
Abstract
Stretching techniques like proprioceptive neuromuscular facilitation (PNF) or tissue work, like foam rolling (FR), are assumed to increase the range of motion (ROM), but little is known about consecutive adaptations in complex movement techniques. The study aimed to quantify short-term adaptations in the squat movement due to the potentially raised ROM after FR or PNF stretching. Forty young adults (20 females) participated in the study. The intervention group applied PNF stretching or FR in a cross-over design between the first and the second set of five squats, whereas the control group rested. After each set of squats, a questionnaire measured easiness, smoothness, and enjoyment using visual analog scales. Ankle ROM and hamstring flexibility were tested using the Weight-Bearing Lunge Test (WBLT) and the Stand and Reach Test (SaR). The squat movement was assessed through joint angles, specifically including the pelvis motion, utilizing a motion capture system (250 Hz). Results of rANOVAs show a significantly higher ROM increase in the intervention group than in the controls (p = 0.006 for FR and p < 0.003 for PNF in WBLT and SaR, respectively). Angle pathways did not change. After the second set, all groups recorded enhanced perceptions of ease, smoothness, and enjoyment. Interestingly, the larger ROM did not change the squatting motion. In conclusion, both interventions increased ROM in direct ROM tests. However, ankle dorsiflexion and pelvic tilt in squatting, hypothesized to be constrained by ROM, did not change.
Keywords
Introduction
Warming up is widely accepted and recommended to improve muscle activity and to lower the risk of injury.1,2 Comparing different warm-up strategies, some research indicates relative performance enhancement, e.g., in a coordinative jumping task when stretching is included. 3 There are three common variations of stretching techniques: static, dynamic, and proprioceptive neuromuscular facilitation (PNF). The contract-relax type of PNF (CR-PNF) combines a static stretch, an isometric contraction with subsequent relaxation, followed by another static stretch. This PNF technique has various complex effects on muscle biomechanics and neuromuscular activity, for example reduced neural activation and reduction of muscle stiffness allowing for increased range of motion (ROM).4,5,6 However, neurophysiological stretching mechanisms are also suspected to reduce muscle activity, which result in detrimental effects on performance when maximal muscle strength is needed.7,8 A more recent and popular technique for increasing flexibility, potentially without detrimental effects on performance, is using a foam roller.9–14 When foam rolling (FR), a limb or body part is placed on a cylindrical tube and rolled alongside the muscles, such that the underlying tissue is mechanically stressed.
Whereas stretching and FR can be assumed to increase ROM, the effect on subsequent movement performance is still discussed. Stretching and FR not only acts on muscles but also on the muscle-tendon and tendon properties. Thus, when looking into stretching and FR effects on movement, the muscle-tendon action can provide more information than active or passive ROM alone. Changes in muscle-tendon properties5,15,16 might alter motor control strategies and influence movement coordination.7,17 Therefore, changes in ROM and tissue properties might affect movement pattern execution, provoking performance adaptations in complex movement techniques. Studies concerning stretching and FR effects on performance mainly concentrated on force production, sprint, and jump performance.18–21 Whereas the literature reports small advantage for FR effects on performance, 19 the short-term impact of FR or CR-PNF stretching due to increased ROM on coordinative execution patterns in demanding movements is unclear and has only been rarely studied. 22
One of the most basal movement patterns is the squat. It is an established resistance training exercise for effectively enhancing physical strength and power.23,24,25 The bilateral bodyweight squat at or below 90° knee flexion, with proper symmetry and coordination, has been proposed to indicate overall movement quality.23,26 Athletes who do not demonstrate appropriate mechanics may utilize compensatory movement strategies. One example of a possible movement adaptation is seen when the dorsiflexion ROM of the ankle is limited, which will restrict the forward knee motion. This, in consequence, can cause excessive forward lean of the trunk during the squat and will likely transfer the load inappropriately to the lower back.25,27,28 Secondly, when athletes lack hip mobility greater trunk or lumbar flexion is a possible compensatory movement strategy, which leads to increased compressive and shear forces. 23 Ankle ROM and hamstring flexibility determine squatting depth with correct hip positioning when muscle strength is sufficient. Therefore, changes in ankle ROM and hamstring flexibility could facilitate a better quality of squatting execution, specifically: this is a higher squatting depth without a counter-movement of the pelvis, the so-called “Butt Wink”.
Considering these dependencies, the study aimed to investigate whether an increase in ankle ROM and hamstring flexibility would lead to improved subsequent squatting execution quality. In detail, the study investigates whether CR-PNF or a FR intervention will result in greater ROM and, consequently, will potentially lead to different changes in the movement execution of squats. Based on the current literature comparing the effects of PNF-stretching or FR, we (i) hypothesized that both interventions (CR-PNF-stretching and FR) would be adequate to increase ROM in ankle dorsiflexion and hamstring flexibility. As a consequence, we expected that the squatting movement pattern would change to a higher technical performance level. Accordingly, we (ii) hypothesized that joint angles (ankle, knee, upper-body-thigh, pelvis) quantified during squatting would change due to an increased ROM after CR-PNF stretching or after a FR intervention, favoring FR effects. In addition, we (iii) hypothesized that the participants would report changed motion feelings after the intervention when performing the squats.
To ensure that hypothesized increased ROM and movement changes are not an effect of repetition alone (learning or adaptation), we introduced a control group who conducted the same experimental measurements but rested in between. In summary, the main aim of the present study was to compare the joint angles of the ankle, knee, and pelvis during squatting and the motion experience before and after a CR-PNF stretching or a FR intervention. The interventions follow a cross-over design, and results will be compared to a control group. While the intervention is likely to increase joint ROM, immediate effects on movement technique, e.g., in squatting, have, to the best of the authors’ knowledge, not yet been quantified.
