
Abstract
Basketball is the second most participated sport in England. However, little is known about the injury profile of players or the knowledge, perceptions and behaviour of basketball players and coaches towards injury risk and prevention. A cross-sectional survey was administered to coaches and players at the end of the season (2022–2023, 2023–24). Participants were required to have played/coached in England during the season and be 16 years of age or older. A 7-item Likert scale was used to assess knowledge and perceptions of injury risk and prevention. Questions around previous injuries and behaviour were answered using multiple-choice answers. Data are presented descriptively, with a Wilcoxon-Mann-Whitney and 2 × 2 χ 2 tests used to compare results between groups (p < 0.05). In total, 185 participants (152 players, 33 coaches) were included in the study. 97% of players reported having sustained a time-loss basketball injury in their career, with 66% of players sustaining an injury in the present season (16% requiring hospital attention) and 23% sustaining a concussion playing basketball. Players and coaches held positive perceptions towards injury prevention, although significant differences existed on the most effective methods to reduce injury, with coaches favouring strength training and load management (p < 0.01). Both groups had good knowledge of injury risk, although there were differences in the frequency and seriousness of some injuries, such as concussion. Half of the players reported using protective equipment, with only 6% using a mouthguard. Basketball injuries appear frequent and serious, but players and coaches alike possess positive knowledge and perceptions towards their prevention.
Introduction
Basketball is a fast-paced, multi-directional team sport, requiring high-intensity actions such as accelerations, decelerations, change of direction, repetitive jumping and landing efforts. 1 As with all sports, there is a risk of injury associated with playing, which appears to vary depending on gender,2,3 playing level 3 and possibly geographical location due to rule variations. The repetitive nature of the sport is associated with the high prevalence of overuse conditions, such as tendinopathies, 4 whilst numerous injuries are sustained through legal contact facets of the game. 5 As such, the mechanism and type of injuries sustained in basketball is varied, which makes injury prevention challenging for players, staff, and researchers alike.
In England, basketball is one of the most participated sports amongst adolescents and adults, with over 1 million people playing weekly. 6 Despite this, there is a paucity of evidence around the risk of injury in English basketball. The only available evidence is from a longitudinal cohort study conducted at a single college in England (under-17 to 19), which reported a match time-loss incidence of 12 injuries per 1000 athlete-exposure (p/1000AE) and a training incidence of 2.4/1000AE 7 . Furthermore, the severity of injuries sustained was also high, with the mean game and training severity being 18 days and 28 days, respectively. Literature consistently reports that game injury incidence is significantly higher than training injury incidence, although training injuries are more prevalent.8,9 In the limited literature describing injury risk in English basketball, game incidence appears notably higher than studies in similar populations in North American cohorts, where time-loss incidence ranged from 2.4–3.0/1000AE.10,11 Reasons for this are unknown but highlight the need for injury surveillance projects in English basketball cohorts, rather than reliance on injury data from other countries.
No studies have investigated the preventative behaviours of English basketball players and coaches, or their perceptions towards injury prevention strategies, which may influence one's behaviour. 12 There are numerous effective strategies to reduce basketball injury risk. A meta-analysis concluded that implementing a basketball-specific injury prevention warm-up can reduce lower-limb injuries by 31% and ankle injuries by 55%, 13 whilst the use of prophylactic bracing or taping has been found to reduce the risk of ankle injuries significantly. 14 However, for many preventative strategies to be effective, they need to be adopted and adhered to. Unfortunately, such interventions, especially neuromuscular training programmes, are often blighted by poor implementation, with only 12% of Irish basketball players using an injury prevention programme, 15 whilst poor adoption rates have also been reported in a Swiss cohort. 16
The primary aim of this study was to describe the knowledge, perceptions and behaviour of basketball coaches and players, male and female, in England towards injury risk and prevention. The study also sought to provide descriptive information about self-reported player injury history given the sparseness of literature in this cohort.
Methods
Participants and recruitment
A database of clubs nationwide was developed manually, with email addresses found for individuals to circulate the survey links within their clubs. Similarly, a list of schools and colleges participating in the Elite Academy Basketball League (under-19 league; Men's and Women's) and College Basketball League (Men's) was created with email addresses found to contact individuals at these institutions. There was also a social media campaign, with support from Basketball England, to publicise the study and aid recruitment of both players and coaches. Players were targeted through their clubs, schools, and coaches, who provided links to players to complete the survey, with no players directly contacted by the research team. Inclusion criteria for the study were any male or female, currently coaching, training and/or playing basketball for a club/institute within England at any level. Participants must have been 16 years or older on the 1st of September (start of the academic year for those in education).
