
Abstract
A distinction has been drawn between basic (pure) conversation analysis (CA) and applied CA. Applied CA has become especially beneficial for informing areas of practice such as health, social care and education, and is an accepted form of research evidence in the scientific rhetoric. There are different ways of undertaking applied CA, with different foci and goals. In this article, we articulate one way of conducting applied CA, that is especially pertinent for practitioners working in different fields. We conceptualise this as Reflective Interventionist CA (RICA). We argue that this approach to applied CA is important because of its emphasis on the reflective stance that is valuable to an understanding of research data, its commitment to collaboration with practitioners, and its inductive style. In this paper, we outline the core premises and benefits of this approach and offer empirical examples to support our argument. To conclude, we consider the implications for evidence-based practice.
Introduction
Globally there is a growing emphasis for researchers to produce research outcomes that have some impact on practice. One approach that is increasingly being recognised as valuable to achieve that is applied conversation analysis (CA). Stokoe’s (2014) influential scholarship, for instance, highlighted how applied CA can be used to create a training model to inform and alter how people interact in organisations. More recently, Lester and O’Reilly (2019) argued that applied CA is a useful approach because it can make significant and important contributions to the evidence-base of any practical discipline. Antaki (2011) provided a useful typology outlining the various ways applied CA has been conceptualised, one of which was Interventionist CA. We proffer that there is a particular way of doing applied interventionist CA that has found utility amongst practitioners using practice-based data to inform their work. The distinguishing feature of this approach to interventionist CA is that it does not focus on the need to address an a priori problem. We introduce the terminology of Reflective Interventionist Conversation Analysis (RICA) to capture this way of engaging with applied CA. To offer a foundational understanding of the evolution of CA into the various forms of applied CA, and more recently into RICA, we begin with an abbreviated overview of its historical development. We then describe the distinctives of RICA, drawing upon a common dataset to illustrate the key points.
Abbreviated history
CA attends to the organisation of talk, examining how turns are designed to perform social actions (Sacks, 1992). Conversation analysts examine how interlocutors make sense of and respond to one another in talk and are interested in the interactional organisation of everyday and institutional social activities (Lester and O’Reilly, 2019).
Harvey Sacks, a leading pioneer of CA, studied with Erving Goffman and was influenced by ethnomethodology. Notably, Sacks found considerable resonance with the work of Garfinkel (Silverman, 1998) and became interested in studying mundane activities as a legitimate focus of inquiry for sociologists (Pomerantz and Fehr, 1997). Sack’s interest in the ethnomethodological approach of unmotivated looking (Sacks, 1984) ultimately shaped a central premise of CA; that is, people’s talk is not merely descriptive, rather conversation is a site of social action (Drew, 2004). Sacks developed many of the core ideas that are now considered foundational in CA (see Sacks, 1992).
Contemporaries of Sacks included David Sudnow, Emmanuel Schegloff and Gail Jefferson. Jefferson reproduced his lectures and developed the associated CA transcription system. Sacks’ primary influence was ethnomethodology, whereas for Schegloff it was sociolinguistics. An important transition in the trajectory of CA was when Schegloff posthumously took over the work of Sacks, it naturally developed a more sociolinguistic flavour, especially because of his appointment in Applied Linguistics at UCLA. Modern CA has largely retained this sociolinguistic alignment.
During the 1980s CA became popularised and developed a more interdisciplinary focus, with contemporary CA researchers representing different fields. The second major evolutionary transition was signalled by the publications of ‘Order in Court’ (Atkinson and Drew, 1979) and ‘Talk at Work’ (Drew and Heritage, 1992). A distinction therefore emerged between CA’s focus on mundane talk (i.e. ordinary everyday talk) and institutional talk (i.e. deals with institutional business). Following this, researchers recognised that CA could be used to inform practice, and a differentiation emerged between ‘pure’ (or basic) CA and ‘applied CA’. For the most part the term applied CA was used to refer the application of CA to institutional business and investigated how those interactions were organised as institutional interactions (ten Have, 2007). Although the application of CA has predominantly been focused on institutional settings it has always been recognised that CA could and has been applied to mundane conversations (Lester and O’Reilly, 2019). Therefore, its defining feature is not the type of data or setting analysed, but the way the analysis is applied. One might additionally argue that there is a difference between the intentionality of a researcher who sets out to conduct a piece of research that will have a practical application compared to a piece of work that is conducted purely on the basis of unmotivated looking that is retrospectively considered to have a practical application. We would argue that applied CA is intentional at its outset that there will be some form of practical application of the findings.
