
Abstract
There is a global need, including in South Africa, to understand cricket-related injuries among female players better. Hence, this study investigated the relationships between anthropometric characteristics, physical fitness, kinetic factors, and in-season injury occurrence. An observational longitudinal cohort design was employed, involving 31 adult elite female cricketers from four South African franchises. Pre-season assessments included a baseline questionnaire and a standardised testing protocol. These measures were subsequently correlated with injury incidence, which was monitored weekly throughout the competitive season from October 2024 to March 2025. The in-season injury incidence was 41.90%. Multivariable modified Poisson linear regression analysis suggested that injuries were associated with higher medicine ball power throw test values, whereas shorter broad jump distances and slower 20 m sprint time are independently associated with lower injury risk. These findings suggest a performance–injury trade-off, where higher physical outputs may increase mechanical loading and injury susceptibility in the absence of appropriate load management, recovery strategies, and neuromuscular control. Accordingly, these variables should be used for athlete monitoring and profiling rather than for selection or deselection purposes. While this study has limitations, the findings contribute to the development of pre-season screening approaches that consider the balance between performance and injury risk. Further research is required to confirm these relationships and inform evidence-based injury prevention strategies.
Keywords
Introduction
Cricket is a highly popular sport played globally by both males and females at the professional level.1,2 Cricketing injuries hinder players’ progression and development,3–5 despite potentially being controllable. 6 Existing research in this domain mainly focuses on male cricketers,7,8 often applying findings to females despite differences in bodily make-up, physiology, and function. Research on injuries in female cricketers is limited. 3 Scientific evidence on risk factors can inform evidence-based injury prevention protocols, contributing to player safety and strengthening the integrity of the game.3–5
Existing research on female cricketers has identified several injury risk factors. Fast bowling shoulder injuries in female cricketers have been associated with a limited internal rotation (IR) range of motion (ROM) in the bowling shoulder, 9 as well as a higher IR-to-external rotation (ER) strength ratio measured with a dynamometer, which are identified as key risk factors. 9 Additionally, weaker hip abduction strength and imbalanced hip adduction-to-abduction strength ratios are significantly linked to shoulder injuries among female fast bowlers. 9 Kinematically, a larger thoracic lateral flexion angle relative to the pelvis during the delivery stride also correlates with female fast bowlers who have a history of lower back pain. 10 Moreover, reduced broad jump (BJ) measure (horizontal lower-body power) and 20 m sprint outcome are likely indicator of injury risk. 11
The paucity of scientific evidence8,12,13 highlights the need to investigate injury incidence and risk factors more comprehensively. 14 Accordingly, this study aimed to determine the injury incidence among female South African cricketers and examine the anthropometric, physical fitness, and kinetic factors associated with injuries, expanding the evidence within the South African context.
Modifiable injury risk factors in sport are commonly assessed through anthropometric, kinematic, kinetic, and physical fitness measures. Anthropometric characteristics, such as body composition, may influence load distribution and injury susceptibility, yet these have not been widely investigated in female cricket. 15 Kinematic and kinetic variables, including landing mechanics, deceleration forces, and vertical ground reaction forces, are recognised determinants of injury risk in female athletes.14,16 Additionally, deficits in muscular strength, flexibility, power, speed, and balance have been associated with increased injury risk.17,18 However, these relationships have not been well established in female cricketers.
Due to limited research in this population, specific injury risk factors for female cricketers remain unclear. 19 In contrast, studies in male cricketers have identified risk factors such as fast-bowling techniques, higher workloads, previous injury, and reduced hip IR.20–22 This highlights a gap in the literature regarding female players. Therefore, investigating these modifiable factors may assist in developing screening protocols to better identify injury risk in female cricketers, which this study aims to address.
Materials and methods
Study design and participants
This was an observational, longitudinal, prospective cohort study conducted according to the STROBE guidelines for observational cohort studies. 23
In-season musculoskeletal injury surveillance was conducted weekly over a six-month period during the 2024/2025 cricket season at four participating franchises. Uninjured elite 24 adult female cricket players, regardless of their role on the team, from university first teams (collegiate), domestic franchises, or national team, aged 18–40 years, were targeted as potential participants. At the onset, a convenience sample of 47 eligible cricketers was selected based on player access and geographical proximity.