Survey
A cross-sectional survey was employed to investigate basketball players’ injury history (throughout their career and within season), perceptions towards injury prevention strategies and their preventative behaviours (appendix 1). A similar survey was conducted for basketball coaches to investigate their use of preventative behaviours and the level of medical provision within their basketball teams. Bespoke surveys were created using questions from similar studies conducted in basketball17,18 and rugby union. 19 Aside from demographic questions, all survey questions were multiple choice, with many using a 7-item Likert scale to avoid central tendency bias. 20 Both surveys were conducted electronically using Online Surveys (https://www.onlinesurveys.ac.uk/), with all questions set as mandatory to ensure no missing data.
Surveys were distributed between March (end of regular season) and May (end of play-offs) at the end of the 2023 and 2024 seasons to allow players to respond with injuries and behaviours from the season which has just ended. Participants were only allowed to complete each survey once, so if a player completed it for both seasons, responses from their second season were removed prior to analysis.
No sample size calculation was performed due to conducting a nationwide study and recruiting as many participants as possible to aid the generalisability of the results across different settings of the game in England.
Ethical approval
All participants were required to read a participation information sheet and sign a consent form prior to completing the electronic survey. Participation was voluntary, with data anonymised prior to analysis. Ethical approval was gained from the Research Ethics Committee at the University of Gloucestershire, UK (REC Number 23.77.2).
Analysis
Demographic data was analysed descriptively (mean, SD). Ordinal Likert scale responses were analysed using median, mean, inter-quartile ranges, percentages (%) and 95% confidence intervals (95% CI). For Likert scale questions asked to players and coaches, differences in scores were assessed using non-parametric Wilcoxon-Mann-Whitney tests. A 2 × 2 χ2 test was used to compare differences between coach and player responses for dichotomous questions. P-values were adjusted using a Bonferroni correction (45 statistical tests) with statistical significance set at p < 0.05.
Results
Demographics
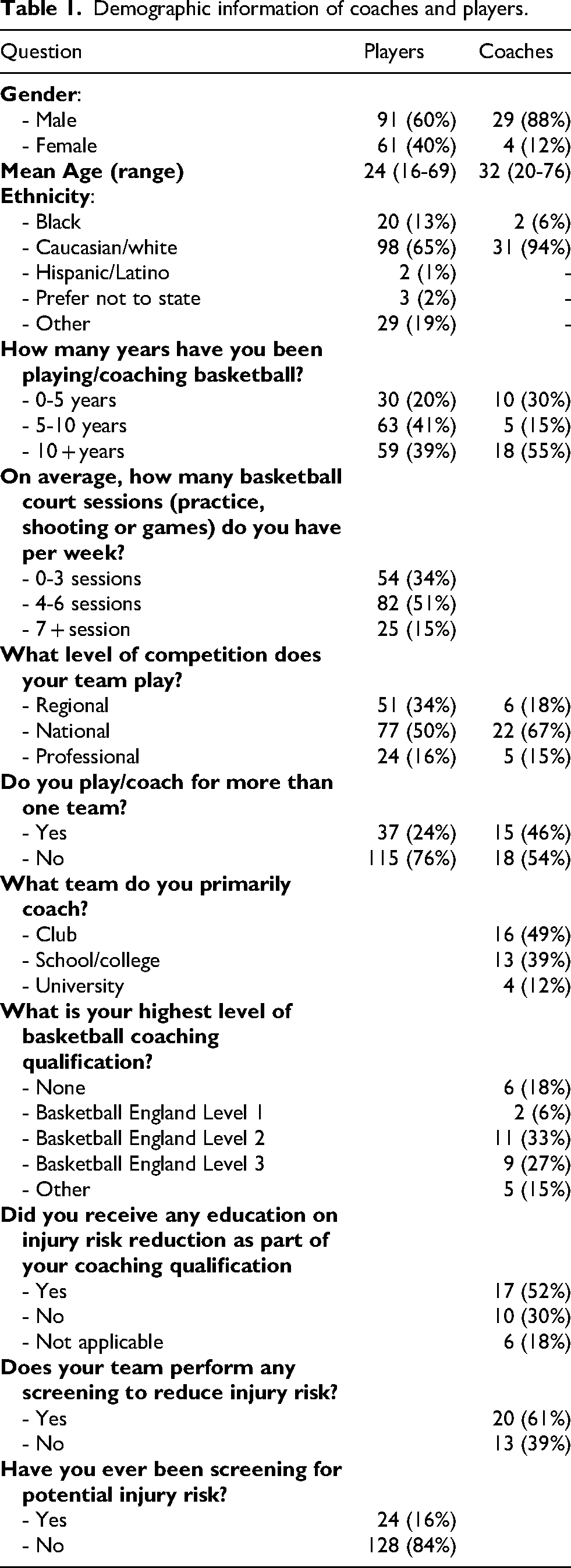
In total, 194 people completed the survey. Eight players were subsequently excluded due to being under-16, whilst one coach filled out the player survey and was excluded, leaving 185 participants (152 players, 33 coaches). Full demographic information is available in Table 1. Players reported they trained for a mean duration of 8.1 h per week (median 7 h). Only 36% of coaches were aware of Basketball England's ‘Starting Five’ programme.
