
Abstract
Background:
Advanced age is an independent risk factor for poor outcomes following aneurysmal subarachnoid haemorrhage (SAH). However, Australian data are lacking. Our aim was to evaluate outcomes for older patients admitted to an Australian intensive care unit for management of aneurysmal SAH.
Methods:
We conducted a single centre retrospective observational study looking at adult patients admitted with aneurysmal SAH to an Intensive Care Unit (ICU) over a 10-year period. Patients were grouped by age; <70 years, 70–79 years, ⩾80 years, and were of sufficient complexity to be unsuitable for our neurosurgical high-dependency unit. The primary outcome was in-hospital mortality. Secondary outcomes were ICU and hospital length of stay, and discharge destination.
Results:
Of 372 patients admitted to ICU with aneurysmal SAH, 302 (82%) were younger (<70 years), 46 (12%) were septuagenarians and 24 (6%) were octogenarians. There were no differences between clinical or radiological grade of aneurysmal SAH between age cohorts. When compared to the patients younger than 70 years, there was increased odds of dying for those 70–79 and ⩾80 years (70–79: OR 1.98, 95% CI 0.93, 4.20 p = 0.077; ⩾80: OR 4.01, 95% CI 1.55, 10.35 p = 0.004). There were no associations between age and duration of admission. Only 6% of patients aged ⩾70 years were discharged home alive.
Conclusion:
It was uncommon for patients over 70 years of age who present with a SAH to be discharged home from hospital, and those aged ⩾80 are four times more likely to die in hospital than younger patients.
Introduction
Systemic improvements in health and declining mortality will see the global population of older adults (60 years or older) double to 2.1 billion people by 2050, with patients aged 80 years or older representing the fastest growing cohort. 1 Accordingly, there will be an increase in the number of elderly patients treated in intensive care units (ICUs) and by 2030 over a quarter of patients admitted to an ICU in Australia will be aged 80 years or older. 2
The incidence of aneurysmal subarachnoid haemorrhage (SAH), increases linearly with age and is three- to four-fold greater in people aged over 70 years compared to younger cohorts. 3 Up until the 1970s, active management and neurosurgical intervention were considered futile in older patients and conservative management was advocated in those aged 60 years or older. 4 With improved surgical techniques, aggressive vasospasm management and the advent of endovascular coiling, population based survival rates have improved dramatically for SAH, including in older people, such that active management and neurosurgical intervention is now widely adopted in this cohort.5 –7 As a result, the number of older patients with SAH requiring intensive care is increasing. 6
Several international observational studies,8 –14 and one Australian study 15 have identified advanced age as an independent risk factor for poor functional outcomes following SAH. Few contemporary studies from the endovascular treatment area have compared outcomes between younger and older patients with SAH.6,16,17 There is no data specifically examining the Australian population admitted to the ICU. This is important given the recognised heterogeneity in SAH prevalence and management globally. 18
Our aim was to compare aneurysmal SAH outcomes between older and younger patients admitted to a large Australian intensive care unit. We hypothesised that older age would be independently associated with increased hospital mortality.
Methods
We conducted a single-centre retrospective observational study of consecutive patients admitted to the Royal Melbourne Hospital ICU with a diagnosis of aneurysmal SAH. 19 The Royal Melbourne Hospital is a large mixed medical-surgical ICU providing neurosurgical critical care to a catchment of approximately half a million people. 20
We screened all adult patients over a 12 year period (January 2009–December 2020) admitted to the ICU with a principle diagnosis of ‘Subarachnoid Haemorrhage’ recorded on the ANZICS (Australian and New Zealand Intensive Care Society) Adult Patient Data Base. 21 Patients with non-aneurysmal SAH attributed to infection, trauma or arteriovenous malformations were excluded, as were patients without an aneurysm found on imaging. Patients who were transferred from another hospital after primary intervention, or who were admitted for elective clipping or coiling were excluded. Patients who were palliated before transfer to ICU were excluded.
