
Abstract
This study primarily aims to establish current practices to tailor support for female athletes, including menstrual cycle tracking, health screening, female-specific education, and other practical supports to address concerns related to menstruation. A secondary aim was to explore the relationships between the participant characteristics and practices implemented to tailor support for female athletes. One hundred and forty-one practitioners (i.e., coaches, athletic trainers, high performance managers) working with female athletes responded to an online survey between March and December 2023. Frequency analyses demonstrated that it is more common for practitioners to avoid discussing menstrual cycle tracking with athletes than to either encourage or require them to undertake tracking. Tracking was most often undertaken to establish and identify changes to athletes’ usual menstrual characteristics, and to identify and manage menstrual symptoms. In terms of health screening, disordered eating and iron deficiency were screened for most commonly, while screening for pelvic floor dysfunction was least common. Female-specific nutrition, relative energy deficiency, and menstrual cycles were the topics most commonly included in female athlete-specific education targeted at athletes and practitioners. Further analysis revealed that respondents’ tracking and education practices were closely associated. This study provides a snapshot into the practices that are currently implemented to tailor support to female athletes around their menstrual cycle.
Keywords
Introduction
A criticism of the current sport science evidence-base is that with the limited representation of female and women participants, physiological and socio-cultural differences between men and women are generally not considered when extrapolating research findings based on male athletes to a female athletic population. 1 In applied sport settings, these differences should also be considered to tailor support to athletes. Some of the ways women athletes’ experiences of sport differ to men's are that there are generally less resources invested in and opportunities available to them, societal pressures relating to body image tend to emphasise thinness rather than muscularity. Females also have unique physiological and anatomical considerations such as experiences of disruptive menstrual symptoms and concerns about menstrual bleeding, and need for breast support.2–4 While sociocultural influences are apparent when it comes to menstrual-related practices, given the focus is on the physiological monitoring of the menstrual cycle and other sex-specific considerations, we will predominately use the term ‘female athlete’ throughout this paper. There is a need to consider how these sex- and gender-based differences may be affecting athlete health, performance, and wellbeing, and adopt practices that address these to maximise opportunities for athletic development and provide optimal health support.
One way that multi-disciplinary support may be tailored to female athletes is through the consideration of menstrual cycles or menstrual dysfunction 5 ; menstrual cycle tracking is an example of a strategy recommended for the purpose of identifying common symptoms of menstrual disorders and empowering athletes to gain greater awareness of their bodies. However, barriers such as a lack of research and low knowledge of menstrual-related topics may influence initial decision-making related to its implementation and, ultimately, how useful it may be in promoting athlete health and performance. 6 Other strategies recommended considering the experiences of female athletes within the context of menstrual health include collecting information such as age of menarche and current menstrual cycle length during athlete screening, educating athletes on menstrual-related topics, creating environments where discussions of these topics may be had openly, and making menstrual products accessible to athletes to alleviate concerns related to menstruation and flooding.4,7 Recent work exploring menstrual cycle tracking in sport has demonstrated that a considerable proportion of practitioners in rugby (22%) monitor players’ menstrual cycles as a support strategy 8 and almost half (48.5%) of endurance athletes track their own cycle. 9 Despite reports of menstrual cycle tracking in specific settings, it is not currently understood how widespread the practice is in high performance sport settings, and the overall purpose of tracking and methods used have not been described.
There is a raft of other considerations beyond menstrual health that can also be made to tailor environments to support female athletes. This includes addressing experiences of female athletes (i.e., promoting breast health, appropriate bra fit, and pregnancy considerations), and the prevention and/or management of conditions that are not unique to but highly prevalent in female athletes (i.e., eating disorders, iron deficiency, stress urinary incontinence). 5 Periodic health screening is also an important practice common in applied settings for the prevention of and early intervention for conditions that may be detrimental to health or performance. 10 While the literature consistently recommends that various domains of female health be included in preparticipation exams, it appears that questions related to these domains, particularly relating to relative energy deficiency in sport (REDs), breast, and pelvic floor health are not usually included in such exams. 11 While screening practices in elite sport have been described, 10 there is little research to show how often female-specific screening outside of preparticipation exams takes place. Anecdotally, it is also common in applied settings to deliver some form of education to athletes, as well as practitioners, on topics such as sleep, recovery, and nutrition with the intention to promote health and wellbeing management, and optimise performance. The provision of education on topics relevant to female athletes, such as breast health, is recommended,12,13 with current evidence suggesting knowledge in this area is low; for example, most female rugby players are unaware of potential complications of contact breast injuries 14 and it is uncommon for females in both the general and athletic population to have correct fitting bras.13,15 However, the prevalence of providing education related to issues important to female athlete health and performance in these settings has not been reported.
Given there is a lack of research pertaining to current practices to tailor support to female athletes, the primary aim of this study is to understand current practices regarding menstrual cycle tracking, the provision of female-specific education, health screening, and other practical supports (e.g., menstrual product availability, uniform choice) to address concerns about menstruation in high performance sport. Describing the practices implemented in high performance sport settings to support female athletes may highlight discrepencies between research and practice, which could assist in determining priorities for future research, and guide practitioners in priorities and approaches to tailor support for female athletes in their environments. A secondary aim of this study is to explore to explore how factors such as group size, sport type, and country influence these practices to tailor support for female athletes. In doing so this study will offer a preliminary insight into the factors that may influence the implementation of female-specific practices in applied settings to be investigated further.
Methods
Participants
A cross-sectional survey design was used to capture responses from practitioners working with highly trained female athletes. Potential participants were contacted via email and invited to respond to the survey. The participants could work in roles related to coaching (i.e., head coach, assistant coach); rehabilitation (i.e., athletic trainer, physiotherapist); performance (i.e., strength and conditioning coach, sport scientist); nutrition (i.e., dietitian, nutritionist); medicine (i.e., physician); manager/director (i.e., program director). The study information was also shared via social media (e.g., LinkedIn and X) of the research team and their institutions. Snowball sampling was also used, where participants were encouraged to share the survey and study information with colleagues from other sporting organisations. In an attempt to minimise potential skewing of the data, participants were also asked to have only one practitioner from their organisation (i.e., club, team, or program) complete the survey. Practitioners were eligible to complete the survey if they worked with a group consisting of a minimum of two female athletes that were competing in at least national-level events (if individual athletes) or in an elite competition within their country (if team-sport athletes), and undertaking structured and periodised training. No exclusion criteria were applied based on type of sport or country; however, the survey was only available in English. Participants had to respond to at least eighty percent of the non-branched questions to be included in the analysis.
