
Abstract
This article introduces the revised Athlete Sleep Behavior Questionnaire (ASBQ-2), refining the original ASBQ to better assess athlete sleep behaviors. Updates were based on expert consensus and new research evidence, and address factors like late naps, caffeine use, nighttime training, sleep medication, and electronic device use. Contextual factors, including travel, household disruptions, and large pre-bed meals, were incorporated. The ASBQ-2 maintains its original scoring while merging or removing minimally impactful items, resulting in an 18-item practical assessment tool. These enhancements improve the questionnaire's ability to identify maladaptive sleep behaviors, supporting targeted interventions to optimize recovery, performance, and well-being in athletes, a group prone to sleep challenges.
Introduction
Sleep is a critical factor in athletic performance, recovery, and overall well-being, yet athletes are particularly susceptible to poor sleep. 1 We originally proposed the Athlete Sleep Behavior Questionnaire (ASBQ) in 2018, 2 with the purpose of identifying maladaptive sleep behaviors contributing to poor sleep among athletes. The widespread uptake and use of the ASBQ in both research and practical settings highlight the need for such a tool. At the time of writing this article, the ASBQ has been translated to multiple other languages, including; French, 3 Japanese,4,5 Portuguese, 6 Arabic, 7 Turkish, 8 Persian, 9 and Korean. 10 Previous work has confirmed the reliability of the ASBQ, via a meta-analysis of Cronbach's alpha and intraclass correlation coefficients. 11 A reliability generalization meta-analysis of studies from 10 databases demonstrated good internal consistency (Cronbach's alpha = 0.73; 95% CI: 0.63–0.80), and excellent test–retest reliability (ICC = 0.88; 95% CI: 0.87–0.89) with no significant heterogeneity. Perhaps more importantly, given the ASBQ was originally proposed as a practical assessment tool, rather than a clinical screening questionnaire, practitioners around the world have reported using it across many different settings, from development/youth through to professional/elite athletes. In these settings, practitioners have reported using it to identify poor behaviours (as identified by athletes responding “sometimes”, “frequently”, or “always” to any of the items) and subsequently, designing interventions to address those issues. However, given the rapid advancements in sleep science and emerging research on sleep behaviors, especially in sport and athletes, several updates were warranted to improve the questionnaire's accuracy, comprehensiveness, and relevance. New research findings have deemed some items of the original ASBQ to be either irrelevant, or inaccurate, prompting the need for an update. This article outlines key changes made to the ASBQ in the proposal of a revised version, the ASBQ-2 (Table 1), and provides evidence-based justification for each modification. The ASBQ-2 is primarily designed as a practical assessment tool rather than a research-intensive or clinical measurement instrument, and given the ASBQ-2 is the refinement of the ASBQ, its core principles and constructs have already been assessed for validity and reliability. Therefore, we propose that the modifications do not warrant an entirely new validation process, and the tool retains its fundamental purpose and structure.