The developments in applied CA were situated within the larger context of the discourse of evidence-based practice. The evidence-based practice movement emerged in the field of health and advocated for a new form of clinical decision-making which explicitly synthesised outcomes-based research, user-experience, and clinical judgement (Sackett, et al., 1996). The underpinning assumption of this drive was that best practice should be developed and informed by appropriate evidence (ibid.); an ideology that has become embedded in many fields of practice since. In addition, practitioners are actively encouraged to contribute to that evidence-base by engaging in research and/or partnering with academics. A starting point for many applied researchers working within the paradigm of evidence-based practice is to seek to address an identified problem in the institutional setting. Thus, within the environment of applied research in which applied CA is often located, there is a common understanding that the research endeavour begins with a focus on identifying solutions to pre-existing problems (Bickman and Rog, 2009). However, we argue that for CA research to be conceptualised as applied rather than pure it is not always a necessary or even desirable pre-requisite that there would be a pre-defined problem which the analysis seeks to redress. It is entirely appropriate to conduct applied CA from the perspective of wishing to inform practice that may or may not identify areas that require improvement or change and may or may not identify areas of existing good practice.
Applied CA
Over time CA has earned respect across a range of disciplines, and different practitioners have “developed distinctive styles of working and a variety of analytical preoccupations, major domains and subdomains of study have crystallized”, with researchers from across different disciplinary fields developing partnerships with each other (Heritage, 1999: 69). Notably, however, many conversation analysts do not actively or intentionally position themselves within the wider applied research paradigm. In our experience, even applied CA researchers often consider themselves as conversation analysts first and applied researchers second (if at all). In other words, many analysts utilise their CA work to apply it to practice, rather than setting out to be an applied researcher who happens to use CA as one methodological approach in their repertoire. Although not all applied CA is focused on institutional talk, there is often a focus on using CA to address an interactional ‘problem’ (Antaki, 2011). While recognising that there are debates regarding what constitutes institutional interactions (see for discussion, Lester and O’Reilly, 2019), they typically have linguistic and structural characteristics that distinguish them from mundane conversations, and are often explicitly connected to the topic of the institutional business and setting within which they are produced. For example, one aspect of such talk is that the professional identities and institutional agendas are often made relevant via the working activities in which the speakers are engaged (Drew and Heritage, 1992). Thus, the turn-taking organisation and sequence organisation of institutional interactions are commonly different from mundane talk (Heritage, 2005).
With the growth of popularity of applied CA in different institutional contexts, several different approaches to using CA in these arenas have emerged. A significant voice in the area of applied CA has been Charles Antaki. In a seminal book, Antaki (2011) identified six primary ways of undertaking applied CA. These were: 1) Foundational, which seeks to reframe foundational concepts within a discipline such as psychiatry or psychology; 2) Social-problem-oriented, which posits that pre-existing ‘social problems’ can be analysed through CA practices; 3) Communication, which seeks to identify the features of what has been constructed as disordered talk; 4) Diagnostic, which seeks to correlate speech patterns with a medical diagnosis; 5) Institutional, which explores the distinctive features of conversations that constitute institutional business and distinguish it from mundane talk; and 6) Interventionist, which assumes pre-existing problems and works to offer solutions based on CA findings.
Notably, two ways of doing applied CA were positioned as not taking a problem or deficit-focused starting point, that is, foundational (1) and institutional (5), whereas four of these six (2, 3, 4, 6) were positioned as a response to an a priori problem for which CA was deemed useful to address. Of relevance to the current discussion is that one of these is interventionist CA. Wilkinson (2014) explained that interventionist CA is an approach that aims to ‘change some feature(s) of the conduct’ of participants within the interaction. In addition, Wilkinson noted that in this approach, participants might be actively involved in decisions about what conduct should be targeted for change, and there is a consideration of the implications of findings for the participants being analysed.
It is recognised that interventionist CA is a valuable approach for applied researchers. However, we wish to identify a subtle differentiation between the kind of interventionist CA that explicitly has a goal of change in practice and the type of interventionist CA that retains a stance of unmotivated looking. Thus, in this article, we propose to refer to this way of doing analysis as Reflective Interventionist CA (RICA). Aligned with Wilkinson’s description, RICA retains the characteristic features of interventionist CA that it; a) involves participants in partnership and b) considers the implications of the findings for those participants. However, it also has a broader goal to notice what is happening in the interaction without identifying a problem as its starting point. As part of the participant partnership focus, RICA emphasises the value of participant/analyst reflection. This leads to the potential of identifying either practices that are working well and/or areas that may benefit from change. Thus, there are two potential outcomes of a RICA study:
The identification of good practice so that best practice might be used more, or more in certain situations it can be articulated in a tangible way as a pedagogical tool for training purpose
The identification of areas for change or improvement may emerge but this is not necessarily the goal.