Ethical clearance, permissions and consent
Ethical clearance was granted by the tertiary institution's Human Research Ethics Committee (Ref. 367/2024), where the research was conducted. National and provincial governing bodies approved access to contracted players and domestic franchises, and team gatekeepers also granted permission. Each participant received an information sheet and provided written informed consent.
Study pre-season procedures
The study was conducted in two phases: pre-season and in-season.
Participants completed a pre-season questionnaire regarding age, ethnicity, player role (batter, bowler, wicketkeeper, or all-rounder), level of play (collegiate, domestic franchise, or national team), playing experience (years of play and years of national play), current injury status (injured or uninjured), and previous injuries to anatomical regions. The face and content validity of the questionnaire have been previously confirmed, and it has been used in multiple studies25,26 examining injury risk factors in the South African population.
Supplementary Table 1 details the pre-season screening anthropometric, physical fitness, and kinetic tests performed by the same trained researchers and research assistants during the testing session. The test battery was based on an evidence-based screening protocol from previous studies27,28 with additional reliable tests (Supplementary Table 1). Testing commenced with the three anthropometric measures, followed by ROM, kinetic strength and power, and additional lower-body and upper-body power tests that were not kinetically analysed. Finally, all speed and change-of-direction tests were completed. Measurements were recorded on a study-specific data sheet, and each team's screenings happened on different days based on availability.
The medical personnel of the respective cricket teams assisted with weekly injury surveillance from 1 October 2024 to 31 March 2025, using an injury surveillance questionnaire.25,26 An injury was defined according to a 2016 consensus statement 29 as; any musculoskeletal issue resulting from activity on the cricket field during training or matches, excluding concussions and illnesses,29,30 regardless of mechanism. The anatomical regions were recorded. The face and content validity of the questionnaire have been previously confirmed and utilised in multiple similar studies in South Africa.25,26 In many cases, medical professionals preferred to capture players’ injury data in their existing injury surveillance systems and provided the relevant data to the researchers.
Statistical analysis
IBM SPSS Statistics (version 29.0; IBM Corp., Armonk, NY, USA) was used for statistical analysis. Players were classified as injured or uninjured according to the definition stated previously, with no subgroup analysis due to the limited sample size. All variables were analysed and represented in the Tables in the results section and supplementary materials. The skewness of continuous variable distributions was tested using the Kolmogorov-Smirnov test (KST) 31 and related histograms. 32 Inferential statistical analyses were used to compare the absolute pre-season anthropometric, ROM, strength, power, speed, and change of direction variables between the injured and uninjured groups using the independent-samples t-test for parametric data and the Mann-Whitney U (MWU) test for non-parametric data. 33 Statistical significance was set at P < 0.05. The mean difference (MD) quantified the direction and magnitude of the differences between the injured and uninjured groups of parametric data.
A modified Poisson regression analysis with robust standard errors was used to assess the correlation between pre-season anthropometric, physical fitness, and kinetic predictors and in-season injuries. Variables with a P-value < 0.200 obtained from the univariate part of this analysis were considered for multivariate analysis to avoid missing potential predictors that may become significant after adjusting for confounders. 34 Variables that retained statistical significance (P < 0.05) 34 were considered as potential risk factors. The dynamic decisions made during the regression analysis are explained in the results section. Goodness-of-fit statistics complemented the analysis.
Relative risks (RR) and 95% confidence intervals (CIs) were reported to quantify the magnitude and direction of the associations. The occurrence of injury (uninjured=0; injured=1) was used as the outcome measure. Robust standard errors were adjusted for small sample sizes. Risk ratios were used to describe the association between anthropometric, physical fitness, and kinetic variables and injury.
Results
Participant information
Complete in-season injury datasets were received for 31 (66%) of the 47 cricketers who were approached to participate. The group comprised players with multiple overlapping roles; however, their predominant identities were reported as 6 specialist batters (19%), 12 all-rounders (39%), 7 pace bowlers (22%), 3 spin bowlers (10%), and 3 wicketkeepers (10%). A post hoc power analysis conducted using G*Power 3.1 indicated that, with a sample size of 31 participants, the study achieved approximately 52.6% power to detect a medium effect size (r = 0.3) at an alpha level of 0.05.
