
Abstract
High-G flight presents extreme neuromuscular and cardiovascular challenges, particularly for fighter pilots exposed to repeated accelerative stress. While traditional training emphasizes aerobic capacity and dynamic strength, these paradigms often fail to reflect the static, posture-bound demands of flight operations. The constrained cockpit environment, combined with helmet and night vision goggle (NVG) load, creates persistent axial stress on the cervical and lumbar spine, while G-onset imposes lower limb and lumbar tensing requirements to preserve cerebral perfusion. These realities position isometric strength training (IST), characterized by force production without joint movement, as a biomechanically superior approach for enhancing G-tolerance, posture stability, and injury resilience. This narrative review integrates current evidence on task-specific muscular demands in tactical aviation and presents isometric strategies as a low-cost, high-transfer training modality. It emphasizes the distinction between yielding (HIMA) and overcoming (PIMA) isometrics, maps these to specific flight tasks (e.g., cervical holding under load, Anti-G straining maneuver tensing), and outlines pragmatic assessment protocols using field-accessible tools such as handheld dynamometry and endurance hold benchmarks. The review further proposes region-specific programming (neck, trunk, lower limb) and embeds these within realistic operational schedules through micro-sessions and warm-up integration. Adopting IST across the pilot training continuum offers three major operational advantages: improved G performance via muscular tensing and vascular compression, reduced in-flight fatigue through enhanced isometric endurance, and fewer musculoskeletal injuries by reinforcing high-risk anatomical regions under strain. This work advocates for formalized implementation of isometric protocols as a foundational element in aircrew conditioning, supported by targeted research into normative data, dose-response, and performance outcomes.
Keywords
Introduction
During high-performance maneuvers, fighter pilots are predominantly exposed to + Gz (head-to-foot) acceleration, which increases the hydrostatic pressure gradient along the body and places substantial demands on cardiovascular regulation and musculoskeletal stabilization.1,2 While general health-oriented conditioning paradigms (i.e., those typically prescribed for the general population) emphasize dynamic strength and aerobic capacity, these approaches may inadequately mirror the static, constrained postures characteristic of actual flight operations. In contrast, aircrew-specific conditioning programmes have been developed and evaluated for their influence on + Gz-related performance outcomes (e.g., the Royal Air Force Aircrew Conditioning Programme) and for broader physical performance adaptations in military pilot populations.3–7 Unlike sports movements that allow full joint excursions, cockpit environments require force generation under fixed, quasi-static conditions with limited momentum and joint repositioning. 8
The unique ergonomic demands of the cockpit, restricted movement, sustained axial loads, and head-mounted mass, place specific strain on the cervical and lumbar regions.9–11 Individual differences in G-tolerance are multifactorial, and even plausible predictors such as ACTN3 genotype and body composition have shown inconsistent associations in fighter-pilot samples. 12 Given these constraints, a mismatch arises between traditional training goals and in-flight neuromuscular demands, which are more aligned with isometric endurance, joint-specific stabilization, and postural tensing.13–15
Recent literature has highlighted the unique neuromechanical advantages of isometric strength training (IST), including enhanced joint-angle–specific force, improved force steadiness, increased tendon stiffness, and superior fatigue resistance during prolonged submaximal exertions.3,10,16 Such adaptations are crucial during prolonged high-G exposures, where mechanical stability and neuromuscular control prevent posture collapse and reduce injury risk.4,17
The anti-G straining maneuver (AGSM), essential for preserving cerebral perfusion during G-onset, involves repetitive, high-effort isometric contractions of the lower limbs and trunk. These contractions are performed under increasing fatigue, underscoring the relevance of repeatable isometric force production.8,18 Yielding isometrics, defined as holding posture against external force, more accurately reflect the neuromechanical demands of G-loading, helmet weight, and AGSM than overcoming isometrics, which involve pressing into an immovable object.13,19, 20
Despite this task alignment, isometrics remain underused in high-performance military conditioning. Perceived as “non-functional” or “static,” they are often undervalued despite their efficiency, minimal equipment needs, and reliable metrics such as peak force, time-to-fatigue, and variability.9,11 Importantly, tools like handheld dynamometry and helmet-attached force sensors now allow precise, field-friendly assessments of neck and postural strength relevant to flight demands.19–21
Isometric training represents a physiologically congruent, logistically feasible, and evidence-supported countermeasure to the physical challenges of high-G environments. Its integration into military performance paradigms should not be seen as supplemental but foundational, equipping pilots with the neuromuscular resilience to stabilize, brace, and resist fatigue under the extreme demands of repeated acceleration. Future research should aim to expand normative IST profiles for pilots, optimize joint-specific protocols, and explore hybrid models that combine yielding and overcoming modalities for maximal transference to in-flight performance.4,8 Despite this clear task alignment, isometrics remain underutilized in military human performance programs. One reason is the perception that “static” training is less engaging or lacks functional value. However, the efficiency, minimal equipment requirement, and measurable outcomes of isometric training (e.g., peak force, hold time, force variability) make it ideal for operational settings with time and logistical constraints.3,9 Additionally, assessment tools like handheld dynamometry or time-to-fatigue tests allow trainers to monitor progress and mitigate injury risk, especially in the cervical spine.10,16
High-G flight: task analysis and physiological loading
G-load physiology relevant to training
