
Abstract
Elite soccer players consistently report using several recovery methods after practices and games. However, it is unclear how their subsequent performance could be enhanced using broad protocols. The aim of this study was to compare the effectiveness of two different comprehensive recovery protocols in physiological, neuromuscular, and perceptual outcomes. Eighteen Mexican National Team players (19.56 ± 0.62 years) were recruited. Using a randomized parallel group design, players followed one of two recovery protocols: (a) carbohydrate and protein shake, foam roller, cold-water immersion, and tart cherry juice concentrate (n = 9) or (b) carbohydrate and protein shake, stretching, and intermittent cold-water immersion (n = 9) following the completion of an unofficial game and the day after. Muscular creatine kinase, countermovement jump, hamstring maximal voluntary contraction, perceived recovery, and muscle soreness were assessed before, immediately after, and 20-44-68 h post-game. Significant effects (set at ρ≤0.05) of time were present in both interventions. Muscular creatine kinase was normalized entirely at 68 h post-game, while neuromuscular and perceptual outcomes were homogenized at 44 h. No statistically significant effects between protocols were found. Still, the interaction effects showed changes only in the group using protocol (a) at post-game and 20 h after in neuromuscular and muscle soreness. There were large correlations between muscular creatine kinase and accelerations, decelerations, sprints, and high-speed running distances. In conclusion, the interventions are equally effective for improving physiological, neuromuscular, and perceptual outcomes. Thus, elite soccer players may benefit from different combinations of methods after practices or games to obtain positive effects on recovery after them.
Keywords
Introduction
Soccer is a complex, strenuous contact team sport characterized by unpredictable intermittent activity patterns interspersing low and high-intensity efforts with passive or active recovery. 1 From an organizational point of view, elite professional soccer is defined as a medium-density sport where the average player is exposed to high-congested fixture periods with a mean of 60 competitive games per season, 5.5 per month, 1–3 per week, or one every 4.3 days. 2 Frequent national team participation during the competitive season and travel issues may create an even more complex scenario to achieve a proper recovery before competitions.3,4 This accumulation of events, games and training sessions, combined with reduced recovery time between all these activities results in potential underperformance. 3 Thus, the ability to recover after competitive or intense training bouts is important to maintain or increase performance in subsequent efforts. 5
Soccer-related physical performance is immediately impaired after a game and recovers to the previous levels gradually. 6 After a single game, total normalization of performance parameters such as sprint, jumping ability, or maximal strength is frequently observed after 72 h, 7 even with signs of biochemical and physiological stress. 8 However, when playing additional games during the week, subjective wellness values, perceived recovery, and physical performance parameters (e.g. sprint, jump, and strength) take longer, 96 h, to be normalized,9,10 which increases the need for recovery strategies. 11 Moreover, some external load parameters of the game, such as high-intensity distance covered (total and per minute), high-speed running distance (HSR), and the number of sprints were significantly correlated to a creatine kinase (CK) increase, a muscle damage marker, at 24-h post-game.12,13 These levels may remain increased for 3 days 14 and have to be considered as a basic marker that may be targeted by recovery strategies. 11 Therefore, quickly restoring pre-performance levels before the next competition is one of the main aims for soccer players. 15 Although protocols for specific soccer post-exercise recovery based on scientific evidence are available, 16 a gap exists between theory and practice in professional settings. The use of recovery interventions is not always based on research evidence, 17 which can negatively affect players’ recovery and limit the ability to provide new guidelines to professional standards. 18 Thus, deep knowledge about physical performance profiles, time courses, players management, personal approaches, and players’ awareness of recovery strategies post-practice/game can lead to faster performance recovery. 19
Currently, scientific literature presents many methods to enhance recovery based on the type of practice, the time between sessions or competitions, and equipment or staff availability. 15 According to data from elite professional soccer staffs, the strategies most frequently used after a competition are an active recovery, stretching, food/fluid intake, ergogenic aids, cold/ice bath/shower/immersion, massage, and foam rolling. 17 However, to our knowledge, only three scientific studies present positive effects when combining different recovery methods in soccer.20–22 Still, none of them have assessed the impact on health or performance, neither additive nor adverse effects in elite soccer players after a competition, although team staffs report combining more than one method when periodizing and performing recovery. 23 Therefore, the main aim of the current study was to compare the effectiveness of two comprehensive protocols on physiological, neuromuscular, and perceptual outcomes after an unofficial soccer game in elite players during a national team camp. It was hypothesized that a comprehensive recovery protocol combining more methods could speed up and be more effective in enhancing objective and subjective players’ recovery parameters. In addition, as a secondary aim hypothesis, the acute changes of muscular CK (CK-III) correlate with the global positioning system (GPS) external load variables recorded during the game.