Demographic characteristics, processes of care, mortality and discharge destination data were recorded from the ANZICS Adult Patient Database. 18 Patient medical records were then reviewed to extract the following variables: SAH severity using the World Federation of Neurosurgical Societies (WFNS) grade, treatment modality (conservative, endovascular coiling or neurosurgical clipping) and complications including rebleeding, acute hydrocephalus necessitating treatment with an external ventricular drain, cerebral vasospasm and ventriculitis. We diagnosed cerebral vasospasm radiologically on computed tomography (CT) angiography or digital subtraction angiography findings. Admission CT scans were evaluated and graded according to the modified Fisher scale. 22
Our primary outcome was in-hospital mortality. Our secondary outcomes were ICU and hospital length of stay (days), and disposition at hospital discharge.
Data analysis and statistics
We sub-classified older patients into two cohorts; septuagenarians aged 70–79 years6,9,23 and octogenarians or older (⩾80 years). 24 For the binary outcome of hospital mortality, we fitted a multivariable logistic regression model, which included WFNS grade as a confounder. For the outcomes of ICU and hospital length of stay, we fitted Cox proportional regression models. Finally, we assessed if there was an association with time and the number of aneurysmal SAH admissions overall by fitting a negative binomial model, and then assessed if the association varied by age group by fitting an interaction term in the negative binomial model between age group and time.
The Melbourne Health Human Research Ethics committee approved the study and waived the need for patient consent (HREC QA2019089). The study was conducted according to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. 25
Results
Between January 2009 and December 2020, 534 patient records were reviewed against the eligibility criteria. Of these, we identified 372 eligible patients admitted to the ICU with a principal diagnosis of aneurysmal SAH (Figure 1). The median [interquartile range, IQR] age was 57 [49–66] years and 233 (63%) patients were women. Clinical characteristics and processes of care data by age cohort are presented in Table 1.
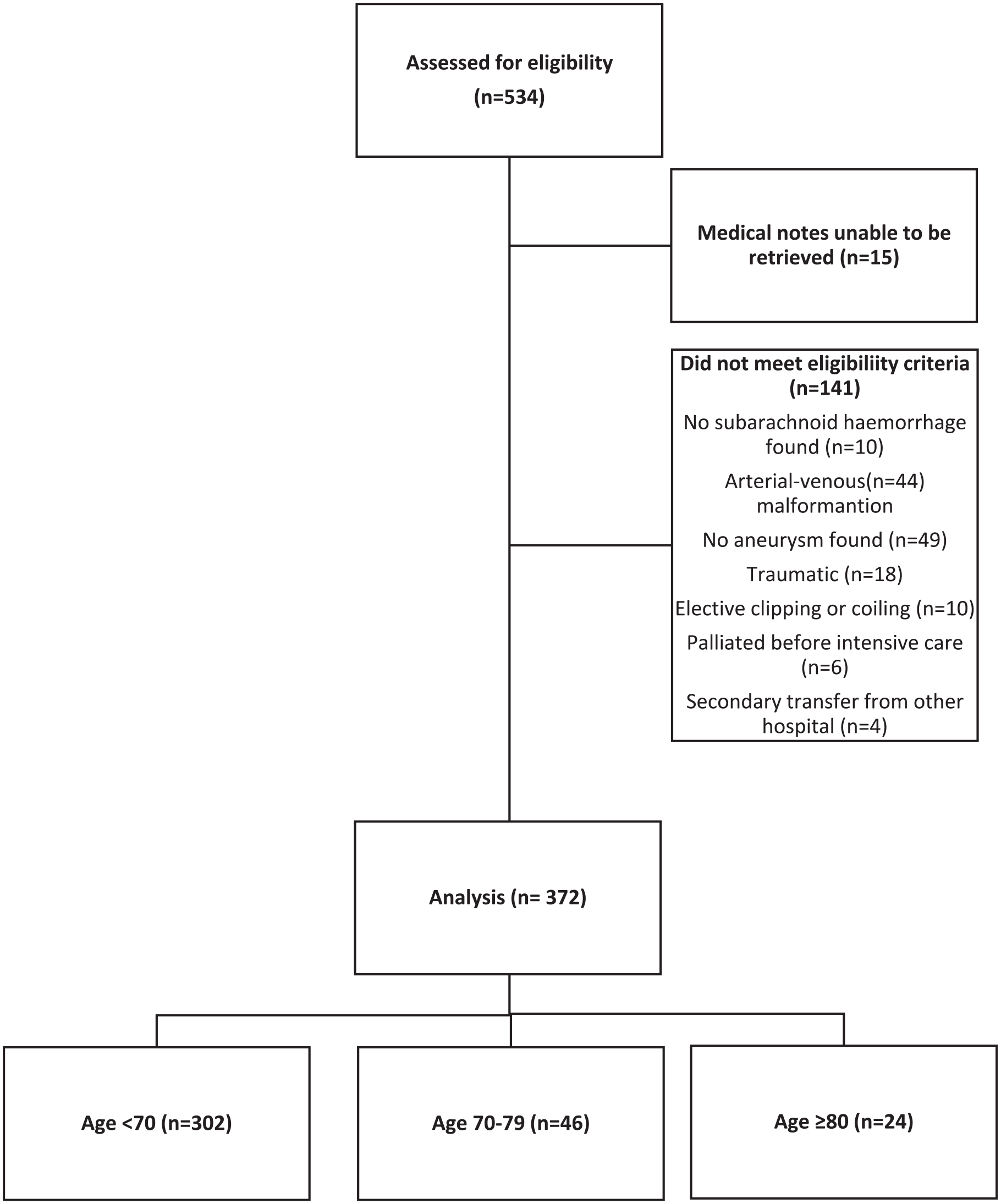
Flow diagram demonstrating patient inclusion, exclusion and analysis.
Demographic and clinical characteristics, processes of care and complications.
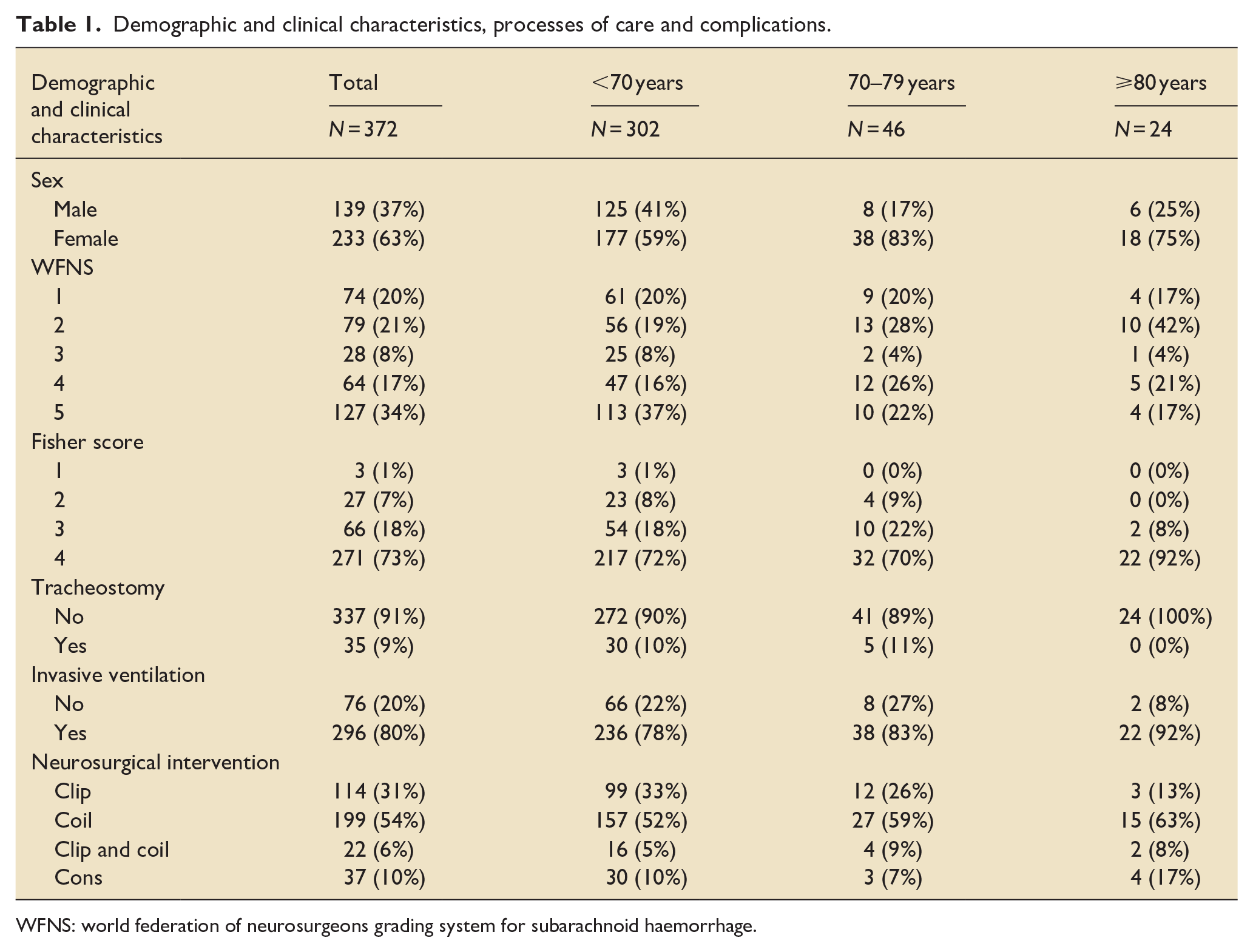
WFNS: world federation of neurosurgeons grading system for subarachnoid haemorrhage.