High-G flight places the human body under extreme accelerative forces that frequently exceed +9 Gz in tactical aviation environments.5,6,22–25 These forces dramatically alter hydrostatic gradients, driving blood into the lower extremities, thereby reducing venous return, impairing cardiac output, and diminishing cerebral perfusion pressure. Such hemodynamic shifts contribute to transient visual impairments, including grey-out and blackout. and, in severe cases, G-induced loss of consciousness (G-LOC).1,26
While aerobic fitness has traditionally served as the cornerstone of pilot conditioning, emerging evidence underscores that G-tolerance is not determined solely by cardiovascular capacity. Rather, it is the integration of neuromuscular strategies, particularly continuous whole-body muscle tensing maintained throughout + Gz exposure as part of the AGSM, which plays a critical role in maintaining vascular resistance and cerebral blood flow during rapid G-onset27–29 These muscular strategies act as mechanical aids to circulatory control by reducing lower-body blood pooling and augmenting venous return, thereby supporting arterial pressure and cerebral perfusion and supplementing baroreflex limitations during extreme gravitational transitions.30,31
The Anti-G Straining Maneuver (AGSM) exemplifies this neuromuscular-cardiovascular interface. During high-G exposure, pilots engage in a sequenced combination of lower-limb, pelvic floor, and abdominal muscle contractions, synchronized with thoracic pressure regulation and forced expiratory techniques. These isometric contractions serve to compress the major veins in the abdomen and legs, thereby increasing systemic vascular resistance and maintaining upper-body blood volume.32,33 Effective AGSM performance is therefore not merely procedural but physiological; it requires significant isometric endurance and coordination to sustain the maneuver across repeated G-onsets, often under cognitive and physical fatigue.16,24,34
Crucially, the rate of + Gz onset is one factor influencing pilot tolerance. Although rapid onset profiles reduce the available time for cardiovascular compensation and increase reliance on anticipatory (feedforward) control and pre-activation of tensing musculature, G-LOC may still occur during relatively low onset-rate exposures depending on the magnitude and duration of + Gz, the effectiveness of the AGSM, and individual susceptibility.1,9,14,35 This dynamic elevates the importance of isometric force-readiness in key anatomical regions, notably the gluteals, hamstrings, and abdominal wall. Therefore, to ensure operational safety and resilience, training paradigms must extend beyond aerobic capacity to specifically cultivate localized isometric strength and neuromuscular control, traits essential for mitigating G-LOC risk during rapid, high-intensity flight transitions.28,36
Musculoskeletal loading profile
High-G flight imposes a highly specific and non-random musculoskeletal loading profile, directly linked to the anatomical and functional demands of flight operations. 1 These mechanical stressors target critical regions of the body, each playing a distinct role in maintaining pilot performance and safety under gravitational extremes. 1
Cervical spine loading is among the most pronounced. Pilots must stabilize their heads against G-forces while bearing head-supported mass from helmets, night vision goggles (NVGs), and communication systems, often adding 1.5 to 2.5 kg to the head's weight. This augmentation significantly increases cervical torque, especially during high-speed turns and head rotations. Compounding this load are cockpit constraints that force the neck into sustained, often asymmetric postures, such as rotation and extension, under axial + Gz load and vibration. In parallel, effective tolerance to + Gz requires high levels of activation across the lower-limb musculature (in addition to trunk muscle tensing) as part of the AGSM, which further increases whole-body musculoskeletal demand during maneuvering. The cumulative result is an elevated risk for overuse injuries, such as disc degeneration, cervical strain, and long-term mobility impairments, all of which directly undermine mission readiness and flight endurance.37–42
In contrast, the lumbar spine and trunk are subjected to prolonged axial compression while seated in semi-reclined positions. Although seatback angles are designed to reduce spinal loading under G, they inadvertently restrict trunk mobility and require sustained trunk activation for postural stability.14,16,43 Lumbar tensing becomes even more critical during the Anti-G Straining Maneuver (AGSM), where force transmission from the lower body must be stabilized through a rigid trunk to optimize vascular compression and protect the spine.41,44 Chronic tensing under vibration and constraint elevates the risk of lumbar disc injuries, pelvic misalignment, and muscle fatigue, especially in high-flight-hour personnel and multi-aircraft operators. 45
The lower limbs, particularly the gluteals, hamstrings, and quadriceps, function as dynamic countermeasures during AGSM. These muscle groups contract isometrically to compress venous reservoirs in the legs and abdomen, reducing blood pooling and maintaining cerebral perfusion. Functioning as “muscular tourniquets,” they must sustain high-intensity contractions repeatedly, often under extreme fatigue and cognitive load.41,46 Inadequate muscular endurance, particularly in the posterior chain and hip stabilizers, leads to rapid degradation of AGSM performance, diminished G-tolerance, and elevated injury risk, manifesting as hamstring strains, hip asymmetries, or patellofemoral overload. 31
In sum, the musculoskeletal demands of high-G flight are precise, regional, and biomechanically task-aligned (See Figure 1). The cervical spine safeguards sensory and communication capabilities; the trunk serves as the structural anchor for force transmission and posture; and the lower limbs operate as active pumps and vascular controllers. Recognizing this anatomical-functional mapping is essential for developing evidence-based training interventions that elevate operational performance, mitigate injury risk, and prolong career longevity in high-G environments. 1 Although isometric contractions dominate the muscular profile of high-G flight, pilots are not entirely motionless. Tasks such as “check-six” head turns, visual scanning, or reaching movements during flight require dynamic cervical and trunk mobility — often under partial G-load. These maneuvers introduce additional neuromuscular challenges, including rotation under load, rapid repositioning, and reactive control. As such, while isometric training forms the foundation of bracing and endurance, dynamic exercises, particularly those targeting cervical range of motion, thoracic rotation, and hip control, remain essential complements to maintain agility and reduce injury risk during unexpected movement.
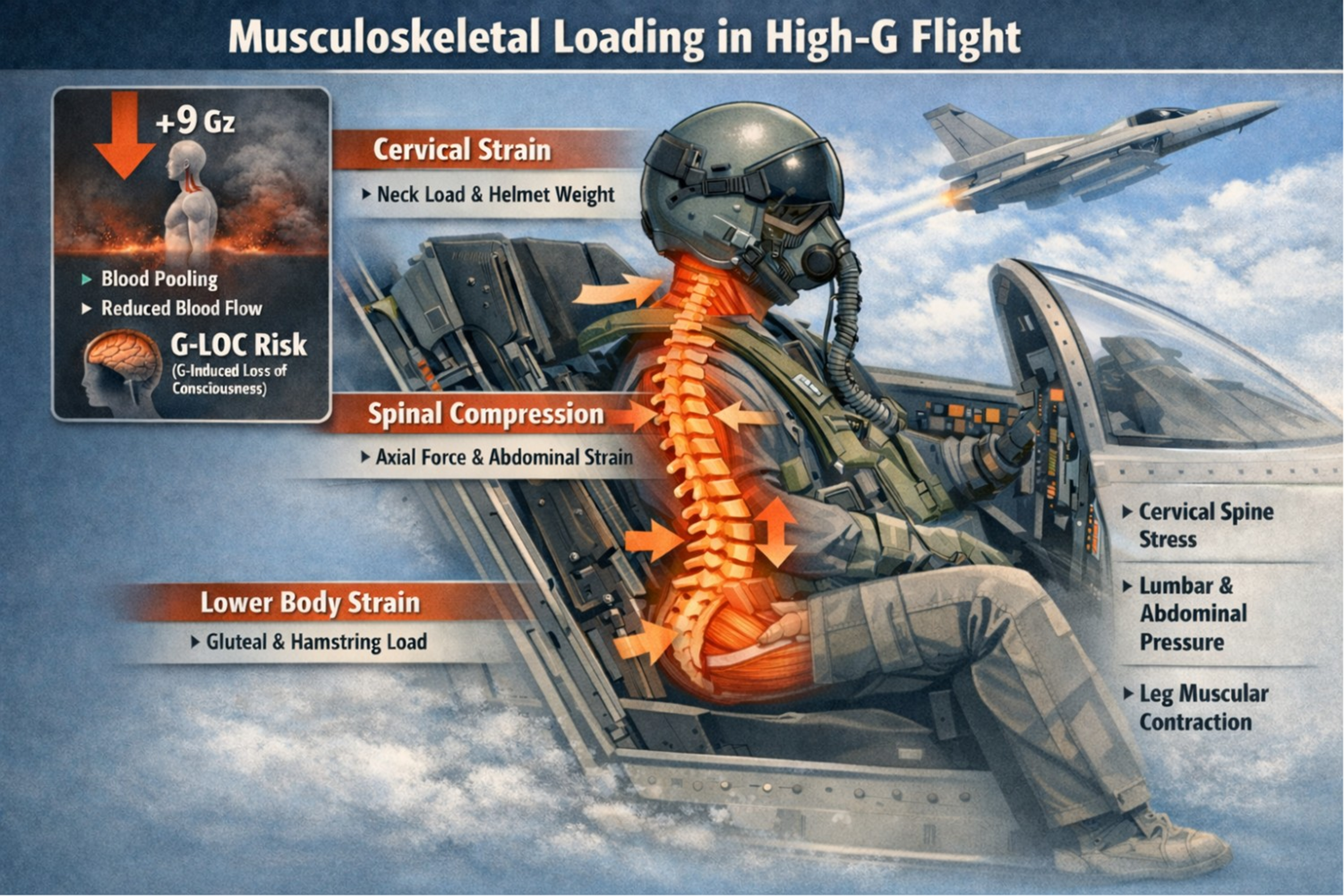
Musculoskeletal loading in high-G flight.