Survey
The online survey was developed and delivered using QuestionPro (Austin, TX), and open between March and December 2023. Approval was received by the Institutional Ethics Committee (HEC22384). Participants confirmed that they consented to the data collected being used for this study at the start of the survey. All questions were optional apart from those used to assess participant eligibility. The survey contained five sections (Figure 1), consisting of fixed-response questions with either single or multi-select response options and within each section of the survey there were at least two questions that contained branching logic to inform follow up questions presented to participants. Where multi-select response options were available, it was made clear to participants that multiple options could be selected and this has been specified in the results presented. The survey is included in the Supplemental Material. Participants were instructed to respond to the survey based on their current practices implemented with a single group of athletes (that is, if working across multiple groups, the practitioner responded with reference to only one group).
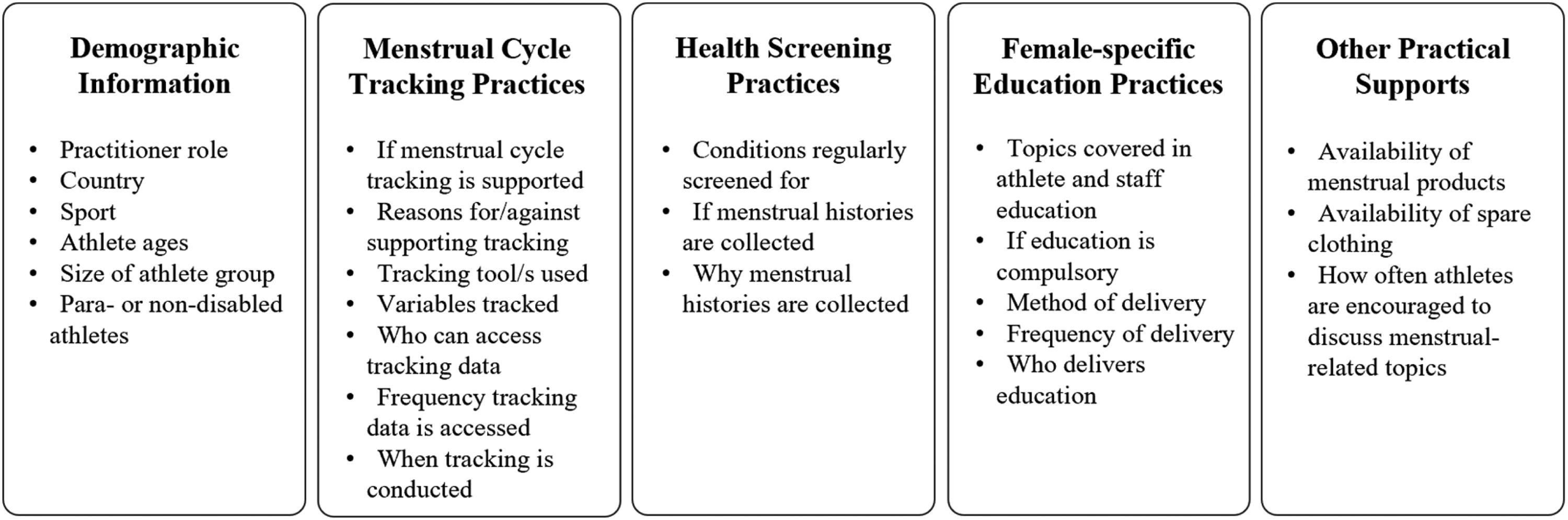
Summary of topics contained in the five sections of the survey.
Statistical analysis
Frequency analyses were conducted for each multiple-choice question, with counts and percentages presented. Pearson's chi-squared tests of association were conducted to determine whether there were any relationships between practices implemented and the characteristics of the group the participants worked with. The accepted significance level was .05. The characteristics of interest included support for tracking (i.e., if menstrual cycle tracking is required or encouraged), provision of menstrual-related education (i.e., if athletes or staff members received any education on menstrual cycles, menstrual dysfunction, REDs, and/or hormonal contraception), sport type (i.e., team or individual sports), group size (i.e., groups of athletes containing more or less than 20 athletes), and country (i.e., if the participant was based in the United States of America or another country). In the results, only the significant associations with effect size > .2 (i.e., moderate association or stronger based on the Phi or Cramer's V coefficient 16 ) are reported.
Results
One hundred and forty-one practitioners responded to more than 80% of the non-branched questions and were included in this study. All participants worked with athletes that could be described as ‘highly trained’ (Tier 3) or above, 17 were largely based in Westernised countries, and involved in invasion (i.e., football, basketball) and racing (i.e., track and field, swimming) sports. Figure 2 provides a summary of countries and types of sports represented in these survey responses and information regarding the athlete groups the participants work with including the size of the group, ages of the athletes, and whether they are non-disabled or para-athletes.
