
Abstract
Estimation of bleeding risk in critical care patients undergoing interventional radiological procedures is frequently made on the basis of blood tests. If these tests are abnormal, fresh frozen plasma and/or platelet transfusions may be given to reduce the risk of bleeding. We performed an audit and national survey of the use of fresh frozen plasma and platelet transfusions prior to interventional radiological procedures. We identified 68 consecutive chest, abdominal or pelvic drain insertions in 54 critical care patients between 2008 and 2011 at a single intensive care unit. Eight (12.3%) patients were transfused fresh frozen plasma prior to drain insertion despite having a prothrombin time below 22 s. One patient with a prothrombin time above this threshold received fresh frozen plasma. One patient received a platelet transfusion, at double dose, despite a platelet count above 50 × 109/l. A national survey of interventional radiologists demonstrated extensive variability in safe thresholds for invasive procedures and usage of fresh frozen plasma. There is a need for further clarification around coagulopathy and interventional radiology in the critical care setting.
Keywords
Introduction
The assessment of bleeding risk in interventional radiological procedures is important in risk stratifying patients to minimise bleeding complications. The British Committee for Standards in Haematology (BCSH) 1 guideline on assessing bleeding risk prior to surgery or invasive procedures recommends taking a bleeding history to determine whether patients are at increased risk of bleeding. However, in the critical care setting, a bleeding history is frequently not available. Consequently, routine laboratory tests of haemostasis (notably prothrombin time (PT), activated partial thromboplastin time (APTT) and platelet count) are frequently used to estimate bleeding risk. This is problematic, as PT and APTT are poor predictors of bleeding risk with previous studies reporting a positive predictive value for bleeding of 0.03–0.22 for a prolonged PT, with a likelihood ratio ranging from 0.94 to 5.1. 1
Patients judged to be coagulopathic or at risk of bleeding on the basis of PT and/or APTT are often transfused fresh frozen plasma (FFP) prior to interventional procedures as prophylaxis against bleeding. The evidence base for this practice is poor.2,3 Laboratory indices of clotting correct in only a small proportion of patients following FFP administration and there have been few studies looking at whether prophylactic FFP mitigates bleeding risk. 4 This is of significance as FFP transfusion is associated with risks such as transfusion-related acute lung injury, transfusion associated circulatory overload and anaphylactic reactions. 5
Whilst there is greater consensus over platelet transfusion thresholds prior to invasive procedures, 6 there is still inconsistency in the thresholds used in clinical practice and in the dose that is administered. Despite little evidence to support the practice, administration of ‘double dose’ platelets remains common. 7 A recent national UK survey in haematology patients found that 10% of all prophylactic platelet transfusions were ‘double dose’ and 28% of all platelet transfusions were considered inappropriate when assessed by a validated algorithm. 8
In this study we assessed the use of FFP and platelet transfusion prior to invasive radiological procedures as well as current practice in the interpretation of coagulation tests prior to invasive radiological procedures in critical care patients, both locally and nationally.
Methods
This study involved two parts: a retrospective local audit, followed by a national survey.
Retrospective audit of current practice
To define appropriate audit standards, the authors searched for guidelines on the use of thresholds for tests of coagulation prior to performing drain insertions. There is little data to guide this practice but consensus guidelines from the Society of Interventional Radiology (SIR) and Cardiovascular and Interventional Radiological Society of Europe (CIRSE)
9
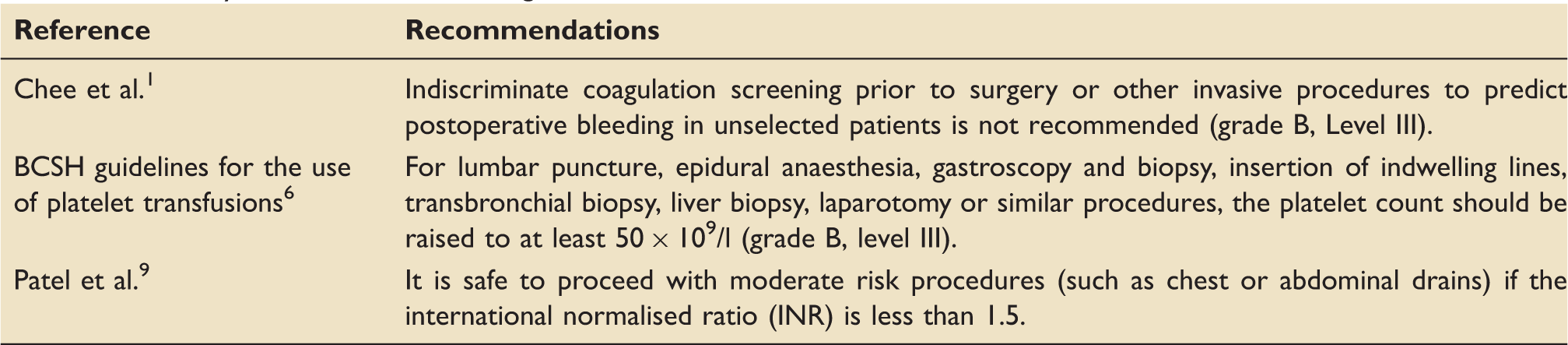
recommend that it is safe to proceed with moderate risk procedures (such as chest or abdominal drains) if the international normalised ratio (INR) is less than 1.5. There is no consensus on how to interpret a prolonged APTT before an invasive procedure. The BCSH guidelines for platelet transfusions suggest a threshold of <50 × 109/l platelets before transfusion for liver biopsies, chest drain insertion and abdominal drain insertion.