There were 302 (82%) patients younger than 70 years, 46 (12%) septuagenarians and 24 (6%) octogenarians. No patient was older than 89 years. There were a greater proportion of women in the older cohorts.
A greater proportion of patients younger than 70 years had the most severe WFNS grade of aneurysmal SAH (Grade 5) (Table 1), whilst older patients were most likely to have grade 2 aneurysmal SAH (Table 1). There were no differences in interventional management strategy by age cohort (Table 1), with most patients (i.e. >50%) undergoing coiling across all age groups. Most patients received invasive ventilation during their ICU admission (Table 1). No patients in the ⩾80 years group were tracheostomised. (Table 1).
In terms of complications (Table 2), the proportion of rebleeding, hydrocephalus necessitating an extra ventricular drain, cerebral vasospasm, and ventriculitis were similar between age groups. There were 119 (32%) deaths in hospital. Compared to patients younger than 70 years, there was a two-fold increase in the odds of dying for those 70–79 years of age (OR 1.98, 95% CI: 0.93, 4.20 p = 0.077), and there was a four-fold increase in the odds of dying for those ⩾80 years of age (OR 4.01, 95% CI 1.55, 10.35 p = 0.004) (Table 3). Only four patients that were 70 or older were discharged home (Table 4).
Complications.
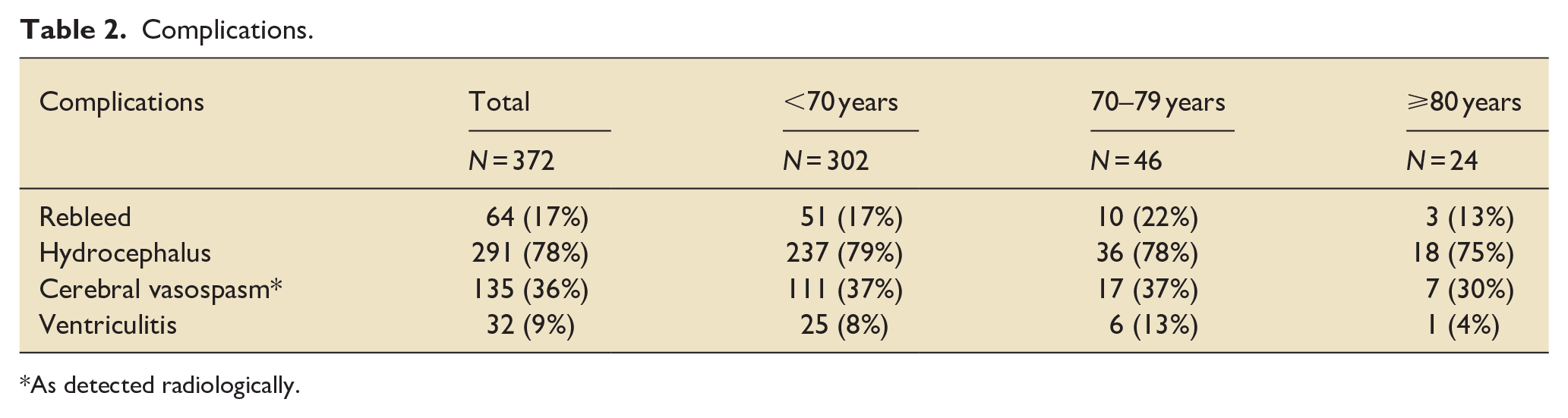
As detected radiologically.
