
Abstract
We present the case of a 40-year-old woman diagnosed with Austrian syndrome, an association of endocarditis, meningitis and pneumonia caused by Streptococcus pneumonia. She had none of the risk factors previously described in the literature but on immunological assay was found to have low serum levels of mannose-binding lectin, a protein required for complement activation. The clinical manifestation and treatment of this condition are discussed, and we emphasize the importance of early recognition of cardiac involvement and prompt surgical management.
Introduction
Austrian syndrome is a triad of endocarditis, meningitis and pneumonia first described by pathologist Richard Heschl in 1862 after the autopsy of five patients. The clear predisposition of the condition to the aortic valve was demonstrated by Robert Austrian, an American physician in 1957. 1 Austrian syndrome is associated with a high mortality due to the acute and aggressive evolution of endocarditis and the increasing prevalence of pneumococcal resistant strains. 2 The prevalence of pneumococcal endocarditis now accounts for less than 3% of all cases after the introduction of penicillin in the early 1940s and most often occurs in immunocompromised patients. 2 Mannose-binding lectin (MBL) protein deficiency is defined as a serum level <500 ng/mL and is associated with a poorer outcome after infection in otherwise immunocompetent patients. 3 We describe a case of Austrian syndrome in a patient with no apparent risk factors and a mild deficiency in MBL protein that developed severe acute heart failure requiring emergency cardiac surgery and made a full recovery.
Case presentation
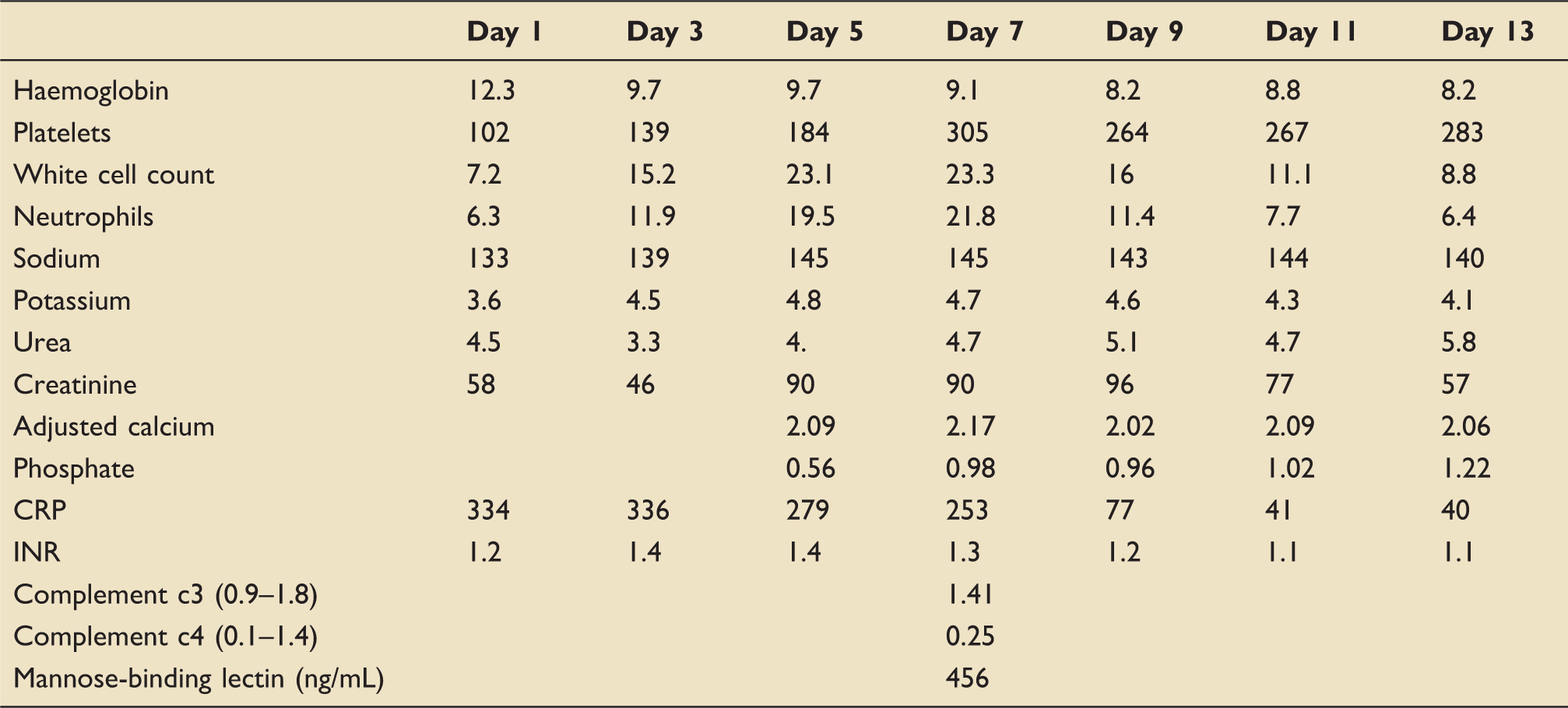
Written consent for the publication of this report was gained from the patient. A 40-year-old female patient presented to the Accident and Emergency department with a three-day history of headache, vomiting and rigours. She was otherwise healthy with no known medical problems and no history of alcohol consumption. On examination, she was pyrexial with a Glasgow Coma Scale (GCS) of 10 and a non-blanching rash. She was haemodynamically stable and did not require oxygen therapy at the time. Blood tests