Demographic information of coaches and players.
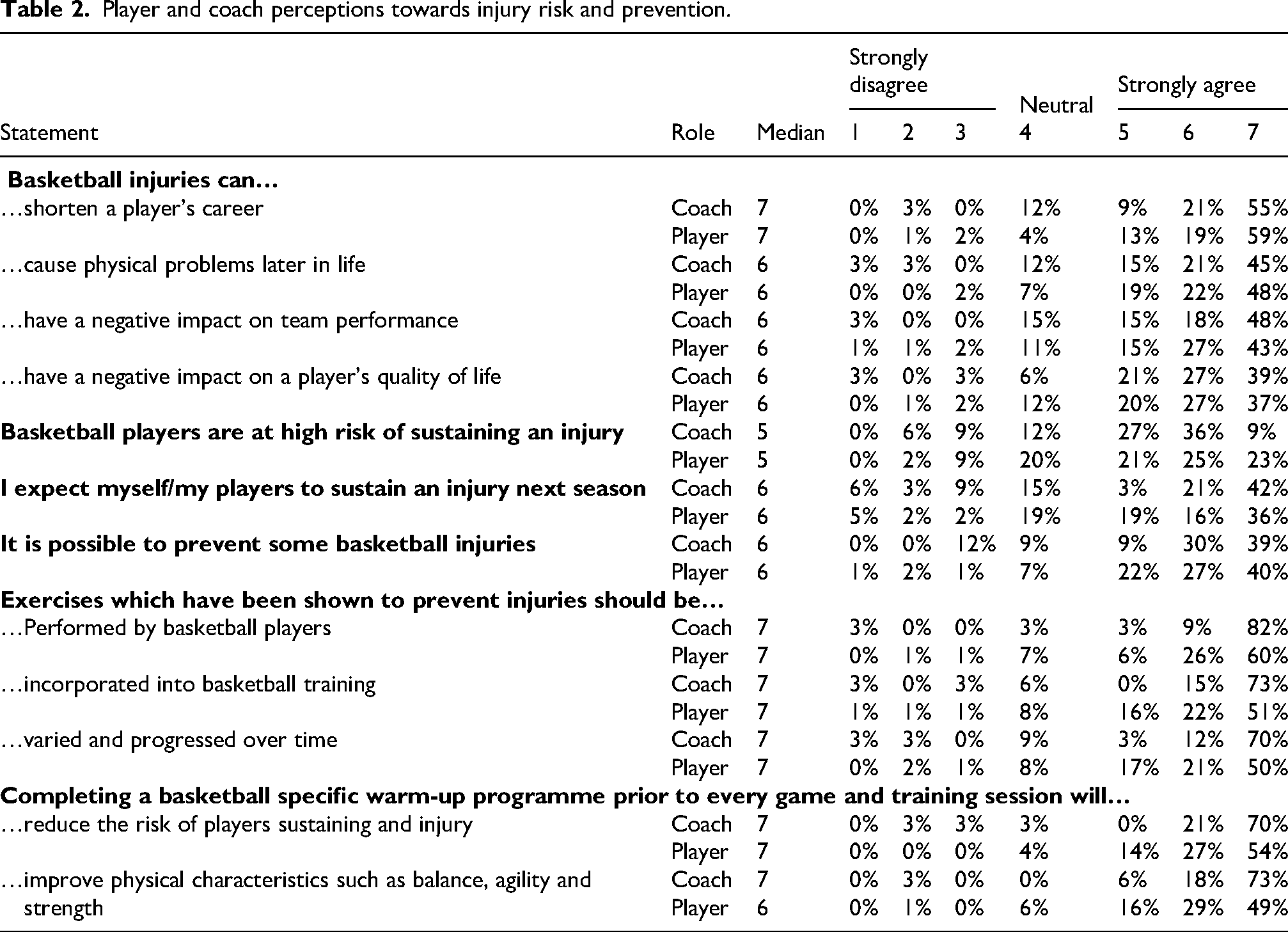
Player and coach perceptions towards injury risk and prevention.