Association between age group and mortality.
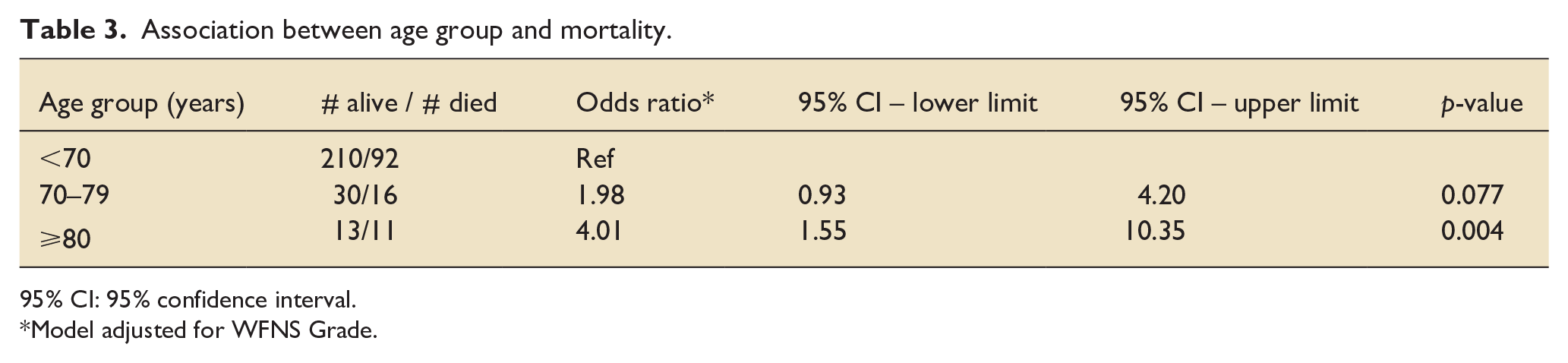
95% CI: 95% confidence interval.
Model adjusted for WFNS Grade.
Cross tabulation of age group and hospital outcome.
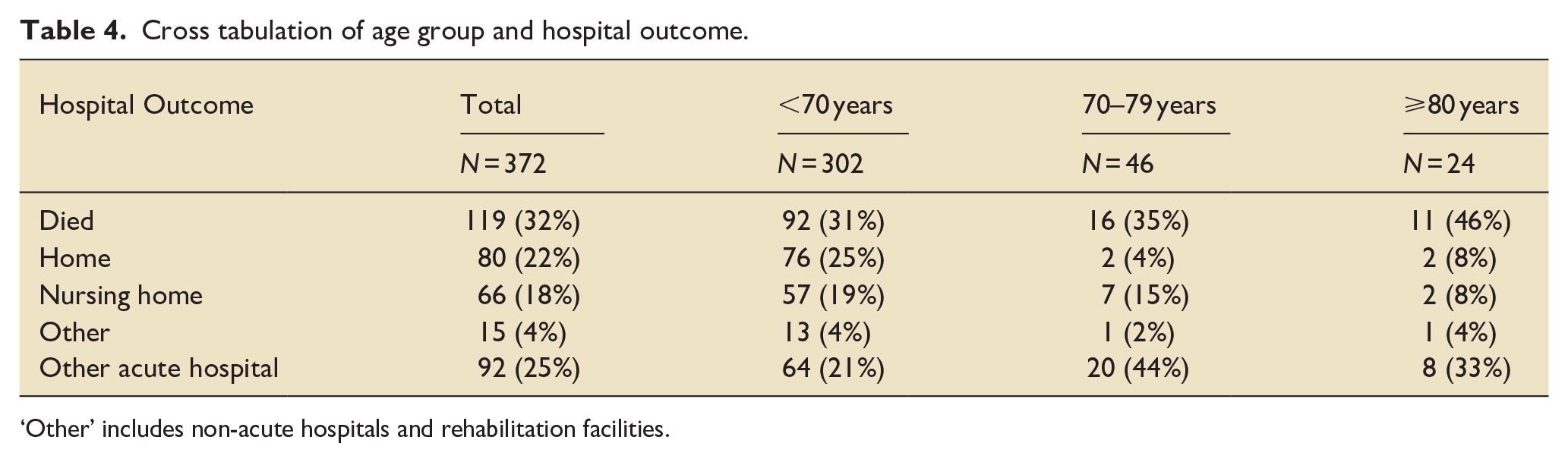
‘Other’ includes non-acute hospitals and rehabilitation facilities.
