
Abstract
Background
Cardiac surgery is increasingly performed on patients aged 80 years and over. Previous studies have shown an associated longer length of hospital stay and higher morbidity and mortality. Our aim was to establish whether an increased mortality was demonstrated in patients aged over 80 undergoing surgery in our centre, and the impact of age upon critical care and hospital stay, and 30-day and 6-month survival.
Methods
Over a 12-month period, 2042 critical care episodes were examined collectively and divided into those undergoing thoracic and cardiac surgery. Propensity matching of 216 patients who underwent cardiac surgery was performed for parameters including Acute Physiology And Chronic Health Evaluation (APACHE) II and Intensive Care National Audit and Research Centre score.
Results
Of the admissions studied, 1784 were of patients under 80 years of age, and 258 over 80. Thirty-day mortality of those aged over 80 was significantly higher (8.9% vs. 3.8%, p < 0.0001), although the number of days of each level of organ support and total duration of critical care stay was not significantly different. Propensity matching of cardiac surgery patients indicated a longer length of hospital stay in those aged over 80, but no significant difference in length of critical care stay or mortality at six months.
Conclusions
As previously demonstrated, we found an increased mortality in the older patient group. Following propensity matching, there was no significant difference in 30-day or 6-month mortality. Older patients must be fitter than their younger peers to compensate for the effects of age on APACHE II score. Even when this is taken into consideration, cardiothoracic operations appear to be safe in patients aged over 80.
Introduction
An increasing proportion of cardiac surgery is now being performed on patients over 80 years of age, with workload on octogenarians approaching 10% in some centres. 1 Studies have shown that patients aged 80 and over undergoing cardiac surgery have a longer length of stay, higher morbidity and higher 30-day mortality than younger patients 2 with one study finding a 30-day mortality of 10.6% for those over 80. 3 This has a significant impact upon resource utilisation and surgical throughput and also may influence the decision of patients to proceed with surgery. Nonetheless, for patients undergoing uncomplicated cardiac surgery with few preoperative comorbidities, the outcome for octogenarians can be very good.4,5 Several studies describe a significant improvement in quality of life4,6 with many of the surviving patients continuing to live at home, functioning independently and enjoying leisure activities. 7 As a result, despite the increased risks, even a decade and a half ago, 87% of octogenarians having undergone cardiac surgery felt that they had made a good decision. 8
In 2011, 4.6% of the population of England were aged over 80 9 and this proportion is expected to continue to increase with a resultant increase in referral rates for cardiac surgery. 10 If these patients require prolonged critical care stays or ongoing rehabilitation following their surgery compared to the traditional demographic, current resource allocation may have to be reconsidered.
Our aim was to establish whether an increased mortality was demonstrated in patients aged over 80 compared to younger patients, the impact of age upon length of critical care and hospital stay and the 30-day and 6-month survival rates between the two groups.
Methods
Study design and population
We performed a retrospective study on patients undergoing cardiac or thoracic surgery at the Liverpool Heart and Chest Hospital in the UK. Approval for the study was given by the hospital’s Cardiothoracic Directorate and by the Data Quality Department, specific ethical approval was sought and waived.
An institutional, prospectively collected database was examined for all patients admitted to the critical care unit from 1st January 2012 to 31st December 2012, totaling 2177 admissions. Of these, 117 patients were admitted to the critical care area on more than one occasion during their hospital visit, accounting for 252 entries. Where patients were readmitted within a single hospital stay, a composite entry was created to represent total days of critical care and of each level of organ support. All survival statistics were calculated from the first day of the first critical care admission. Consequently, the analysis was performed on 2042 entries. Where possible, patients undergoing cardiac and thoracic surgery were identified for later subgroup analysis.
Statistical analysis
Statistical tests were performed using JMP 10.0.0 for Mac (SAS Institute, Inc., Cary, NC, USA). Categorical variables were compared using Fisher’s exact test and continuous variables using Student’s t-test or Wilcoxon ranked sum tests, depending on distribution. We performed 1:1 nearest neighbour propensity matching of patients admitted to the critical care unit following cardiac surgery with a 0.25 caliper, matching for height, weight, Intensive Care National Audit and Research Centre (ICNARC) and Acute Physiology and Chronic Health Evaluation (APACHE) II scores on admission as well as operation type; 216 patients were matched.
