
Abstract
Objectives
To explore the usage and awareness of the FIFA 11 + (11 + ) across multiple stakeholders involved with amateur football.
Methods
Coaches, players, non-coaching staff and medical personnel in New South Wales (NSW), Australia, were invited to complete a cross-sectional online survey, which was disseminated using a targeted email to
Results
In total 328 players, 55 coaches, 37 non-coaching staff and 16 medical personnel completed the survey (n = 436). Awareness of the 11 + was lowest among non-coaching staff (16.2%) and players (32.6%) but higher among coaches (52.7%) and medical personnel (93.8%). Once aware of the 11 + , 75.8% of all respondents used the program although 89.5% of them did so with modifications. In addition, only 40.0% of players reported completing all three parts of the 11 + program. Veteran players were less likely to complete any type of warm-up compared with junior players (63.7% vs. 96.3%, respectively).
Conclusions
Although awareness of the 11 + varied amongst survey respondents, 3 out of 4 respondents who were aware of the 11 + adopted the program. However, respondents reported modifying the 11 + and not completing the program as intended, which suggests modification guidance is required to maintain the efficacy of the 11 + .
Introduction
Football (soccer) is one of the most popular sports worldwide, offering numerous physical, social, and psychological benefits, 1 but it also comes with a potential risk of injury. Knee joint injuries such as anterior cruciate ligament (ACL) ruptures, lower limb fractures and ankle sprains are common2,3 and can have long-term consequences. 4 Injuries also pose a significant financial burden to the player, health 5 systems, and the community. 4 In New South Wales (NSW), Australia, football-related injuries accrued insurance costs of AU$13,716,173 over three seasons (2018–2020), at an average cost of $3309 (95% CI 3042–357) per injury. 6 Knee injuries accounted for almost half (49%) of all costs with ACL ruptures representing a quarter (26%) of all costs reported. 6 Similar cost data have also been reported for amateur football injuries in Switzerland, 7 a country with a comparable population to NSW.
Sports injury prevention research in football has gained traction over the last two decades with countries including New Zealand, Belgium, Germany, and Switzerland implementing population-wide preventative measures with mixed results. 8 Arguably the most well-known injury prevention exercise program in football is the FIFA 11 + (henceforth, 11 + ). The 11 + was designed in 2006 in collaboration with the Santa Monica Sports Medicine Foundation and the Oslo Sports Trauma and Research Centre with the aim of preventing the most common lower limb injuries in football players (knee ligament injuries, ankle sprains and hamstring injuries). 5 The 11 + includes 15 football-based exercises and comprises three parts (part 1: running exercises; part 2: strength, plyometric and balance exercises; part 3: dynamic running exercises) and takes approximately 20 min to complete. 9 The 11 + has been shown to decrease injuries by up to 40% 10 (50% for ACL injuries) 11 and is one of the most researched injury prevention interventions with over 40 scientific studies supporting its efficacy. 12 The physiological and biomechanical effects of the 11 + have been tested in Italian male amateur players, 13 junior male Malaysian professional players 14 and Portuguese male sub-elite players 15 reporting generally positive results. However, a recent systematic review has advised against using the 11 + before competition, reporting that the program may acutely decrease player performance (sprinting and dribbling). 16 Adherence with the program is critical as a dose response exists in that players who completed the 11 + three times per week sustained fewer injuries than those who completed the program less often.17,18
Adherence has been defined as a pro-active behaviour to follow recommendations. 19 As the 11 + is not mandated in Australia, the decision to implement and complete this program rests with the respective associations, clubs, coaches and players.