While interventionist CA does not have to be institutionally focused (see e.g. Beeke et al’s, 2014 analysis of communication between an aphasic man and his wife), much of the work does examine talk in institutional settings. For example, a recent review showed there has been a surge of interest from applied disciplines in the value of CA studies to improve practice (Barnes, 2019). Barnes illustrated that in the context of medical encounters, CA can illuminate examples of best practice, can inform recommendations, and can inform change via training. Examples of interventionist CA include; the use of specific training workshops for doctors to effectively design questions (Jenkins and Reuber, 2014); to shape discursive practices of mediators for effective communication (Stokoe, 2014); and to identify strategies to improve effectiveness of telephone helpline services (Hepburn et al., 2014).
Method and analysis: Reflective Interventionist Conversation Analysis (RICA)
Thus far, we have acknowledged the aligning features of RICA that are foundational to interventionist CA and explained the way that it also encompasses the potential for explication of good practice as well as identification of areas for change. We now turn our attention to the details. The defining characteristics of RICA are that: a) it is responsive to and emphasises reflection on practice through the process; b) it takes a collaborative and/or co-production starting point between academics, practitioners and/or clinical academics; c) it is an inductive inquiry approach which is not deficit-driven; d) it prioritises unmotivated looking as an iterative practice; e) it has a goal to identify implications for practice and communicate this through accessible language. We address each of these in turn with illustrative data and examples to present a pedagogical framing of how one might undertake a RICA study. To exemplify each of these aspects we draw upon a data set (described below) that epitomises the RICA approach.
The mental health assessment study
Our analytic examples are drawn from one specific research study whereby we utilised the approach to applied conversation that we now refer to as RICA. The focus of this study was on initial child mental health assessments from a mental health service in the UK. These assessments included a multidisciplinary team of 29 practitioners of consultant, staff-grade and trainee child and adolescent psychiatrists, clinical psychologists, assistant psychologists, community psychiatric nurses (CPNs), occupational therapists and psychotherapists. The assessments were approximately 90 minutes long, were video-recorded and occurred naturally in practice. In total, 28 families participated, with 64% boys and 36% girls, aged 6 to 17-years-old. Children and young people attended with their families (27 mothers, 7 fathers), and some with siblings, extended family members and/or other practitioners. Data were transcribed using CA conventions of Jefferson (Jefferson, 2004) and were analysed using CA within the RICA framework; the characteristics of which now follow.
Reflection on practice
Throughout any given RICA informed project, reflection on practice is foundational. Reflective practice is central to the work of many professional disciplines, and a distinction is made between reflective practice and reflexivity. Reflection is defined here as the process of reviewing practice both at the time of and after an event, which Schőn (1983) describes as ‘reflection in action’ (occurring during the interaction) and ‘reflection on action’ (occurring retrospectively after the interaction). That is, reflection involves considering any process that is engaged in and the application of theory to practice (Taylor and White, 2000). When reflecting on practice, practitioners typically rely on their memory, written notes, and some may have recordings used for supervision, but they do not usually have a word-for-word transcription. The advantage of adding rigorous analysis of transcription to the reflective cycle is that more in-depth learning can be achieved. This is where RICA is especially pertinent. For those using RICA, both the academic team and practitioner team actively encourage one another to engage in reflection. For instance, the practitioner team is encouraged to engage in active reflection ‘on action’, while the academic team is encouraged to produce a reflective analysis that promotes application and translation of CA knowledge. Furthermore, RICA attends to the real-world practices of professionals and their reflections on those practices. When combined with the core findings from the CA, the new types of knowledge created provide a basis for any change or new ways of working, as well as identification of best or good practices that can help advance a field.