Results
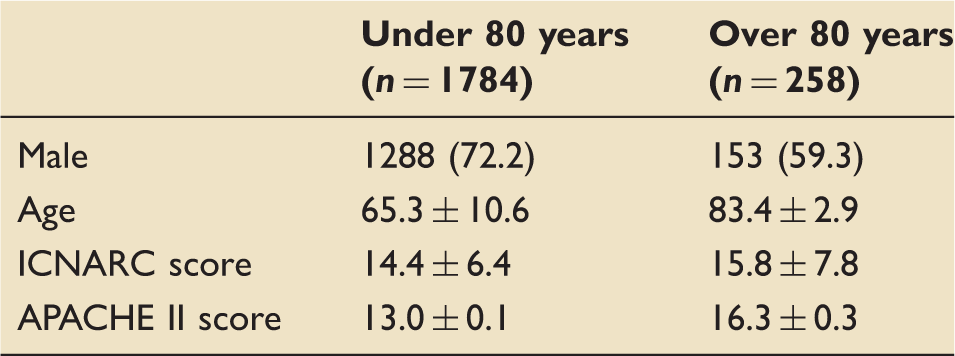
Demographic information of all patients – cardiac and thoracic surgical patients combined. Data represent number (percentage) or mean ± standard error.
Morbidity and mortality outcomes in the combined cardiac and thoracic surgery groups
Thirty-day mortality in the over 80 group was significantly higher than in the under 80 group (8.9% vs. 3.8%, p < 0.0001), as was 6-month mortality. Overall, mortality within the critical care area in the over 80 group was more than double that of the under 80 group (10.9% vs. 4.7%, p < 0.0001). A Kaplan–Meier survival curve (Figure 1) demonstrates the precipitous fall in survival of the over 80 group in the first 30 days over a median six-month follow-up.
Log-rank survival curves for six months postadmission (over 80 blue; under 80 red, p < 0.001).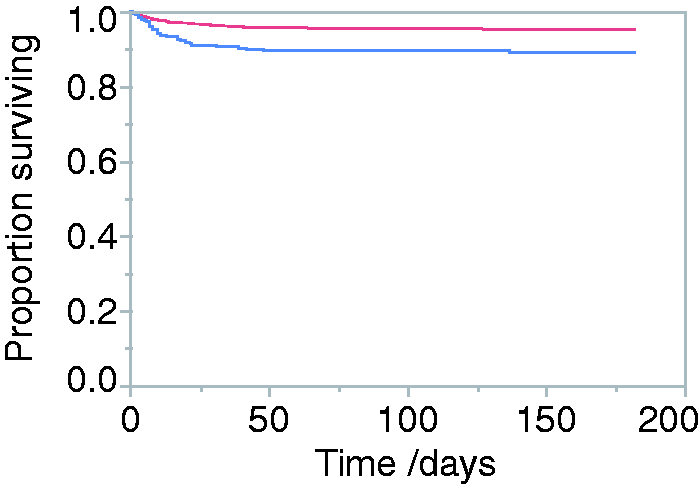
Comparative duration of ICU stay, morbidity and mortality of patients aged under and over 80 years – cardiac and thoracic surgical patients combined. Data represent number (percentage), median (interquartile range [IQR]) or mean ± standard error.