AGSM: isometric demands and training implications
The Anti-G Straining Maneuver (AGSM) remains the cornerstone of physiological defense against G-induced loss of consciousness (G-LOC). Though often described through its respiratory mechanics, AGSM is fundamentally a full-body isometric performance, integrating high-force muscular contractions with precision breathing strategies. 47 Its efficacy is not rooted in dynamic movement but in the rapid initiation and sustained maintenance of isometric tensing throughout each high-G event. 31
At the neuromuscular level, AGSM requires near-maximal co-contraction across multiple muscle groups: the gluteals, quadriceps, hamstrings, abdominals, and spinal stabilizers form a rigid kinetic chain that simultaneously preserves posture and compresses venous reservoirs in the lower body.5,48,49 This vascular compression is essential to minimize blood pooling and maintain cerebral perfusion during elevated Gz loads. Simultaneously, the diaphragm and intercostal muscles coordinate with trunk and pelvic musculature to generate intra-abdominal and thoracic pressures, further supporting brain perfusion by creating a mechanically reinforced pressurized cavity. 49
A central component of the maneuver, the respiratory phase, involves forceful exhalation against a closed glottis (a Valsalva-like technique), which is functionally ineffective without proper musculoskeletal pre-tension.47,50 Without sufficient postural rigidity and pre-contraction, thoracoabdominal pressure dissipates, compromising blood flow stabilization. Thus, AGSM effectiveness hinges not just on technique timing but also on isometric strength, neuromuscular control, and intermuscular coordination. 31
One of the most challenging elements of AGSM is its repeatability under fatigue. Operational flights and combat training often involve multiple high-G onsets, requiring pilots to reproduce AGSM contractions dozens of times per sortie. Neuromuscular fatigue undermines force output, timing precision, and breath-pressure synchronization, factors that cumulatively degrade G-protection and increase the risk of both acute blackout and long-term musculoskeletal injury.5,51
Postural integrity, especially in the lumbo-pelvic region, is a critical yet often overlooked determinant of AGSM success. Weakness, instability, or loss of spinal neutrality under load disrupts the entire kinetic chain, reducing leg compression force, thoracic pressure generation, and increasing spinal shear stress. 1 This may partly explain the high prevalence of low back pain and lumbar degeneration in tactical aircrew. 42 Targeted isometric trunk training, emphasizing anti-extension, anti-rotation, and hip-stabilizing patterns, can help fortify these links and improve both AGSM efficiency and spinal resilience. 9 52–57
Given AGSM's fundamentally isometric nature, traditional dynamic resistance exercises may be insufficient for preparing pilots for real-world in-flight demands. Effective conditioning must replicate the neuromechanical characteristics of AGSM, including fixed-posture tensing, joint-angle specificity, sustained submaximal contraction, and cognitive load integration. 51 Training protocols that incorporate structured isometric holds in AGSM-relevant positions, such as seated tensing, unilateral hip compression, and trunk anti-rotation under load, are more likely to produce transference to flight performance and reduce both acute and chronic injury risk. 42 While AGSM represents a key physiological countermeasure, other isometric demands arise from sustained postural control, particularly due to helmet-mounted systems and cockpit ergonomics. It is important to distinguish AGSM-related isometric efforts—focused on vascular compression and straining sequences, from the more continuous, postural isometric demands imposed by cockpit constraints, head-supported mass, and vibration. These represent parallel but distinct muscular challenges.
Why isometric strength may outperform dynamic strength for high-g tasks
Specificity and neuromuscular control
Training adaptations follow the principle of specificity,19,20 meaning that performance improvements are greatest when the training stimulus closely mirrors the target task.19,20,58 In high-G aviation, most critical motor demands are not dynamic or full-range
Isometric strength training (IST), on the other hand, allows for joint-angle–specific loading, 66 enabling precise targeting of neuromuscular control in flight-relevant positions.3,14,58,61 For example, cervical isometric holds can be performed in the exact rotational angles required during target tracking,11,17,21 and trunk tensing drills can replicate the posture held during AGSM.18,23,32 These positions are rarely addressed in conventional dynamic protocols. 17 Moreover, isometric training enhances motor unit recruitment,3,54 force steadiness, 67 and intermuscular coordination, 68 which are all vital under the unpredictable perturbations of flight.13,67
Fatigue resistance and “usable strength”
Pilots do not need a 1-repetition maximum (1RM) bench press to survive a high-G turn. 23 What they need is “usable strength”, the ability to generate and sustain submaximal force across repeated G-onsets,18,23,69 often while managing task complexity, threat load, and cumulative fatigue. 67 Research suggests that isometric protocols, particularly yielding holds, equally effective as muscle endurance and fatigue resistance than dynamic training alone.13,15,19,20 These benefits directly map onto the requirements of AGSM and postural stabilization.18,52,57
Isometric conditioning may also enhance fatigue resistance during sustained contractions by improving force steadiness and neuromuscular recruitment and by increasing tolerance to metabolite accumulation and other fatigue-related stressors, 70 which may help reduce systemic fatigue71,72 during prolonged or multi-sortie operations.61,73 When muscles contract statically, they maintain tension without the repeated metabolic cost of concentric-eccentric cycles.61,62 For aircrew who must preserve alertness and control across hours of sustained G-exposure, this efficiency becomes operationally meaningful. 67
Translational flight examples
The superiority of isometric strength becomes apparent when analyzing real-world flight tasks.14,67,74 Pilots may spend prolonged periods in constrained cervical postures; however, head movements remain frequent and functionally necessary, including during + Gz exposure, and are performed under elevated axial loading,11,21,75 particularly in rotated or extended positions. 75 This demand is best trained using multi-angle neck isometrics,14,17,76 rather than dynamic neck flexion/extension which rarely mimics cockpit constraints.17,75
During AGSM, the lower body isometrically contracts to compress veins and generate intra-abdominal pressure.1,18,26,77 These contractions involve simultaneous recruitment of the glutes, hamstrings, and quadriceps, 18 not through movement, but through intention-driven, high-tension holds.19,20,54 Wall sits, isometric split stances, and glute bridges performed under duration and load mimic these patterns 78 far better than leg presses or squats alone.23,32
In the trunk, postural integrity is critical to anchor the upper and lower body during flight. 67 This includes resisting extension (e.g., lumbar hyperlordosis under G), lateral flexion (during lateral maneuvers), and rotation (from asymmetric movements). Training with anti-extension (planks), anti-lateral flexion (side holds), and anti-rotation (Pallof holds) develops the multi-planar tensing ability required for real-time flight corrections.