Sports injury prevention is part of a complex systems phenomenon,20,21 with contextual variation21,22 and multiple stakeholder involvement 23 which is problematic for universally applied programs like the 11 + . Such programs frequently prove efficacious 12 but are often poorly adopted in the real world. 21 For example, despite the 11, and partially 11 + , being part of coach education in Switzerland, supported by a nationwide implementation effort, 24 uptake amongst coaches remains below 22%. 5 If coaches are not adopting the 11 + , understanding why they are not using the program is critical. The reported barriers to using the 11 + include coach buy-in, motivation, concerns regarding the duration of the program and player fatigue from completing the second part of the 11 + at the start of a training session.25–27
Cross-sectional surveys are an important research tool for investigating the awareness, usage and implementation of the 11 + . Surveys from other countries28–31 and states 32 have generally focused on coaches and professional or youth players rather than the broader category of amateur players. Implementation should be measured and disseminated across all stakeholder levels, not just players or coaches, to potentially increase program uptake and effectiveness. 33 Non-coaching staff and medical personnel contribute significantly to the implementation of injury prevention programs but are often omitted from survey research. Coach awareness of the 11 + varies between 42% and 80%28,29 with the majority of studies finding that coaches who were aware of the 11 +, used the program.28–30 This type of research is lacking at the amateur level in Australia and elsewhere.
The primary aim of this study was to assess the awareness and usage of the 11 + and other warm up/cool down practices of coaches, players, non-coaching staff and medical staff involved with amateur football. A secondary aim was to stratify players to compare usage and awareness of the 11 + by sex and age group.
Materials and methods
The study was approved by the institutional Human Research Ethics Committee (HREC, 2021/156).
Study sample
Football NSW is the largest football member federation in Australia. 34 Approximately 160,000 amateur football players (aged 11 years and older), coaches, non-coaching staff and medical personnel registered with Football NSW were eligible to complete the survey. 34 Amateur playing level in NSW is divided into: National Premier League 1; National Premier League 2–4; State league/Championship One; Regional; and Other (metropolitan based teams below state league level). Football NSW has 17 metro associations (433 clubs) and 15 regional associations (179 clubs). Northern NSW has seven associations and 178 clubs.
Player age groups were stratified into Junior (7–17 years), Senior (18–34 years) and Veteran (35 + years), which is consistent with Football Australia's age group stratification. 34 Amateur football was defined as clubs registered to compete below the top tier (A-League or W-League) in Australia. Non-coaching staff included paid and volunteer staff in roles such as managers, administrative staff and treasurers. Coaching staff included technical directors (head of club development), coaches and coaching assistants. Medical staff included non-coaching staff involved with player welfare including physiotherapists, sports trainers and doctors. For adults, consent was implied by completion of the survey. Children under 18 years were highlighted by a check box at the start of the survey and parental consent was required for participants aged under 18 years.
Survey design
The online cross-sectional survey's development was guided by similar surveys25,30,31 and the RE-AIM framework. 35 The survey was pilot tested with people representing the target population (players, coaches, one administrator, and medical personnel). The survey collected information on respondents’ demographic characteristics (age, sex, and playing level), injury history (players only), warm up/cool down practices and awareness/use of the 11 + . The survey included multiple choice, yes/no and 5-point Likert scale responses (Tables 1 and 2 outline the type of response for each question). Branching logic was used within the survey, for example, only respondents who answered ‘yes’ to the question, “have you ever used the 11 + ?”, were directed to the question, “does your team currently use the 11 + ?”. The notes section in Tables 1 and 2 outline the filter process. The survey was created using Research Electronic Data capture (REDCap, Nashville, TN, US). 36
Injury education and warm-up behaviors of players, coaches, non-coaching staff and medical personnel by role (n = 436).