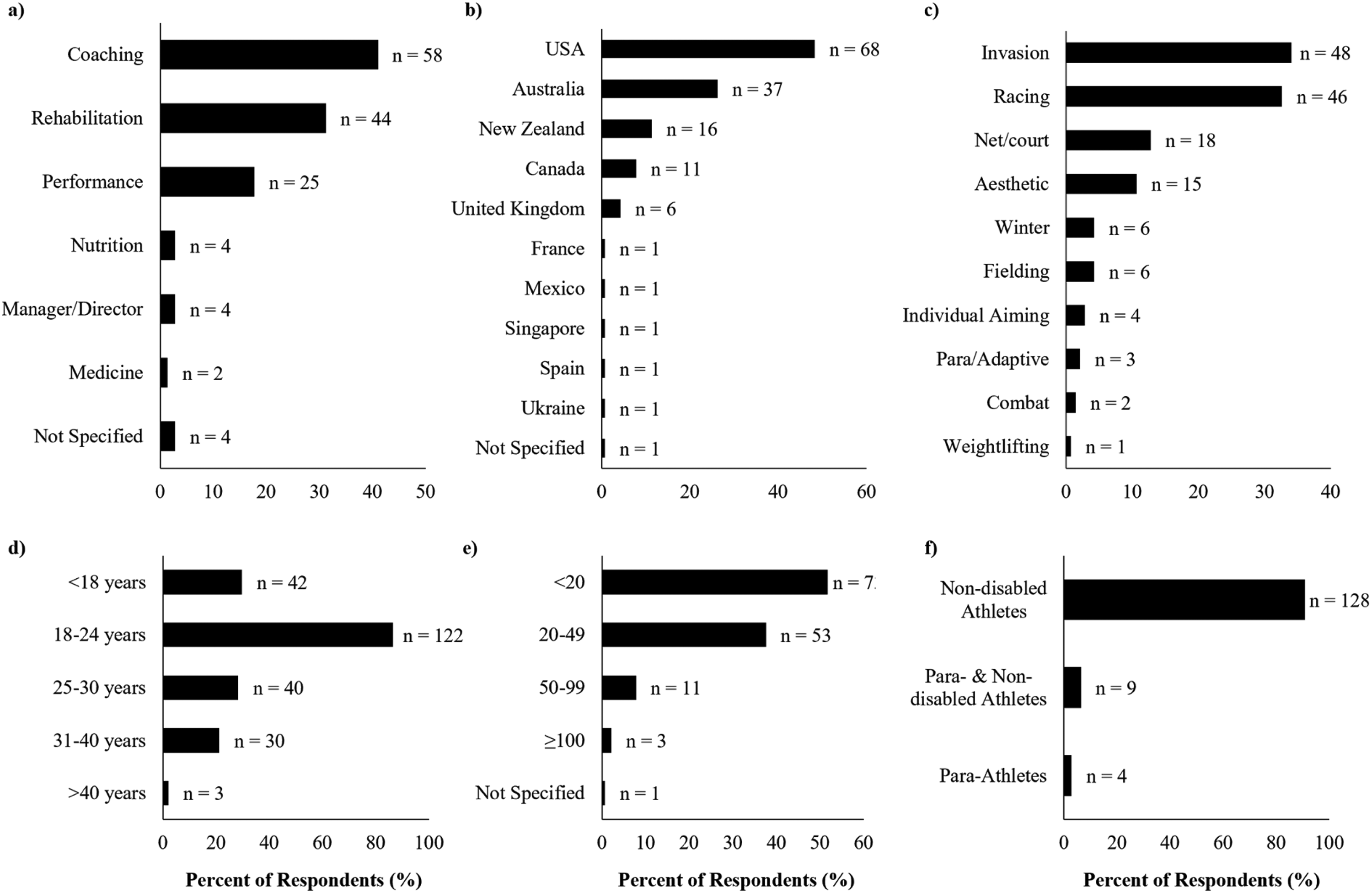
Summary of participant characteristics, including a) current role occupied by the participant; b) country they are based in; c) type of sport; d) ages of the athletes in the group; e) size of the group they work with (i.e., number of athletes); and f) whether the group consists of non-disabled or para-athletes.
Menstrual cycle tracking
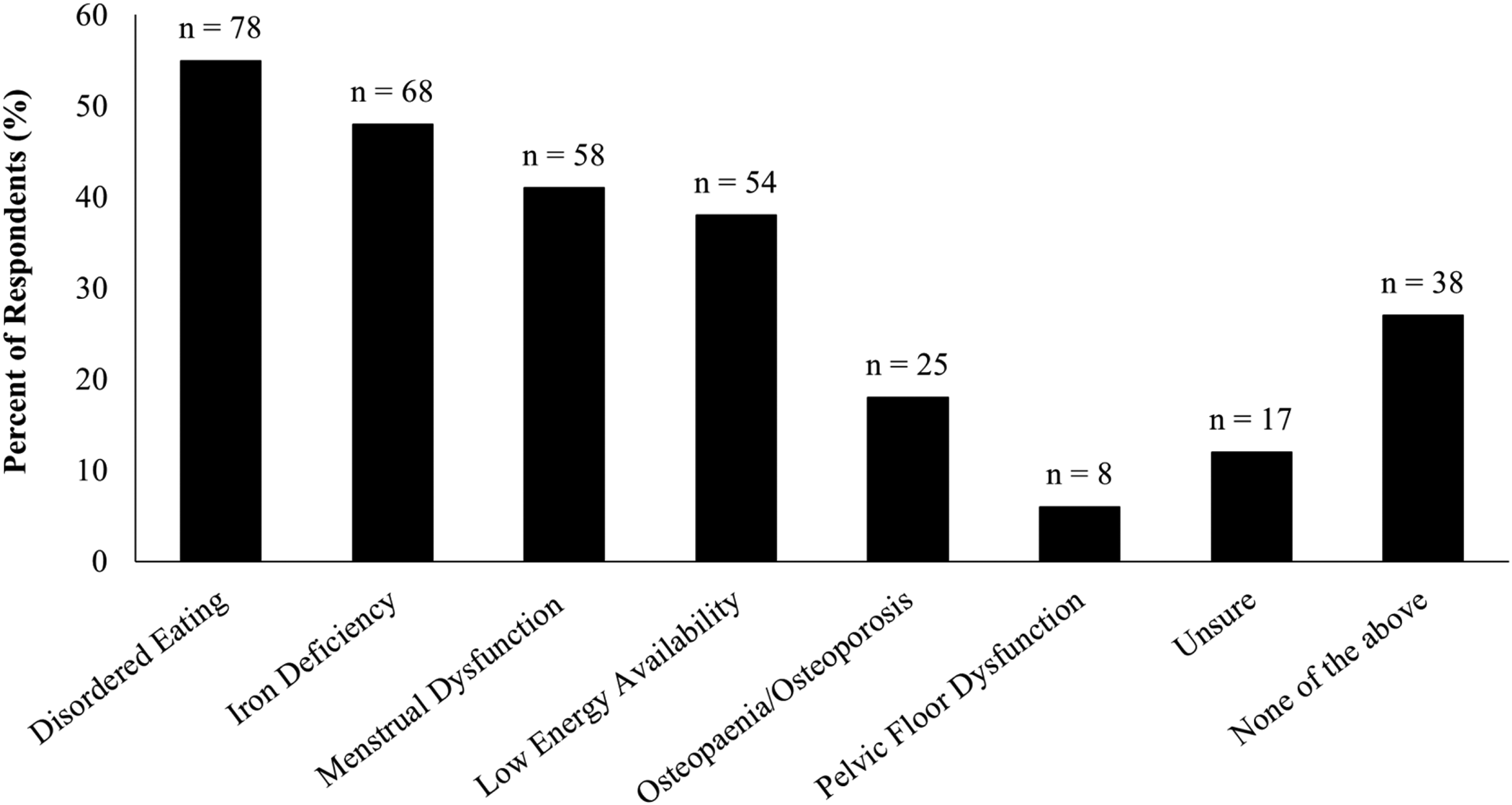
Close to half of the participants reported not discussing menstrual cycle tracking with athletes at all (n = 65 [out of 141], 46%). Few practitioners required athletes to track their menstrual cycle (n = 12, 9%); instead, participants more often encouraged (rather than mandated) tracking (n = 51, 36%). No participants actively discouraged athletes from tracking their menstrual cycle but several reported instances in which specific athletes were discouraged from tracking (n = 4, 3%) or tracking was not discussed with some athletes (n = 16, 11%). Multiple responses were allowed, and seven participants indicated they took multiple approaches to tracking with their athletes (e.g., encouraged some athletes to track and discouraged others from tracking). The reasons behind the participants’ approach to menstrual cycle tracking with their athletes, and further details regarding when cycles are tracked and access to tracking data are presented in Table 1.