These task examples illustrate that functional readiness in high-G environments is not well-served by conventional dynamic paradigms alone.14,67,74 Isometric strength offers a more biomechanically and neurologically appropriate stimulus for preparing pilots to meet the real-world demands of high-G flight, including stabilization, vascular compression, and repeatability under stress
Overcoming vs yielding isometrics (HIMA vs PIMA)
Definitions (operational)
Isometric muscle actions can be categorized into two functionally and neurologically distinct types: overcoming isometrics (PIMA) and yielding isometrics (HIMA).19,20,61 While both involve no visible joint movement, they differ in intent, neuromuscular activation, and application relevance (see Figure 2).3,13
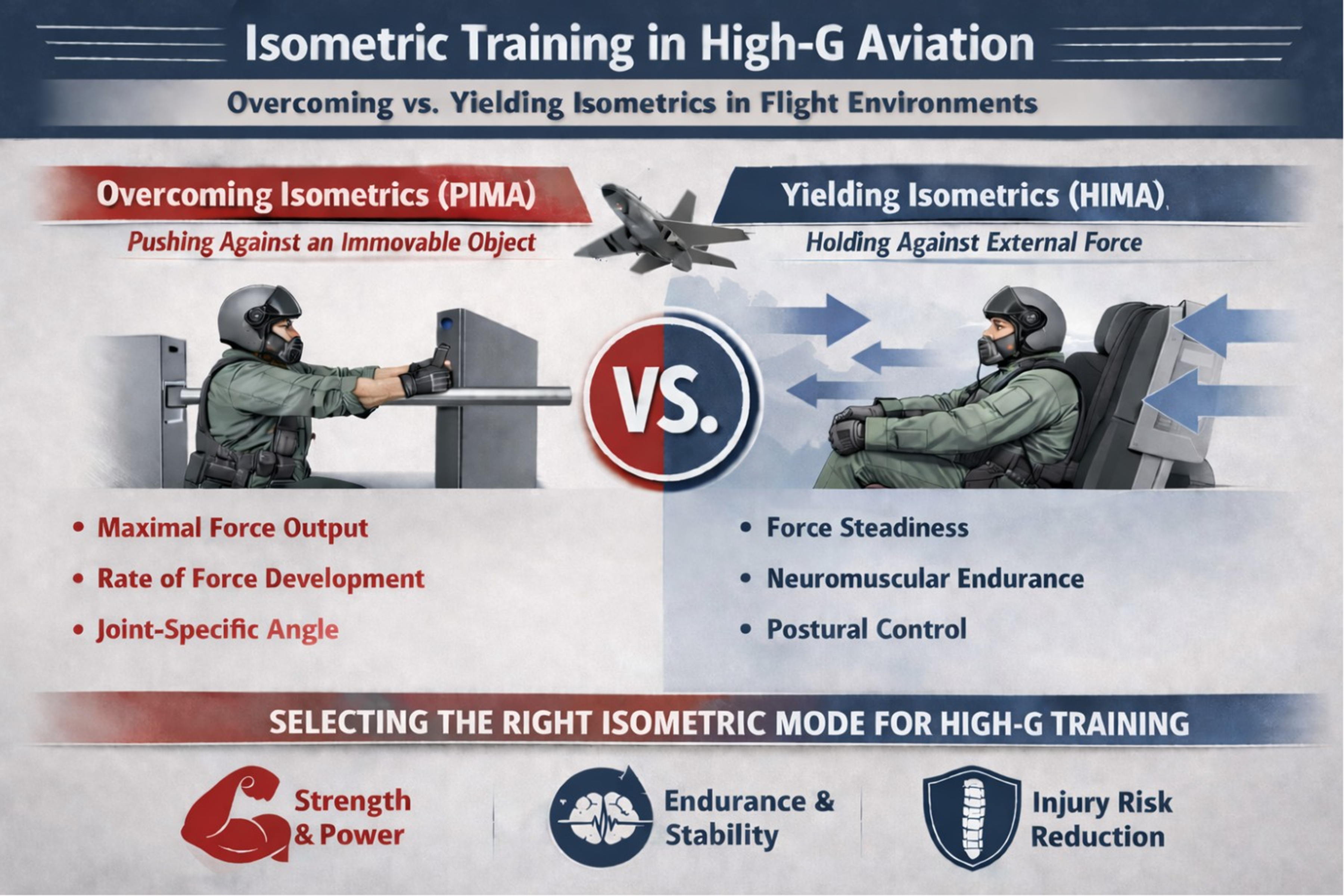
Isometric training in high-G aviation.