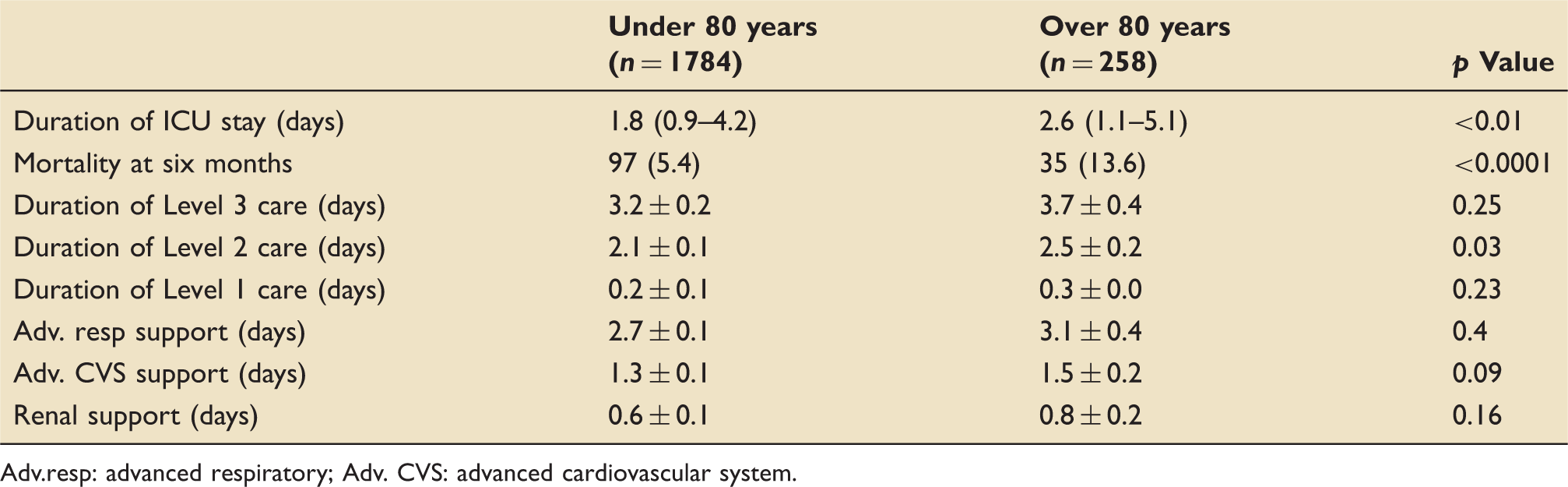
Adv.resp: advanced respiratory; Adv. CVS: advanced cardiovascular system.
Cardiac surgical admissions
Comparative duration of ICU stay, morbidity and mortality of patients aged under and over 80 years – patients undergoing cardiac surgery only. Data represent number (percentage), median (interquartile range [IQR]) or mean ± standard error.
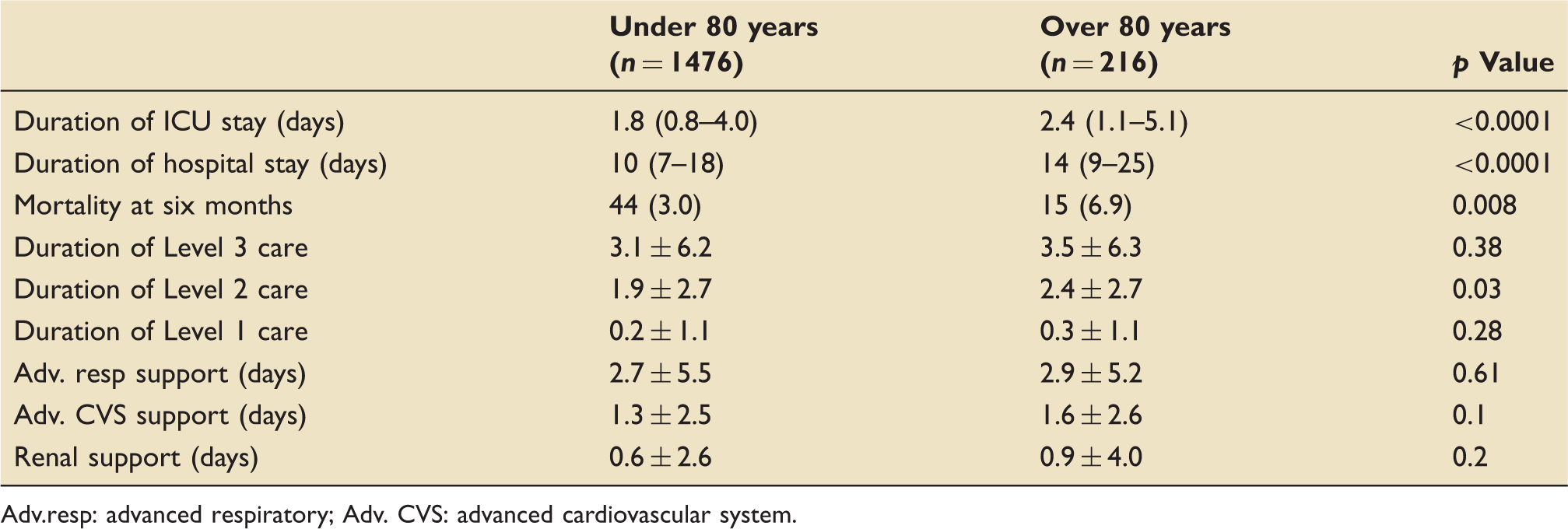
Adv.resp: advanced respiratory; Adv. CVS: advanced cardiovascular system.