Methods
This is a controlled mixed methods study, collecting quantitative data using a 3D motion tracking system (Vicon, eight Bonita B10 cameras) and gathering qualitative data with a three-item questionnaire investigating participants’ perception of their squats using a visual analog scale (VAS). A within-subject design was used to compare FR and CR-PNF stretching effects on ROM and the following squatting movement. A control condition without stretching was implemented for comparison (Figure 1). The Institutional Review Board has granted the study ethical approval (certificate 13/2020) in accordance with the declaration of Helsinki and the ethics commission of the University of Innsbruck.
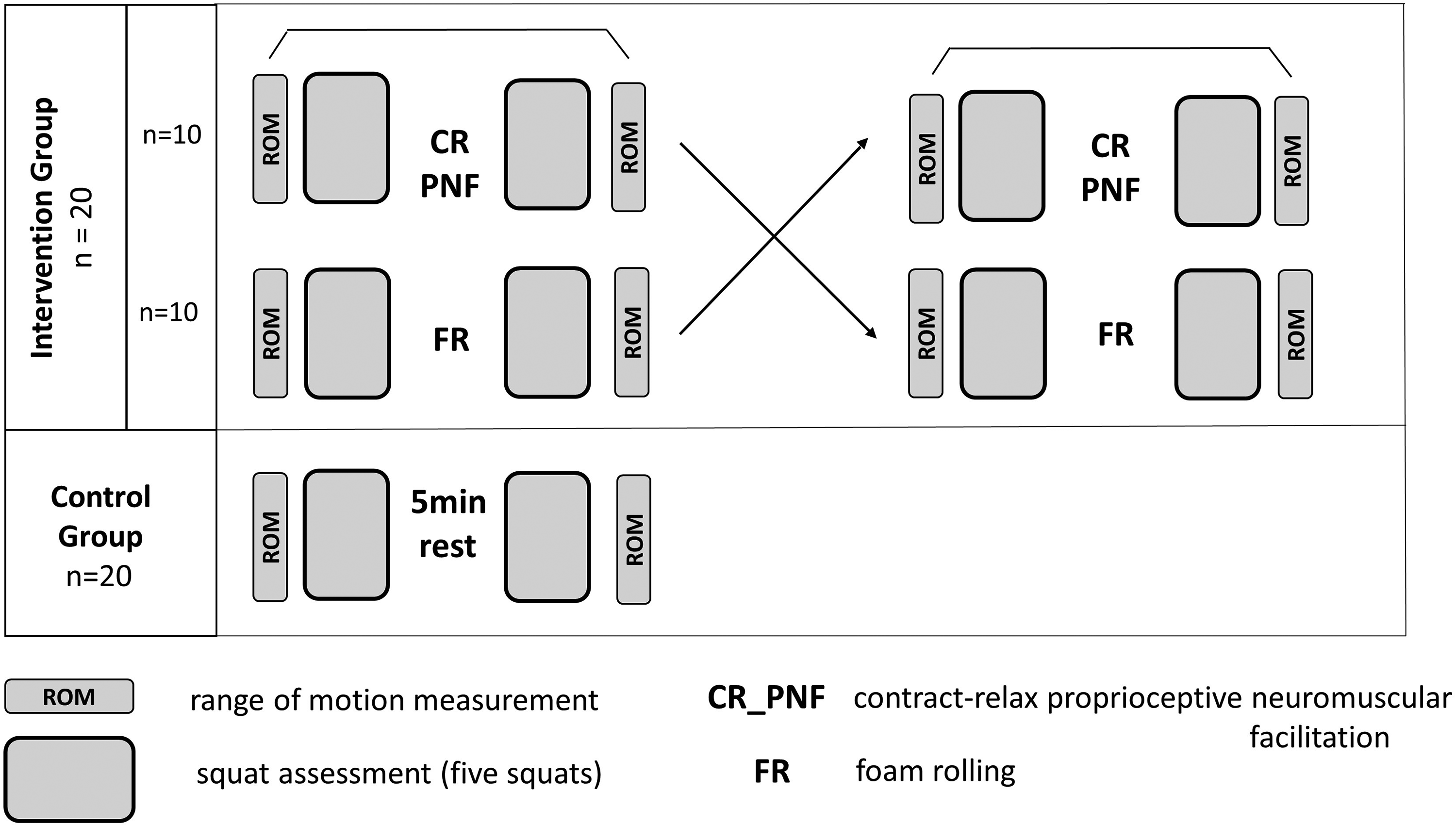
Schematic outline of the testing procedure, CR-PNF: contract-relax proprioceptive neuromuscular facilitation intervention, FR: foam rolling intervention.
Participants
A power analysis (g*power 3.1) 29 ), assuming at least a medium effect to achieve training relevance, claiming a minimal power of 0.90 when correlations are around 0.60 in a repeated measures design, proposed a sample size of 25 participants for inner-subject comparisons. Regarding comparisons to the control group (2 groups, 2 measurements), 36 participants were proposed. Striving for a stable squat performance, physically active individuals were sought. A convenient sample of forty students from the Department of Sports Science at the University of Innsbruck was recruited. All subjects were healthy and free of injury for at least six months. Twenty participants served as a control group (age: 24.4 ± 2.1 y, height = 171.6 ± 6.7 cm, weight = 70.6 ± 10.7 kg; (M ± SD)), while the other 20 participants underwent both interventions (age: 24.2 ± 2.8 y, height = 172.0 ± 10.3 cm, weight = 68.1 ± 12.0 kg; (M ± SD)), all groups were gender balanced. Ten students from the intervention group started with FR, and the other ten with PNF stretching. The participants performed the two intervention conditions with at least one week in between. All participants were informed about possible risks and gave written consent to participate.