Here we present several data examples, wherein we identified discursive practices that were analysed and subsequently shared with practitioners. The knowledge gained was ultimately woven into practice. We present the data examples for context, and then illustrate the relevance of RICA subsequently. In the following extracts we focus on concerns pertaining to a potential diagnosis of Autism Spectrum Disorder (or ‘Condition’ as many scholars prefer). Our analysis highlighted that families frequently presented a candidate diagnosis during assessments, and one such possibility was autism. They did this in various ways, but often simply presented it as an option:
Example three: Family 16 (from O’Reilly et al., 2017: 73)
Example four: Family 5 (From O’Reilly et al., 2017: 74)
At the decision point of the assessment therefore, the proposals put forward by family members are accounted for in the sequence of conversation as the two practitioners provide a decision regarding the outcome of the institutional business. Using CA, we were able to address the sequential nature of the interaction and examine how practitioners attended to a prior candidate diagnosis. Our close interrogation of the data resulted in noting something unexpected and interesting. While intuitively there is a sense that a concern for autism would not be a positive outcome of an assessment, analysis revealed the contrary. When confirmation of the candidate diagnosis proposed by families was offered by practitioners, it was done so quickly, easily and by one practitioner (consistent with agreement); yet when the candidate diagnosis was disconfirmed, it was performed over a protracted series of turns, was complex and performed by both practitioners in collaboration (consistent with disagreement) (see O’Reilly et al., 2017 for full discussion). We show one example of each for illustrative purposes.
Example five: Family 24 (from O’Reilly et al., 2017: 78)
Example six: Family 22 (from O’Reilly et al., 2017: 78 – see this paper for the full extract)
The analysis of these data facilitated both reflection of the individual practitioners involved in the mental health assessments, as well as collective reflection within the team. This happened in several stages with individuals and groups in various settings. We deal with each of these in turn.
First, both practitioners and academics constituted the research team that analysed the data from this project. Notably, practitioners within the research team may or may not be the same practitioners that were involved in the institutional interactions being analysed. In this case, some practitioners from the institutional setting did participate in analytic development, and other practitioners in the research team did not. In the cases of practitioners not reflecting on their own personal practices, but reflecting on others’ practices, they were involved in the same field. The benefit of these partnerships is that during the inductive inquiry, practitioners can notice social actions within the talk that may be valuable for further attention. This primarily occurred through the distinctive process of reflecting on action. Thus, through this collaborative endeavour the analysis was developed with both an analytic and applied focus.
Second, post analysis, a collaborative workshop was organised for the academics involved in the project and the participants in the assessments to actively involve the practitioners who provided the data. The findings were initially presented, including this autism specific data, allowing for an additional tier of reflection. In this setting it was not possible for practitioners to reflect on their own personal practices because of the need for anonymity in the data. However, reflective discussions centred around communicating with children and young people, good practices, and decision delivery. Specifically, in relation to decision delivery of the possibility of ASD, one of the learnings from this reflective process was that when delivering decisions that are contrary to parental expectation, it is useful to do so in a collaborative way with both practitioners contributing, that combines their expertise and reinforces the validity of their diagnosis.
Third, one of the practitioners involved in the study was able to utilise the data to reflect on their own personal practice. In addition, the same practitioner was able to facilitate similar reflection on practice for other participants through individual supervision by watching excerpts of video and reading through transcripts. The value of such reflection was made possible by the naturally occurring data, which allowed these participants to focus on areas of their own practice related to how they deliver decisions to families.
Fourth, using the whole corpus of data and the analysis of several practitioners it was possible for this practitioner to teach trainees about good practice and lessons learned from close engagement with data. Thus, when trainees are engaged in real-world practices and families propose candidate diagnoses of autism, they were able to learn lessons of good practice for delivery of both confirmatory and non-confirmatory decisions.
In summary, these four areas represent different lenses through which different combinations and subsets of practitioners were able to reflect on practice. This was facilitated by the academic practitioner collaboration. In other words, the workshop allowed for reflective discussion between the academic and practitioner (participant) team; the individual review of the naturally occurring data enabled practitioners to reflect on their own practices; and trainees (via supervision) were encouraged to engage in reflection on practice as they learned lessons from the analysis of the wider data corpus and through the collective action of the practitioner and academic team. While we do not claim that using participant feedback forums such as this to engage practitioners is unique to RICA, it is one way that robust analysis of institutional data can be disseminated so as to invite further discussion about application to practice.