PSM of 216 cardiac surgery patients – characteristics of group and comparison of morbidity and mortality. Data represent number (percentage), median (interquartile range [IQR]) or mean ± standard error.
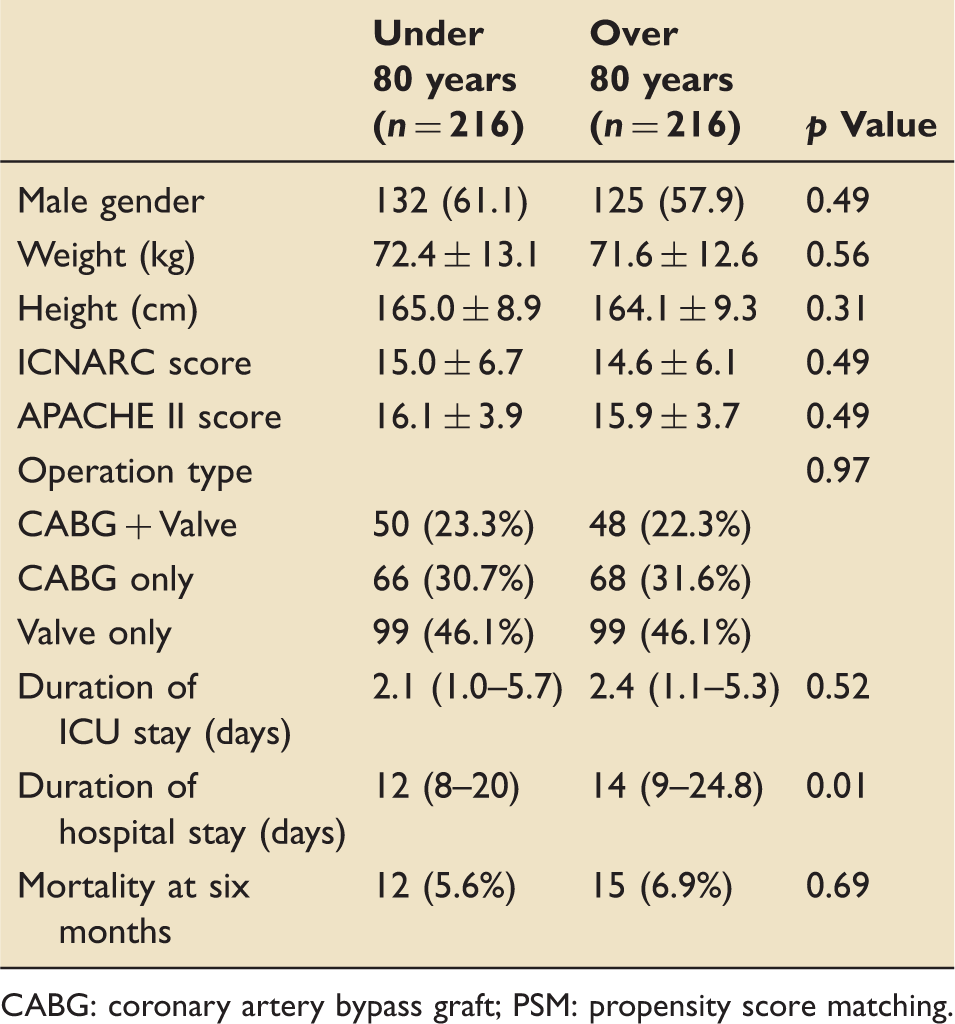
CABG: coronary artery bypass graft; PSM: propensity score matching.