Testing procedure
Each test session started with a two-minute low-intensity warm-up on an ergometer (50 W, 50–60 rpm). Afterward, baseline measurements of ankle dorsiflexion and hamstring ROM were taken from all participants at each visit. Then, participants performed two sets of five unloaded back squats using a gymnastic bar for positioning. Between the two sets, the intervention or control situation took place. Instantly following the last set of squats, ROM was assessed again. After each set of squats, the subjects’ motion experience was documented with a perception questionnaire. The intervention group was evaluated using a cross-over design on two different days. Figure 1 provides a schematic outline of the testing procedure.
ROM assessment
Functional ankle ROM was determined using the Weight-Bearing Lunge Test (WBLT), which has been shown to have high inter-rater (r = 0.99) and intra-rater (r = 0.98) reliability and has been used by other researchers before.30,31 Starting with the foot ten centimeters back, perpendicular to a wall, participants then flexed their knees until they reached the wall. For a successful attempt, the knee touched the wall and traveled over the foot's midline, and the heel had to stay firmly on the ground. 31 The test was invalid if heel movement, displacement, or lift-off occurred, which the test instructors carefully monitored. Participants were allowed to counterbalance their body position by using two fingers of each hand at the wall. The distance between the big toe and the wall was measured with a ruler attached to the floor. The furthest distance after five attempts was recorded. The test was conducted using both the right and left leg; the average of the maximum distance reached with each leg was used as the test outcome.
The Stand and Reach Test (SaR) was performed on a bench using an appropriate panel to measure the hamstring muscle flexibility. This test has previously been reported to meet reliability (r = 0.88–0.98) and objectivity criteria (r = 0.95–0.98) 32 and has been used by other researchers investigating the effects on muscle flexibility. 14 Participants stood barefoot on a wooden bench, feet together, legs extended, and toes touching the test panel. Then, participants bent forward as far as possible, still keeping their legs extended, touching the test panel with their fingers, and holding for 2 s. Two trials were conducted with a short rest in between (10–15 s). The best trial of the two attempts was recorded at the farthest position on the vertical scale (above or below the toe-line). Distance above the toe line (0 line) was indicated with a minus, while data below indicated a plus. Half of the intervention group started with the WBLT measurement, the other half with the SaR test.
Squat assessment
To avoid influencing each individual's movement pattern (timing, speed, depth, and performance), no detailed instructions on squat performance were given. However, according to the National Strength and Conditioning Association, an image series of a barbell back squat was shown to the participants before their first set, and they were advised to perform a smooth and continuous movement as they would usually do. An 8-camera motion tracking system with a sampling rate of 250 Hz (Vicon Bonita B10 with Nexus 2.2.4 software; Vicon Motion Systems Ltd, Oxford, UK) was used to record the trajectories of 40 spherical reflective markers. These markers were attached to the volunteers according to the “Plug-In Gait” marker setup (Vicon Motion Systems Ltd, Oxford, UK), with an additional marker positioned at the end of the sacrum. This marker (SACR) was attached to illustrate the pelvis tilt during the squat movement. The magnitude of the error of the Vicon system in a dynamic task is less than two millimeters, 33 which ensures high accuracy for recording angular changes. Data for movement perception of squatting was collected with a questionnaire consisting of three items regarding “easiness” (easy to demanding), “smoothness” (smooth to discontinuous), and “enjoyment” (pleasant to unpleasant). Each item was reported on a ten cm VAS.
Interventions
The FR intervention consisted of rolling the hamstring and calf muscles on both sides using a polypropylene foam roller (length: 29,5 cm, diameter: 14,8 cm, BLACKROLL AG, Bottighofen, SUI). Starting with the hamstring muscles of the right side, FR was performed unilaterally for three bouts of 30 s, with ten-second rest intervals, for a total time of two minutes. Afterward, this procedure was repeated on the left hamstring muscle group, followed by the calf muscles, starting again with the right side. Participants were instructed to start seated with their legs extended, their feet relaxed, and crossed with the foam roller just below their ischial tuberosity, with their leg maintained in an extended position. Then, lifting the pelvis off the floor and placing force on the roller, participants rolled down until they reached their popliteal fossa in a slow, continuous motion. A time-based rhythm was enforced to reduce variance in the rolling technique – rolling down in three seconds and back to the starting position in one, 31 repeating this process until the time had elapsed. Subsequently, subjects were instructed to place the top of their calf on the roller. Again, putting pressure on the foam roller with the calf muscle group and the arms supporting the body, subjects actively rolled down to the Achilles tendon insertion and back up in the same cadence as previously mentioned. The amount of exerted pressure was standardized using a value of six to seven on a numerical rating scale (0 = no discomfort, 10 = maximal discomfort) as used in previous literature. 34 Markers were already attached to the body at this point. In case exposed markers fell off, the intervention of rolling or stretching was fully completed before the marker was attached again.
PNF-stretching exercises were performed in the “contract-relax” type, similar to the procedures of previous studies.4,7,35 After a 30-s self-applied passive static stretch, participants conducted a five-second isometric contraction against resistance with 70% of their individual's maximal force, which was then followed by relaxation and another 30-s passive static stretch. The 70% maximum effort was approximated with guidance, but no measure of the actual degree of contraction was taken. Four repetitions of each stretch were performed with no rest between repetitions to maintain an equivalent time to the FR intervention. The intervention was performed unilaterally and was executed first on the hamstring muscle group, alternating sides before stretching the calves, always starting on the right side. Participants were encouraged to hold a position of six to seven on the numerical rating scale, where five represents the onset of pain but achieving maximum stretch throughout the duration. 36 The duration of the stretches and intensity instructions were similar to those for FR to allow comparisons between treatments. The total time required to complete the CR-PNF-stretching treatment per muscle was approximately 140 s. The hamstring muscle group was stretched with the participant standing upright placing one leg with the heel on a chair and knee extended. For the isometric contraction, participants were then instructed to push the heel down into the chair and towards themselves with a slight bend in the knee to achieve a hamstring contraction. Subsequently, the hamstring muscles were stretched by straightening the leg again and leaning forward. Participants were instructed to keep their backs straight and lean forward from the hip with an anterior tilt in the pelvis to avoid compensation with the spine. Calf muscles were stretched, standing on the edge of a stepper on the balls of the feet and dropping down the heels. Participants pushed off their toes for contraction, keeping an isometric contraction at around 70% of their maximum capacity. For balance, subjects were allowed to assist themselves with their hands on the wall.