Most participants (28 of 31, 90%) were national-level players, with nine (29%) having played at this level for six years or more, 10 (32%) for four to six years, six (19%) for one to three years, and three (10%) for one year or less. The remaining three participants (10%) participated at the collegiate level. All player roles were included: batters (100%), bowlers (87%), wicketkeepers (10%), and all-rounders (50%). The bowlers were identified as 40% fast bowlers, 20% seam bowlers, 32% spin bowlers and 8% swing bowlers. Their mean age was 21.90 ± 4.30 years. The sample included a high proportion of national-level players, with multiple overlapping roles (e.g., all-rounders), limiting the ability to meaningfully stratify injury occurrence by role.
In-Season and previous injuries
The total number of participants who sustained in-season injuries was 13 (42%), of which eight were non-contact injuries, five were overuse injuries and five acute contact injuries, whereas 18 (59%) participants remained uninjured throughout the season. In the same sample, 17 (55%) participants reported prior injuries, throughout their lifetime. Of the 13 participants with in-season injuries, four sustained multiple injuries, and eight (62%) had a history of previous injury, whereas five (39%) did not have prior injuries but sustained injuries during the season. Five players sustained reinjuries at previously injured sites.
Figure 1 depicts the injuries by anatomical site for both the previous injuries and those incurred during the 2024–2025 season.

Injuries per anatomical site of 17 previous and 13 in-season injuries. Picture generated with Copilot TM.
Modified poisson linear regression analysis
Table 1 presents the results of the modified Poisson linear regression analysis (with robust standard errors) comparing the relationships between pre-season anthropometric, kinetic, and physical fitness predictors and in-season injury occurrence.