revealed a neutrophilia (WBC 15.2 × 109/L, neutrophils 79%) and a thrombocytopenia (102 × 109/L. A summary of her laboratory results is given in Table 1. Cranial computed tomography was unremarkable, and a chest radiograph showed bilateral hilar shadowing. A lumbar puncture was performed, and cerebrospinal fluid (CSF) analysis showed WBC 992 × 106/L, glucose 1.9 mmol/L with negative CSF culture but a positive pneumococcal polymerase chain reaction. Her urine was also positive for the pneumococcal antigen. Immunological assay was performed, and this included testing for MBL protein. Interestingly, the results revealed a MBL level of 456 ng/mL (normal range >500 ng/mL). She had remained clinically stable over the first three days, but during day 4 of her admission, she became increasingly more agitated and her oxygen requirements increased resulting in admission to the intensive care unit (ICU), where she was intubated and ventilated. Her subsequent chest X-ray showed pulmonary oedema, and she was started on noradrenaline for vasopressor support. She was initially treated for meningitis with ceftriaxone, rifampicin and amoxicillin which was later replaced by linezolid. The following morning daily review on the ICU revealed normal heart sounds. However, approximately 5 h later, she became increasingly more unstable with increasing oxygen and vasopressor requirements. On auscultation, a new loud pan systolic murmur was heard, and an urgent trans-oesophageal echo revealed destruction of the right coronary aortic valve leaflet with a small vegetation causing severe aortic regurgitation. Over the next 24 h, she made a slight improvement with regard to her oxygen requirements and was extubated. Unfortunately, this was unsuccessful secondary to decompensated heart failure, and she was re-intubated. After discussion with the local tertiary centre, she was transferred for an emergency aortic valve replacement. An image of her aortic valve taken from her trans-oesophageal echocardiogram can be seen in Figure 1. Her aortic valve was replaced with a mechanical valve, and she was successfully extubated post-operatively without any significant complications. She made a full recovery and was discharged home.