Understanding the operational difference between these two is critical for selecting and programming the appropriate isometric mode for flight environments.19,20,61
Why yielding/holding is especially cockpit-relevant
In high-G flight, the human body is subjected to persistent external forces, from gravity, inertia, vibration, and equipment load,1,17,59,60 all of which behave like external vectors trying to displace the pilot's posture.13,19,20 In this environment, the body must resist movement more than it initiates it, placing yielding isometric demands at the center of neuromuscular strategy.19,20,61
For example, the cervical spine must counter the constant pull of the helmet and NVG systems during turns and high-G maneuvers.11,17,21,75 These loads attempt to rotate, extend, or flex the head uncontrollably, and the neck musculature must hold static positions against these external displacements.13,75 This is a textbook yielding isometric scenario, not an overcoming one.13,19,20,61
Similarly, the lumbo-pelvic region and trunk are required to brace against inertial shifts and torso collapse.1,80 During high-G maneuvers, pilots must maintain seated posture, resist spinal flexion, and stabilize the torso, often in asymmetrical or twisted positions. 17 These demands are postural, not propulsive, aligning again with holding-based isometric control.19,20
However, AGSM introduces a hybrid demand.1,59 When pilots execute the AGSM, they perform coordinated tensing of the lower-limb and abdominal musculature (with cyclic breathing), aimed at reducing lower-body blood pooling and augmenting arterial pressure during + Gz exposure, rather than generating force against an external resistance.18,77 The maneuver therefore combines intent to produce force (PIMA) and intent to resist external displacement (HIMA), requiring capacity in both contraction types (see Figure 3).13,19,20
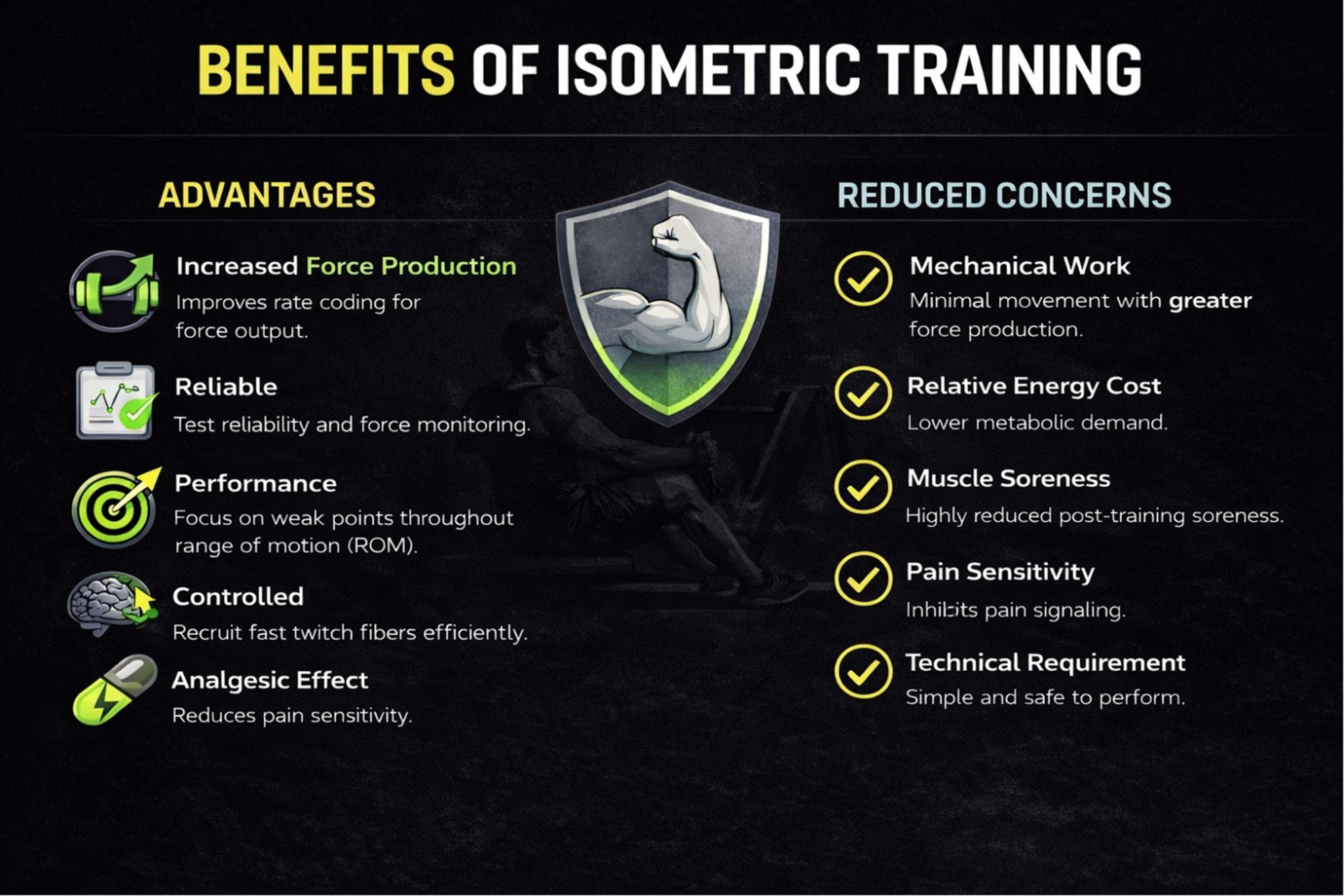
Benefits of isometric training.
Programming implication
Effective high-G conditioning should integrate both overcoming and yielding isometrics, selected based on anatomical region, task demand, and performance goal.1,19,20
Overcoming isometrics, also known as pushing isometrics (PIMA),are most effective for developing maximal force output at specific joint angles.9,13,14,19,20,58 These involve high-intensity contractions against immovable resistance and are typically performed for short durations.9,19,20 Ideal applications include isometric trunk press-outs against fixed surfaces to build tensing capacity,19,20 neck push efforts into resistance using manual pressure or harness-based setups,11,21,55 and AGSM-specific isometric drills where pilots execute maximal full-body tensing combined with controlled breath holds.18,77,80 These targeted efforts help improve neural drive, joint-specific strength, and the capacity to generate high force under pressure,3,14,54,58,74 critical for sustaining posture and pressure during rapid, high-G transitions.1,2,18,67
Yielding isometrics, also known as holding isometrics (HIMA),should form the foundation of training programs designed to enhance postural control, fatigue resistance, and fine motor regulation.13,19,20,67 These exercises involve maintaining positions under load for extended durations19,20,62,78 and are especially effective when applied to key regions such as the neck (with holds in extension or rotation against gravity),11,21,57 the trunk (including planks, side planks, and anti-rotation presses), and the lower body (with wall sits or split-stance holds that simulate AGSM posture and tension).18,78
It's critical that training programs clearly differentiate between yielding and overcoming isometrics.13,19,20,61 Simply prescribing “isometric” work without specifying whether the goal is to hold against load or push maximally against resistance can lead to a disconnect between training outcomes and the actual biomechanical demands of flight.1,19,20,67 By aligning each drill with the appropriate isometric mode, practitioners can significantly improve the effectiveness of training, ensure better transfer to in-flight performance, and enhance long-term resilience in aircrew.3,19,20,52,57
Isometric strength assessment & monitoring
What to assess (pragmatic test menu)
For isometric training to become an operationally viable component of military human performance programs,1,26,5981–84 practitioners must have access to assessment tools that are simple, repeatable,61,81,85 and aligned with the physical demands of high-G flight.1,60 These tests should focus on the anatomical regions most affected during flight operations17,75 and be feasible in both field and garrison settings.11,21,55 Because maximal force can be expressed in distinct ways depending on load and time constraints, assessment should target the specific strength qualities required rather than treating ‘strength’ as a single attribute. 86
For the cervical spine, assessments should capture isometric peak force in flexion, extension, and lateral flexion11,21 using tools like handheld dynamometers or fixed harness systems.11,21,55 Endurance holds, such as maintaining head position against load in rotated or extended postures, can replicate the strain experienced during sustained flight with helmets or NVGs.17,75
Trunk assessments can rely on foundational drills like front planks and side bridges to evaluate basic tensing capacity. Where possible, anti-rotation tasks such as banded Pallof presses or stability-bar holds should be included to simulate the spinal stabilization demands of AGSM.1,18
Lower-limb assessments can incorporate wall-sit endurance as a low-tech yet effective measure of AGSM-relevant muscular contraction.77,78 When resources are allowed, isometric mid-thigh pull (IMTP) testing provides a quantifiable metric of posterior chain force production.61,87–89 Where isometric tests are used as practical alternatives to 1RM-style methods, practitioners should avoid assuming that high correlations imply interchangeability and instead evaluate agreement and context-of-use. 90 Additionally, calf isometric endurance, evaluated through sustained plantarflexion, helps reflect the role of distal vascular compression during high-G exposure.1,2,18,59,91
Together, these tests are easy to administer, scalable across units, and tightly aligned with the specific muscular demands required for maintaining G-tolerance and cockpit posture during operational flying.1,2,61,77,81
Key outcomes