Univariate modified Poisson regression comparison between pre-season anthropometric, kinetic, and physical fitness predictors and in-season injuries (P-value <0.200).
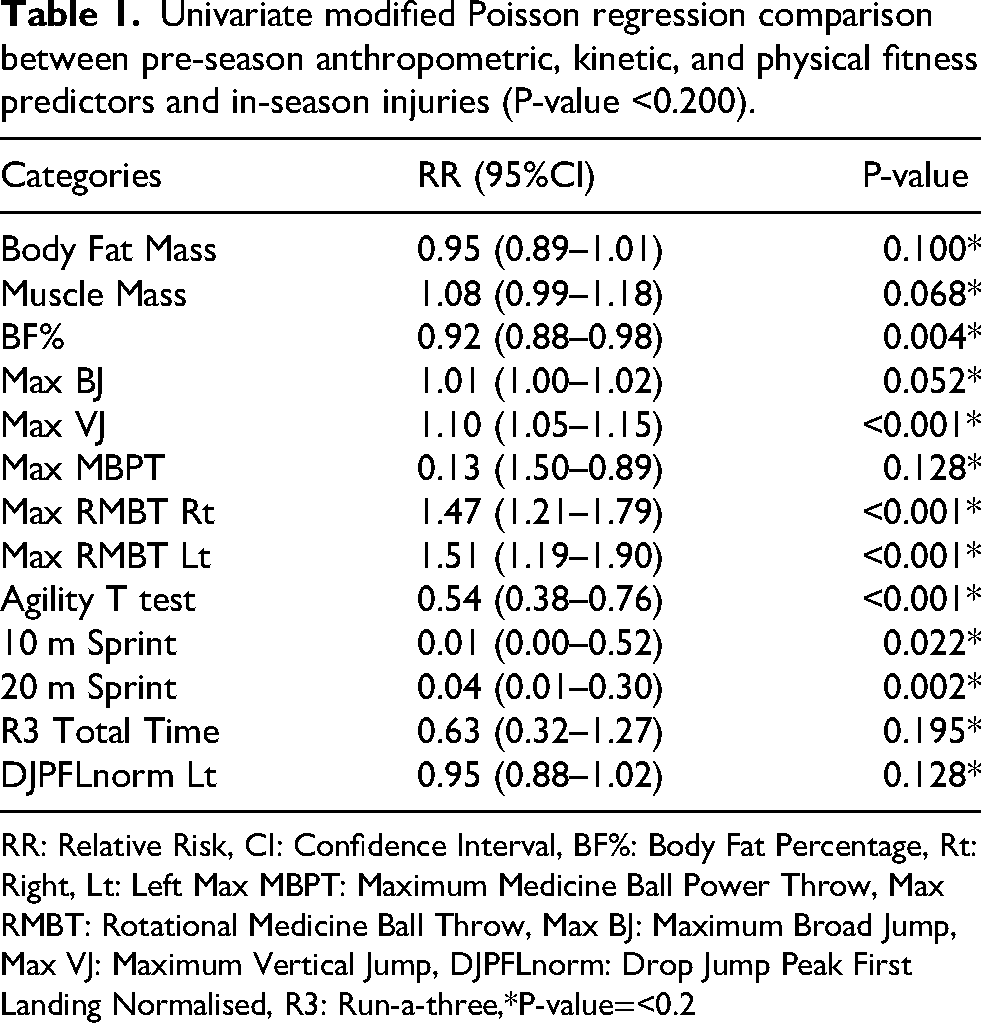
RR: Relative Risk, CI: Confidence Interval, BF%: Body Fat Percentage, Rt: Right, Lt: Left Max MBPT: Maximum Medicine Ball Power Throw, Max RMBT: Rotational Medicine Ball Throw, Max BJ: Maximum Broad Jump, Max VJ: Maximum Vertical Jump, DJPFLnorm: Drop Jump Peak First Landing Normalised, R3: Run-a-three,*P-value=<0.2
Variables with RR < 1.00 had a protective effect, whereas those with RR > 1.00 were risk-increasing. Although the variables with P < 0.200 met the multivariate regression qualification criteria, the univariate regression model was considered significant at P < 0.05. The following variables were identified as having a significant (P < 0.05) protective effect: 1) BF% (RR = 0.92, 95% CI [0.88–0.98], P = 0.004) with each unit increase lowering injury risk by approximately 7.7%; 2) Agility T-test (RR = 0.54, 95% CI [0.38–0.76], P = <0.001) with each unit increase lowering injury risk by approximately 46%; and 3) the 20 m Sprint (RR = 0.04, 95% CI [0.01–0.30], P = 0.002) with each unit increase lowering injury risk by 96%.
The risk-increasing factors with significance were 1) Max VJ (RR = 1.10, 95% CI [1.05–1.15], P < 0.001) each unit increase raises the risk by 10%, 2) RMBT Rt, and max RMBT Lt (RR = 1.47, 95% CI [1.21–1.79], P = < 0.001) indicating each unit increase causes 47% increase in injury risk, and (RR = 1.51, 95% CI [1.19, 1.90], P = < 0.001) indicating a 51% increase in injury risk per unit increase, respectively.
Multivariate poisson regression
Table 2 contains the multivariate modified Poisson regression results, including variables with P < 0.200. 34
Multivariate modified Poisson regression with robust standard errors for anthropometrical, physical, and kinetic injury risk factors.
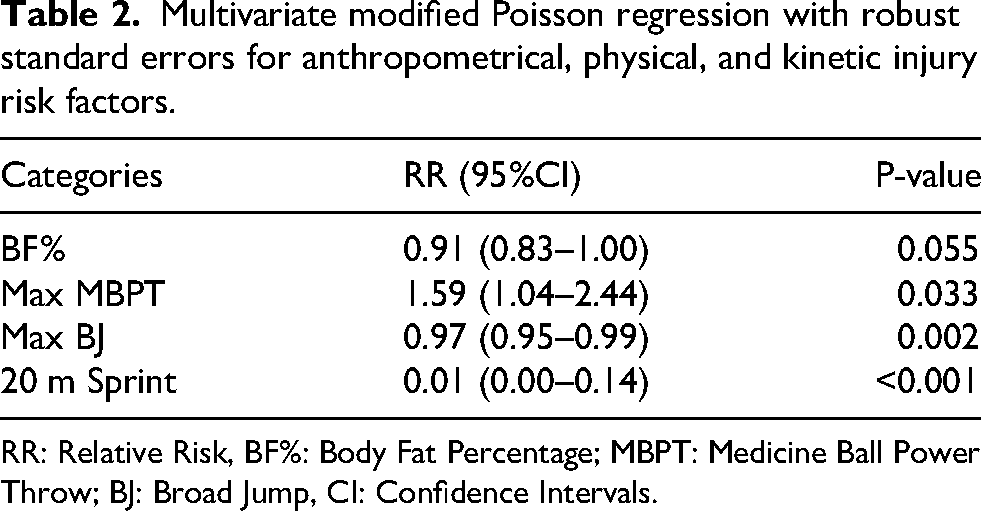
RR: Relative Risk, BF%: Body Fat Percentage; MBPT: Medicine Ball Power Throw; BJ: Broad Jump, CI: Confidence Intervals.