Methods
Experimental approach to the problem and participants
Twenty elite male soccer players (mean ± SD: age = 20 ± 1 years; height = 178.8 ± 5.0 cm; body mass = 72.9 ± 6.1 kg) from the under 21 (U-21) Mexican National Team were enrolled in this study. The study used a convenience sampling technique to select players from the U-21 Mexican National Team, allocating the players to the two groups using a block randomization technique. 24 All players had more than 10 years of experience playing soccer and performed 5–7 full-team soccer training sessions for a total training load of approximately 8–10 h per week, with at least one official game. Participants completed a medical questionnaire and initial screening. None of them had any diseases, and they did not smoke, drink alcohol, or take stimulants or substances that potentially alter hormonal responses. No participant presented any severe lower limb muscle injuries 2 months before the research. To ensure that the load and the intensity imposed were representative and similar, goalkeepers and outfield players who did not complete the total training camp sessions were excluded from the final analyses. After receiving information about the study aims, possible risks, benefits, and requirements, participants signed a written informed consent. Every participant could withdraw from the study at any moment. The study was conducted following the Declaration of Helsinki and its later amendments and was approved by the Research Ethics Committee of the University of Vic-Central University of Catalonia, Spain (registration number: 123/2020).
Design
An interventional balanced (1:1) parallel group-randomized trial was conducted to determine the effect of the two recovery protocol interventions after a 90-min unofficial soccer game. In this professional context, establishing a comparison group (control) was not suitable. 24 The study was conducted during the FIFA International break (August-September 2021) as a training camp developed for 9 days in Mexico DF. Before any data acquisition, the participants performed 6 days of similar practices. Food and fluid intake were controlled individually by a nutritionist using a food diary. Players were instructed to avoid any strenuous exercise outside the training requirements nor modify usual sleeping patterns monitored and controlled, in quality 25 and duration. One familiarization session was developed to practice all the tests to ensure reliability, with a full explanation of the experimental protocols and testing procedures. Every participant had more than 1 year of experience using recovery methods and perceptual/well-being questionnaires. The outcomes were assessed on four different days (five time points). The first part of each testing session, except post-game, was designed to collect the players’ perceptual outcomes. Immediately after that, the team physician took blood samples from all participants. Before performing the neuromuscular tests, a 5-min standardized dynamic warm-up using several different running patterns at an increasing intensity, joint mobility exercises, and dynamic stretches followed by two submaximal jumps was implemented (Figure 1). The testing battery lasted 25 min for every group of four players. Three days after the game, players participated in the regular training routine of the training camp.