Collaborative and co-produced
A central feature of RICA is that is that it is based on the premise of collaboration, in the sense that the practitioner(s) is/are engaged and involved in the entirety of the research process. Engaging and collaborating with practitioners from the outset to the conclusion ensures research ‘success,’ promotes buy-in from key stakeholders, and also provides a mechanism for feeding back into practice, ensuring a bi-directional relationship between the practitioners and academics. Collaboration also ensures respect for local and practice-based knowledge in the generation of the data and analysis. In other words, it creates an iterative evidence model that accounts for practitioner knowledge, scientific endeavour and the generation of evidence that is practitioner-informed, knowledge-based, and scientifically robust. Furthermore, the collaborative style of RICA ensures that there is knowledge-sharing and knowledge-generation between practitioners and academics, with knowledge translation built into the process. In some cases, RICA can be pursued as a co-production, with a strong commitment to a participatory approach to designing and carrying out the research. In other words, for some data collection and analytic processes a co-applicant(s) on the project and co-analyst in the procedure is also an experienced practitioner who may or may not also be a participant in the data. This equal partnership facilitates a co-production and is a beneficial aspect of RICA because of the contextual and situated insights and expertise of the co-producer. Figure 1 is a diagrammatic representation of a non-collaborative approach to knowledge production and dissemination where the production of knowledge through research sits with the academic, who disseminates to journals and books, which the practitioner then takes initiative to access and apply to practice themselves. Figure 2 represents the co-production of research knowledge that is facilitated by the academic and practitioner partnership.
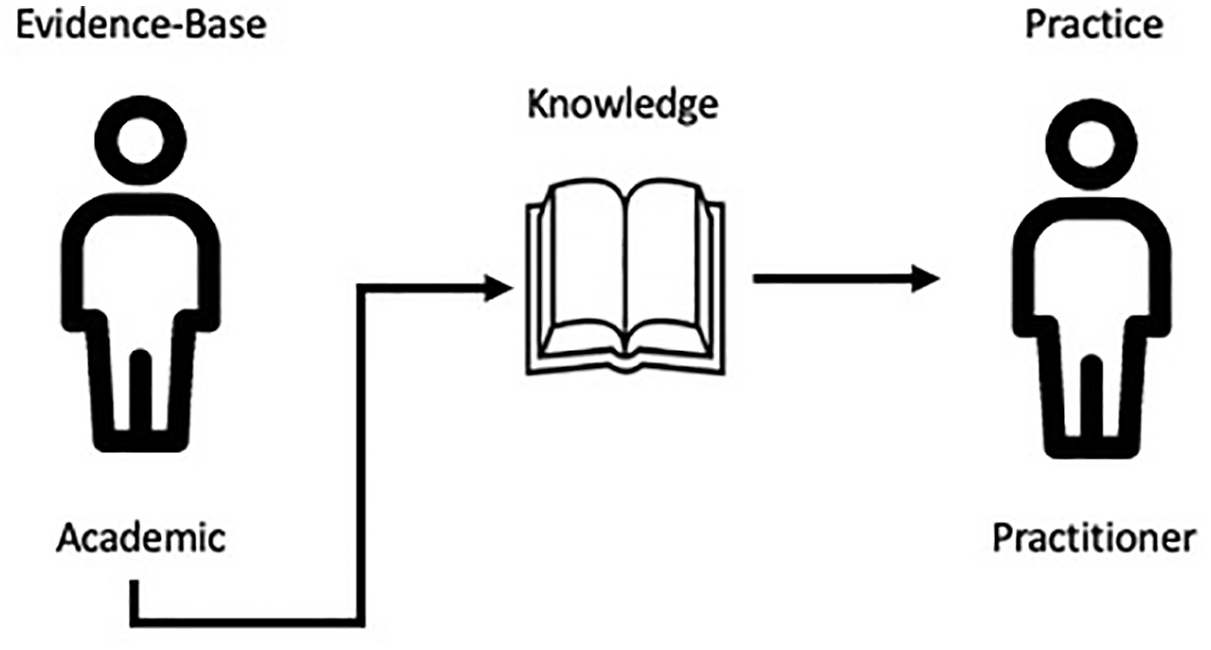
Non-collaborative knowledge production and dissemination.