Player injury history (career)
Most players reported they had sustained a basketball-related injury during their career (96.7%, n = 147), whilst 65.1% of participants reported they had sustained a basketball injury that required a hospital visit during their playing career (16.1% of these requiring an overnight stay, 16/99). Furthermore, 18.4% of participants had required surgery for a basketball-related injury in their career (n = 28), whilst over 20% of players had been diagnosed with a concussion sustained whilst playing (n = 35, 23.0%).
Player injury history (within season)
Two-thirds of players reported they had sustained a time-loss injury during the season for which they completed the survey (66.4%), with a quarter of these requiring assessment or treatment at a hospital (26.0%, 25/101). Of the 101 players who reported sustaining an injury during the season, a combined total of 160 injuries, the ankle was the most commonly injured location (41.9%), followed by the knee (16.3%) and finger/hand/wrist (15.6%). Player contact was the most common mechanism (35.1%), followed by non-contact (18.3%) and contact with the ground/surroundings (16.0%). The median injury severity was 8–28 days lost, with 27% of injuries resulting in more than 28 days lost. Half of players reported experiencing anterior knee pain, defined as around or below the patella, during the season (49.3%), with 29.3% of these resulting in time-loss from matches or training (22/75). Over a quarter of players (28.3%) reported achilles pain during the season, with 23.3% of these resulting in time-loss (10/43).
Perceptions towards injury risk and prevention
There was similarity in answers between coaches and players towards the negative impact basketball injuries can have a player's career, team performance and quality of life (Table 2). Both groups ‘agreed’ that some basketball injuries could be prevented, whilst holding positive views towards the use injury prevention exercises, and specifically the benefit of an injury prevention warm-up to reduce injuries. Coaches were more positive than players that a warm-up could improve physical characteristics such as balance, agility, and strength (coach median = 7 ‘strongly agree’; player median = 6 ‘agree’), with all findings non-significant (p > 0.05).
Coaches rated load management and strength training as the two most effective ways to reduce injury risk (mean 6.5/7), whilst players favoured improving landing mechanics and recovery (mean 6.2/7 and 6.1/7, respectively). The largest differences in perceived effectiveness were observed in the benefit of strength, speed and agility training, load management and educational strategies, with coaches holding significantly greater positive beliefs than players for all strategies (all p < 0.01; Figure 1).