Responses to questions related to menstrual cycle tracking practices.
*Multiple responses were allowed and may add to more than 100%.
From those who stated they used tracking to inform menstrual cycle phase-based training (n = 17, 32%), responses to branching questions identified phase-based training most commonly occurred through the prediction of when symptoms or negative side-effects would occur and altering the program to accommodate (n = 14, 82%), and by adjusting volume or intensity in certain menstrual cycle phases (n = 13, 76%).
When tracking, most practitioners reported requiring or encouraging athletes to use a calendar-based method (n = 37 [out of 53], 70%), however, some were unsure (n = 12, 23%), and few (n = 4, 8%) used a combination of calendar-based and additional physiological methods. The variables reportedly tracked include days that bleeding occurs (n = 36, 68%), days that symptoms occur (n = 24, 45%), heaviness of bleeding (n = 21, 40%), and type and severity of symptoms (n = 19, 36%). Numerous participants were not sure what variables were tracked (n = 14, 26%) and none tracked days non-active hormonal contraceptive pills were consumed. Physiological methods that were reported as part of menstrual cycle tracking include cervical mucous (n = 1, 2%), home ovulation test kits (n = 1, 2%), basal body temperature (n = 2, 4%), and blood hormone measurements (n = 3, 6%). No participants reported using salivary or urinary hormone measurements.
There was a significant relationship between education provision and tracking practices. Participants that provided education on menstrual-related topics (i.e., menstrual cycles, menstrual dysfunction, hormonal contraception, and/or female athlete triad/REDs) were more likely to encourage menstrual cycle tracking,
Health screening
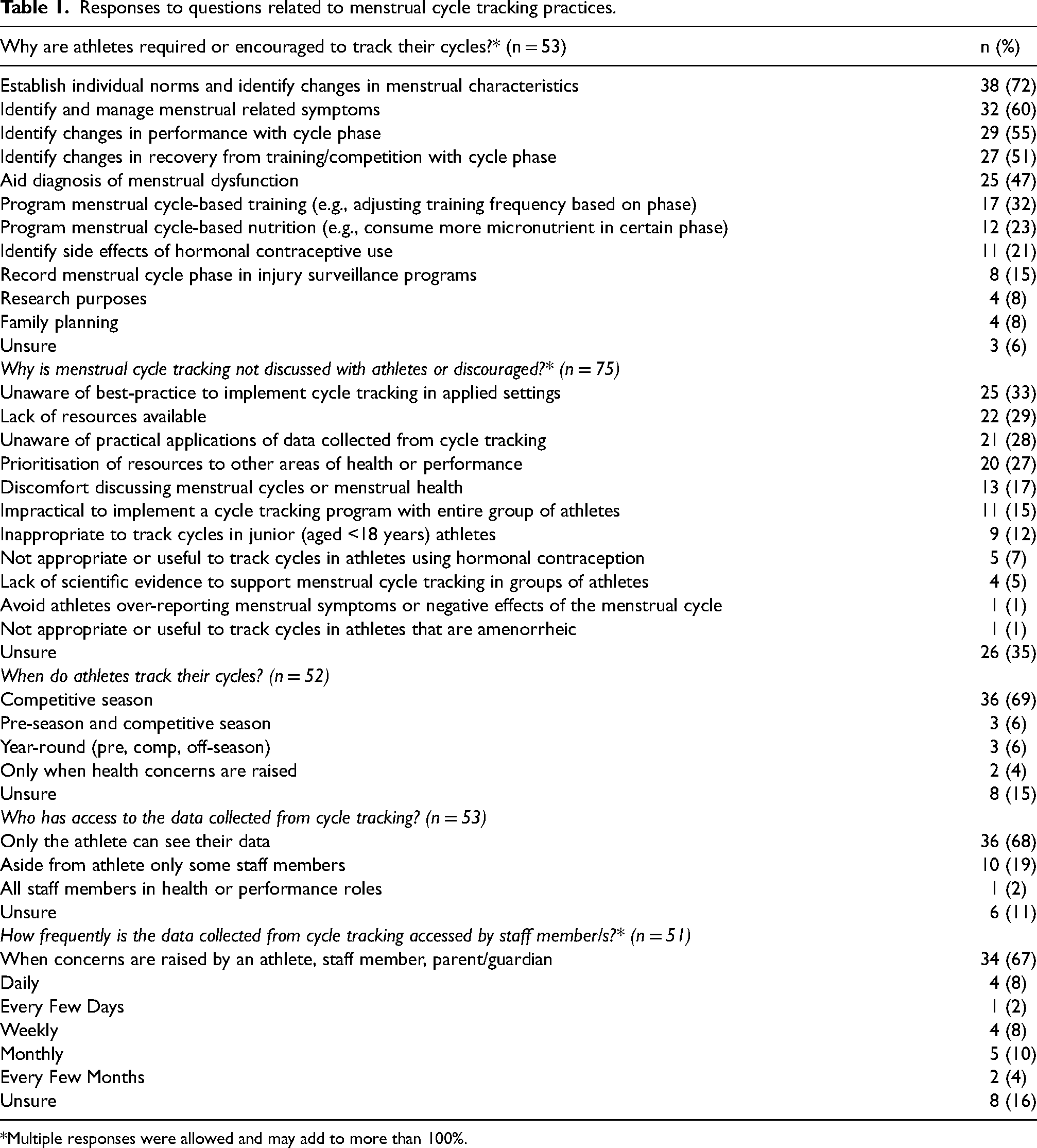
Figure 3 illustrates the number of participants that conduct routine screening for various conditions pertinent to female athletes, with disordered eating and eating disorders being the main condition screened for (n = 78 [out of 141], 55%).