Snapshot of her aortic valve showing severe aortic regurgitation. Summary of laboratory results.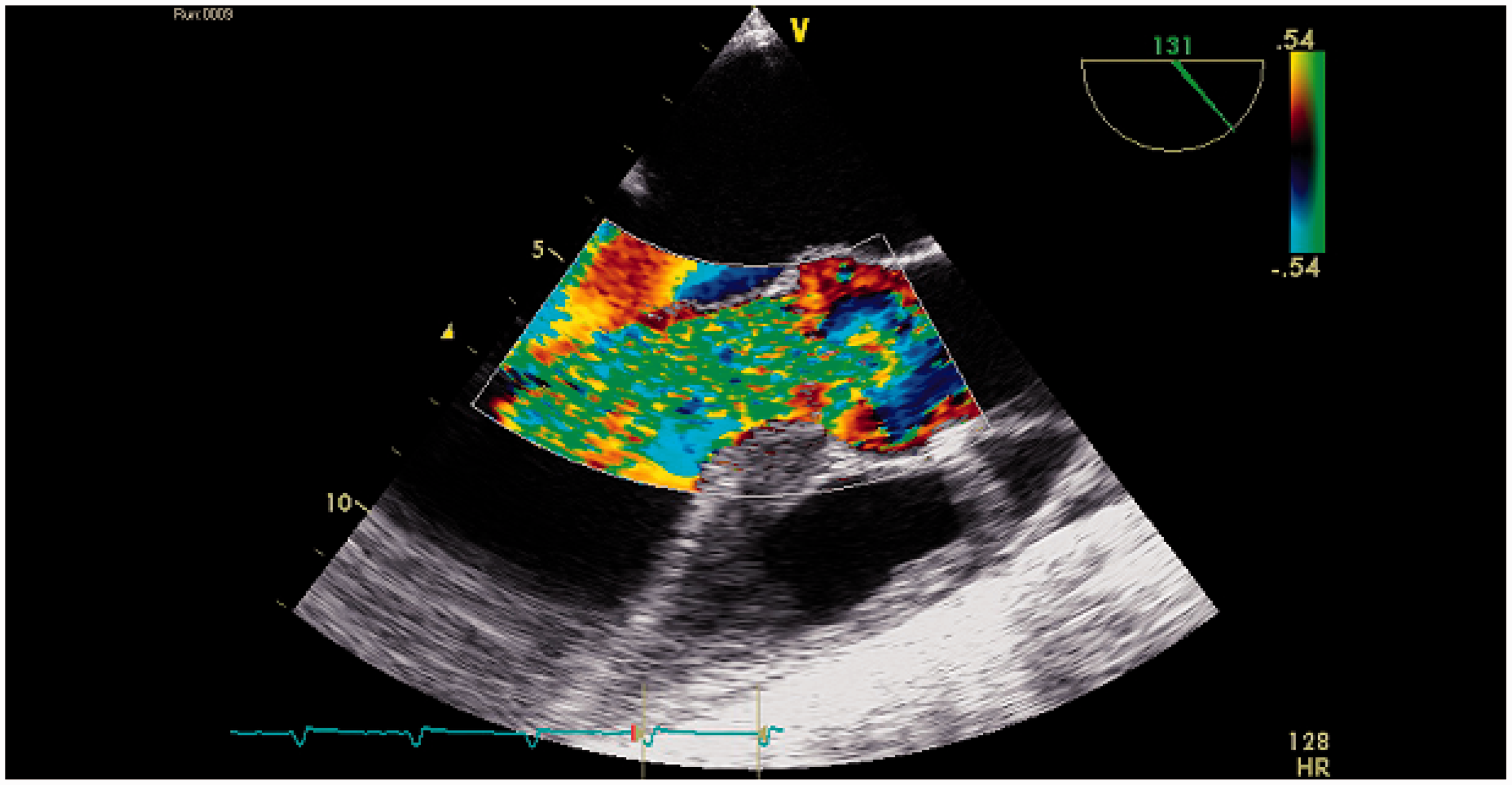
Discussion
Austrian syndrome is a triad of meningitis, endocarditis and pneumonia and is a clinical rarity. S. pneumonia, a gram-positive bacterium first discovered in 1881, remains the most common bacterial aetiology of meningitis in adults of all ages and despite appropriate treatment with antibiotics, it is associated with high rates of morbidity and mortality. 4
In the current antibiotic era, the prevalence of pneumococcal endocarditis now accounts for less than 3% of all cases compared with 15% in the pre-antibiotic era. 2 However, the incidence of worldwide pneumococcal resistance to penicillin has increased dramatically over the last 10 years and has posed a significant challenge to treatment.
Host factors recognized to pre-dispose to Austrian syndrome include male gender, middle-age, alcoholism and immunosuppression. 5 In the immunocompetent host after invasion of S. pneumonia, various immune responses are activated which include both cellular and humoral mechanisms and activation of the complement cascade. Our patient was not known to have any of these well-recognized risk factors and had no significant past medical history. On immunological assay, a decreased level of MBL protein of 456 ng/mL was noted. MBL is a protein involved in complement activation via the lectin pathway. MBL deficiency is associated with a large and heterogeneous group of disease processes, although subnormal levels have been found in healthy people. 6 Deficiency of MBL was defined in the largest series as a serum level <500 ng/mL measured within 48 h of admission in patients hospitalized with pneumococcal infection. 7 Although many patients with low levels are unaffected, low levels have been associated with poorer outcomes in certain infections and are associated with increased susceptibility to meningitis. 8 In a study of 272 critically unwell patients in ICU, low levels of MBL were associated with increased risk of sepsis, septic shock and fatal outcome. 9 The association of MBL deficiency and Austrian syndrome has not previously been described in the literature.