The following variables were selected for the multivariate modified Poisson regression analysis: Medicine ball power throw (MBPT) and BF%, as they are measures used in female and overhead ball sports to indicate injury risk.35,36 A 20 m sprint was included, as it is a frequently used risk indicator for male cricketers.30,37 The maximum BJ was previously associated with injury risk in female cricketers.38,39 Other factors were not included in the model due to intervariable correlation.
The findings showed that max MBPT was significantly associated with a higher injury risk, with each unit increase raising the risk by 59.20%. Conversely, max BJ and the 20 m sprint demonstrated protective effects, with relative risks of 0.97 (P = 0.002) and 0.01 (P = < 0.001), respectively, indicating reductions in injury risk of 3% per unit increase and >90% per unit increase, respectively.
Goodness-of-fit statistics showed that the deviance and Pearson chi-squared, divided by their degrees of freedom, were 0.618 and 0.576, respectively, well below 1, indicating a good fit and no overdispersion. The omnibus test (likelihood ratio chi-squared, df = 7.23, P = 0.124) suggests that the whole model does not significantly improve the fit over the intercept-only model. However, individual predictors were notably associated with injury prevalence.
Anthropometric measurements
Supplementary Table 2 outlines the anthropometric measurements of all participants. The KST significance values were used to evaluate the normality of each independent variable. For non-parametric data, only the median and inter-quartile ranges (IQR) are reported, rather than the mean and standard deviation (SD).
There was a statistically significant difference in the sit height (P = 0.039) and BF% (MD = −5.46; P = 0.019) between injured and non-injured players, with injured players having a higher sit height and BF%. Uninjured participants had a 6 cm lower sit height, and injured participants had a 5.46% lower BF%.
Physical fitness and kinetic measurements
The differences in ROM, power, speed, and agility between injured and uninjured participants are presented in Supplementary Table 3. The differences in kinetic dynamometer measurements across the injury status groups and the differences in single-leg drop-jump (DJ) force plate measurements between injured and uninjured participants are also provided in Supplementary Table 3.
There was a statistically significant difference in max vertical jump (VJ) (P = 0.003), Rotational medicine ball throw (RMBT) right (Rt) (MD = 1.74; P = 0.001) and RMBT left (Lt) (MD = 1.69; P = 0.001) between injured and uninjured players. The injured group, on average, showed 6 cm (17%) higher VJ height and threw 1.74 m (27%) to 1.69 m (26%) farther than the uninjured group. The agility T-test also revealed a significant difference (P = 0.023), with uninjured participants being, on average, 0.88 s slower than their injured counterparts. Similarly, uninjured participants took approximately 0.18 s longer to complete the 20 m sprint than injured participants (MD = −0.18; P = 0.007). For the 30 m sprint, the median times indicated that uninjured participants were slower than their injured counterparts.
Dynamometer tests showed no kinetic differences between the injured and uninjured participants. During single-leg DJ force plate analysis, injured participants displayed a 5 s longer contact time (Lt) than uninjured participants. (P = 0.021).
Discussion
This study is the first to link injuries in South African female cricketers with anthropometric, fitness, and kinetic indicators, focusing on the 2024–2025 season injuries, some with multiple occurrences. Key findings show that in-season injuries correlated with MBPT, BJ, and 20 m sprint times, which are plyometric/explosive tests, indicating that these factors may predict injury risk.