Number of participants who conduct screening for a variety of conditions important to female athlete health (n = 141). Multiple responses were allowed and may add to more than 100%.
Education provision was related to health screening practices with those that provided menstrual-related education being more likely to conduct screening for disordered eating,
Participants more commonly reported not collecting menstrual histories from athletes (n = 60 [out of 141], 43%); however, a considerable proportion of participants (n = 26, 18%) were unsure whether or not they were collected. The most common reasons for collecting menstrual histories were to identify athletes at risk of female athlete triad or REDs (n = 44 [out of 55], 80%) and to inform discussions with the health/medical professional (n = 34, 62%). There were significant relationships between the collection of menstrual histories and country, group size, and sport type. Menstrual histories were more likely to be collected by those in the USA than other countries,
Female-specific education
Table 2 demonstrates how frequently various female-specific topics are covered in education delivered to athletes and staff.
Topics included in female-specific education delivered to athletes and staff members.
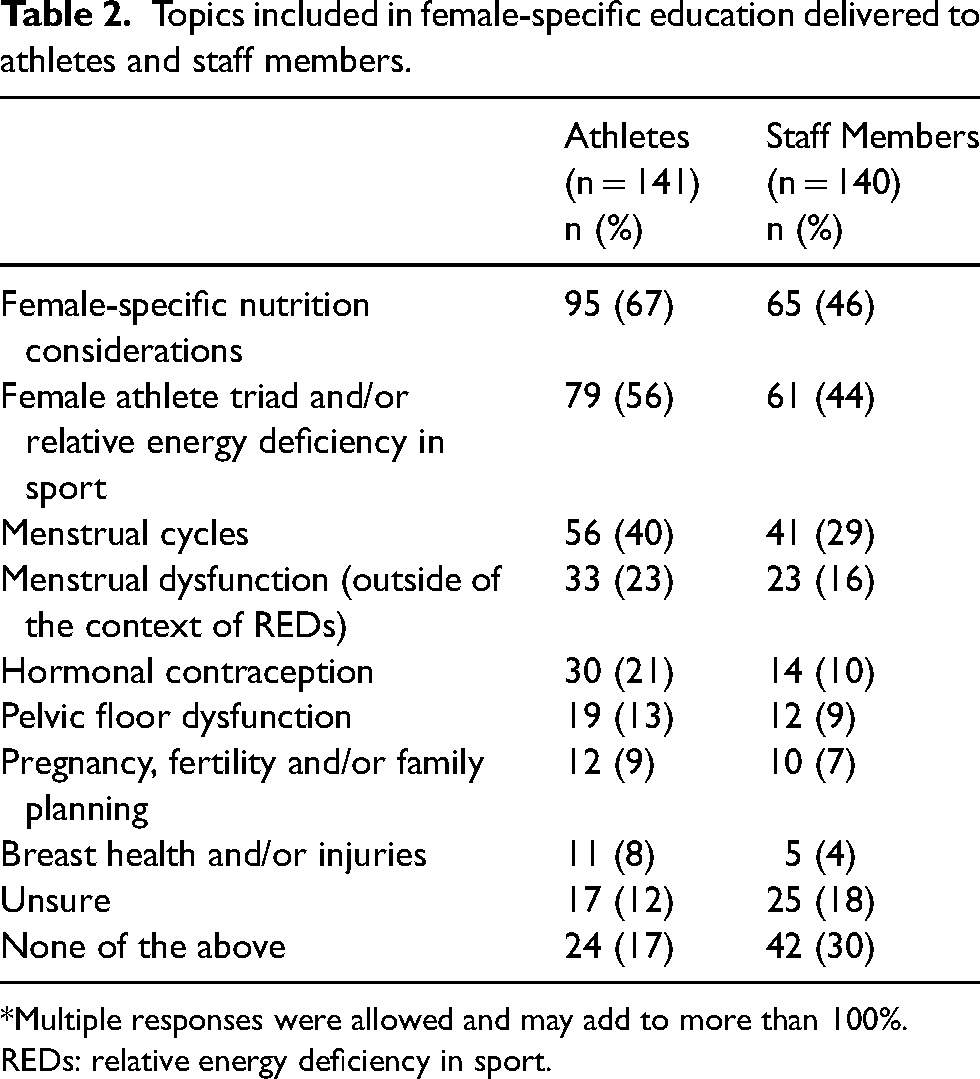
*Multiple responses were allowed and may add to more than 100%.
REDs: relative energy deficiency in sport.
The provision of take-home resources (i.e., handouts, links to online resources) were the main avenue of providing education to athletes on topics relevant to female athlete health and performance (n = 84 [out of 105], 63%), followed by individual counselling with a medical professional (n = 80, 60%), informal discussions (n = 75, 56%), and presentations (i.e., workshops, question and answer sessions) (n = 68, 51%). Attendance at education presentations is usually an opt-in (n = 29 [out of 63], 46%) or compulsory (n = 27, 43%) process for athletes. For those who reported providing education to staff, this was most often delivered as a presentation (n = 19 [out of 28], 68%), take-home resources (n = 17, 61%), and informal discussions (n = 11, 39%). For staff, education is usually an opt-in process (n = 17 [out of 27], 63%) and less often compulsory (n = 5, 19%). The delivery of education on these topics was most commonly the responsibility of practitioners embedded within the sporting organisation, including the dietitian/nutritionist (n = 67 [out of 110], 61%), physician (n = 50, 45%), or coach (n = 35, 32%). It was less common to engage content-experts (n = 26, 24%), dietitian/nutritionists (n = 26, 24%), or physicians (n = 25, 23%) external to the sporting organisation.