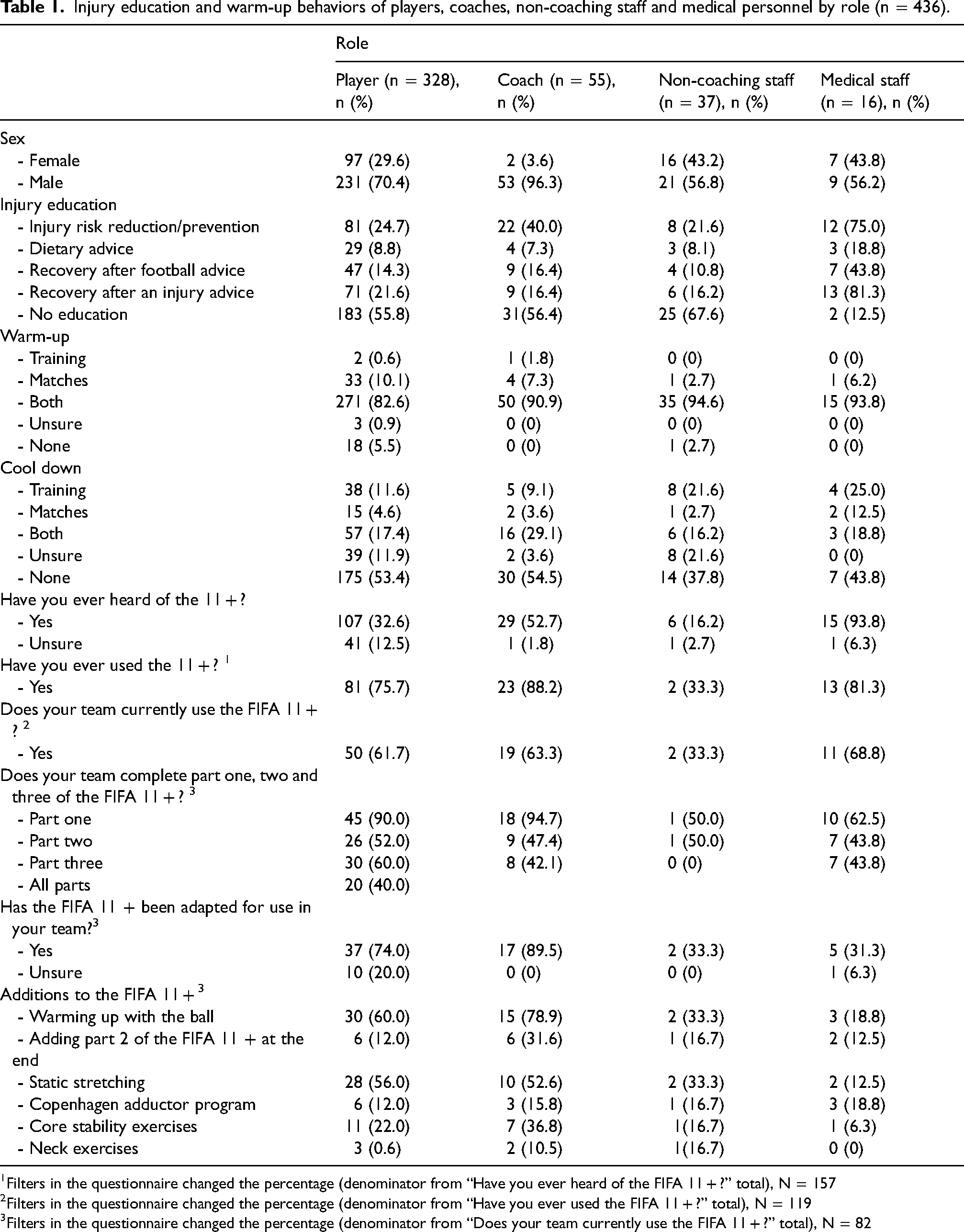
Filters in the questionnaire changed the percentage (denominator from “Have you ever heard of the FIFA 11 + ?” total), N = 157
Filters in the questionnaire changed the percentage (denominator from “Have you ever used the FIFA 11 + ?” total), N = 119
Filters in the questionnaire changed the percentage (denominator from “Does your team currently use the FIFA 11 + ?” total), N = 82
Injury education and warm-up behaviors of players by age group and sex.