In this study, the in-season injury incidence rate was 42% in a single season, with five players experiencing more than one injury, and no players experienced repetitive injury to the same body part. Also, the level of play did not differ significantly between national-level and collegiate-level players (P = 0.121). However, higher-performing players may have increased exposure (training and match load), which could partially explain the association between superior physical performance and injury risk. The injury rate was 62% among the eight fast bowlers represented in this sample. No other study has compared this specific incidence rate for the same period in percentage terms, making direct comparison difficult. However, the injury incidence among cricketers is notably high, affecting nearly half the players. An Australian study that followed 121 female cricketers observed that 78% of players reported one or more injuries over a two-year period. 40 Other studies reported incidence per playing hours or per match. A previous study, for example, found a match injury incidence of 169.4 injuries per 10 000 h across two cricket seasons for Indian and English female cricketers (n = 30). 41
The most common injuries in this study (Figure 1) were to the knees (n = 4; 23%), wrists (n = 3; 17%), fingers (n = 2; 12%), shoulders (n = 2; 12%), lower leg (n = 2; 12%), and ankle (n = 2; 12%). Again, not all studies reported injury incidence by body region in a standardised way, making direct comparisons challenging. In a similar study 42 the incidence rates per body region was as follows: ankle (9%); elbow (3%); head and neck (5%); hip/groin (7%); knee (14%); lower back (3%); lower leg (13%), shoulder (9%); thigh (7%); and wrist/hand (17%). 42 Female players from India mainly experienced knee (33%), wrist/hand (33%) injuries, 41 while those from England (n = 18) primarily suffered from wrist, hand (19%), thigh (14%), shoulder (13%), and lumbar spine injuries (12%). 41 It therefore seems that, among female cricketers from South Africa, Australia, England, and India, the knee, wrist and hand areas are consistently identified as high-risk anatomical sites. 41
Previous injury has been suggested to be a strong predictor of injury risk. 38 In this study, 62% of the injured group had a history of prior injury, predominantly in the hip/buttock/groin (18%), shoulder (15%), ankle (15%), and knee (11%) regions. More studies reported previous injury rates of approximately 50%,38,41,43 and a 2017 systematic review concluded that previous lower limb injuries are associated with recurrence, but not necessarily to the same injury site. 44 Susceptibility to shoulder reinjury is influenced by prior shoulder injury, especially in overhead athletes. 45
This study found, in the adjusted Multivariate Poisson regression with robust standard errors model, that increased MBPT was independently associated (P < 0.05) with an increase in in-season injury risk. Furthermore, the BJ distance and 20 m sprint scores had a protective effect, reinforcing that reduced neuromuscular control of the lower limb significantly increases injury risk,2,19,39,46 especially in cricket movements like rotational actions, jumping, and sprinting. This is critical, given that lower limb injuries are more common among females.38,39 Similarly, inadequate explosive power and sprint-specific training movements in male cricketers have been associated with a higher risk of soft tissue strains. 47 This collectively indicates that explosive performance tests are critical indicators of injury risk across all cricket populations.
A prior review examined physical fitness, including MBPT, and injuries in female team ball sport athletes; MBPT was not linked to injury risk. 35 Our study appears to be the first to report such a finding. MBPT is a commonly used upper-body power test. 35 Upper-body power is crucial for cricketers’ bowling and throwing. 39 Greater upper-body power movements, like fast bowling, generate more force, requiring stabilisers to work harder and causing fatigue in endurance games like cricket. Upper-body power executed with muscle imbalances 48 and neuromuscular control deficiency2,49 is associated with overuse injuries2,38,48,49 and affects the shoulder and lumbar spine. 38
This study found longer BJ distances and 20 m sprint time are independently associated with lower injury risk, supported by another study linking BJ and 20 m sprint to lower-body injuries in females cricketers. 11 Another study 11 associated shorter BJ distances with an over 10% risk of non-contact lower-limb injury among female volleyball players. 35 Cricket movements like running, jumping, and fast bowling demand explosive power, causing excessive lower limb loading joints. 38 Horizontal force generated when performing a BJ 14 influences cricket-specific movements such as sprinting (acceleration phase), landing, diving when fieliding, 50 and a change-of-direction between wickets. 51 It should be considered that extrinsic factors could influence ground reaction forces (GRF), i.e., centre of mass (COM) which alters both the direction and magnitude of GRF dynamics. 52 Increased GRF during landings happen when eccentric control falters, 14 possibly due to physiological issues like neuromuscular deficits, gluteal weakness, and core instability, 14 which may indicate injury risk. 35 Individuals with a higher COM have been shown to have reduced eccentric control, 52 which may place taller individuals at a higher risk of injury.
The study found faster 20 m sprinting cricketers were independently more injury-prone (Table 2), possibly due to increased effort. The 20 m and 30 m sprints measure linear speed used in training and matches. Without proper recovery, excessive load may cause musculoskeletal vulnerability,53,54 as previously shown in female football players. 54
The study suggests lower BF% may have a moderating effect (P = 0.055) to increase musculoskeletal vulnerability in female cricketers. 55 The average BF% for the injured category players were 25%, categorised at the low end of average/healthy BF% (25–31%), 56 while the uninjured group average BF% were 30%, considered to be overweight. 56 Low BF% may lead to insufficient energy 55 and hormonal imbalances,57,58 impairing bone density, soft tissue repair and tendon integrity.57,58 Previous studies show female cricketers are more prone to overuse injuries, 38 more common in females in general. 49 Reduced tissue resilience and slower soft-tissue recovery indeed increase the likelihood of overuse injuries. 49
Several other variables differed between the injured and uninjured groups but could not be isolated as independent risk factors in the regression analysis due to the small sample size. However, it is essential to evaluate these associations.