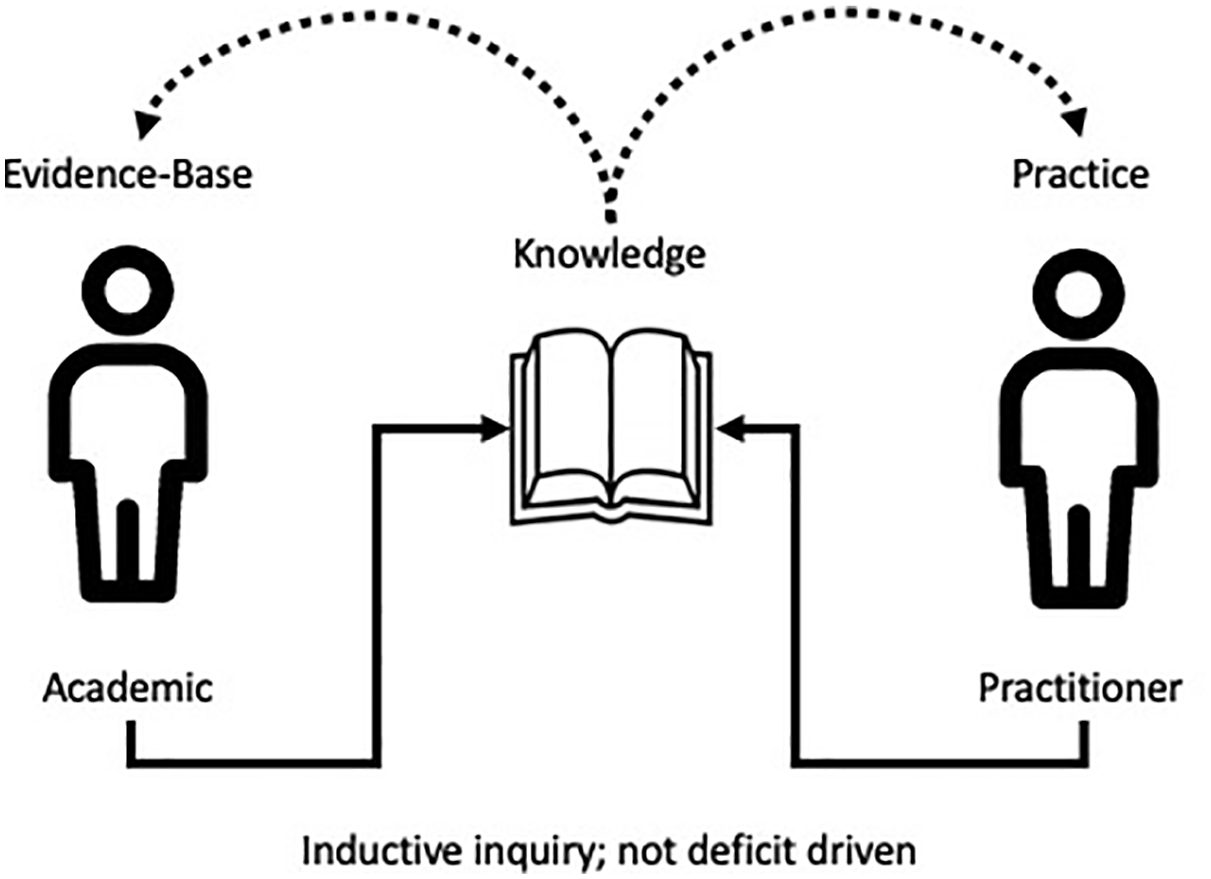
Collaborative knowledge production and dissemination.
Inductive inquiry; not deficit-driven
CA is an inductive, data-driven, and emic form of inquiry. In some ways of undertaking applied CA, it is acceptable as part of the process to identify an a-priori problem of focus, which acts as a starting point for interrogating the data. However, in RICA, this problem-focused, potentially deficit-driven agenda is not the starting point. During the process of inductive inquiry, there may be deficits or problems that come to be identified, but importantly, the analyst does not start out with a practice-based problem or deficit to drive the creation of the research question. Rather, an analyst who positions their work as RICA does not assume before beginning collecting or analysing data that there is a specific problem of practice that needs to be explicated and consequently changed. Rather, the focus is on how the institutional business unfolds and how institutional goals are accomplished through social interaction.
Indeed, some institutional business is by its nature problem-oriented, such as courts that seeks to identify criminal action. However, we suggest that there is a distinction between the institutional business of problem resolution and the analyst’s frame of reference when approaching a study generally and data specifically. That is, a researcher using RICA does not set out to align with the institution’s problem-discourse. Instead, they aim to come to the context with the assumption that the work being done is meaningful and full of potential insights. Aligning closely with discursive approaches generally, RICA presumes that analysis functions to make the tacit visible, and, through this visibility there are possibilities for learning from those engaged in the institutional work.
A good example of this was when questions about how practitioners talk about risk were highlighted as a focus for approaching our data set. Within our broader question about how mental health assessments are conducted, our analyses led to the identification of certain conversational practices resonating with risk-based questioning. Prior to analysis, neither, the practitioners nor academics had identified a ‘problem’ with a way in which staff were asking their clients about risk. Thus, the initial research question was not focused on explicating the ways in which practitioners engage with their clients on the topic of risk management. However, upon closer interrogation of those practices it was noticed that within the corpus of 28 families only 13 were asked about risk. Through adherence to the inductive philosophy and discussions about findings with practitioners it was consequently identified as an area where they could improve their practice with regards to more consistently requiring practitioners to ask about risk. Furthermore, through engaging with RICA, we collaboratively noted that there were ways in which these risk questions (about self-harm and suicidal ideation) were asked where children/young people responded in detail. From this descriptive information, practitioners were able to make clinical judgements about good practice; and we present two such examples below (see O’Reilly et al., 2016).