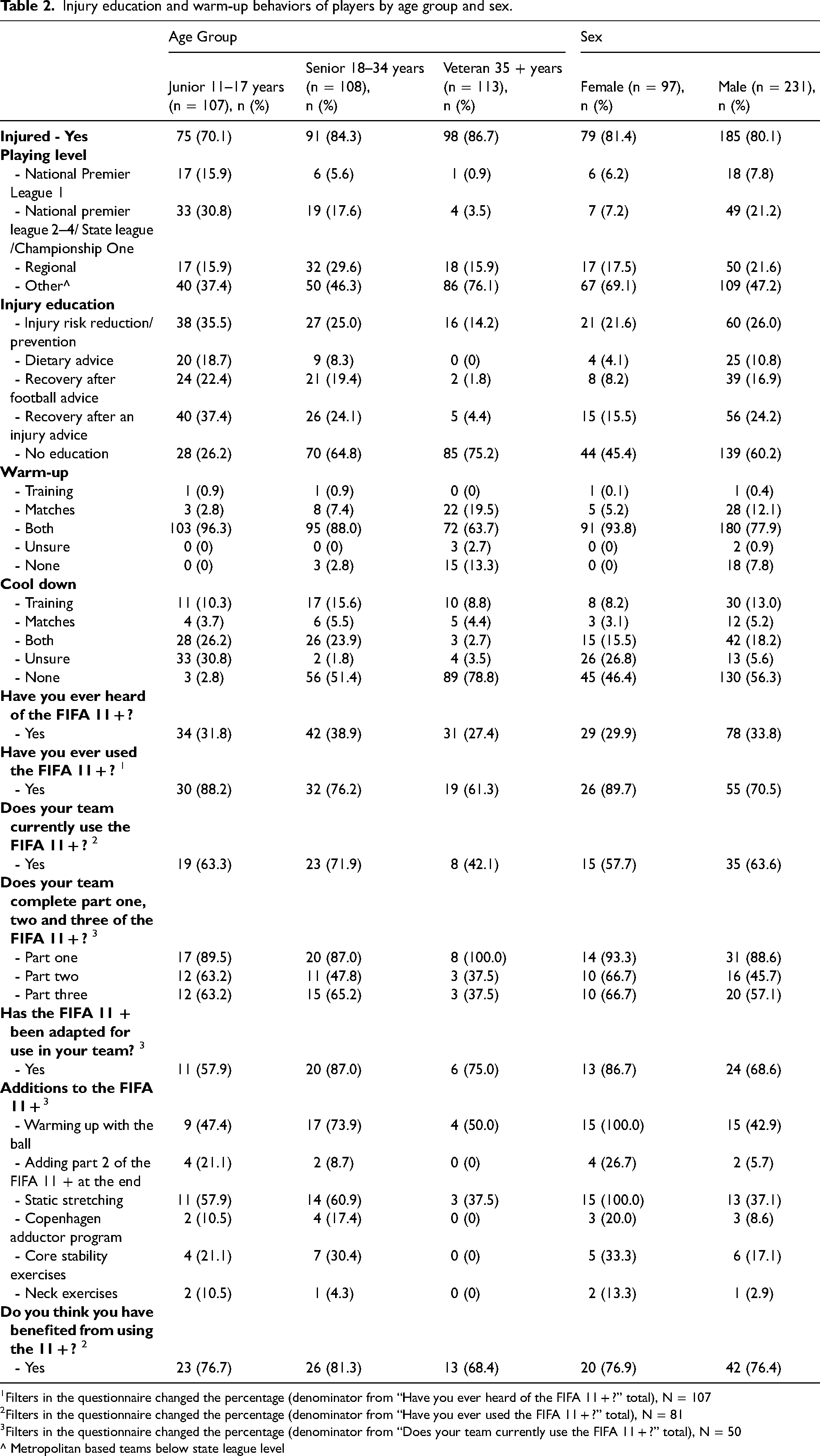
Filters in the questionnaire changed the percentage (denominator from “Have you ever heard of the FIFA 11 + ?” total), N = 107
Filters in the questionnaire changed the percentage (denominator from “Have you ever used the FIFA 11 + ?” total), N = 81
Filters in the questionnaire changed the percentage (denominator from “Does your team currently use the FIFA 11 + ?” total), N = 50
^ Metropolitan based teams below state league level
Survey distribution
The Chief Executive Officer/Head of Football from two member organisations (Canterbury and District Soccer Football Association and Northern Suburbs Football Association) registered with Football NSW received a targeted email from the research team requesting them to invite their clubs to participate in the survey. A digital poster asking stakeholders to complete an online anonymised cross-sectional survey was disseminated via social media (Twitter and Facebook) to target coaches, players, non-coaching staff and medical personnel. An a priori sample size was calculated using the Qualtrics© online calculator 2022. 37 Using a Confidence level of 95% and a Confidence interval (CI) of 5, it was calculated that a minimum of 384 completed surveys was required.