The volunteers in the control group performed the first set of unloaded back squats, rested for five minutes, and then performed the second set.
Data analysis
The marker trajectories were reconstructed, and appropriate software filled timeline gaps (Nexus 2.2.3, Vicon Motion Systems Ltd, Oxford, UK). Further data processing was implemented using a custom software in Matlab® (The MathWorks Inc., Natick, MA, USA). A single squat cycle was defined as participants starting in an upright position, moving downwards, and returning to the upright position. As depicted in Figure 2, ankle, knee, pelvis, and trunk joint angles were calculated from marker positions. The ankle, knee, and trunk angular variables were averaged between both sides. The trunk angle represented the angle between the upper body and thigh (UBTH). The mean of the minimal (ankle, knee, UBTH) and the maximal (pelvis) angles out of five squats were determined as target variables for the statistical analysis.

Marker positioning and angles defined for squat assessment.
Statistical analysis
Data are expressed as mean (M) ± standard deviation (SD). Data distribution was assessed by applying the Shapiro-Wilk test, the homogeneity of groups was evaluated using the Levene-Test, and variance analyses with repeated measures (rANOVAs) were conducted. First, evaluating a possible order effect, rANOVAs of ROM measurements with two repetition factors (pre-post and stretching method CR-PNF vs. FR) and one grouping factor (CR-PNF first or FR first) were calculated for ankle mobility and hamstring flexibility, respectively. All effects showed independence of the intervention sequence. Therefore, CR-PNF and FR intervention measurements were each pooled, discounting whether CR-PNF or FR intervention was implemented first and regarded as independent conditions. Now, rANOVAs with two repetition factors (pre-post, CR-PNF_FR) were conducted to evaluate the intervention effect on ROM for ankle and hamstring flexibility, respectively. For comparisons of intervention effects with the control group, 2 by 2 rANOVAs (pre_post, group) were calculated. If the normality of data was violated, Mann-Whitney U-Tests and Wilcoxon Tests were calculated to compare stretching effects between the intervention group and control group, as well as between the different stretching interventions. Pairwise comparisons’ p-values are reported Bonferroni corrected for three comparisons.
To evaluate the effect of increased ROM on squatting execution, 2 by 2 rANOVAs of all angle variables were conducted separately with the repetition factor pre_post and a between factor of groups. Finally, all angle variables were compared pre-post intervention within CR-PNF and FR condition. VAS scores of reported perceptions were likewise analyzed using rANOVAs for easiness, smoothness, and enjoyment. Effect sizes are reported utilizing partial eta squared with effects between 0.01 and 0.06 considered small, above 0.06 as moderate, and higher than 0.14 as large, 37 and Cohen's d in case of pairwise comparisons, 29 with effects considered small below 0.50, medium between 0.50 and 0.80, and large above 0.80. The significance level was set to p ≤ 0.05. All analyses were performed using SPSS version 26.0 (Somers, NY, USA).
Results
Range of motion
ROM of ankle dorsiflexion measured with the WBL test (Figure 3) showed a significant interaction effect of the pre-post * intervention, (F(1,19) = 7.68, p = 0.036, η2p = 0.29), favoring FR with significant pre-post changes for the intervention group (CR-PNF: p = 0.021, d = 0.71; FR: p < 0.002, d = 1.2 respectively) but not for the control group (p = 0.627). Further, the analysis between groups showed a significant difference between the FR intervention and control group (p = 0.006, d = 1.2); however, there was no difference between the CR-PNF intervention and controls (p = 0.667).