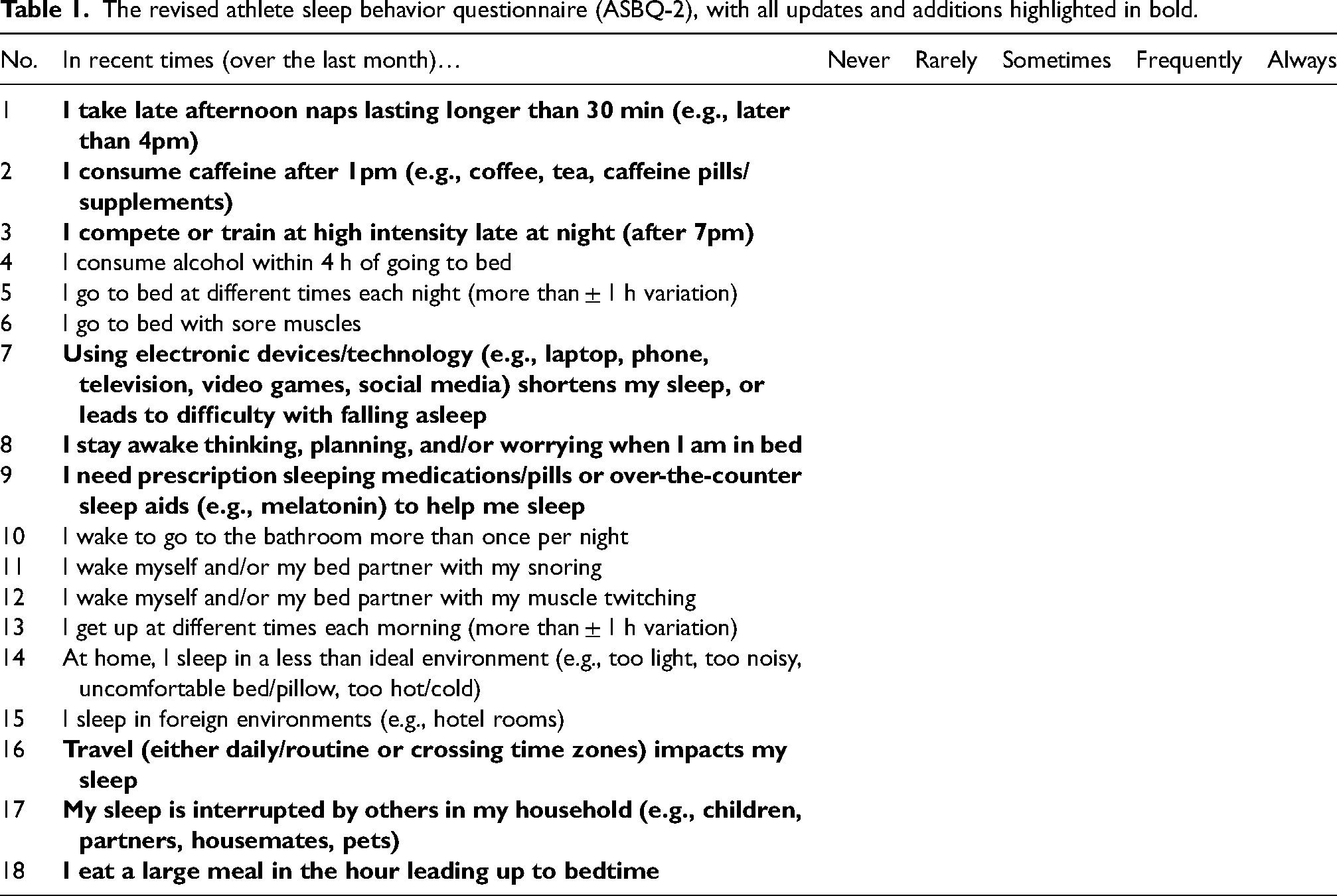
The revised athlete sleep behavior questionnaire (ASBQ-2), with all updates and additions highlighted in bold.
Enhancing specificity: refining existing questions
Late afternoon naps (question 1)
Original: “I take afternoon naps lasting two or more hours”
Updated: “I take late afternoon naps lasting longer than 30 min (e.g., later than 4pm)”
When performed appropriately, napping is a commonly used, and effective tool for athletes.12,13 However, this change in wording recognizes the potential negative circadian impact of late-day naps. In a systematic review by Lastella et al. 14 of 37 studies, the main recommendations were that athletes consider napping for 20–90 min, between 13 : 00 and 16 : 00 h. Recent research has suggested that when naps (even lasting up to 90 min) are completed before 15 : 00, they are unlikely to have a negative impact on subsequent nighttime sleep. 15 In contrast, when naps are completed too late in the day, it may come at the cost of quality nighttime sleep. Mograss et al. (2021) tracked 62 healthy young adults using 7–14 days of wrist-actigraphy and sleep diaries to compare the impact of “early ( > 7 h before bedtime)” versus “late ( < 7 h before bedtime)” daytime naps on nocturnal sleep. 16 The study found that naps taken closer to bedtime significantly increased sleep fragmentation, sleep-onset latency, and wake-after-sleep-onset compared to earlier naps. Therefore, by specifying a time cut-off, the revised question aims to capture behavior more likely to affect sleep outcomes. In the original questionnaire, where no time of day was specified, there was potential that athletes were taking naps early in the day (e.g., before 1pm) without having a negative impact on nighttime sleep.
Caffeine timing (question 2)
Original: “I use stimulants when I train/compete (e.g., caffeine)”
Updated: “I consume caffeine after 1pm (e.g., coffee, tea, caffeine pills/supplements)”
Emerging research highlights that caffeine consumed later in the day, even as little as one cup of coffee after 1 pm, can delay sleep onset and reduce total sleep time. 17 A recent systematic review and meta-analysis of 24 studies suggested that ∼100 mg of caffeine (∼250 mL coffee) should be consumed at least 8.8 h before bedtime to avoid total sleep time reductions. 17 This update ensures the questionnaire reflects caffeine's half-life and its potential to interfere with nighttime sleep, particularly when consumed in the early afternoon or later. The mention of “stimulants” has been removed due to the wide range of substances athletes may take, each with varying impacts on sleep. Additionally, the reference to pre-workout supplements as an example was removed, as their stimulant ingredients can vary widely, making them less suitable for generalized inclusion in the questionnaire.