Practitioners working with team sport athletes more often reported providing education to athletes on breast health,
Other support
This survey also captured other practices that were implemented to support female athletes. Most participants ensured menstrual products were available to athletes, either freely (n = 49 [out of 136], 36%) or on request (n = 35, 26%). Similarly, spare uniforms and training shorts were available freely (n = 45, 33%) or on request (n = 42, 31%) for athletes. Figure 4 outlines how often athletes are encouraged to discuss menstrual-related topics with different people within their sporting environment. The provision of menstrual-related education was associated with how often athletes were encouraged to discuss menstrual health with their physician,
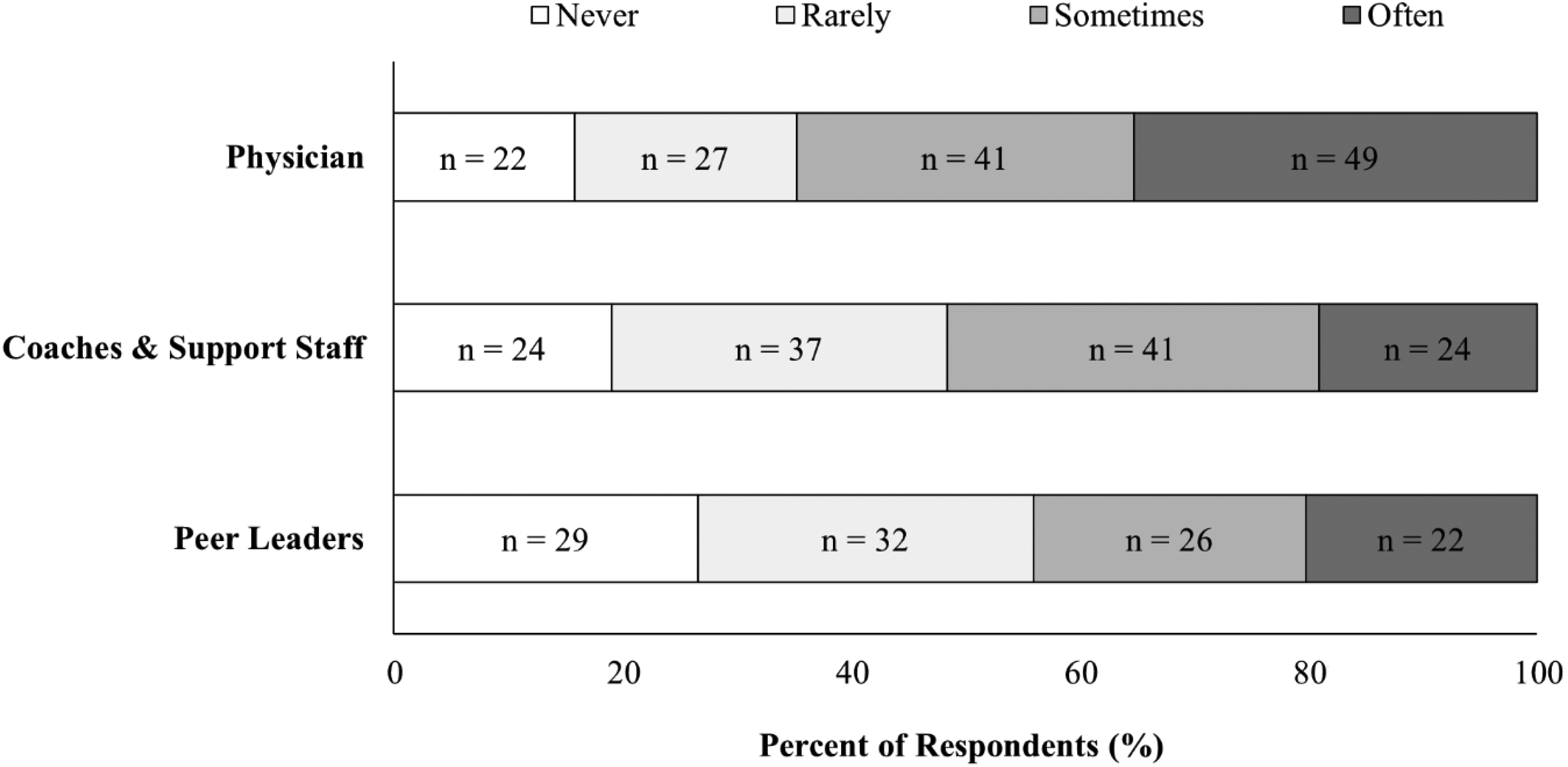
How often female athletes are encouraged to discuss menstrual-related topics with various individuals within their training environment.
Discussion
The aims of this study were primarily to understand current practices relating to menstrual cycle tracking, health screening, education and other considerations to tailor support to female athletes and, secondly, to explore how factors such as group size, sport type, and country influence these practices. The survey results indicate that menstrual cycle tracking is not a widely used practice in high performance settings, with 36% and 9% of participants encouraging or requiring athletes to track their menstrual cycle respectively, most commonly via calendar-based methods. Additionally, tracking is more likely to be encouraged or required in organisations where menstrual-related education is provided to athletes and/or staff. Female-specific nutritional considerations and female athlete triad or REDs were the topics most often included in education tailored to female athletes while topics such as breast health/injuries, pelvic floor dysfunction, and fertility/pregnancy were covered the least. There were also differences observed in practices implemented by those based in the USA compared with other countries, such as those based in the USA being less likely to educate athletes on menstrual cycles and require athletes to track their cycle, but being more likely to collect menstrual histories and screen for menstrual dysfunction. These results may indicate a gap in the evidence-base for practitioners to work from, or the slow translation of research to practice and highlights contextual factors that may be key contributors to the practices implemented in high performance sport settings.
Are rationales for tracking supported by research?