Example one: From Family 18 (O’Reilly et al., 2016: 483)
Identified through analysis was that some practitioners in attending to risk questions did so in an incremental style. When interrogating the sequential nature of the question-answer sequences, analysis showed that practitioners slowly built up to questions of a more sensitive nature. As can be seen in this example, the practitioner (a psychiatrist) began with an emotional regulation question about showing frustration. The nature of the analysis revealed a risk of harm to self and this was actively pursued by the practitioner or hurting yourself? Once this shared knowledge was established the practitioner moved to the specific as the child revealed suicidal ideation. Through the reflective process of RICA, with consultation between the academics and practitioners, it was identified that such an incremental style of questioning constitutes good practice and was a useful revelation for clinical change. The second example shows a different approach to question design.
Example two: Family 21 (O’Reilly et al., 2016: 484)
By interrogating the data inductively, a second question design for assessing risk was identified. As this extract illuminates, some practitioners utilised a normalising question to elicit information about self-harm and suicide from children and young people. Using a phraseology that presents the question as a routine part of an assessment agenda, it indicated that this young person had not been singled out for the question. Again, consistent with the RICA approach, practitioners were engaged in discussion about this type of question design and they identified this as good practice. In other words, as a result of reflection on practice facilitated by RICA, practitioners committed to change things in their practice. For example, one change was to ensure that risk was consistently asked about in all families, and that when practitioners did ask, they utilised these question design types as good practice models of how to do so. Notably, these practice-based changes were not founded on analyst judgement of what constituted good or poorer communication, but instead, analysts described what happens in real-world settings and practitioners determined how and whether to apply the findings/knowledge.
Unmotivated looking as an iterative practice
Unmotivated looking is a foundational practice of CA (Sacks, 1984), which means that the analyst does not have a socio-political motivation or agenda for undertaking the research. While there is a recognition that there is likely to be some kind of motivation for generating the type of data set originally collected, the guiding premise of analysis is to allow whatever emerges from the data to be revealed. This means that the analyst does not know what will be found a priori. Consequently, the process is iterative as the research question develops, emerges and is, in some cases, collaboratively refined. In our data, for example, the original research question was very broad: ‘what happens in mental health assessments?’. Through unmotivated looking, it was noticed that there were large numbers of question-answer sequences. On closer inspection we saw that some of these question-answer sequences were focused around the topic of self-harm and suicidal ideation. This iterative process of refining the research question led to a close analysis of the extracts within the corpus that were related to this part of institutional business, and conversational practices and question design were identified. What we seek to clarify in making this a defining feature of RICA is that this way of conducting interventionist CA is positioned within the cluster of approaches of applied CA that are inductive and thus not necessarily problem-driven.
Implications and accessible language
An advantage of RICA is its commitment to enabling practitioners to make sense of the core messages and findings it produces. Given the specialist nature of CA training, relatively few practitioners have the opportunity to study the methodology themselves. Hence, the terminology and methodological processes involved in CA are typically not familiar to practitioner audiences. As a result, there is often a gap between the production of CA knowledge and its translation into practice. Although it is important that CA is conducted rigorously and robustly, our concern is that in doing so it does not become exclusive and only ‘readable’ to those relatively few trained academics. Therefore, one of the defining features of RICA is that when the implications of the findings are disseminated, it foregrounds a commitment to increasing inclusivity through accessible language.