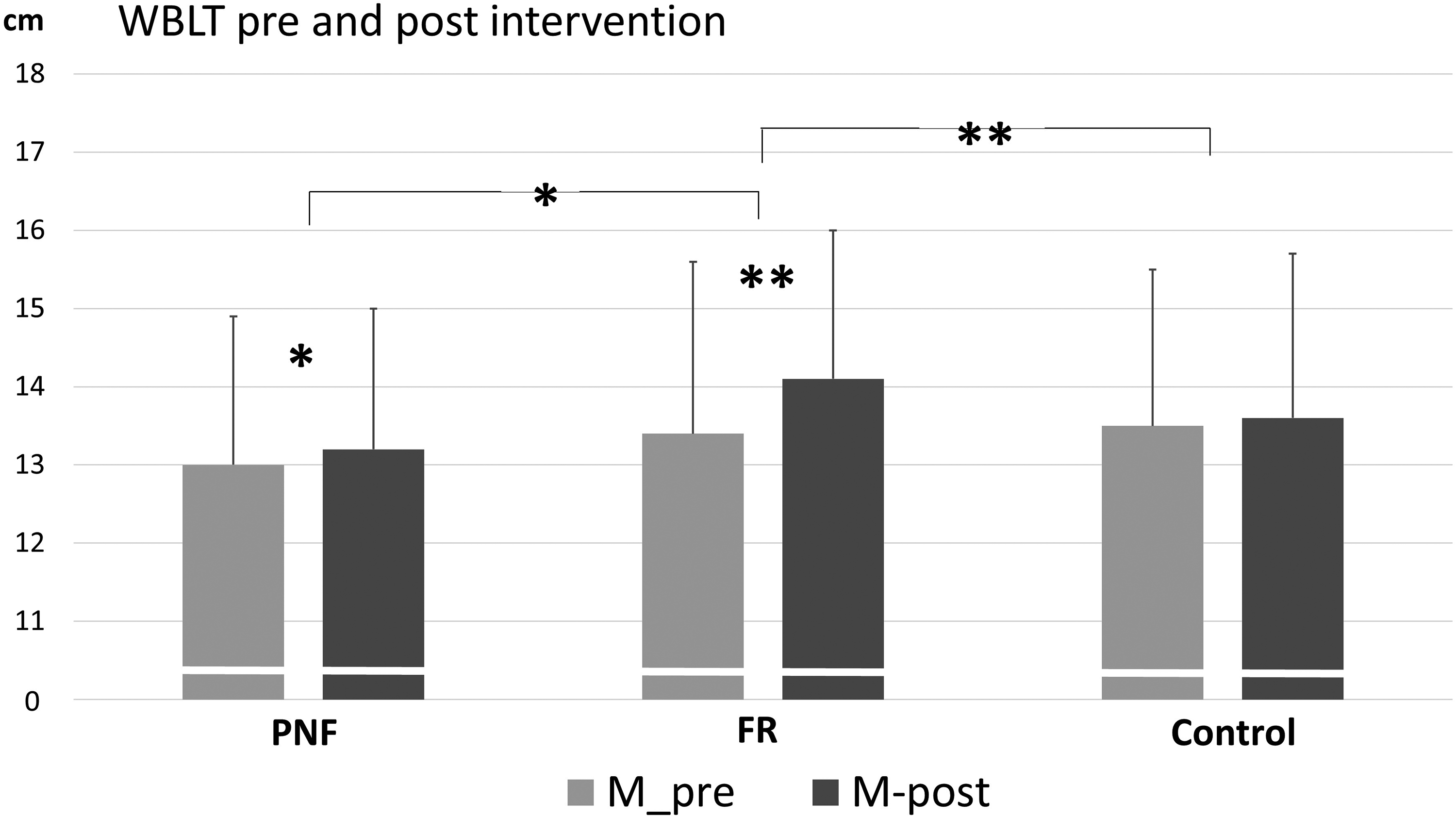
Results of the Weight-Bearing Lunge Test (WBLT) pre and post-intervention, distance to the wall in [cm], (**) represents significant differences p < 0.01, (*) represents significant differences p < 0.05, Bonferroni-corrected for PNF versus FR. PNF: contract-relax proprioceptive neuromuscular facilitation; FR: foam rolling.
A significant pre-post increase in the SaR test (Figure 4) was found for both interventions but no interaction effect of pre-post and intervention occurred (F(1,19) = 70.55, p < 0.001, η2p = 0.79, F(1,19) = 2.76, p = 0.114, η2p = 0.13, respectively). The between-groups analysis revealed that the improvement in flexibility was significantly more pronounced after CR-PNF stretching than in the control group (F(1,38) = 14.67, p < 0.003, η2p = 0.28), and no significant difference between FR and the control group (F(1,37) = 5.37, p = 0.078, η2p = 0.13).
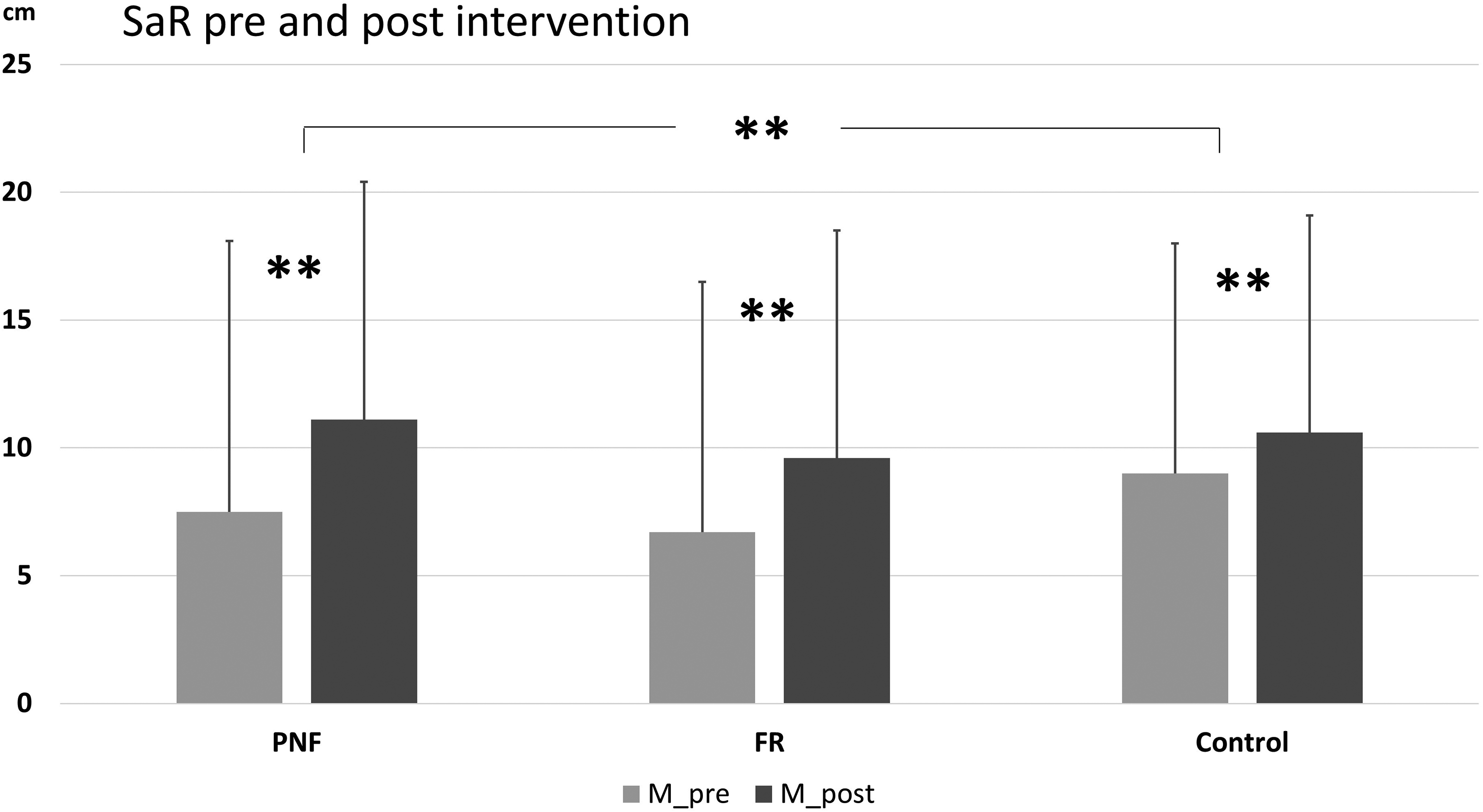
Results of the stand and reach test (SaR), (**) represent significant differences (p < 0.01).