Key outcomes from isometric assessments provide critical insight into both performance capacity and potential risk factors.17,53,89 One of the primary variables is peak isometric force,20,89 typically measured as maximal voluntary contraction (MVC) at a specific joint angle,9,58,92 such as neck extension at 45°,11,20,21 which represents the maximum force available for tensing and stabilization during high-load situations.11,53,67 In applied monitoring contexts, peak force is also one of the most defensible “anchor” outcomes because it repeatedly demonstrates good-to-excellent test–retest reliability when assessed with standardized procedures (e.g., IMTP peak force showing generally high ICCs and low CVs across studies).87,88 Endurance time, measured as the duration, a static hold can be maintained (e.g., wall sit or plank), 78 offers an indicator of fatigue resistance15,62,91 in postural or AGSM-relevant musculature.18,77 Force steadiness, ideally tracked with force sensors or load cells, refers to the consistency of force output during an isometric hold.19,20 Significant variability can point to compromised motor control or early fatigue onset.19,20,91 However, these time-sensitive outputs tend to be less stable than peak force, with greater between-session variability and stronger dependence on protocol factors (e.g., familiarization, warm-up specificity, sampling rate, and joint-position consistency). 88 Practically, this means early-phase force metrics can be informative, but they should only be interpreted as “change” when the observed difference clearly exceeds typical error, and when testing standardization is high. 88 In monitoring systems where force-time data are collected, it is also good practice to report both relative reliability (e.g., ICC) and absolute error (e.g., CV and/or SEM), because absolute error improves individual-level interpretation and readiness decisions.87,88 Additionally, side-to-side asymmetry is a crucial metric, particularly in cervical lateral flexion,11,21 where imbalances greater than 10–15% may elevate injury risk 93 and signal the need for targeted corrective work.20,94 Collectively, these metrics not only reflect current performance but also serve as early indicators of reduced operational readiness or increased vulnerability to injury.17,53,89
Practical instrumentation
To promote widespread implementation, isometric testing protocols must be adaptable across diverse settings, from forward-deployed units to centralized human performance centers.11,20,21 Several scalable tools support this versatility. 61 Handheld dynamometry offers a portable solution for assessing peak cervical and lower-limb force in field conditions.20,95,96 While results can be operator-dependent, handheld dynamometry may not provide accurate estimates during near-maximal contractions, as tester strength and difficulties with stabilization can limit the ability to ‘break’ or resist the participant, thereby constraining recorded force. Where feasible, externally stabilized or fixed dynamometry (or rigid bracing/strapping) should be preferred to improve measurement validity and repeatability.4,20,21,81,87,88 For more precise and standardized assessments, functional electromechanical devices, fixed rigs or force frames, commonly found in unit gyms and rehab facilities, allow multi-planar evaluation of trunk, neck, and lower-limb force output.11,20,21,61,87,88,97,98
Wearables and load sensors, where available, add value by capturing real-time data on force steadiness, rate of force development (RFD), 99 and compensatory movement patterns during isometric holds.20,89,100 Newer wireless models have made this technology more accessible, even in austere environments.11,20 Monitoring should occur at decision points to guide prescription and readiness: baseline (screening and load-setting), mid-block (∼4–6 weeks) (progression adjustment), post-block (∼8–12 weeks) (training response/readiness), and periodic or symptom-triggered reassessment during routine flight-readiness checks.11,19–21,56,100,101
Why assessment matters
Isometric assessment 85 plays a vital role in bridging the gap between physical preparation and operational performance in aviation.1,67,89 It allows for individualized training prescriptions, 100 enabling pilots with neck or abdominal imbalances, low force endurance, or diminished tensing ability to receive tailored protocols,15,17 specific to their needs in terms of hold types, joint angles, or durations.9,58 Beyond training design, it supports readiness monitoring by detecting early signs of overtraining, cumulative fatigue, or inadequate recovery,21,102 often before such issues begin affecting in-flight performance. 67
This type of assessment also serves as a key tool for injury-risk mitigation, particularly in the cervical spine,11,17,21 which is highly susceptible to strain due to repetitive loading and asymmetrical equipment weight.17,75 Identifying early signs of weakness or imbalance provides the basis for injury risk reduction.11,17,103,104 In high-G aviation, where failure to maintain posture or pressure can compromise both consciousness and mission outcomes,1,2,80 having clear, quantifiable isometric performance metrics is critical.11,21,89 These assessments convert generalized strength goals into actionable, repeatable indicators that directly enhance both human performance and flight safety.67,81,89
Training recommendations: high-G oriented isometric protocols
Isometric strength is a trainable, position-specific quality,9,14,58,61 and when targeted correctly, it supports both AGSM effectiveness1,2,18,80 and postural resilience under high-G load.11,17,75 The protocols below are structured by anatomical region17,18 and emphasize efficiency,9,63,78 transfer to flight tasks,17,18,58,61 and minimal equipment dependence.16,20,55 These exercises can be easily embedded within aircrew strength programs55,105 or pre-deployment training. 106 The cervical spine faces continuous isometric loading distinct from AGSM, requiring separate analysis and training considerations.
Neck and head-supported mass: postural load and injury risk
Pilots are required to stabilize their heads against complex, multidirectional forces generated by G-loading,11,75 helmet and NVG weight, 17 and asymmetric cockpit movements. Training should replicate these demands by targeting all primary planes of cervical motion.11,17,21 This includes progressive isometric holds in flexion and extension, such as chin tuck holds or resisted neck press-backs11,21; lateral flexion using ear-to-shoulder holds with resistance bands or manual pressure11,21,55; and rotation holds at 45°–60° angles to simulate the head-turning actions commonly used in flight.