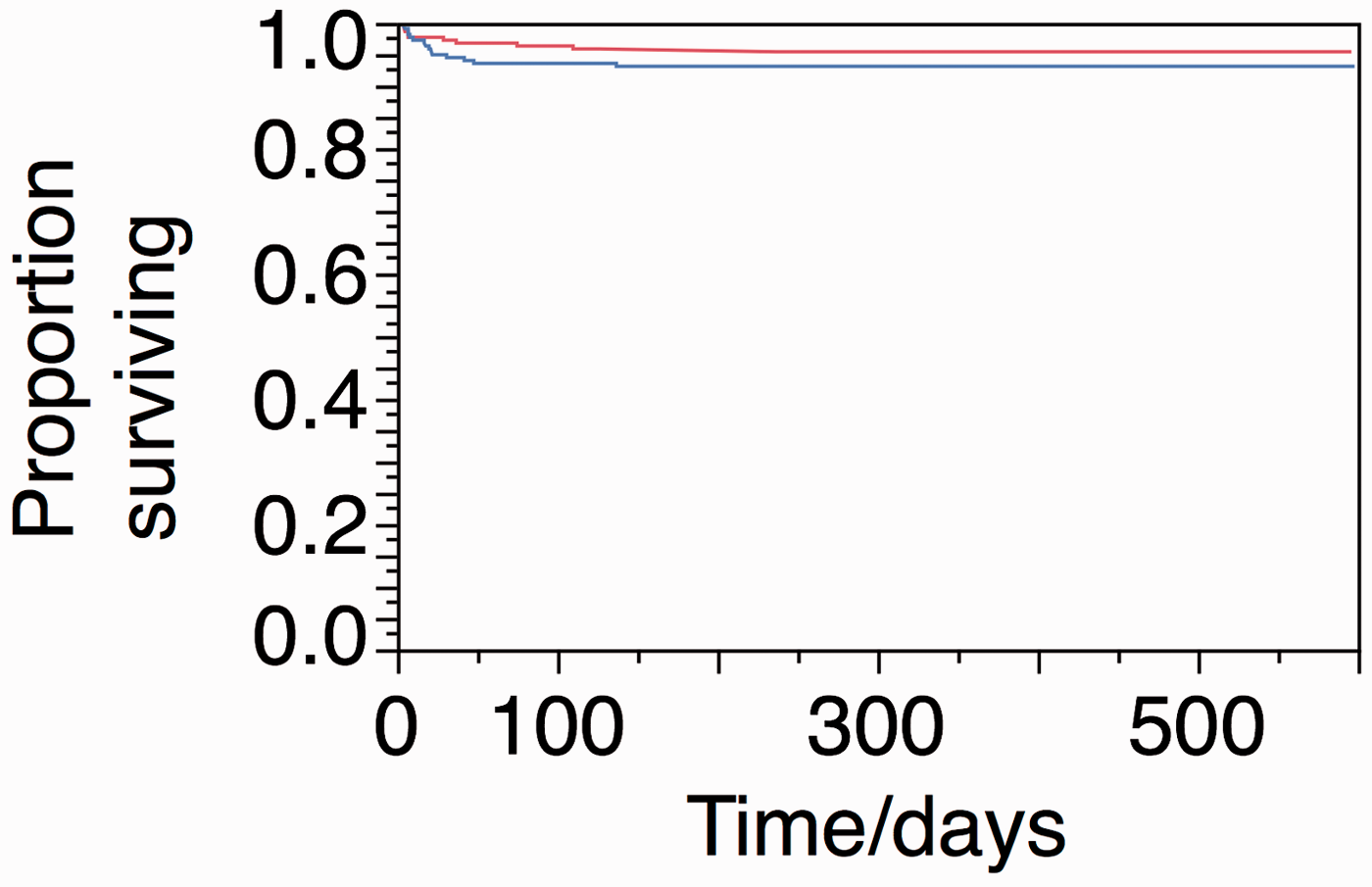
Log-rank survival curves for propensity-matched cardiac surgery patients for six months postadmission (over 80 blue; under 80 red), p = 0.3.