In this study, uninjured players had notably lower sit heights than injured players, possibly due to biomechanical factors or confounding factors, but it could also be explained by biomechanics. A taller trunk height reduces trunk stability because of a higher centre of mass,59,60 reducing neuromuscular control during dynamic tasks, such as increased trunk flexion during landing or stepping mechanics. 61 Inadequate trunk control leads to compensatory movements 61 and muscle imbalances 60 that impair force transfer between the upper and lower body, consequently increasing stress on the knee joint.60,61 Specifically, trunk instability in the transverse and frontal planes increases rotational instability and knee valgus, risk factors for patellofemoral pain and anterior cruciate ligament injuries. 61 Further investigation is necessary to understand trunk height mechanics, as it was a confounder.
Injured players also had higher VJ heights, possibly due to confounders. VJ height links to increased GRF during landing,62,63 which is associated with higher lower limb injury risk injuries.62,63 Furthermore, a previous meta-analysis found higher vertical GRF as a consistent predictor of running injuries, 64 though this study mainly focused on runners, 64 The underlying biomechanical principles apply to cricket-related movements. Prior research showed that uninjured male and female athletes in non-contact sports demonstrated superior VJ performance. 65
Injured participants unexpectedly threw a medicine ball farther bilaterally, despite stronger power movements like greater trunk rotational force typically leading to better performance conditioning,66,67 higher load tolerance, and lower injury risk. 66 Throwing and swinging mechanics rely on sequential force transfer from proximal to distal segments,67,68 which is a key principle in rotational power sports. Compensatory strategies or poor thoracic mobility can affect trunk and hip rotational stability, 68 possibly leading to an increased risk of injury. Female cricket tournaments mainly feature T20 and ODI matches, requiring aggressive batting, strong counterattacking fielding and bowling, and significant trunk and hip rotation for impactful batting, bowling, and fielding performance. 66 Confounders may have affected these results, and further research is recommended to clarify how rotational power, thoracic mobility, and workload interact to influence the injury risk.
The current injured group showed significantly higher performance in the agility T-test and 20 m and 30 m sprints, but higher scores also correlated with better performance. 54 Higher speeds not only contribute to match-winning actions, 69 but also increase mechanical loading, amplifying susceptibility to lower-body injuries.64,70 The 20 m sprint has been independently associated with increased injury risk. As previously explained, running injury risk increases with higher vertical GRF,64,70 and neuromuscular stress 53 and output also increase. 71 Change-of-direction is explicitly associated with injury risk due to rapid deceleration and asymmetric loading of the lower limbs during the action. 71 This study did not examine running biomechanics at higher speeds. Future research should include biomechanical assessments during screening, not just speed.
In the current study, single-leg DJCT Lt was the only kinetic variable that differed significantly between the injured and uninjured groups. The delayed contact time suggests that the injured group could not attenuate the impact on the left leg (most players’ non-dominant side), consistent with the BJ findings, which may indicate that inadequate eccentric-landing control causes higher impact forces. However, this was considered a confounding factor in the regression analysis.
Conclusion
The findings of this study should be interpreted as preliminary associations within a performance–injury context rather than as prescriptive screening criteria. MBPT, BJ, and 20 m sprint were associated with injury and should inform prevention strategies, particularly within screening protocols and monitoring frameworks for female cricketers. Importantly, these findings reflect a performance–injury trade-off, whereby higher physical outputs, such as faster sprint speeds and greater trunk rotational power, which may increase mechanical loading and injury susceptibility in the absence of appropriate load management, recovery strategies, and neuromuscular control. As such, these variables should be used for athlete profiling and monitoring rather than for selection or deselection decisions. The role of body fat percentage remains unclear and warrants further investigation.
Limitations
The study's inferences should consider these limitations. The level of play was excluded from the final analysis due to the small subset of non-national players, however not identified as a confounding variable. Furthermore, the absence of workload, exposure, and role-specific analyses limits causal interpretation and may have introduced residual confounding.