6
A summary of relevant guidelines is presented in Table 1. Audit standards were therefore:
Percentage of procedures where platelets were transfused above threshold of 50 × 109/l. Percentage of procedures where platelets were not transfused despite platelet count less than 50 × 109/l. Percentage of procedures where FFP was given despite a PT of less than 22 s (equivalent to an INR of 1.5 in the John Radcliffe Hospital). Summary of relevant transfusion guidelines.
All critical care patients at the John Radcliffe Hospital, Oxford who had been booked for chest, abdominal or pelvic drain insertion between December 2006 and November 2011 were identified using the Computerised Radiology Information System. The last recorded PT, APTT and platelet count taken prior to each procedure were recorded to demonstrate the transfusion triggers that were used for FFP and platelet transfusions. Bleeding complications recorded by the interventional radiologist performing the procedure were extracted from the Picture Archiving and Communication System (PACS) system. Records of FFP and platelet transfusions were extracted from hospital blood bank records.
PT and APTT were assessed using Neoplastine R and TriniCLOT, respectively, on Stago analysers at the John Radcliffe Hospital. PT and APTT results are reported in seconds. The international sensitivity index of Neoplastine R was 0.95 with a mean normal PT of 14.5 s. Therefore in the local setting, an INR threshold of 1.5 corresponds to a PT threshold of 22 s. Platelet counts are assessed using a Sysmex analyser.
Unpaired t tests (95% significance level) were used to compare patients who received blood components to those who did not. Data are reported as mean (SD) unless otherwise indicated. Statistical analysis was performed using SPSS 22.0 (IBM, Armonk, USA).
National survey of current practice
An online survey was distributed to all hospitals with interventional radiology departments. Responses were collected in May and June 2013. The following questions were asked (see Appendix 1 for full questionnaire):
Does your department have guidelines on assessing bleeding risk and/or performing coagulation tests prior to routine thoracic or abdominal drain insertion (y/n)? Do you routinely take a ‘bleeding history’ (e.g. previous history of heavy bleeding after surgery/invasive procedures/dental extractions) prior to performing routine thoracic or abdominal drain insertion (y/n)? If a bleeding history is taken, is it used to guide whether further coagulation tests should be performed (y/n)? Above what level of the following would you NOT insert a chest drain? PT APTT What management strategies do you use if a patient has a PT or APTT above the threshold?