Thoracic surgical admissions
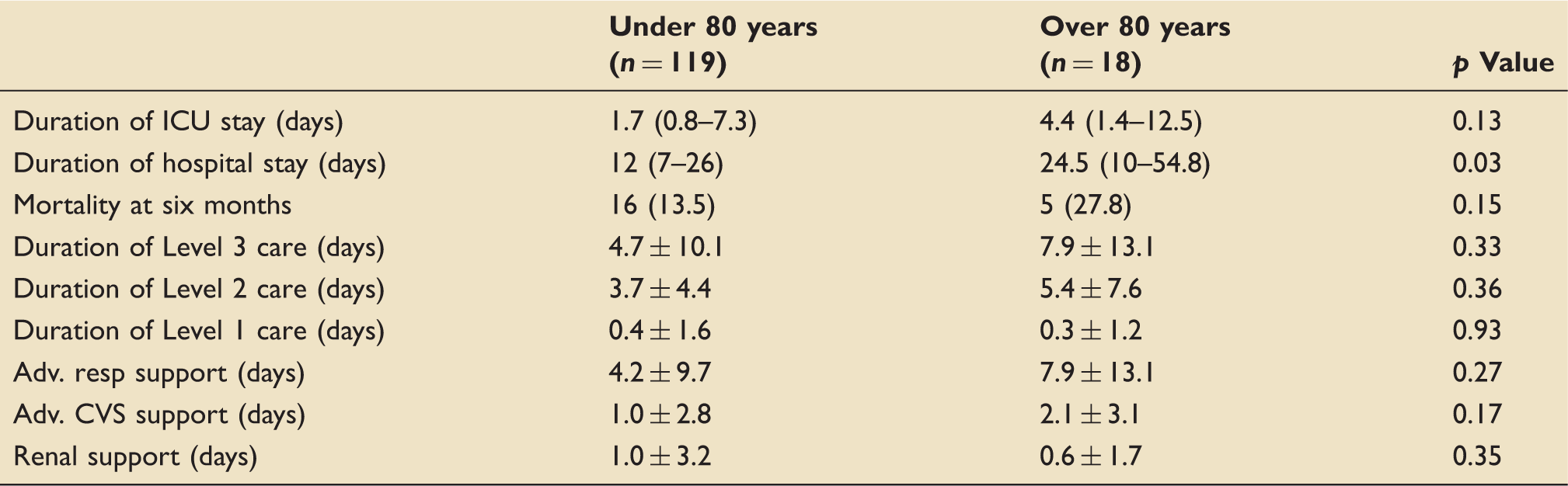
Comparative duration of ICU stay, morbidity and mortality of patients aged under and over 80 years – patients undergoing thoracic surgery only. Data represent number (percentage), median (interquartile range [IQR]) or mean ± standard error.
Discussion
Our rate of operation in octogenarians and nonagenarians is one of the highest in the literature at 12.7% for cardiac surgery. In line with similar studies, we found that there was increased mortality in the older population. Mortality was three times higher in octogenarians undergoing thoracic surgery requiring admission to the critical care unit, compared to those in the younger age group, despite a similar premorbid state. By contrast, the older cardiac surgery patients were only twice as likely to die as their younger counterparts. However, levels of organ support were similar in both young and elderly patients, suggesting that a tendency to conservative weaning in elderly patients may have prolonged their stay on critical care.
The APACHE II score was designed as a method of risk stratification for patients admitted to general critical care units. Allocation of points according to parameters assessed and measured on the first day of admission to a critical care area give an aggregate score that can be used to quantify risk of mortality. 11 Patients admitted to the critical care following cardiac surgery invariably have high levels of temporising support that is usually weaned predictably and rapidly. As a result, admission on high levels of cardiovascular and ventilator support does not necessarily reflect poor prognosis in cardiac surgical patients, and the APACHE II developers excluded them from the population from which the score is derived. 12
Both the APACHE II and ICNARC systems assign points according to the age of the patient, and propensity matching in this study will have artificially normalised comorbidity according to age. In order to balance the effect of higher scores in the older population, the matching process will have selected patients with fewer comorbidities to compensate for the points assigned for age. We found that following propensity matching, there was no significant difference in 30-day or 6-month mortality, suggesting that the APACHE II score can reliably stratify for patient risk. Older patients must be fitter than their younger peers in order to compensate for the effects of age. Even when this is taken into consideration, however, cardiothoracic operations appear to be safe in patients over 80 years of age. Whilst we did not set out to assess the utility of the APACHE II scoring system in cardiac surgical patients, the comparable mortality despite differing ages between the two groups supports the effectiveness of APACHE II as a method of mortality prediction.
It should also be noted that all patients undergoing cardiac surgery were routinely admitted to the critical care area, whereas the majority of patients undergoing thoracic surgery were discharged in the first instance to a separate high dependency unit. Patients transferred to the critical care unit following thoracic surgery were therefore self-selected due to poor progression or increasing organ failure, which may explain the relatively higher complication rate in thoracic surgical patients.
Our study shows a significantly higher six-month mortality for patients over 80 requiring admission to the critical care area, but without an associated increase in the number of days of each level of care. A similar finding was recently reported by Deschka et al. 11 When examining admissions of patients following thoracic surgery, no significant differences in duration and level of care were found.
Arguments against surgery and critical care admission in the over 80 group often centre on the increased length of critical care stay and resource utilisation compared to younger patients and the impact this has on overall hospital surgical activity. The small propensity matched group of patients indicated no difference in mortality according to age. The potential for a prolonged hospital stay should be made clear to patients – but those surviving beyond 60 days are likely to continue to reap the benefits of their surgery into the mid term.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.