One of the key reasons practitioners did not discuss cycle tracking with their athletes was due to their lack of awareness of the best method to track or use the data collected. As such, there appears to be a slow translation of research to practice with research often recommending that cycle tracking be conducted.5,18–20 For those who did encourage or require tracking, one of the most common reasons was for the management of menstrual symptoms. Given many athletes experience a wide range of menstrual symptoms, 21 many of which contribute to athletes’ negative perceptions of the menstrual cycle, 22 tracking for the purpose of managing symptoms is arguably important in sport. However, the effectiveness of menstrual symptom management strategies, specifically in athletic populations, has yet to be researched. Effective management strategies are likely to be highly individual to the athlete and their symptoms. 23 This presents challenges for those working with large groups of athletes. Therefore, the usefulness of tracking for this purpose (i.e., effectiveness of tracking and implementing symptom management strategies on actual and perceived performance), and the role of practitioners in supporting athletes to manage symptoms still needs to be explored. A longitudinal study examining the effect of a cycle tracking and symptom management intervention may further the understanding of the potential efficacy of tracking for symptom management. It is important to note that there are perhaps differences in practices implemented by those who encourage or require athletes to track that could not captured in this study and mandatory tracking is not recommended due to issues surrounding consent and privacy. 24
Another common reason tracking was encouraged was to identify changes in performance and recovery related to menstrual cycle phase. Researchers currently recommend that where tracking is used to understand the influence of the menstrual cycle on performance, it should be approached on an individual basis. 25 This is due to only trivial to small effects of cycle phase on exercise performance or recovery markers being observed at a group level.25,26 While literature reviews show a trivial influence of the menstrual cycle on performance and recovery outcomes, a large proportion of athletes perceive their performance to be influenced by their cycle (i.e., reduced performance during particular phases in their cycle).27,28 This negative perception around the menstrual cycle rather than a specific cycle phase has been linked to reduced performance. 28 This highlights that in practice it may be important to consider what messaging surrounding menstrual cycles is presented to athletes when discussing cycle tracking or providing education on menstrual-related topics to avoid reinforcing these negative perceptions.
Phase-based training is currently implemented by some practitioners, mainly via making changes to accommodate symptoms or modifying training variables (i.e., intensity, frequency) with cycle phases. Researchers are still investigating the effect of phase-based periodisation on training adaptations, particularly in resistance training, and findings are conflicting. While research may lag practice in being able to empirically support its implementation, further ecological studies evaluating the outcome of such strategies is required, both from a physiological and sociological perspective. While there may be small changes in performance across the menstrual cycle or possible benefits of training specific to menstrual cycle phase or symptoms, likely the greatest opportunities for improving training and performance experiences of athletes may be through appropriately managing their symptoms, as well as ensuring other key aspects of athlete preparation, such as nutrition, fatigue, and sleep are addressed.
Are the methods of tracking used suitable?
Calendar-based methods (without additional physiological measures i.e., hormone measures) were the most common means of tracking. These methods are appropriate in identifying trends related to menstrual symptoms and identifying obvious changes in menstrual cycle characteristics (i.e., menstrual cycle length, amenorrhoea). Even though 61% of participants indicated that tracking was used to identify and manage symptoms, only 46% reported monitoring which days symptoms occurred and even fewer tracked details such as symptom type and severity. These additional details may be useful when trialling management strategies, as assessing the type and severity of symptoms enables practitioners and athletes to check the efficacy of strategies to alleviate these symptom/s. Menstrual cycle length can identify severe forms of menstrual dysfunction by identifying oligomenorrhea (i.e., menstrual cycle length greater than 35 days) or amenorrhoea (i.e., menstruation absent for at least 90 days). However, subtle menstrual disturbances (i.e., anovulation or luteal phase deficiency), which can occur whilst regularly menstruating and portend more severe forms of menstrual dysfunction, cannot be captured by calendar-based methods alone. While many (n = 25) participants used tracking to aid diagnosis of menstrual dysfunction, very few (n = 4) participants used additional physiological methods of tracking, such as ovulation test kits, basal body temperature, or hormone measurements. These methods can be clinically useful to flag subtle menstrual disturbances, which affect up to half of the female exercising and athletic population.29,30 The presence of these sub-clinical menstrual disturbances has been linked to LEA, 31 which, if sustained, can contribute to the development of REDs 32 and negatively impact various markers of bone health and increase stress fracture risk. 33 As such, when tracking menstrual cycles, understanding the reasons for tracking may help dictate the relevance for using more sensitive monitoring methods in addition to calendar-based methods. This would enable early interventions to be implemented before severe menstrual dysfunction and greater health impacts occur.
How does education relate to menstrual cycle tracking practices?
Our results demonstrate that practitioners who provided education on menstrual-related topics were more likely to require or encourage athletes to track their cycles. Additionally, those providing this education were more likely to encourage athletes to discuss menstrual health with a physician and other staff, and to conduct screening for disordered eating, iron deficiency, osteopenia/osteoporosis, menstrual dysfunction, and LEA. The relationship between education and support for cycle tracking has emerged due to the likely benefits of providing menstrual-related education on facilitating communication, reducing stigma, and addressing knowledge gaps for both athletes and practitioners. Education on these topics is seen by athletes and practitioners to be important for facilitating communication within the training environment.34–36 Practitioners have previously identified that they want to learn more about these topics so they can provide appropriate and useful advice to athletes 35 ; while athletes want education to learn more about how to manage their symptoms and address remaining stigma associated with menstruation. 37 The main ways athletes learn about menstrual cycles are through school and personal research, which may not be sport-specific or accurate. 34 and many view practitioners such as coaches to be a source of information regarding menstrual health. 38 Based on our findings, we are unable to determine the causal relationship between the provision of menstrual-related education and its association with tracking and screening practices. Instead, we hypothesise (1) education was provided to support the tracking or screening practices already implemented, (2) those who received education were more inclined to implement tracking and health screening, and/or (3) those with the time or resources to provide education on these topics also had the means to implement tracking and additional screening. Further research on the differences in education provided to athletes and practitioners is warranted, this includes exploration of the educational content and sources. A focus on practitioner education is especially important given their role as a source of information for athletes.
Where are the gaps in education?
The topic of female-specific nutrition was most often included in education for athletes and practitioners. We hypothesise nutrition was popular as it is generally a more researched and discussed topic in sport science, and clear guidelines regarding nutritional strategies have been established. 39 Conversely, topics such as pelvic floor dysfunction, breast health/injuries, and pregnancy/fertility, that have a lower general awareness and guidance available, were least often covered in education for both athletes and staff.
Stress urinary incontinence, a common form of pelvic floor dysfunction, affects around 44% of female athletes. 40 Given the prevalence of and stigma associated with incontinence, and limited awareness of pelvic floor dysfunction in athletes, education surrounding this topic including where help may be sought (i.e., women's health/pelvic floor physiotherapist) may be useful to limit the negative impacts this may have on athlete performance, confidence, and preparation. 41
Covering breast health in education may introduce athletes, particularly those in contact sports, to options for breast protection and provide information regarding potential complications associated with breast injuries (e.g., calcified breast tissue appearing similar to malignancies). 42 It could also raise awareness relating to the importance of bra fitting, which can influence performance as increased breast support can improve efficiency during running. 43 Survey participants involved in team sports were more likely to address breast health in education than those involved in individual sports; 9 of the 11 participants that reported this topic was included in athlete education were involved in invasion or net/court sports, where athletes are likely to sustain contact from an opponent or ball. Highlighting pelvic floor dysfunction and breast health/injury in education are valuable, but often overlooked, strategies to tailor support based on female-specific considerations.