Angles
Examples of knee angle changes after CR-PNF stretching of two participants are shown in Figure 5. Regarding the comparison of the two interventions, no differences in changes could be detected (ankle: F(1,19) = 1.48, p = 0.238, η2p = 0.07; knee: F(1,19) = 0.49, p = 0.491, η2p = 0.03; UBTH: F(1,19) = 0.29, p = 0.597, η2p = 0.02; pelvis: F(1,19) = 1.43, p = 0.247, η2p = 0.07). Regarding all participants, both interventions showed no effect compared with the control group (see detailed results in the Appendix). Although both interventions increased ankle dorsiflexion and hamstring flexibility in the SaR test, the mean minimum value of each angle and the mean maximum pelvis tilt did not change during the subsequent set of squats. If any trend, but more likely regarding FR intervention than CR-PNF stretching compared to the control group, ankle angle minimum (FR pre-post*group: F(1,38) = 2.19, p = 0.147; η2p = 0.06) and knee angle minimum (FR pre-post*group: F(1,38) = 3.51; p = 0.069; η2p = 0.09) showed at least moderate effect sizes but missed significance. The mean forward lean of the trunk (UBHT angle) was significantly lower in the control group than in the intervention group throughout the measurements (F(1) = 6.89 for CR-PNF and 6.99 for FR; p = 0.012, η2p = 0.15 for CR-PNF and 0.16 for FR, respectively).
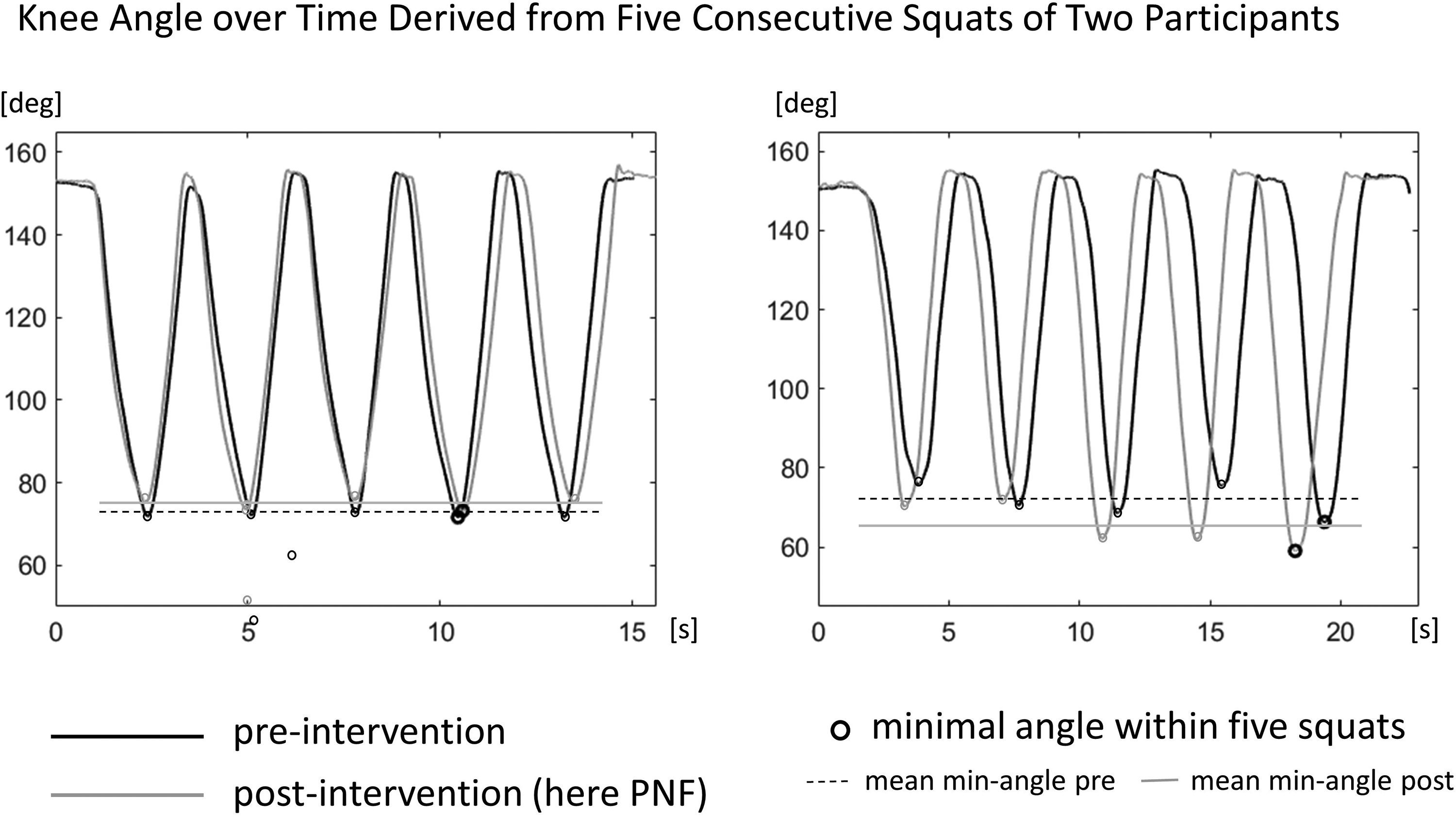
Two examples of the knee angle during five consecutive squats pre- (black) and post-intervention (gray line) for two participants. It shows the minimal knee angle within five squats and the mean of five minimal angles for pre- and post-intervention.