A well-rounded program incorporates both yielding holds, sustained contractions of 20–40 s under light to moderate load to build endurance and postural control under G,13,17,19 and overcoming efforts, which involve maximal intent holds of 3–5 s against an immovable surface like a wall or harness to train force production.9,19,20,55 These strategies closely mirror real-world G-maneuvering demands such as head-on-swivel tracking, and they help mitigate neck fatigue, a major contributor to in-flight injury risk.11,17,21,55,107
Trunk and lumbar loading during high-G flight
The trunk serves as a critical tensing structure during AGSM, helping maintain spinal alignment and transmit force effectively under load.1,2,18,77 Isometric trunk training should prioritize resisting undesired motion rather than producing movement.13,19,20,61 Effective programming includes anti-extension drills such as standard and weighted planks 13 to counter lumbar hyperextension during G-loading 80 ; anti-lateral flexion exercises like side bridge holds, which prepare the body to maintain posture in twisted or tilted flight positions; and anti-rotation drills such as Pallof holds, resistance band or cable holds, and medicine ball stabilization, all of which mimic the need to resist torsional forces experienced in the cockpit. 17
Key coaching cues focus on maintaining postural integrity, ensuring a neutral spine, activated glutes, and engaged abdominals throughout each hold. 18 Controlled breathing patterns should be integrated during these exercises to simulate the coordination required during AGSM,18,80 without placing excessive focus on the ventilatory mechanics themselves. This strategy enhances both postural control and the body's ability to transmit force through the spine during high G-force exposures1,2 and other high-pressure operational maneuvers.59,60
Lower limb role in AGSM and G-tolerance
The lower limbs are essential to effective AGSM performance, playing a key role in both venous compression and trunk stabilization.1,2,59,77,108 Isometric exercises should mirror the tensing patterns used during straining maneuvers to build targeted strength and endurance.18,77 Recommended drills include wall sits at a 60–90° knee angle,78,92,109 beginning with 30–60 s holds62,110 and progressing to weighted or extended-duration holds; split-stance lunge holds to encourage gluteal and hamstring co-contraction that aligns with AGSM posture18,92; and calf holds using standing plantarflexion isometrics,111,112 either bodyweight or loaded,56,91 with bent-knee variations to specifically train the soleus for endurance. A crucial element of these drills is the integration of AGSM-style breathing,1,2,18,59 such as tensing on the inhale and holding a partial exhale, which transforms each drill into both a strength and motor control exercise. 18 This method enhances vascular compression capacity and helps maintain AGSM performance under fatigue conditions.59,108
Frequency and integration
The objective isn’t to increase overall training time, but to apply precise isometric stimuli that directly correspond to operational needs.19,20,63 A low-dose, high-impact approach is the most sustainable model.63,78,113 Performing isometric sessions two 101 to three times per week9,14,114 is sufficient when drills are both intense and position-specific. These sessions can be organized by targeting different regions across the week, 20 such as neck work on one day, trunk on another, and lower limb on a third, or adapted to fit around flight schedules. Each session requires only 10 to 15 min of focused effort to produce meaningful neuromuscular adaptations.9,55,78 These blocks can be scheduled after main training19,20 or used as short micro-sessions before or after flying, as long as fatigue before sorties is avoided.9,20 This structure supports progressive overload and neuromuscular readiness while minimizing interference with flight operations or broader training programs.20,89 Much like the execution of AGSM itself, the key to effectiveness lies in consistency and control, not in training volume alone.18,63
Implementation challenges and operational solutions
Despite strong physiological rationale,1,2,9,59 isometric training often faces adherence and integration barriers in operational settings.52,55,63,78 These challenges are not primarily technical, they are cultural, perceptual, and logistical.16,55 If isometric protocols are to support high-G readiness across units,1,2,17,80 they must be presented not just as effective, but as practical, efficient,16,55,63,78 and directly mission-linked.1,2
Barrier: “static is boring”+knowledge gaps + time + equipment constraints
Among both aircrew and strength professionals, there is a widespread perception that isometric training lacks the intensity or variety of more dynamic methods. 17 When compared to activities like heavy lifting or high-tempo conditioning, holding static positions can appear unchallenging or even unproductive,19,20 particularly if users are unaware of the neuromuscular depth and operational relevance these holds offer.19,20,67 This perception is compounded by several systemic challenges: limited time for strength development during high-tempo operations or flight-heavy schedules,55,63,78 restricted access to specialized equipment such as fixed rigs, force plates, or neck-specific training tools,11,16,19,20,55 and a prevailing training culture that prioritizes movement volume and visible outputs, such as reps and weights, over internal tension control or positional endurance.19,20,115 Without a deliberate shift in both education and program design, isometric training risks being marginalized as an optional or filler activity,17,19,20 rather than recognized as a mission-critical tool for strength, control, and resilience.11,17,67
Solutions
Micro-sessions (10–12 minutes max)
Isometric protocols are effective even when kept brief, requiring neither high volume nor long duration.9,63,78 A focused “short micro-sessions (≈15–20 min) or very brief high-intensity blocks19,20,55,78 that targets two to three regions with two sets per exercise19,20,101 can yield measurable adaptations when done two to three times per week.14,56,101,114 This efficiency makes isometric training particularly well-suited for low-load recovery days,9,73 post-exposure / recovery days,9,102 and weeks when time is limited but maintenance work is still needed.20,63
Minimal equipment requirement
Most isometric drills can be executed using just bodyweight, resistance bands, 116 or resistance provided by a wall, floor, or training partner.19,20,55,61 This versatility makes it easy to incorporate these exercises into settings like flight line gyms, hotel rooms, or austere environments.11,16,55 For instance, wall sits or split-stance holds require no equipment at all 78 ; neck holds can be performed using bands, towels, or manual resistance17,55; and trunk anti-rotation drills only need a loop band or a stable anchor point.19,20,61 This approach reduces logistical barriers while promoting regular exposure and consistency in training.16,20,63
Embed in warm-ups or post-flight “reset” routines
Instead of treating isometric exercises as standalone workouts, they can be integrated into movement preparation routines, such as performing neck holds before flying or training sessions, and used as post-flight resets to restore positional stability following long-duration sorties. Notably, elements of this approach (e.g., targeted neck and trunk strengthening and pre-flight preparation strategies) are already incorporated within some aircrew conditioning programmes; however, the specific inclusion and dosing of isometric protocols varies by service and unit.20,55,61,102 Embedding them in this way makes the practice more habitual and accessible,52,55 promoting consistent use and allowing cumulative adaptation to develop over time.20,56,101
Use simple metrics to drive adherence
While high-tech instrumentation can be beneficial, it isn't essential.11,20 Consistency and engagement are often enhanced through simple feedback loops11,20 such as tracking hold time with progressive targets,15,62,78 noting rate of perceived exertion (RPE) at the end of a hold,21,102 and making side-to-side comparisons to identify and monitor asymmetries, particularly in the neck.11,21 These straightforward metrics are easy to record, repeat, and communicate to operators,11,21,78 helping maintain a clear focus on practical relevance and ongoing progression.20,89
Explicitly tie exercises to flight tasks