Exercise timing and intensity (question 3)
Original: “I exercise (train or compete) late at night (after 7pm)”
Updated: “I compete or train at high intensity late at night (after 7pm)”
The original question was modified to emphasize high-intensity evening exercise, especially competition, is more likely to affect sleep onset. Studies have shown that low-to-moderate evening exercise does not significantly impair sleep, 18 but high-intensity training or night time competition might have a negative impact on sleep.19,20 Further, a recent, large-scale study of 14,689 adults across 4,084,354 person-nights, revealed that high-strain exercise bouts ending within 2 h of sleep, (e.g., often after 7 pm), delayed sleep onset, reduced total sleep time, worsened sleep quality, raised nocturnal resting heart rate, and lowered heart rate variability. 21 Therefore, the update to this question captures the “intensity” of the exercise, which may be a key factor in sleep disruption and impaired athlete recovery.
Electronic device use (question 7)
Original: “I use light-emitting technology in the hour leading up to bedtime (e.g., laptop, phone, television, video games).”
Updated: “Using electronic devices/technology (e.g., laptop, phone, television, video games, social media) shortens my sleep or leads to difficulty with falling asleep.”
The update to this question reflects the somewhat conflicting research on the impact of screen light exposure on sleep, and instead includes the impact of cognitive and psychological stimulation through device use, which may ultimately reduce the time window available for sleep.22,23 Studies highlight that device-related cognitive and physiological arousal, such as engaging content, notifications, and social media use, can exacerbate sleep problems or encroach on the time available for sleep. 24 For example, in a survey of over 45,000 young adults, each extra hour of in-bed smartphone scrolling was associated with 24 min less sleep. 25 This revision integrates emerging findings that both screen light and content-driven stimulation may contribute to sleep disturbances. 24 By expanding the question to include “shortened sleep” and “difficulty with falling asleep,” the revision captures a broader scope of device-related risks, ensuring comprehensive assessment.
Combining psychological arousal questions (question 8)
Original(s): “I think, plan, and worry about my sporting performance when I am in bed” and “I think, plan and worry about issues not related to my sport when I am in bed”
Updated: “I stay awake thinking, planning, and/or worrying when I am in bed”
The update combines both sport-related and non-sport-related worries into a single question to reduce redundancy and simplify the questionnaire. Research highlights that general cognitive arousal, regardless of the source, is a key factor delaying sleep onset and reducing sleep quality. 26
Clarifying the use of sleeping aids (question 9)
Original: “I use sleeping pills/tablets to help me sleep.”
Updated: “I need prescription sleeping medications/pills or over-the-counter sleep aids (e.g., melatonin) to help me sleep.”
The revised wording includes prescription sleep aids (e.g., benzodiazepines) as well as over-the-counter sleep aids (e.g., melatonin), which have different mechanisms and risks. If used regularly, both may lead to dependence, next-day drowsiness, or impaired performance. 27
Recognizing contextual and environmental factors (question 16)
Original: “Travel gets in the way of building a consistent sleep-wake routine.”
Updated: “Travel (either daily/routine or crossing time zones) impacts my sleep.”
This revision broadens the scope to include not only disruptions to the sleep-wake routine but also other travel-related sleep issues, such as jet lag, unfamiliar sleeping environments, and altered schedules. 1 The revised question ensures a comprehensive assessment of how travel impacts athletes’ sleep, which can include either daily travel routines (e.g., to and from training), or when crossing time-zones.
We have also removed one question from the original ASBQ, which read: “I go to bed feeling thirsty”. Subjective thirst ratings show poor concordance with objective markers (e.g., urine specific gravity or osmolality), 28 and in a 24-h fluid-restriction trial inducing ∼1–2% body-mass loss, mild hypohydration paradoxically increased total sleep duration by ∼1 h even as it impaired ease of sleep onset, 29 illustrating the complex, and sometimes counterintuitive, relationship between hydration status and sleep. Further, a study by Arnaoutis et al. 30 found no significant differences in sleep parameters between dehydrated and euhydrated states in young healthy adults, thus undermining the utility of a standalone ‘I go to bed feeling thirsty’ item in the ASBQ.