Regarding dissemination, all academics have a range of options for suitable outlets for their work. In order to publish applied CA findings in journals designed to reach practitioner audiences, editors typically require certain kinds of revisions to the standard ways in which CA might be reported to facilitate readability. Some of these kinds of revisions may be to remove some details in Jeffersonian transcription and to include more pedagogical explanations about the meaning of certain CA terms. Thus, one of the priorities of RICA is to use language that is relevant to the given substantive field, assuring that the language is closely related to that of the practitioners. This involves, at times, working closely with practitioners, inviting them to review and critique how we are writing up findings. We provide an example of this below from our interrogation of question design (Kiyimba and O’Reilly, 2018):
Example seven: Family ten (From Kiyimba and O’Reilly, 2018: 150)
Our focus for this analysis was on question design, specifically those prefaced by ‘you said x’, and the article was published in a journal designed for practitioners in mental health ‘Child and Adolescent Mental Health’. As most readers of this journal would likely be unfamiliar with applied CA, it was important that the analytic narrative not only stayed faithful to the robust methodological procedures and concepts, but also that there was a pedagogical thread to explain the process and terminology in a way that was accessible. Thus, in our analysis we explained the sequence itself (the ‘you said x’ preface and reflected speech, response slot and question-answer adjacency pair), but we also provided clear explanations of the meaning so that the implications of the research were accessible to a practitioner audience. For example; “there are naturally occurring opportunities within the conversation for another person to speak, these are known as transition relevance places (TRP) (Sacks et al., 1974)” (Kiyimba and O’Reilly, 2018: 150). Thus, when utilising a common CA concept put forward by Sacks et al., 1974, and citing the appropriate reference, there was also an explanation of what that means. This is something that is not necessary for CA audiences, but when disseminating the implications of the research to practitioner audience, the pedagogy is more important.
Discussion
In introducing RICA, we outlined the defining features of one way of doing applied interventionist CA, providing a framework for application. RICA prioritises collaboration between academic knowledge production and reflective application in a variety of fields of practice. It is a way of doing interventionist CA that engages a reflective conversation between practitioners and academics with a goal of translating research knowledge into a field of practice. We have illustrated a framework for those interested in undertaking a RICA study by providing data examples from a mental health assessment study. First, looking at a larger corpus of data enables the possibility of identifying recurrent patterns and practices which can help practitioners to reflect on process, and for illustrative purposes we used data extracts that explored the practice of delivery of decision-making in autism. Second, data on self-harm were utilised to demonstrate an avoidance of the circularity that can be precipitated by having a predetermined problem focus, illustrating instead how this form of inductive inquiry can reveal unanticipated findings. Such unexpected findings can be valuable for highlighting areas of practice where practitioners may be less aware of ‘problems’ at play. Similarly, unexpected findings might highlight areas of good practice. This is helpful in terms of providing an opportunity for practitioner reflection. Third, we have demonstrated the importance when working at the interface between academic knowledge production with the identification of implications and application to practice of creating a shared vocabulary by explaining technical CA terminology.
From a purely pragmatic point of view, the adoption of RICA creates possibilities for practitioners to engage in reflective practice in a manner that it is rigorous and empirical, thereby countering some of the dominant outcome-focused discourses surrounding evidence-based practice (Taylor and White, 2000). What we have argued in presenting this collaborative approach to applied CA is that this methodology can be extremely valuable in informing practice. This is very timely as academics are now being required by funding bodies to provide a ‘pathway to impact’ to demonstrate the applied value of a given project. From a value-based perspective we feel that RICA is a highly appropriate and ethical way to do research. This is because there is an ethicality of ensuring that the cost to participants is balanced by the added value in terms of impact on practice, possibility for change, and quality improvement via dissemination of knowledge, which is greatly enhanced by a collaborative approach. Furthermore, from an ethical standpoint from the outset of the project, partnerships enable practitioners to make decisions and engage in dialogue in ways that facilitates the promotion of best interests for participants (i.e. decisions about service user involvement from a professional practitioner perspective). In addition, for the practitioners involved in research, it enables them to examine and reflect on their own and colleagues’ practice and develop ways of working that are consistent with best practice evidence. Ultimately this is beneficial for service users.
Researchers and indeed conversation analysts work in a different world to the one Sacks was working in and there are now various pressures fed through from editors, funding bodies, ethical governance, higher education institutions and so on. It can be challenging to find funds or meet the expectations of universities with theoretical thinking alone. In other words, we are working in a different research environment to Sacks in the 1970s, and one where there are greater expectations of ‘proving’ the impact of our work in areas of practice relevant to it, not least due to the rhetoric of evidence-based practice. Notwithstanding some of these greater debates that are important and should continue to be addressed, RICA is responsive to this new climate as it has an impact agenda and collaborates with practitioners to ensure relevance, while staying faithful to the scientific procedures of the approach.
Footnotes
Acknowledgements
We are very grateful to both academics and practitioners who commented on earlier drafts of this paper. Specifically, we thank Alison Drewett (Lecturer in Speech and Language Therapy, De Montfort University); Alexa Hepburn (Professor of Communication, Rutgers University); and Ian Hutchby (Honorary Professor of Sociology, University of York). We are also grateful to the families and clinicians who participated in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The initial scoping work for the project on mental health assessments was funded by the ‘Heart of England Hub’.