Adherence improves significantly when the relevance of each task is clearly understood. 52 Every isometric drill should be directly connected to a specific cockpit or Anti-G Straining Maneuver (AGSM) performance requirement,17,19 for example, a neck lateral hold simulates resisting helmet pull during night turns,17,75 a wall sit mirrors the lower limb compression experienced during AGSM,18,78 and a side plank helps brace the spine against torque during G-turns.13,19 When personnel recognize the operational purpose of a drill, especially in terms of in-flight survival or mission effectiveness, they are more likely to approach it with intent and focus. 19
Ultimately, the primary obstacle to implementing isometric training isn't complexity, it's perception.17,19,20 By reducing friction in terms of time and equipment,16,20,63 clarifying each drill's purpose, and embedding isometrics within existing training routines,20,55 units can effectively integrate static strength work in a way that mirrors real-world pilot demands.17,18,75 With minimal adjustments, isometric training can shift from theoretical recommendation to practical application, enhancing both performance and injury resilience. However, well-controlled studies are still needed to determine whether these implementation strategies translate into measurable operational benefits (e.g., improved + Gz tolerance/AGSM effectiveness, reduced G-LOC incidence, lower neck pain burden, fewer duty limitations, and improved sortie endurance) in real-world aircrew contexts.11,17,20,55,67,78
Research gaps and future directions
As the operational relevance of isometric strength training gains traction, several critical evidence gaps remain.11,17 These must be addressed to transition from conceptual endorsement to full-scale integration within military aviation systems.17,55 The following areas represent high-priority targets for future research, 17 with direct implications for flight safety, injury prevention, and performance sustainment.1,2,17
Normative data gaps
Although the cervical and lumbar spine play a central role in pilot biomechanics, 80 there remains a lack of normative isometric strength profiles for aircrew across different aircraft platforms.11,17,21 Research is required to establish reference ranges for cervical flexion, extension, and lateral flexion strength and endurance,11,21 considering variables such as aircraft type, whether fixed-wing fast jet, rotary-wing, or transport,17,57 along with helmet and night vision goggle (NVG) configuration and weight,11,17,21 and total flight hours to capture trends related to cumulative loading and fatigue. 80 Comparable data collection for lumbar and trunk endurance is also necessary, 80 particularly in seated or rotated positions that reflect the constraints of cockpit environments. 17 Such data would support more effective individualized load management,11,21 enhance return-to-fly decision-making, and facilitate early detection of strength decline that could signal a higher risk of injury.11,17,53
Best-Dose uncertainty
There is little consensus on the optimal isometric dosing parameters for high-G environments.19,20,73,78 Key questions remain unanswered: (1) What is the ideal balance between overcoming and yielding isometrics for specific mission profiles?13,19 (2) How should programs emphasize endurance versus peak force, particularly in AGSM-related muscle groups?18,54,62 (3) Is joint-angle specificity more critical in the cervical spine than in the lower limbs?11,14,58,74 (4) What are the minimal effective doses for isometric maintenance during high-tempo flight periods?19,63
Answering these questions requires controlled trials, ideally embedded in flight training pipelines or squadron readiness programs, to capture both short-term adaptation and long-term retention.18,78,80
Prospective injury outcomes
While preliminary studies and narrative evidence suggest that isometric strength training may reduce the incidence of neck and lower back pain,17,55,57,80 high-quality prospective cohort data are lacking.17,53 and clinical tendinopathy evidence does not show blanket superiority of isometrics. 117 Needed studies include: (1) Longitudinal tracking of injury incidence (especially cervical strain and lumbar overuse) in pilots participating in structured isometric training programs versus standard care17,55; (2) Identification of protective thresholds (e.g., neck lateral flexion asymmetry <10%, trunk hold time >60 s) that correlate with lower injury rates11,21,53; (3) Cost-benefit analyses comparing isometric-focused training models to more conventional dynamic-only programs in terms of both injury burden and flight downtime.16,63 Such evidence would provide command-level justification for integrating isometric strategies into standard pre-deployment conditioning.1,2,17
Tool development and integration
Even when training value is understood, the lack of accessible and field-ready measurement tools can hinder adoption.11,21 To enable scalable assessment and feedback loops: (1) There is a need for portable, low-cost, and validated dynamometry solutions, particularly for neck and trunk isometrics,11,19–21 that can be used in unit gyms or deployed environments11,16; (2) These tools should be compatible with existing human performance ecosystems, 118 allowing integration with wearable data, digital logs, and pre/post-flight assessments11,20,100; (3) Development should prioritize repeatability, minimal user bias, and rapid setup, so they can be used by non-specialist personnel with brief familiarization.11,20,21
Embedding such tools into pre-flight screens, return-to-fly assessments, and longitudinal monitoring11,21 would improve not only performance outcomes, but also mission assurance and resource optimization.1,67 In summary, the case for isometric training in military aviation is mechanically and operationally sound,1,9,17,58 but the supporting science must evolve to match its potential.17,73 Addressing the above research gaps will allow the field to move from expert-informed practice to evidence-based doctrine,17,20 advancing both human protection and performance at high G.1,2,11,17
Conclusion
Isometric strength training (IST) aligns precisely with the neuromuscular demands of high-G flight. In contrast to traditional strength models focused on movement through ranges of motion, the high-G environment requires pilots to maintain postural integrity and resist displacement while under external load, a scenario where muscular tensing and joint stabilization are paramount. Whether resisting helmet-induced torque on the cervical spine or generating intramuscular pressure during AGSM, isometric contractions are the dominant mode of effort. Their joint-angle specificity, task relevance, and low fatigue cost make them not only effective, but also efficient in high-tempo flight environments where training time is constrained.
To realize their full potential, isometric protocols must be formally integrated across the training continuum, from accession schools through operational squadrons. Programs should include both overcoming and yielding contractions, target multiple planes of motion, and reflect flight-specific postures such as neck extension under NVG load or trunk tensing during AGSM. Importantly, these protocols are measurable, allowing for individual baselines, asymmetry tracking, and progression monitoring using accessible tools like handheld dynamometry, force sensors, or even hold-time benchmarks. Units can implement short-duration blocks (10–15 min), embedded within warm-ups or post-flight resets, without disrupting flight operations or broader physical training cycles.
The operational benefit of such integration is clear: a triad of enhanced G-tolerance, reduced in-flight fatigue, and lower rates of chronic musculoskeletal strain, especially in high-risk regions like the neck and lumbar spine. Isometric strength is not a niche intervention, it is a scalable, evidence-aligned countermeasure to one of the defining physical threats in tactical aviation. As mission demands grow more complex and pilot career longevity becomes a strategic asset, IST offers a low-cost, high-return method to fortify human performance under gravity.
Footnotes
Abbreviation list
Ethical considerations
This narrative review did not involve the collection of new data from human participants or animals, and therefore formal ethical approval was not required in accordance with prevailing standards for secondary research of this type.
Consent to participate
Not applicable. This article is a narrative review and did not include any primary data collection involving human participants or animals requiring consent to participate.
Consent for publication
Not applicable. No individual person's data (including individual details, images, or videos) are reported in this article that would require specific consent for publication.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
No new data were generated or analysed in this narrative review. All supporting information is derived from previously published studies cited in the reference list, which are available through the original publishers or databases.