Results
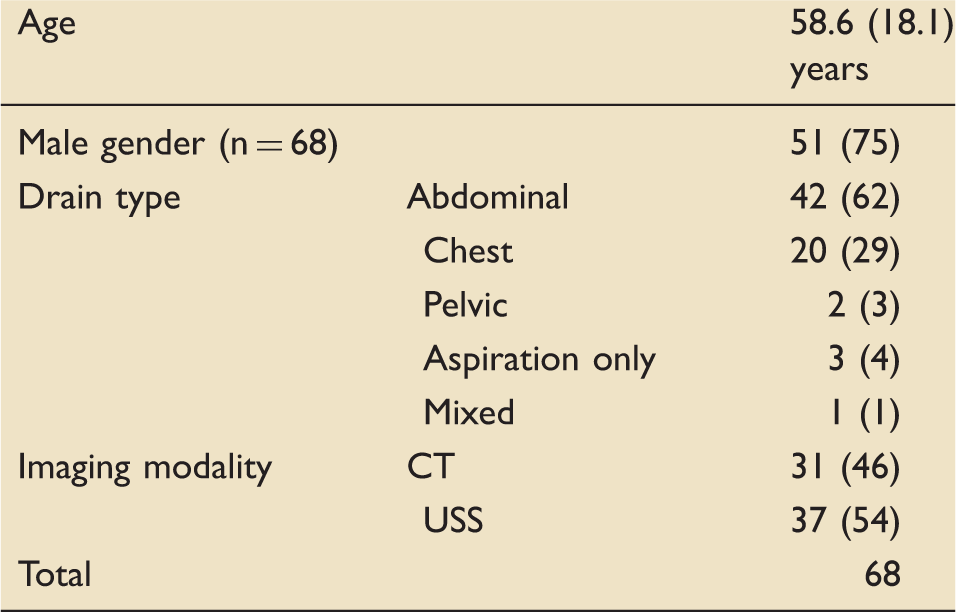
Demographic information of the patients in our audit. Data are presented as mean (SD) or number (%).
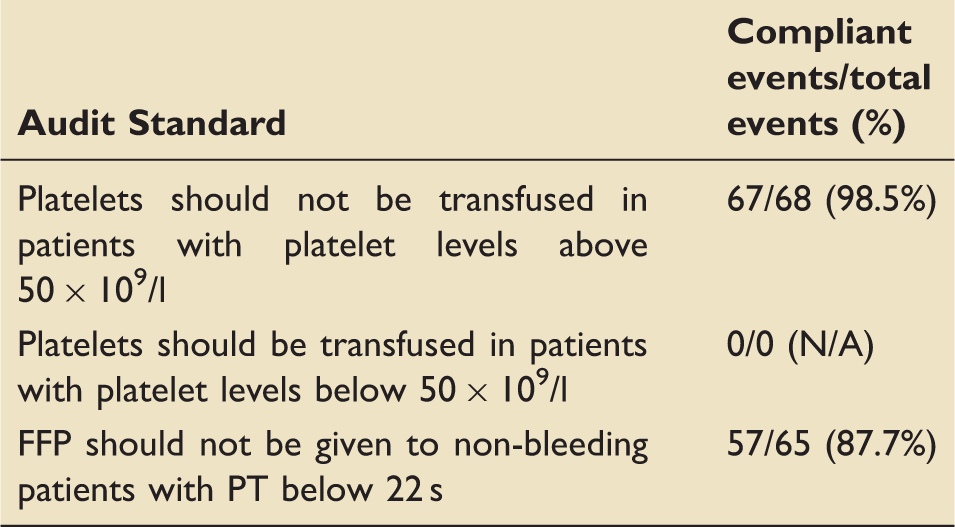
Audit standards and percentage compliance: each ‘event’ refers to insertion of a chest, abdominal or pelvic drain. No patient had a platelet count below 50 × 109/l.
Coagulation test thresholds for procedure cancellation or FFP administration
Three patients had a PT above 22 s (22.2, 37.4 and 44.3 s, respectively). The latter two of these patients had chest drains inserted without prophylactic FFP transfusion, and no immediate bleeding complications were recorded. The patient with a PT of 22.2 s received prophylactic FFP before their pelvic drain insertion. Two procedures were cancelled due to prolonged coagulation tests (these were not otherwise included in our analysis). Of these cancelled procedures, one patient was due to have an abdominal drain and had a PT of 19.6 s and APTT of 40.3 s. The other was booked for a chest drain and had a PT of 18.1 s and APTT of 36.6 s.
Nine drain insertions (one chest, seven abdomen, one pelvic) in six patients were preceded by FFP administration. The median (range) dose of FFP administered was 4(2–7) units. In eight of these drain insertions, patients had a PT below 22 s. The mean (SD) pre-transfusion PT in the transfused group was 18.5(2.2) s compared to 16.7(4.9) s in the non-transfused group (p = 0.27). The mean (SD) pre-transfusion APTT in the transfused group was 41.6(6.96) s compared to 39.4(18.3) s in the non-transfused group (p = 0.73).
In summary, 57/65 (87.7%) of patients were compliant with the standard ‘FFP should not be given to non-bleeding patients with PT below 22 seconds’.
Platelet transfusion
No patients in this study had platelet counts below the recommended threshold for platelet transfusion (50 × 109/l). One patient nevertheless received a transfusion of platelets. This was for a female patient having a chest drain inserted with a platelet count of 58 × 109/l. She received two adult doses of platelets and her post-transfusion platelet count was 69 × 109/l.