Data collection and analysis
The survey was active from the beginning of June 2021, to coincide with the NSW football season, until November 2021. Data were analysed using STATA for Mac (version 21.0, Inc. Chicago, IL, U.S.). Categorical data (including age-groups and sex) are presented as counts and percentages and analysed using a Chi-square or Fisher's exact test (when the value for any cell was <5). A significance level of 0.05 was used for all analyses.
Results
From a total number of 503 collected surveys, 67 incomplete surveys (where respondents opened the survey but did not answer any questions) were excluded. This resulted in 436 surveys, including 43 partially completed surveys, being included in the analysis. The total sample contains 328 players (231 male and 97 female), 55 coaches, 37 non-coaching staff and 16 medical personnel.
Players
Table 1 presents the warm-up behaviours of all players and Table 2 presents the injury behaviours of players by age and sex. A high number (80.5%) of players reported having sustained an injury (“have you ever suffered an injury whilst playing soccer as a Football Australia registered player”). There were no significant warm-up behavior differences between sexes.
Injury prevention behaviour by age group
Table 2 presents warm-up behaviours by age group. The number of players who warmed up before games decreased with age (junior players, 96.3% vs. veteran players, 63.7%, p = 0.04). The receipt of injury education also decreased with age, with 75.2% of veteran players and almost 65% of senior players reporting that they received no injury prevention education from their club. A large percentage of veteran players reported completing no off-season preparation compared to senior players (81.4% vs 45.4%, p = 0.008). A higher percentage of veteran players (31.9%) also reported no in-season training preparation, compared with 13.9% of senior players (p = 0.01).
Injury prevention behaviours by role
Players, coaches, non-coaching staff and medical personnel
Table 1 presents injury prevention behaviours by role. The majority of coaches were male (96.3%) regardless of whether they coached male or female teams. Over half of all coaches (56.4%) reported that they provided no injury education information to players. Similarly, just over half of all players (55.8%) self-reported no injury management information from their club. Over half of all players (51.5%) reported no off-season preparation whilst 34.5% of coaches and 54.1% of non-coaching staff reported providing no off-season preparation advice.
Awareness and use of the 11 +
A high number of players (92.7%), coaches (98.2%), non-coaching staff (97.3%) and medical personnel (100%) reported warming up prior to matches, training or both. However, only 18.8% of the entire sample currently use the 11 + at their club (this includes participants who were not aware of the 11 + ). Medical staff reported the highest levels of awareness of the 11 + program (93.8%), whilst coaches (52.7%), players (32.6%) and non-coaching staff (16.2%) reported lower levels of awareness. Of the 107 players, 29 coaches and 15 medical staff who were aware of the 11 + , most reported experience in using the program (75.7%-88.2%) with over 60% of players, coaches and medical staff currently using the 11 + at their present club. A lower number of non-coaching staff (33.3%) reported that their club was currently using the 11 + .
In addition, over half (52.6%) of all coaches and medical staff reported completing the full 11 + (parts one, two and three). The part least likely to be completed was part 2 which contains strength, plyometric and balance exercises, followed by part 3 which contains high-speed running. A large percentage of coaches (89.5%) reported modifying the 11 + for their sessions, including additions such as static stretches and using a ball. Table 1 outlines the modifications that coaches use.
Discussion
Our key findings show that (1) despite the majority of coaches and players reporting that they incorporated a warm-up and cool down into training and match preparation, only 18.8% of all respondents currently use the 11 + ; (2) awareness of the 11 + among non-coaching staff is very low (16.2%); (3) the most common coach modification is the addition of a ball in the warm-up; (4) parts 2 and 3 of the 11 + have poor adherence; and (5) there were notable injury prevention behaviour differences across age groups.