‘Pregnancy, fertility, and family planning’ was the topic least likely to be addressed in athlete education. This finding may be the result of participant demographics (only thirty-three percent (n = 46) of participants who responded to this question worked with athletes over the age of 25), so the topic may not be considered relevant to younger athletes. However, it is common for female athletes to feel uncertainty about family planning alongside their sporting career and desire greater support for family planning from national sporting bodies and organisational leaders (i.e., coaches). 44 Further, the use of fertility treatments is higher in athletes that experienced menstrual dysfunction during their career than those that did not. 45 Inclusion of this topic in female athlete education curricula may support athletes to navigate potential concerns about overlapping fertility and performance windows. 46 Educating athletes on issues such as pelvic floor dysfunction, breast health/injuries, and pregnancy/fertility is important to ensure that they are able to make informed decisions about factors that are likely to impact their sporting careers and lives outside of sport.
How did the USA compare to the rest of the world?
The high response rate from participants based in the USA allowed us to compare practices in high performance sport settings in the USA against other (primarily Westernised) countries. This additional comparison may be of interest as the USA has well-established athletic pathways within the education system, with lawful access for female athletes granted by Title IX, a federal law ensuring students at institutions receiving government funding have equal access to school activities, regardless of gender or sex. 47 Compared to other countries, those based in the USA were less likely to provide athletes and practitioners with education on menstrual cycles. American participants were also less likely to require athletes to track and discuss cycle tracking with their athletes than those from other countries, despite being more likely to collect athletes’ menstrual histories and screen for disordered eating/eating disorders and menstrual dysfunction. It is common to collect menstrual history information during preparticipation screenings in the USA, particularly in high school and collegiate sport settings. 48
The avoidance of menstrual cycle tracking (and related discussions and education) may be linked to issues surrounding reproductive rights and perceptions of safeguarding of athletes. Whilst laws vary between states in the USA, the overturning of Roe Vs. Wade (2022) has caused concern for how menstrual cycle tracking data, both in and out of a sport context, could be used against individuals. 24 This extends to transgender athletes, where mandatory tracking or screening may reveal sensitive information or further the potential risk of discrimination. 24 Further, although abuse in sport is not an issue unique to the USA, the apparent avoidance of tracking could be attributed to wanting to avoid issues with the safeguarding of athletes, 24 as it is considered abuse for a coach to “attempt to control an athlete's weight or menstrual cycle”. 49 As such, given the perceived or actual risks for coercion, mandatory tracking of athlete menstrual cycles are not recommended. 24 Conversely, education and MC-related discussions should be viewed as a positive way to improve stigma, knowledge, and provide justification for why someone may want to monitor their menstrual health. Moving forward, it is important to recognise that societal and cultural aspects may influence how support is tailored to female athletes in high performance sport and understanding these socio-cultural influences will be important for the optimal uptake of tracking. Socio-cultural factors are, therefore, an important aspect that should be reported in subsequent qualitative and quantitative research. It should also be acknowledged that while there are frequent recommendations for MC-related education and discussions to be included in women's sport, there is a gap in the literature pertaining to the culturally safe delivery of such education and communication strategies.
Limitations
This study captures an overview of current practices in high performance sport settings to support female athletes. A strength of this study is the broad range of sports represented; however, a larger sample would have provided a more comprehensive and precise insight into current practices. The results of this study are also limited to English speaking participants, and as such the results are not representative of global practices. Instead, the majority of our findings are specific to practices of Westernised countries. More research to understand the practices of non-western societies is important given the implementation of female-specific support strategies (e.g., menstrual screening or menstrual cycle tracking) are influenced by sociocultural context.50,51 As with any survey, there is also a risk of sampling bias, with respondents potentially being practitioners with an existing interest in female athletes or who are already implementing tailored support to female athletes. However, given less than half of the participants required or encouraged athletes to track their cycle, results do not appear to be skewed in this way and can reasonably be considered representative of practices in high performance sport settings.
The survey also captured whether participants were not sure about the practices implemented in their environment, with anywhere from 4–35% of respondents answering “Unsure” to a specific question. Practitioners’ knowledge of practices implemented within their organisation likely depends on their role. Practitioners in coaching roles were the most represented participants in this survey and these were most frequently head coaches, who would be expected to have a broad grasp of the strategies in place across different areas of athlete support (i.e., physical preparation, rehabilitation, medical). It may be possible that participants in other roles (e.g., dietitian, physiotherapist) may not have a depth of understanding across all areas in order to be able to respond to some of these questions. However, we attempted to address this limitation by instructing participants to discuss the survey with their colleagues if they were not sure how to answer a question. This additional burden may have prevented some participants from doing so when they were not sure of the practices used in their environment. While this means results may be less accurate, it provides an interesting insight into high performance sport settings.
Conclusion
This study offers a general snapshot into the current practices in high performance sport settings to tailor support to the experiences and needs of female athletes. Although menstrual cycle tracking represents one potential approach to providing female-specific support, it is not currently a widely implemented strategy in the majority of high-performance settings. This lack of implementation is probably due to a lack of available research and guidance for how to best approach tracking and related education. Further studies may look to observe the factors that influence practice and explore how this practice evolves over time, particularly as more female-specific research or research including female athlete participants emerges. Finally, future research with a broader sample to capture more countries and cultures is necessary to understand current practices and the best practice implementation for menstrual cycle tracking and other female-specific support strategies.
Supplemental Material
sj-docx-1-spo-10.1177_17479541251361218 - Supplemental material for Tailoring support to the female athlete: A cross-sectional online survey to observe current practices in high performance sport
Supplemental material, sj-docx-1-spo-10.1177_17479541251361218 for Tailoring support to the female athlete: A cross-sectional online survey to observe current practices in high performance sport by Mikaeli Carmichael, Alexandra Roberts, Kate Perry and Anthea Clarke in International Journal of Sports Science & Coaching
Footnotes
Ethical considerations
Approval was received by the Institutional Ethics Committee, La Trobe University (HEC22384).
Consent to participate
Participants confirmed that they consented to the data collected being used for this study at the start of the survey.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.