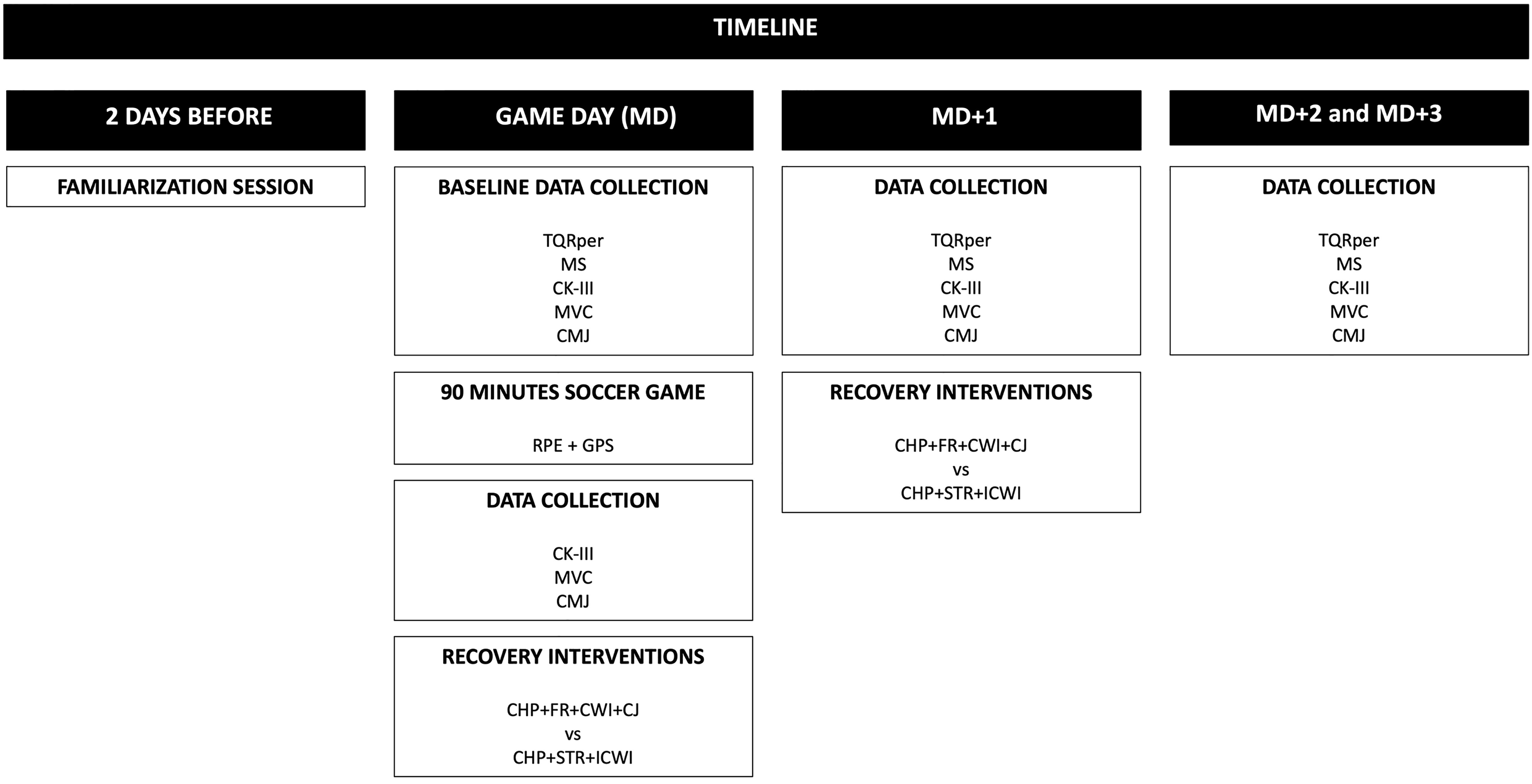
Protocol design timeline. CHP + FR + CWI + CJ: 250 mL of water with carbohydrate and protein, foam roller, cold-water immersion, and tart cherry juice concentrate; CHP + STR + ICWI: 250 mL of water with carbohydrate and protein, stretching, intermittent cold-water immersion; CK-III: creatine kinase muscular isoenzyme; MVC: hamstring maximal voluntary contraction; CMJ: countermovement jump; GPS: global positioning system; TQRper: total quality recovery perceived; MS: muscle soreness; MD + 1: 20 h after game; MD + 2: 44 h after game; MD + 3: 68 h after game; au: arbitrary units; RPE: rate of perceived exertion.