Awareness and use of the 11 +
Considering 95.6% of respondents in our study completed a warm-up before training, matches or both, but only 18.8% currently complete the 11 + , meaning that 76.8% of the sample is potentially using a different type of warm-up with unknown effectiveness in reducing injuries. Our study reported low awareness of the 11 + among players (36.0%) and coaches (52.7%). This is consistent with a German survey with amateur coaches reporting 42.6% awareness of the 11 + . 29 Conversely, a study in Switzerland a much higher awareness rate amongst 1000 Swiss coaches (80%) with 57% adopting the program, 5 although this drops to 21% on 10 year follow-up. 24 A prerequisite for using the 11 + is being aware that it exists (also known as unintentional non-adherence), with our results showing that adherence rates increased substantially once they were aware (adherence increased to 88% of coaches, 76% of players and 81% of medical staff once aware). This is similar to findings from Germany, Saudi Arabia and Australia that reported 73–75% of aware coaches use the 11 + .28,29 These results indicate that despite the 11 + being one of the most widely known football-specific injury prevention programs, there are global issues with dissemination of the program across all levels of football, further confounding adherence data. However, dissemination is only one element as between 12–24% of coaches and players still did not complete the 11 + despite being aware of it. Considering 76.7% of players and 81.3% of coaches in our study reported that they benefited from using the 11 + , alternative methods of delivery and dissemination are warranted. Future research could further explore barriers and facilitators for the delivery, dissemination and implementation of injury prevention programs with the use of semi structured interviews or qualitative surveys.
Awareness among non-coaching staff
Football-related injuries and their prevention are under the control of multiple stakeholders (coaches, medical staff, non-coaching staff and sporting organisations) that intersect with the players at a socio-ecological level. 38 Our study highlighted that only 16.2% of non-coaching staff (administrators) were aware of the 11 + . To improve dissemination, and ultimately increase the chance of implementation success, all stakeholders should be made aware of prevention strategies. 39 Administrators should be encouraged to collaborate and develop partnerships with key stakeholders, including sporting organisations. Switzerland, New Zealand and South Africa are good examples of countries that include multiple stakeholders in the injury prevention conversation. 8 These countries have forged long-term partnerships between researchers, national insurers and community clubs. 8 Incorporating the opinions of multiple stakeholders has helped to emphasise key sporting infrastructure details and highlight the injury culture, all factors that may shed light on the barriers to program adoption.5,8,40 However, challenges remain for all countries attempting to embed preventative programs over long periods. For example, the uptake of the 11 + in Swiss soccer revealed minimal change between 2008 (21.7%) and 2015 (21.9%). 24
Content and delivery
A warm-up with flexible content will provide coaches with more choice and potentially increase buy in and adherence. 41 Modification of the warm-up was common in our study. A large percentage of coaches (89.5%) modified sessions and players (74.0%) received modifications in their sessions. For example, 78.9% of coaches in our study warmed up using a ball. Currently, there is no option to use a ball in the official 11 + material. Therefore, adding this option of a ball to aspects of the 11 + may increase coach buy-in and player interest. Less than half of all coaches and medical staff complete the full 11 + as intended (parts 1, 2 and 3) with only 48.3% of respondents completing part 2 of the 11 + . Flexible modes of delivery may assist with increasing player adherence with part 2 of the 11 + . For example, re-scheduling Part 2 of the 11 + to the end of a training session 42 and completing it as a home exercise program 43 has been shown to maintain its effectiveness and increase adherence. In our survey 31.6% of coaches and between 12–17% of other stakeholders added part 2 of the 11 + to the end of a training session. This research demonstrates that it is possible to move the content of the 11 + to outside the standard warm up structure. Modifying the style of delivery may assist with increasing coach buy-in and ultimately averting football-related injuries.
If coaches are modifying the 11 + with no scientific guidance and players are not completing the full 11 + as intended, the efficacy of the program is at risk. Future research should aim to understand the core components of the 11 + , which may allow for modifications whilst maintaining program effectiveness. For example, low dose (4-week × twice a week) Nordic Hamstring Exercises are safe to implement during a season when accompanied by higher volumes in preseason. 44 This type of research is a step towards understanding the minimal dose required for a preventative effect. In this case, perhaps a low volume of part 2 of the 11 + in-season could save time, a potential solution to one of the barriers to coaches adopting the 11 + (duration of the program). 26
Differences across age-groups
There were significant differences across age-groups. The number of players who warm-up before matches and training decreased with age in our study. We found that although a high percentage of players warmed up before training and matches, veteran players were significantly less likely to warm-up before training and matches compared with junior players. A similar study which undertook routine surveillance of injury and safety behaviours in community-level soccer players over one season in New Zealand reported higher adherence figures in master's players compared with younger age groups (aged 35 and older, matches = 94.8% and training = 90% adherence). 30 The ‘SoccerSmart’ 45 injury prevention program is mandatory for all coaches, which may explain some of the difference between the adherence figures, compared with our study. Studies have found that increasing age could be a risk factor for injury in amateur football players2,46 and injury costs are higher in veteran players in NSW. 6 Therefore, research exploring age-specific injury prevention programs and ascertaining the facilitators and barriers to these programs is warranted.
