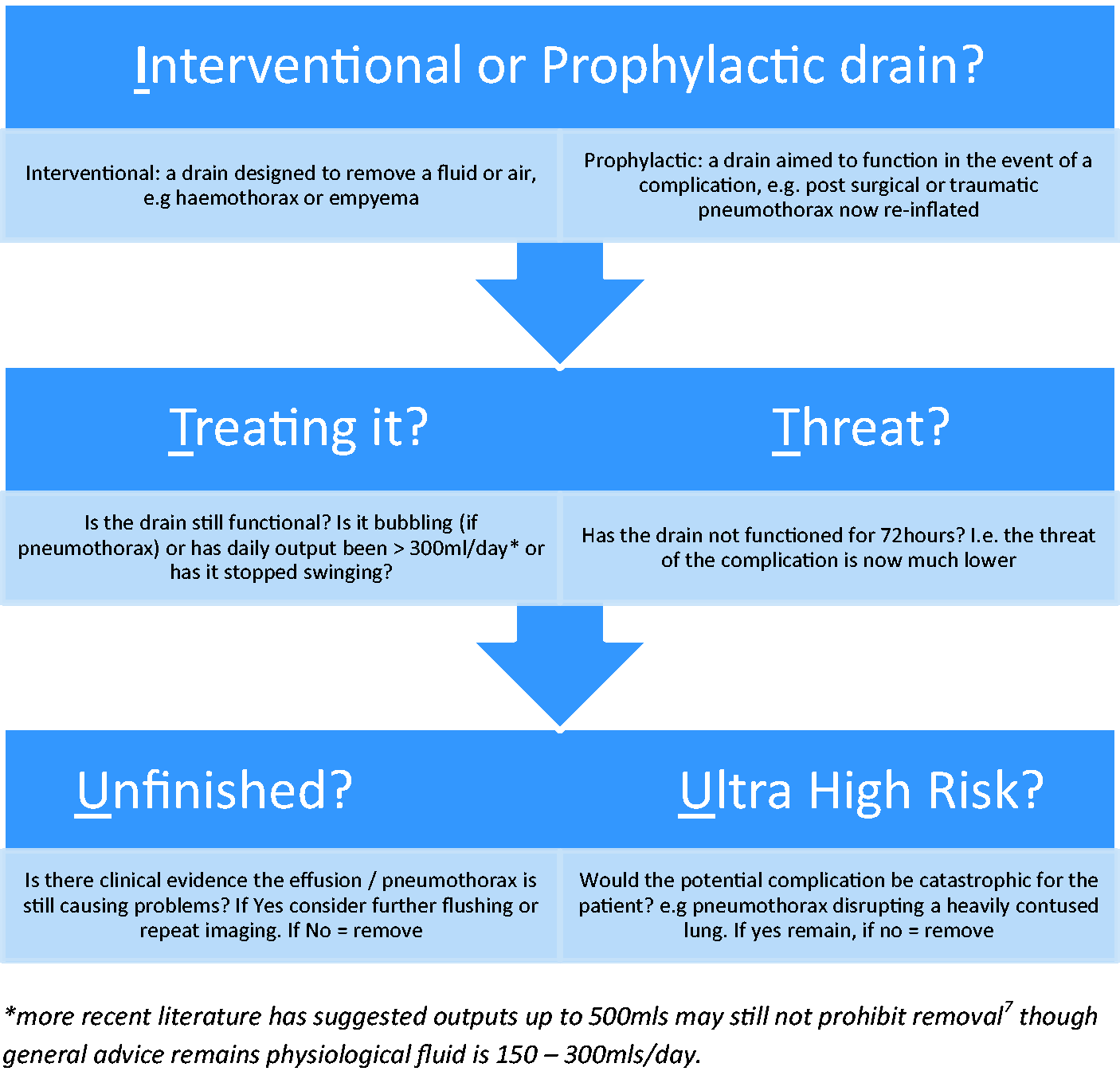
We believe this approach provides a simple and memorable acronym, I-T-U, which can give a clinician confidence to remove a non-functioning chest drain. However, like many decisions on the ICU, removing a chest drain is ultimately a balance of risk against benefit and as covered in our introduction, we do not have an evidence base to quantify the morbidity associated with having a drain in situ. For instance, we do not even know the effect on lung mechanics, let alone the more unquantifiable effects on potential hindrance of rehabilitation. However, the intensivist will continue to commonly come across chest drains for a myriad of clinical scenarios, and therefore, it is important that we can confidently and systematically assess them.
Conclusion
Chest drains have come a long way since their high-risk start in the 1918 flu pandemic, and they are now commonplace throughout hospitals. However, this growth of use provides the intensivist with a unique problem; not only are chest drains common but the reasons behind their presence on ICU are broad ranging. Our audit showed that on average there were 1.5 chest drains present everyday on our ICU and causation ranged from simple pneumothorax to post-complex upper gastrointestinal surgery. It is therefore critical that the intensivist is armed with a memorable, generalisable and reliable structure to assess each chest drain and ensure safe and timely removal. It is in light of this need that we propose the I-T-U questions – is the drain for
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.