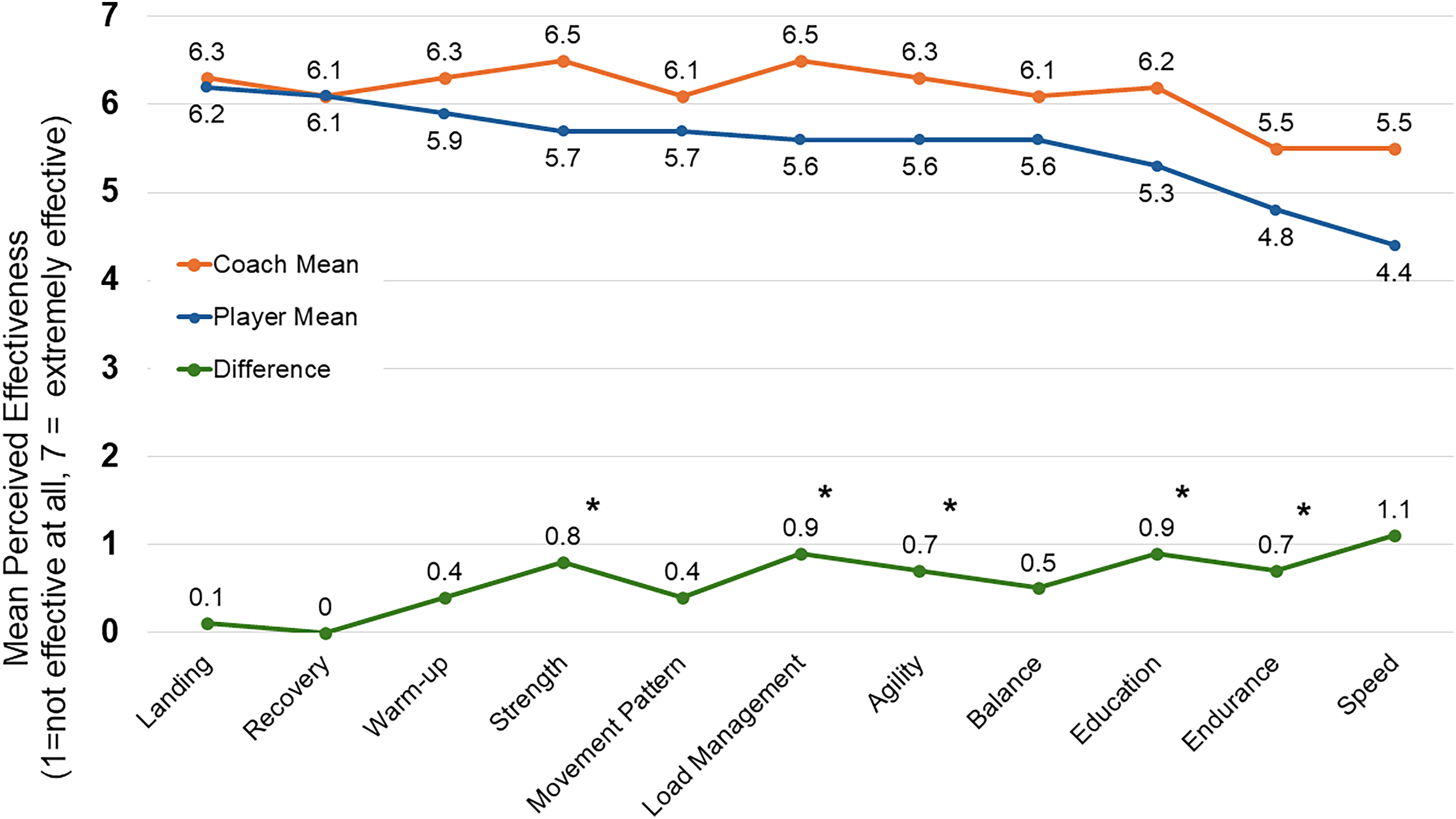
Comparing the mean perceived effectiveness of intervention strategies by coaches and players. *p < 0.05.
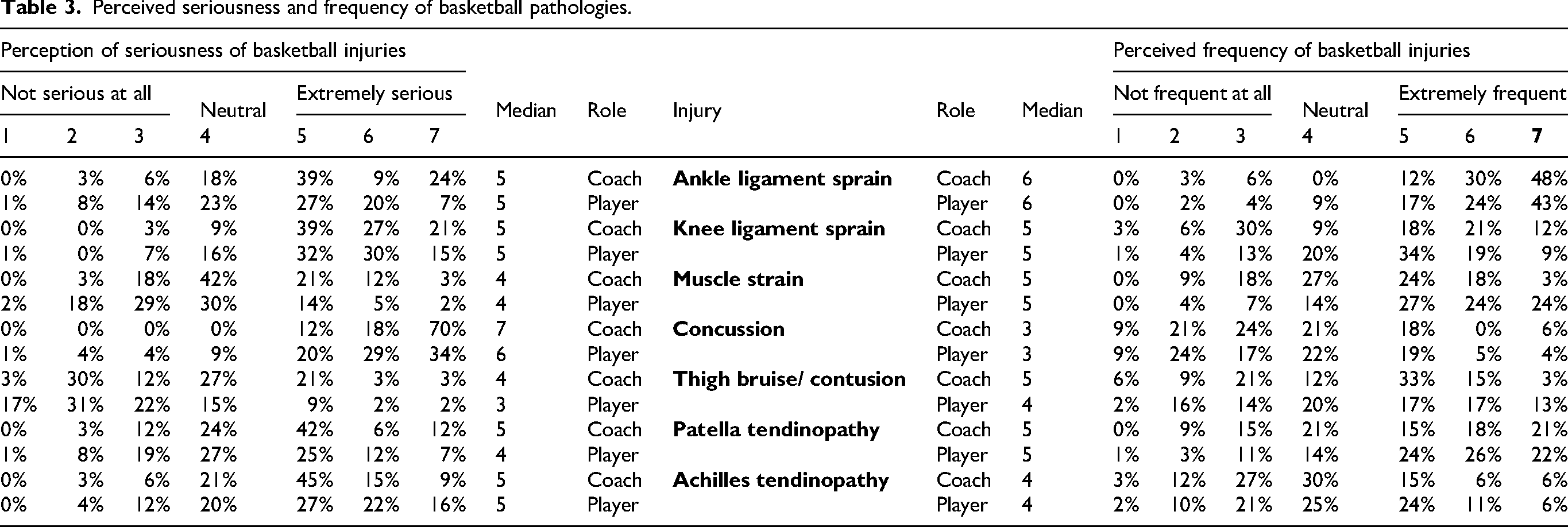
Coaches and players agreed that concussion was the most serious injury, although 69.7% of coaches thought concussion was ‘extremely serious’ versus 33.5% of players (Table 3; z = -4.01, p = 0.003). Coaches and players reported that concussion was the least frequent injury (median = 3), with lateral ankle sprain being the most frequent (median = 6). Players regarded muscle injuries as significantly more common than coaches (z = -3.53, p = 0.018).
Perceived seriousness and frequency of basketball pathologies.
There were notable differences in the perceived responsibility of injury prevention between players and coaches. Players ranked themselves as being primarily responsible (99.4%), whilst believing support staff held more responsibility than coaches. Coaches placed significantly more responsibility on themselves, assistant coaches, parents and the national governing body (all p < 0.01; Figure 2).
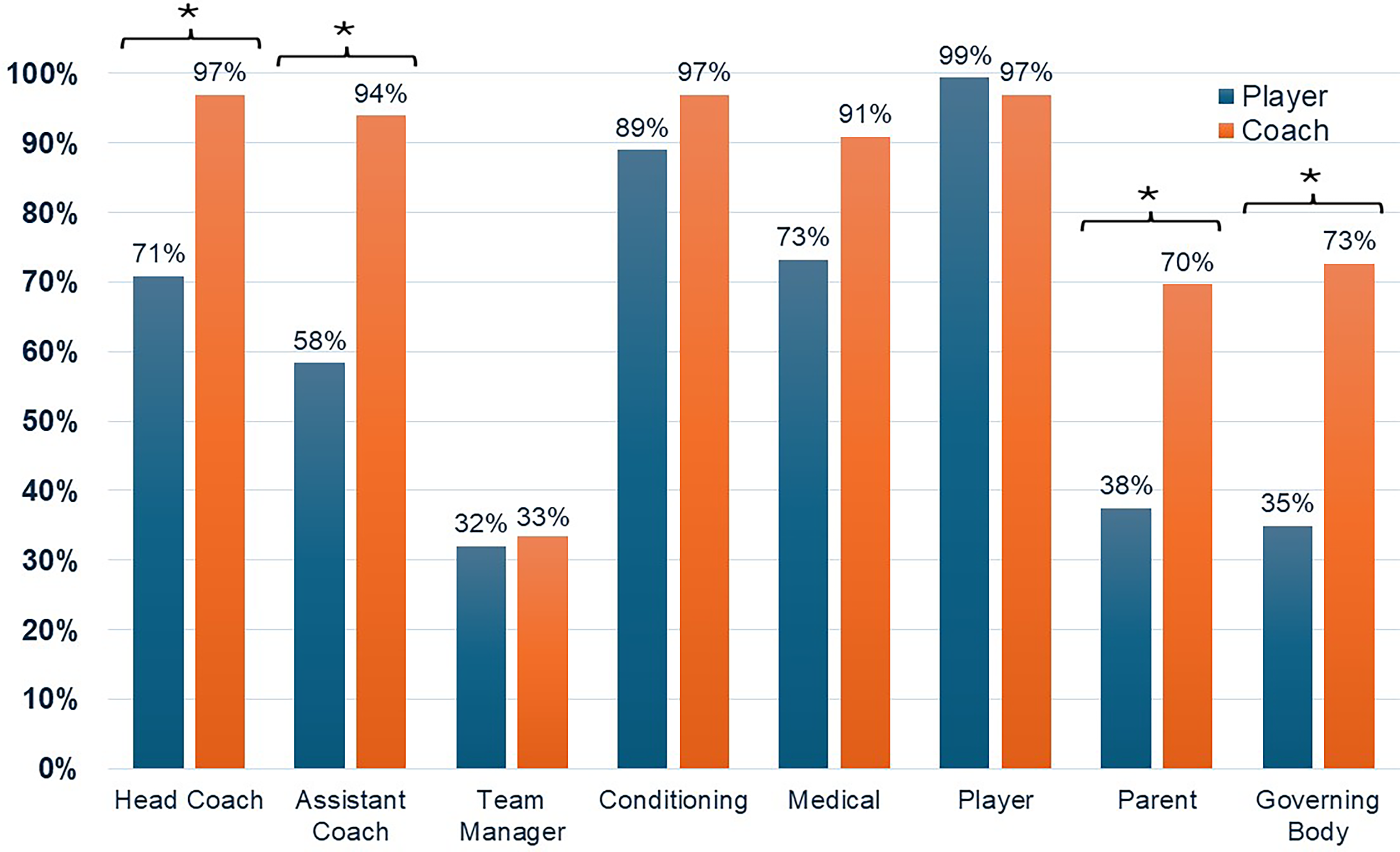
Percentage of respondents agreeing who is responsible for injury prevention. *p < 0.05.
Player preventative behaviour
62.1% of players reported using resistance training as a preventative measure during the season, with 84% of these completing a session weekly (84/100). Less than half of players reported completing any balance training (41%) or integrating landing mechanics (32.9%) or movement competency drills (41%) as a preventative strategy. Half of players reported using protective equipment (50.3%), with 41% of players using ankle bracing (23.0%) or taping (18.0%) during the season, whilst 19.9% of players also wore knee pads. Only 5.6% of players wore a mouthguard and one person wore thigh pads (0.6%).