Overall, the median ICU length of stay was 106 [48–199] hours and hospital length of stay was 419 [190–647] hours. There was no association between age group and ICU length of stay (Supplemental Tables 1 and 2).
Over the 12-year period of observation there was no significant change in the number of aneurysmal SAH ICU admissions per year (Figure 2) and there were no associations between time and number of admissions by age group (Supplemental Figure 1).
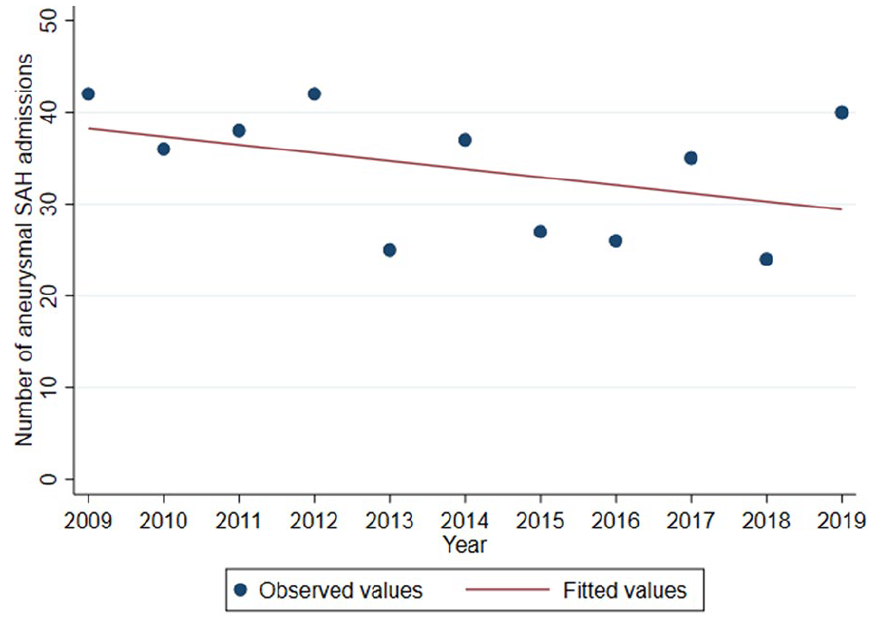
Association between time and number of admissions.
Discussion
There are two key findings from this observational study of outcomes by age group in patients admitted to an Australian ICU with SAH. Firstly, there was an associated four-fold increased odds of death in patients aged 80 and older compared to those younger than 70 years of age. This is despite a lesser incidence of high clinical grade bleeds and no differences in interventions or complications when compared with the younger age group. Secondly, less than 10% of older patients (⩾70 years) were discharged to independent living.