Squat perception questionnaire (VAS scores)
After the second set of squats, all groups reported significantly enhanced perception of ease, smoothness, and enjoyment (p < 0.001) in their motion. Although participants after the CR-PNF-stretching intervention demonstrated the most remarkable rise in all variables, no statistical differences were observed between the groups (Table 1).
Results of the movement perception of the squat series on an analog visual scale (0 easy, very smooth, pleasant to 10 cm demanding, discontinuous, unpleasant respectively) pre and post-intervention. All pre-post comparisons show significant differences.
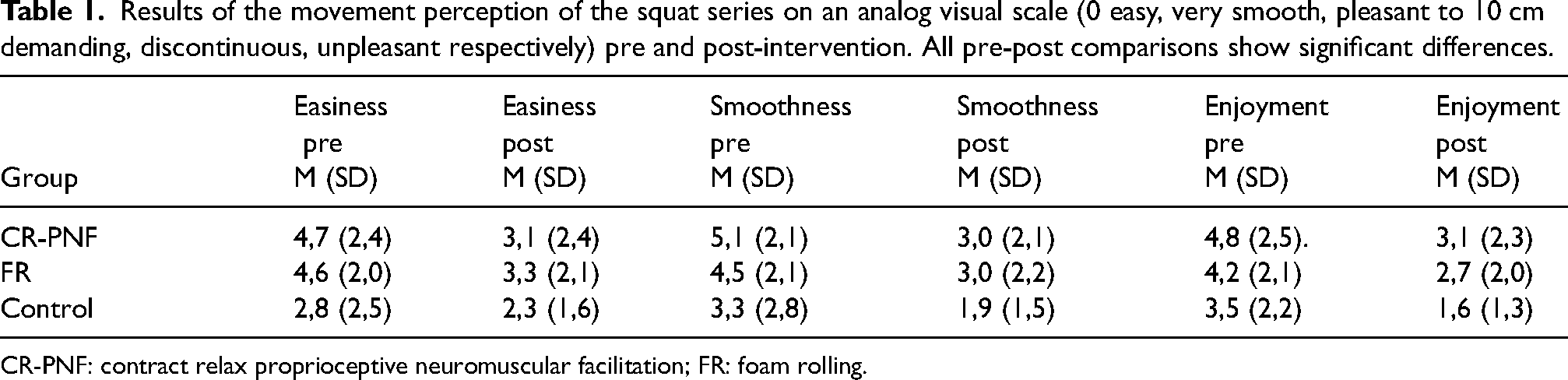
CR-PNF: contract relax proprioceptive neuromuscular facilitation; FR: foam rolling.
Discussion
This study investigated the effects of CR-PNF stretching compared to FR and their impact on subsequent movement performance. CR-PNF stretching and FR targeted ankle and hamstring ROM, and effects on squatting were assessed. As expected, CR-PNF stretching and FR improved ankle and hamstring ROM compared to a control group. However, the raised ROM did not change the movement patterns of squatting.
CR-PNF-stretching and FR interventions on the lower extremities significantly increased ROM in our study. This has already been stated in the literature for CR-PNF8,38 and FR.13,20,22 The direct comparison of CR-PNF and FR intervention effects on ROM of ankle and hamstring flexibility revealed larger effect sizes of FR regarding ankle dorsiflexion (WBLT). In contrast, CR-PNF effect sizes exceeded FR in hamstring ROM (SaR), however, without reaching statistical significance between the two interventions. A meta-analysis of stretching intervention studies 39 found that FR and stretching interventions reach comparable outcomes on ROM, supporting our results in summary. Regarding effect sizes, our results on ROM tentatively suggest that FR could be favored for stretching the calf muscles, whereas CR-PNF might be more effective in hamstring stretch. These results coincide with recent findings, where two minutes of CR-PNF and FR intervention on hamstring muscles showed a significantly higher increase of ROM for the CR-PNF intervention. 40 On the other hand, Konrad et al. 19 reported a significantly higher effect of FR on the calves, whereas hamstrings were indifferent. Longer treatment duration (> the 60 s) was reported to favor the FR effect, 19 which again supports our results of FR on WBLT.