Discussion
This study sought, for the first time, to describe the injury history of basketball players in England, alongside coach and player perceptions towards injury risk, prevention, and current behaviours. Basketball is an extremely popular sport in England but there is a paucity of evidence around injuries and stakeholders’ perceptions towards them. This study highlights the need for further research into this area, given the frequency and seriousness of injuries being sustained.
Most players (96.7%) surveyed had sustained a basketball injury during their career, reinforcing the fact that playing basketball comes with a risk of injury and has a similar injury risk to other contact sports such as football and rugby. 21 However, the seriousness of injuries sustained is alarming, with over 60% of players attending the hospital and 17% requiring surgery for a basketball-related injury in their career. The profile of injuries sustained within the season for which they completed the survey aligns with those described in the literature. The ankle is reported as the most injured body location across various playing levels and contexts,3,22 whilst most injuries occur as a result of player contact. 3 Half of the players reported anterior knee pain during the season, similar to that of Canadian high-school basketballers who self-reported anterior knee pain (43%), 23 but less than the 67% of male basketballers in a professional Croatian league. 24 The prevention of anterior knee pain in basketball, predominantly patella tendinopathy, is challenging given much of the evidence focuses upon rehabilitation or secondary prevention. 25
Players and coaches alike appear to have good knowledge pertaining to the negative effects basketball injuries can have on a player's career length 26 and team performance. 27 Similarly, both groups held good knowledge regarding the benefits of injury prevention exercises and programmes. Evidence suggests that the use of injury prevention programmes, often termed neuromuscular training programmes, can significantly reduce the risk of lower-limb basketball injuries (OR = 0.69, p < 0.001), 13 particularly at the ankle and knee.13,28 Injury prevention programmes require good adherence and maintenance 29 but are often blighted by poor implementation. A season long observational study of 33 Canadian high-school teams found that coaches did not use the designated injury prevention programme for 20% of sessions, whilst only 65% of coaches used the programme twice or more per week. 30 Reported reasons for poor implementation varied from lack of space, player engagement and time. 30 In the cohort of coaches surveyed in this current study, only one-third were aware of Basketball England's injury prevention programme, ‘The Starting Five’, 31 highlighting awareness as a common barrier. Furthermore, only two-thirds reported receiving education on injury prevention as part of their coaching qualifications. This highlights that injury prevention education is not universally embedded within coaching pathways, which may contribute to variability in awareness and implementation of injury prevention strategies.