The inclusion of heterogeneous injury types may dilute the strength of associations between physical performance variables and injury risk. Future research should distinguish between injury mechanisms (e.g., contact vs non-contact, overuse vs acute) to better align screening measures with injury-specific risk profiles.
The data quality was sufficient, with most variables being parametric and only a few requiring nonparametric methods. This study, with 31 female cricketers, was smaller than other samples (17–115) and likely had limited power, yielding non-significant results despite individual predictor effects. Including multiple predictors reduced the degrees of freedom, possibly affecting the estimated stability. As such, the findings should be interpreted with caution, as the study may be underpowered to detect smaller effects. Consequently, the results are best considered exploratory and hypothesis-generating rather than confirmatory. These limitations have been acknowledged within the study, and further research with larger sample sizes is required to validate and expand upon these findings.
Missing data from unidentified questionnaires and staff turnover hindered follow-ups, risking bias as cricketers may withhold personal information. Method differences from other studies complicate comparisons. Future research should address this for accurate results.
Absolute values were used for strength and fitness measures in this study; however, introduced mathematical coupling and potential collinearity with the anthropometric variables were included in the model, potentially obscuring true associations and complicating the interpretation of regression coefficients. Future researchers should consider that normalisation to body mass or fat-free mass may yield additional insights.
Due to overlapping roles (e.g., all-rounders) and small subgroup sizes, role-specific comparisons were not statistically feasible. Future research involving larger samples should categorise participants by playing position and competition level to more accurately identify role-specific physical traits and their connection to injury risk. Also, future work should aim to align physical performance with more specific injury risk profiles for overuse, acute contact, and non-contact injuries as this study did not differentiate between these mechanisms of injury. Therefore, the current findings should be viewed with caution and regarded as preliminary rather than definitive.
Future work should focus on distinguishing between contact and non-contact injuries, as well as between acute and overuse cases, to better align physical performance measures with specific injury risk profiles. The number of training and match days was not collected for this study because workload was not considered, which may have affected the results and certain player roles. Therefore, future studies should incorporate exposure-based metrics (e.g., match hours, workload) and role stratification to better isolate injury risk profiles.
Supplemental Material
sj-pdf-1-spo-10.1177_17479541261451713 - Supplemental material for Identification of physical attributes and injury risk in South African female cricketers
Supplemental material, sj-pdf-1-spo-10.1177_17479541261451713 for Identification of physical attributes and injury risk in South African female cricketers by Tania Postma, Nivash Rugbeer, Licinda Pienaar and Candice MacMillan in International Journal of Sports Science & Coaching
Supplemental Material
sj-pdf-2-spo-10.1177_17479541261451713 - Supplemental material for Identification of physical attributes and injury risk in South African female cricketers
Supplemental material, sj-pdf-2-spo-10.1177_17479541261451713 for Identification of physical attributes and injury risk in South African female cricketers by Tania Postma, Nivash Rugbeer, Licinda Pienaar and Candice MacMillan in International Journal of Sports Science & Coaching
Supplemental Material
sj-pdf-3-spo-10.1177_17479541261451713 - Supplemental material for Identification of physical attributes and injury risk in South African female cricketers
Supplemental material, sj-pdf-3-spo-10.1177_17479541261451713 for Identification of physical attributes and injury risk in South African female cricketers by Tania Postma, Nivash Rugbeer, Licinda Pienaar and Candice MacMillan in International Journal of Sports Science & Coaching
Footnotes
Ethical considerations
Ethical clearance was granted by the University of Pretoria's Human Research Ethics Committee (Ref. 367/2024), where the research was conducted.
Consent to participate
All participants received an information sheet and provided written informed consent to participate in the study.
Consent for publication
Not Applicable.
Author contributions
Tania Postma and Candice MacMillan were involved in the conceptualisation and made substantial contributions to the design of the manuscript; Tania Postma and Nivash Rugbeer have contributed to the acquisition, analysis, and interpretation of the data. All authors have participated in drafting the manuscript: Tania Postma, Candice MacMillan, Nivash Rugbeer, and Licinda Pienaar revised it critically. All authors have read and approved the final version of the manuscript.
Funding
Funding from the National Research Foundation (Grant number: SRUG2204041765) has been received.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
No additional data is available as all is presented in the manuscript and supplementary tables.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.