Peri-procedural complications
In 48 cases (71%), there were no peri-procedural complications noted. Nineteen reports (28%) made no comment on whether complications had occurred (or not). Only one patient (1%) had a recorded immediate complication: haematuria following insertion of an abdominal drain due to inadvertent trauma to the right ureter by the drainage needle. This patient had a PT of 15.6 s and APTT of 40.9 s prior to drain insertion and did not receive any FFP. One patient receiving an FFP transfusion prior to abdominal drain insertion had an anaphylactic reaction.
Survey of national practice
We received 49 responses from 161 hospitals (30%) from interventional radiologists to the survey of national practice. Twenty seven (55%) respondents were from teaching hospitals and 22 (45%) from district general hospitals. Only 12 respondents (25%) routinely took a bleeding history before chest or abdominal drain insertion. There was large variation in the PT threshold above which a clinician would not insert a chest drain, ranging from any value above the normal range up to an INR of 2.5. If a patient had a PT above the clinicians’ threshold, 58% would use empirical treatment with FFP and 26% would use empirical treatment with FFP for treating a prolonged APTT.
Discussion
In this audit, 8/9 FFP transfusions were given to patients who had a PT below 22. In total, 57/65 (87.7%) of patients in this audit were compliant with the standard ‘FFP should not be given to non-bleeding patients with PT below 22 seconds’. The national survey demonstrated significant heterogeneity in knowledge and practice of the recommendations of the SIR/CIRSE guidelines. Additionally, 67/68 (98.5%) patients with platelets above 50 × 109/l did not receive prophylactic platelet transfusions, as per BCSH guidelines.
In the critical care setting, an assessment of bleeding risk using the history alone is difficult and laboratory tests of haemostasis are often used to estimate risk of bleeding. However, PT and APTT are poor predictors of bleeding 3 and FFP has a minimal effect on PT and APTT when they are only mildly prolonged. 10 Recommendations regarding platelet number and bleeding risk are largely drawn from studies examining the risk of spontaneous intracerebral haemorrhage in haematological malignancy patients with thrombocytopenia. 11 Little regard is given to platelet function in current guidelines. Consequently, setting thresholds for prophylactic intervention in critically ill patients on the basis of routine tests of coagulation is problematic and is unlikely to be guided by strong evidence. This may account for the variations in clinical practice suggested by our survey of UK interventional radiology practice.
The BCSH guidelines state that ‘there is no justification for using FFP to reverse a prolonged INR in the absence of bleeding’. 5 This audit found that pre-procedural FFP transfusion practice is inconsistent, with FFP often transfused for mild derangement of PT/APTT. These findings have been noted in other studies. 12 There are risks to over-transfusion with FFP, as demonstrated by the single patient in this cohort who developed anaphylaxis. The transfusion of FFP in non-bleeding ICU patients (TOPIC) trial was designed to see whether prophylactic FFP transfusions could be safely omitted. 4 No difference between bleeding in patients given FFP prophylactically and the control group was seen, although the trial closed early due to slow recruitment and did not reach significance for non-inferiority.
A single patient in this audit received a platelet transfusion. This was with a double dose of platelets transfused at above the recommended threshold of 50 × 109/l. This practice appears common in critical care, with a recent large observational study, the intensive care study of coagulopathy, suggesting that over 40% of platelet transfusions are administered without good indication. 13 Clearly, unnecessary transfusion is expensive, depletes a scarce resource and exposes patients to transfusion reactions and infections.
Taken together, these findings suggest that further clarification is needed in the area of coagulopathy and interventional radiology. This is particularly important in critical care where derangements of the traditional laboratory indices of clotting are common and interventional procedures occur frequently. In particular, clinicians need clear guidelines on the role of APTT in predicting bleeding risk and better education in the safety thresholds of PT. Additionally, hospitals should consider the usage of alternative point of care investigations of coagulation, such as thromboelastography, although prospective studies on their impact are still needed. 14 Inappropriate transfusion of FFP may be harmful, and there is currently little evidence supporting its use outside of the context of active bleeding. This lends strength to a position of using FFP therapeutically rather than as prophylactic ‘cover’. 15
Footnotes
Acknowledgements
The authors gratefully acknowledge the assistance of Dr Simon Stanworth for providing critical feedback on the audit protocol and manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.