While older age is frequently purported to increase the risk of death and poor functional outcome following aneurysmal SAH,8 –14 few studies have compared outcomes between younger and older cohorts.6,16,17 While there is consensus that older age portends a poor prognosis there are key demographic differences between prior comparative observational studies from Japan, 16 Finland 6 and the United States 17 and our Australian population. 15 Internationally, there are marked regional differences in SAH incidence with Japan and Finland recording twice as many SAH per capita than the global average. 26 Moreover, in Japan, the increase in age specific incidence rises more steeply, with a higher proportion of older SAH patients than the rest of the world. 26
Utilising the modified Rankin score, Hironake and colleagues compared functional outcome at hospital discharge between 54,806 Japanese patients with SAH aged <60 years (n = 20,525), 61–70 years (n = 13,616), 71–80 years (n = 11,966), 81–90 years (7613) and ⩾91 years (n = 1085). 16 Older patients tended to have lower consciousness on admission and were less likely to have the aneursym secured by microsurgical clipping. 16 The proportion of poor functional outcomes at hospital discharge increased with patient age; approximately one third of younger patients had a poor functional outcome at hospital discharge, this proportion increased to over two-thirds in septuagenarians, 86% in octogenarians and was nearly ubiquitous in those aged over 90 year (94%). 16
In a single-centre retrospective observational study conducted in Finland, Valimaki and colleagues compared functional outcomes at 12 months between 95 older (⩾70 years) and 317 younger (<70 years) patients with aneurysmal SAH. 6 They only included patients receiving active aneurysm treatment and the acuity of this cohort was lower than the population in our study. In our study the majority of patients had high grade SAH (WFNS 4-5) requiring an extra-ventricular drain, whereas in the Finnish study only one third of patients had a high grade SAH and less than half developed acute hydrocephalus. Valimaki and colleagus report a very low ICU mortality of 2% that was comparable between age cohorts and susbtantially lower than the 32% overall mortality reported in our study. Functional outcomes were worse in older Finnish patients compared with the younger cohort. 6 Outcomes were particularly poor in older patients with high grade SAH with most being dependent at 12 months. 6
In a pre-planned, post-hoc analysis of the Barrow Ruptured Aneurysm Trial study from the United States, Catapano and colleagues compared long-term functional outcomes between 77 older (⩾65 years) and 328 younger (<65 years) patients with aneurysmal SAH who had been randomised to either microsurgical clipping or endovascular coiling. 17 The acuity of this cohort was similar to the Finnish study, with an overall ICU mortality of less than 5%, which did not differ between age cohorts. Whilst only one in ten older patients were independent at hospital discharge a substantial proportion regained independence at later years.
Our data, together with the international experience, highlight the high burden of immediate dependency among older patients who survive an admission to an ICU after a SAH. While age alone should not predicate the decision for active management of SAH, these data can help clinicians frame consent for active intervention. Our study is limited by the absence of long-term functional outcome data; however the Finland and US experiences suggest that, at least in their lower acuity populations, some older patients improve after extended rehabilitation and are able to live independently 12 months later.6,17 Our study is also limited by including only those patients admitted to the ICU. The Royal Melbourne Hospital has a co-located neurosurgical high-dependency unit which admits most self-ventilating patients with SAH. This may account for the high complication and mortality rate and limits the external validity of our findings. We do not have data on patients that were refused admission to ICU on the basis of futility or data regarding withdrawal of life sustaining treatment for those admitted to the ICU. Due to the small number of patients that met the eligibility criteria, we were unable to undertake more detailed analysis of risk factors for mortality by age cohort, particularly by treatment intervention as has been reported in other comparative studies.6,16,17 Similarly, frailty scores were not reported and we were unable to include these in our adjusted analyses. Finally, there is uncertainty in the estimates of delayed cerebral ischaemia as it was inconsistently documented in the medical record.
Conclusion
Older patients admitted to an Australian neurosurgical ICU had greater in-hospital mortality rates when compared to younger patients, and less than 10% of older patients were discharged home.
Supplemental Material
sj-docx-1-inc-10.1177_17511437241301916 – Supplemental material for Outcomes for older patients with subarachnoid haemorrhage who require admission to an Australian intensive care unit
Supplemental material, sj-docx-1-inc-10.1177_17511437241301916 for Outcomes for older patients with subarachnoid haemorrhage who require admission to an Australian intensive care unit by Jeremy Sharman, Natasha Turner, Amalia Karahalios, Ben Sansom, Adam M Deane and Mark P Plummer in Journal of the Intensive Care Society
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.