Expanding sleep-related constructs
Disruptions from others (question 17)
New Item: “My sleep is interrupted by others in my household (e.g., children, partners, housemates, pets).”
Household-related sleep disturbances are a common but often overlooked factor affecting sleep quality in athletes. Studies have shown that sleep fragmentation, caused by children waking up at night, 31 partner movements and chronotypes, 32 or even pet disruptions, 33 can lead to reduced sleep quality. Including this item allows practitioners to identify and address external disruptions, helping tailor interventions for better sleep hygiene and recovery strategies.
Large meals before bed (question 18)
New Item: “I eat a large meal in the hour leading up to bedtime.”
Recent work has shown that meal-to-bed timing profoundly influences sleep. A 2024 cross-sectional study of young adults found that eating within 1 h of bedtime was linked to subclinical sleep disturbances, namely lower sleep efficiency and greater wake after sleep onset, compared to those who abstained for longer before lights-out. 34 Furthermore, Crispim et al. (2011) studied 52 healthy adults using 3-day food diaries and overnight polysomnography and found that greater caloric intake in the hours before bedtime was associated with reduced sleep efficiency, longer sleep and REM latency, and increased wake after sleep onset, highlighting the direct impact of late-night eating on sleep architecture. 35 This new item ensures that a potential contributor to sleep disturbances is considered in the questionnaire, particularly for athletes with varying dietary habits.
Implications for scoring and intervention
The revised questionnaire retains the original ASBQ scoring system, assigning values from 1 (never) to 5 (always) for each item. The ASBQ-2 introduces two new questions (Q17 and Q18), removes one item, and combines two into a single item (Q8), resulting in an 18-item structure. Therefore, the ASBQ-2 is still 18 items, and we suggest that the global score thresholds can still be maintained. As with the original ASBQ, < 36 would equate to “good sleep behavior” and ≥ 42 = “poor sleep behavior”. These thresholds were based on the authors’ interpretation of the data and represent a conservative assessment of threshold range descriptors. The lower threshold of ≤ 36 represents an average response of “rarely” for all 18-items, while the upper threshold of ≥ 42 would require more than one response of either “sometimes”, “frequently” or “always”. However, as suggested in the original ASBQ, these thresholds are suggested as a guide only, and future work should validate these thresholds by triangulating with both subjective (e.g., PSQI) and objective (e.g., actigraphy or PSG) sleep measures. Further, thresholds and normative values may need to be assessed in future studies to establish benchmarks in different cohorts (e.g., amateur vs. professional athletes, youth vs. adult athletes).
Suggested use and guidelines
Practitioners can leverage the ASBQ not only as an assessment tool but as a roadmap for targeted, behaviour-change interventions. Each item represents a modifiable habit; whenever an athlete responds “sometimes (3),” “frequently (4),” or “always (5),” that domain should become the focus of discussion and action planning. For example:
If late-day caffeine use is common, work with the athlete to shift caffeinated beverages/supplements to the morning or early afternoon, substitute with decaffeinated alternatives, or introduce gradual tapering (e.g., reduce consumption) to minimise sleep-disrupting stimulant effects.
If an athlete indicates irregular or shifting bed- and wake-times, work with them to establish a fixed sleep–wake schedule, setting consistent lights-out and rise times (even on weekends), using morning bright-light exposure to anchor circadian timing, and employing pre-bed wind-down rituals to reinforce regularity.
When frequent bedtime muscle soreness is reported, practitioners may introduce targeted recovery modalities, such as hydrotherapy techniques (e.g., cold/contrast water immersion), or the use of compression garments, to reduce nociception and facilitate a more comfortable transition to sleep.
For athletes who describe suboptimal bedroom conditions, optimise the environment by maintaining a cool (∼18 °C), dark, and quiet space. Install blackout curtains, use eye masks, ear plugs, and ensure bedding and mattress support individual comfort and thermoregulation.
By mapping each elevated item to a specific, evidence-based behaviour change, and revisiting the ASBQ-2 periodically, practitioners can track progress, reinforce positive habits, and continuously optimise sleep health for enhanced recovery and performance.
Conclusion
The revised Athlete Sleep Behavior Questionnaire (ASBQ-2) enhances the original by incorporating recent sleep research and refining key areas like napping, caffeine use, sleeping pills, exercise timing, technology use, household disruptions, and diet. It offers a more comprehensive, user-friendly tool for identifying and addressing sleep issues in athletes, supporting recovery and performance. Prioritising practicality and efficiency, ASBQ-2 emphasizes usability and decision-making support over strict psychometric properties.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.