Coaches and players had positive perceptions of the effectiveness of all proposed injury prevention strategies, with coaches rating load management as the joint most effective strategy. Professional basketballers participating in more games and/or with minimal rest between games appear to be at a greater risk of injury, 32 but players with lower game demands also appear to be at an increased risk. 33 The relationship between training load and injury risk appears weak,34,35 and it may be that it is fluctuations in load, rather than high loads, which lead to a greater injury risk. 35 No published data has been reported for training load in English basketballers but given the median number of sessions per week was 4–6, alongside 25% of participants playing for more than one team, one could assume the training load would be quite high and varied.
Players regarded recovery as one of the most important injury-preventative strategies. There is moderate evidence to support the use of various recovery strategies, such as sleep, 36 nutrition and cold-water immersion. 37 However, there is little evidence to suggest recovery reduces injury risk in basketballers as players thought. Balance exercises were not ranked highly in comparison to other methods of prevention, despite appearing to be one of the most integral elements of injury prevention programmes, particularly for the prevention of lower-limb injuries. 38 However, in a Canadian cohort, these were the exercises frequently omitted by coaches, 30 perhaps linked to the perceived lack of effectiveness. Despite players not placing much emphasis on education, this is one example where education may improve knowledge, and possibly behaviour, but coaches should also be educated, given they are the individuals often delivering the warm-up.
Coaches and players held similar views towards the severity and frequency of certain injuries, correctly identifying that ankle sprains were the most common injury. 22 Both also recognised the potential seriousness of a sports-related concussion, 39 although underestimating the frequency of a concussion, deeming them less frequent that knee ligament sprains and achilles tendinopathy. The incidence of concussions in basketball are relatively low compared to a lateral ankle sprain but they are still one of the most common pathologies sustained in men's and women's basketball,8,40 with their prevalence highlighted by nearly a quarter of players in this current study reporting they had sustained a basketball-related concussion.
Strength and limitations
Participation bias may mean that those who have previously sustained a basketball-related injury are more likely to participate than those who have not, inflating the descriptive injury statistics. To minimise this, recruitment was open to all individuals nationwide who had played basketball in the current season, regardless of injury history, age, playing level, or gender.
For a player to detail their previous injury history requires recall. To minimise the effect recall bias may have, players were only asked for specific details, i.e., location and mechanism, about injuries that occurred in the season for which they completed the study and thus participants did not have to recall specific information further back than the 6–8-months since the start of the season.
The sample size of participants is low, particularly amongst coaches. It is not possible to state how many basketball players and/or coaches there are in England given there is no central registration of players and coaches. Whilst Sport England reports hundreds of thousands of people play basketball monthly, 6 these are not necessarily in competitions organised or run by Basketball England (national governing body). As such, it is not known. Over 1000 basketball clubs exist in England, and thus there is no doubt number of participants is extremely small, which affects the generalisability and confidence of the results. However, the unstructured nature of basketball in England is one of the reasons why prospective surveillance or injury prevention studies have not been conducted like those observed in other contexts. Whilst retrospective, cross-sectional studies have their limitations, this study does highlight the need for future, large-scale cohort studies to address the injury prevalence described.
Conclusion
Players and coaches acknowledged the negative effects that injuries can have on an athlete or their team. Both groups also held positive perceptions towards the effectiveness of various injury prevention strategies to reduce injury risk, although there were differences in the most effective intervention and whose responsibility injury prevention was. Players detailed an alarming history of serious injuries, with many requiring hospital attention or surgeries. The use of protective equipment was varied, with some effective interventions rarely used and ineffective interventions frequently used. It is hoped that the findings of this study will reinforce the need for future research in English basketball, ranging from injury surveillance to injury prevention.
Footnotes
Acknowledgements
The authors wish to thank the players and coaches who participated in the study.
Ethical considerations
Ethical approval was granted by the Research Ethics Committee at the University of Gloucestershire, UK (REC Number 23.77.2).
Consent to participate
All participants provided written informed consent.
Author contributions
CB conceptualised the idea and devised the methodology with MDSC and JG. CM and CB analysed the data. CB wrote the initial draft with all authors providing critical input. All authors have approved the submitted version.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
All data is presented in the article. No other data is available as part of this publication.