A plausible mechanism for gaining ROM after CR-PNF stretching is the Golgi tendon organs (GTOs) activation. Because of the contraction at the elongated state, the afferent Ia fibers of the musculotendinous unit decrease the activation of the GTOs and, therefore, reduce the nociception or pain sensed, allowing for a greater ROM and greater force production.8,36,41 In FR, pressure, stretch, and friction between the tissue and the foam roller cause tissue warming, promoting a more fluid-like form of the tissue. 42 Adaptations in FR can be seen, besides others, in a more efficient muscle activation due to increased type Ib afferents activity, leading to greater proprioceptive feedback from the muscle.16,17 Both mechanisms might interfere with converting proprioceptive information to muscle commands when performing complex movements like squatting. Surprisingly, there was no significant change in maximal joint positions (minimal angles during squatting nor maximum pelvis tilt) pre and post-intervention. A recent study 43 found that FR improves the knee joint position sense, whereas the force sense was not modified. The force sense might possibly guide the depth of the squats, and therefore, no angle trajectory changes might have occurred in our study. Although flexibility increased significantly in ankle dorsiflexion and hamstring flexibility after FR or CR-PNF stretching, this greater mobility was not implemented in the subsequent squat movement. A possible weakening over time of CR-PNF-stretching or FR effects can be ruled out since ROM measurements were taken after the last set of squats and, therefore, raised ROM must have been present during the movement execution. Whereas older adults exhibited improvements in step length of gait resulting from increased pelvis rotation and tilting ROM after stretching,44,45 our participants could not gain enhancement in squatting technique despite enhanced ROM.
In contradiction to our results, FR interventions, which exceed 90 s, elevated scores in overhead deep squatting (in the framework of the Functional Movement Screen). 46 The duration of FR or stretching intervention is assumed to play an important role.19,46 Our time demands of FR and CR-PNF intervention passed 2 min per muscle, this is exceeding 90 s, but did not affect the squat movement execution. Despite higher accuracy in the squat assessment provided in our study, results could not detect movement performance changes. Measuring the maximum angles of involved joints avoided scoring bias, which might be present in. 46
The results of our study indicate that well-known movement patterns are more likely represented by time-spatial goals without solely depending on proprioceptive feedback. In addition, our results suggest the existence of a preferred movement path for squatting, where the movement pattern remains unchanged even when altered ROM is present. This observation corresponds to the “preferred movement path concept” postulated by Nigg et al. 47 for shoe-effects in running. Furthermore, the short-term intervention effect established only small angular changes, which might have been too small for squatting adaptation in regular flexible participants.
Lastly, we demonstrated a significant change in the reported feeling of squatting pre- and post-interventions (measured by VASs). CR-PNF-stretching and FR, accompanied by improved ROM, possibly led to enhanced proprioception based on physiological responses.9,10,48 However, the increase in all variables of comfort between the first and second set of squats in all groups was significant and might be due to a greater familiarization with the execution of the movement pattern. Despite this, there was no significant difference in the magnitude of change between all groups, the control group inclusively. Higher ROM in ankle dorsiflexion and hamstring flexibility did not lead to a different squatting experience. Changes seemed provoked by performing the first set of squats, maybe remembering the fine-tuning of muscle coordination in the set repetitions, which might have reduced overall effort.
Limitations
The direction of gaze during squatting was not recorded. Donnelly et al. 49 found that mean maximum trunk-, hip- and knee flexion were greatest when the gaze direction was directed downward. The reported difference between upward and downward gaze was about nine degrees, which is about the same as our study's maximum individual angular changes. In retrospect, more explicit instructions about squat performance (deepness and gaze) might have improved the standardization in our research. Such instructions could be something to heed in future studies investigating angular motion changes resulting from changed ROM.
The squats were performed without load. The additional load might have potentiated recognition of increased ROM and then influenced results, which is also why we favored the bodyweight squat.
In terms of technical limitations, markers occasionally fell off during interventions or due to sweat. This could have introduced some errors in kinematic data, as our analysis relies on the exact placement of markers when calculating angles and planes. However, all cases were reported and documented, and the number of incidents was limited.
Regarding the selected population, the subjects in this study were all active young adults with comparably good knowledge of performing the squat. Therefore, the results should not be generalized to other less experienced individuals or age groups.
Conclusion
Significant short-term effects on the ROM of ankle dorsiflexion and hamstring flexibility were observed after CR-PNF-stretching and FR intervention in ROM tests; however, no alteration of movement patterns in squatting was detected. This suggests that warm-up stretching is unlikely to adversely (or beneficially) affect movement execution in squatting. Thus, it also suggests that acute warm-up stretching effects are insufficient to improve an incorrect execution of squatting movements through greater ROM. Future studies might focus on more prone ROM differences or on long-term effects.
Consequently, warm-up strategies, including CR-PNF or FR, do not affect consecutive movement execution like squatting. This implies that movement patterns depend on convenient joint angle ranges rather than maxima or minima.
Footnotes
Acknowledgments
We want to thank the participants for their dedication to the measurements, Armin Niederkofler for his technical support, and Thomas Haid for analysis programming.
Author contributions
Conceptualization, FD; methodology, FD and IW; validation: FD, PF and IW; investigation FD and IW; writing – original draft preparation IW and FD; writing – review and editing, PF, IW and FD; visualization IW, project administration FD and IW All authors have read and agreed to the published version of the manuscript.
Consent to participate
All participants provided written informed consent prior to participating.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical considerations
The Institutional Review Board has granted the study ethical approval (certificate 13/2020) in accordance with the declaration of Helsinki and the ethics commission of the University of Innsbruck.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
APPENDIX
Comparison of angle changes between the intervention group and the control group
regarding CR-PNF – interaction of pre-post*group
ankle: F(1,38) = 0.03, p = 0.869, η2p < 0.01 knee: F(1,38) = 1.46, p = 0.234, η2p = 0.04 UBTH: F(1,38) = 0.19, p = 0.665, η2p < 0.01 perlvis: F(1,38) = 0.02, p = 0.896, η2p < 0.01 regarding FR – interaction of pre-post*group
ankle: F(1,38) = 2.19, p = 0.147, η2p = 0.06 knee: F(1,38) = 3.51, p = 0.069, η2p = 0.09 UBTH: F(1,38) = 0.01, p = 0.915,
η2p = < 0.01 pelvis: F(1,38) = 0.02, p = 0.895, η2p < 0.01