In pneumococcal endocarditis, the native aortic valve is the most common localization of the vegetation, and it normally follows an aggressive course despite optimal medical management. 5 This is highlighted in a literature review which identified 182 cases of pneumococcal endocarditis and reported an overall mortality of 63%. 5 S. pneumonia endocarditis is commonly associated with both local and systemic complications such as perivalvular abscess and embolization, which also most frequently occur on the aortic valve. The clinical presentation of pneumococcal endocarditis is acute, and peripheral signs and symptoms are not often present which can lead to delays in diagnosis and treatment. This is emphasized in a literature review which showed that in 69% of patients diagnosed with pneumococcal endocarditis, there were no associated stigmata. 10 When symptoms do finally appear, acute deterioration is often seen with haemodynamic instability leading to circulatory collapse. In agreement with this presentation, our patient rapidly developed signs of endocarditis over the course of a morning with a new murmur developing in hours. This then rapidly progressed to decompensated heart failure secondary to destruction of the aortic valve. In a patient with both meningitis and pneumonia caused by S. pneumonia, we emphasize the importance of regular examination and auscultation for signs of endocarditis, as our case clearly demonstrates the acute onset and rapid evolution which can ensue.
The diagnosis of Austrian syndrome is largely clinical and requires a high index of suspicion. The use of echocardiography is invaluable in the rapid and accurate assessment of cardiac function and status of valves. In the majority of studies of patients who have been diagnosed with pneumococcal infective endocarditis, transthoracic echocardiography (TTE) is utilized. It has been demonstrated that the sensitivity and specificity of TTE in detecting vegetations and complications is inferior when compared to transoesophageal echocardiogram (TOE). 11 This is again highlighted in a literature review which found that life-threatening complications such as valvular perforation and abscess formation went undetected in 40% and 100% of cases, respectively. 5 However, we appreciate that there are limitations associated with the use of TOE in that it is operator dependent and patients will normally be required to be intubated and ventilated on the ICU. We, therefore, reiterate the importance of regular clinical assessment of such patients.
Management consists of either medical treatment alone or a combined medical–surgical approach. Medical therapy is supportive in nature with the use of antibiotics, although the specific regimen remains unclear in the penicillin-resistant era. In a study conducted by Vuille et al., 12 only 17% of the vegetations disappeared with medical therapy with the majority requiring invasive surgery. Surgical management has a significant role, and this is evidenced by a literature review which showed that the mortality of patients with pneumococcal endocarditis managed with antibiotics alone or a combined medical–surgical treatment was 62% vs. 32%. 5 However, the timing of surgical intervention will also impact on the overall outcome of the patient, and this may need to be guided by regular echocardiography and clinical judgement. Guidelines for the management of patients with valvular disease recommend early consideration of surgery for valve replacement as soon as a diagnosis of bacterial endocarditis has been established. 13 We know that often these patients deteriorate rapidly so early surgical management may avoid the need for an emergency procedure in a haemodynamically unstable patient.
Conclusion
Austrian syndrome is a rare clinical entity and is associated with significant morbidity and mortality. Although the incidence of pneumococcal endocarditis has declined, it is still associated with a poor outcome. As mentioned, often patients present without clinical stigmata of the disease and by the time these develop, patients are often haemodynamically unstable and critically unwell. This case report has emphasized the importance of regular clinical evaluation in patients presenting with S. pneumonia and meningitis, despite not having any recognized risk factors for endocarditis. This case was associated with MBL deficiency which has been associated with poorer outcome. However, at present, we do not routinely recommend testing for MBL deficiency, as the implications of this deficiency are not fully elucidated. Further research needs to be undertaken on whether there is potential for MBL substitution in these patients or whether there is a role for prophylactic antibiotics. Management of these patients is complex requiring a high index of suspicion for early diagnosis, and we advocate a combined medical–surgical approach for improved overall outcome.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.