A review of the previous coaching curriculum in Australia shows that the 11 + content was not embedded into coaching course material, which may explain the low awareness of the program reported in this study (36.0%). The 11 + has never been actively disseminated within NSW but is endorsed by Football NSW. 47 Football Australia, via consultation with sports injury researchers, coach educators, technical directors, coaches and sports scientists, recently developed the Perform + . 48 The Perform + is an example of an injury program that has evolved from the 11 + . Although the program is based on the 11 + , 12 it contains updated content and addresses barriers to implementation. Although it remains unclear who is ultimately responsible for injury prevention in Australia, the inclusion of the Perform + in the advanced Australian coaching curriculum is a ‘low hanging fruit’ dissemination decision and may have significant population wide preventative effects. New Zealand has had some success with implementing coach education with 96% of football coaches changing their coaching behaviour following a ‘SoccerSmart’ education session. 45 It is the authors hopes that the inclusion of the Perform + in the coaching curriculum is a start in addressing our finding that more than 50% of coaches do not educate players in terms of injury prevention, with senior (64.8%) and veteran players (75.2%) receiving no prevention education at all. Injury prevention strategies clearly require all stakeholders, from the player themselves, through to coaches, parents, sports clinicians, sporting organisations and government to take on the responsibility of injury prevention in football. 49
Limitations
Our descriptive cross-sectional survey design has limitations. Although our sample size meets the power calculation, once stratified into stakeholder role (e.g., coaches, non-coaching staff and medical personnel) the sample size is very low. In total, 328 players out of a total of 160,000 players registered in NSW completed the survey. However, considering one team is likely to have 1–2 coaches and one medical staff member the sample numbers provide an important first step to understanding stakeholder injury prevention behaviours. Since the 11 + was not embedded into the coaching curriculum in NSW, it is important to note that the low awareness of the 11 + program may be partially explained by this factor.
Our survey relied on self-reported measures which may be confounded by recall bias. Data were collected in NSW only, which captures half of all players in Australia. Therefore, results may not generalise to other states and countries. 34 As social media was used during the recruitment strategy along with emails sent to the sporting organisations who then invited their members to complete the survey on our behalf, the specific number of invited people could not to be tracked. Therefore, a survey response rate could not be calculated increasing the risk of nonresponse bias. 50 A further limitation is the lack of information regarding the survey respondents’ club, which adds the possibility of multiple responses from the same player. A high percentage (46.7%) of junior players reported that they played at state league level or above compared to 13.6% of senior and veteran players. The playing level difference amongst age groups may affect data comparisons and distribution.
Conclusion
The current use of the 11 + in amateur football clubs in NSW is low at 18.8% with unintentional non-adherence (or stakeholders being unaware of the program's existence) being a primary contributing factor. In addition, a high number of coaches that are aware and currently using the 11 + in a modified form. Players are not completing the program as intended, indicating that the program may not be meeting their needs. Further research is required on what effect program modification has on its effectiveness as well as further in-depth exploration of why football stakeholders do not complete the 11 + as intended. Age differences were also notable in our study. Veteran players are less likely to warm-up and receive injury prevention advice during the season, which is concerning, considering that increasing age appears to be a risk factor for injury. The results from this study provide a useful baseline measure of the awareness and usage of the 11 + by coaches, players, non-coaching staff and medical personnel in NSW, Australia. It is clear from this survey, and others,28–30 that important opportunities exist for amateur football organisations to improve the uptake of evidence-based injury prevention programs which can make football safer and allow players to reap the full emotional, financial, intellectual, physical, and social benefits of football.
Footnotes
Acknowledgments
The authors would like to thank Football NSW and Northern NSW Football for assistance with disseminating the survey during the recruitment phase.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.