The primary researcher was responsible for the stratified randomizing, using players’ positions as the matching characteristic. Although being an unofficial game, licensed referees were present. Internal load data were collected after the game, using players’ perceived exertion (RPE) rate on a 1–10 scale .26,27 External data from the game were collected using valid and reliable WIMU® pro 10-Hz GPS devices (RealTrack Systems, Almería, Spain) which managed accelerometry data at 100 Hz. 28
Before the start of the study, the protocol was registered at https://clinicaltrials.gov (ID: NCT04716049; https://clinicaltrials.gov/ct2/show/NCT04716049). Moreover, CONSORT guidelines were followed to report data (supplementary material I).
Outcomes
The same researchers supervised all the testing procedures and conducted them in an open official soccer facility at a temperature of 19 ± 1°C and humidity of 65.5 ± 6%.
Physiological outcomes
Creatine kinase muscular isoenzyme III (CK-III or CK-MM). Venous blood sample collection for CK-III isoform ratio in serum determination involved players passively drooling directly into a plastic tube. Samples were sealed and maintained at ideal conditions until analyses were carried out. CK-III was separated from total CK and measured in U/L using an electrophoretic method. 29
Neuromuscular outcomes
Hamstring maximal voluntary contraction (MVC). Participants laid in a supine position, with the tested leg strapped around the ankle (in a neutral position), and performed a hip extension from 90° of hip flexion (with a slight knee flexion of 20°). The nontested leg was resting on the floor and was fixed by one member of the research team. This test was adapted from Matinlauri and colleagues by using a strain gauge instead of a force plate. 30 Players placed their hands on the wall to avoid sliding on the floor. A strain gauge was placed between the ankle strap and the cord to evaluate the force (MVC, measured in Newtons) exerted at a sampling frequency of 80 Hz (Chronojump, Boscosystem®, Barcelona, Spain). The tester gave all participants the exact instructions; “to exert maximal force down to the floor” and continuous and standardized verbal motivation for 5 s. Each limb (dominant and non-dominant) was tested three times, in a randomized order and the average values were used in the subsequent analysis. The assessment of both legs was separated by 30 s, while the time separating two trials of the same leg was 60 s. 30
Countermovement jump (CMJ) was performed using an Optojump® system (Microgate, Italy) with an accuracy of 1 kHz to determine the jump height (cm). For the CMJ, soccer players were required to bend their knees to approximately 90° angle and perform a maximal vertical thrust with the hands fixed on the hips. 31 Participants were instructed to keep their bodies upright throughout the jump and to land with their knees fully extended. Any jump that was perceived to deviate from the required instructions was repeated. Three trials were allowed, and the average values were used in subsequent analysis. 32 A 30-s passive recovery was provided between jumps. 33
Perceptual outcomes
Total quality recovery perceived (TQRper). Players were asked to rate their recovery perception using the subjective validated TQRper questionnaire answering, “How recovered do you feel?”. A scale ranging from 0 (very poorly recovered) to 10 (very well recovered) was used as a subjective measurement to assess fatigue. 34
Muscle soreness (MS) was collected using a 5-point validated scale, with 5 being the best state and 0 being the worst. 25
Procedures
After the soccer game, players were randomly assigned to one of two intervention groups: a carbohydrate and protein shake, foam roller, cold-water immersion, and tart cherry juice concentrate (CHP + FR + CWI + CJ) or a carbohydrate and protein shake, stretching, and intermittent cold-water immersion (CHP + STR + ICWI).
Both included a combination of natural and physical recovery methods and were performed twice, immediately after the game and the day after (20-h). All players drank a maximum of 500 mL of an isotonic sports drink and water “ad libitum” during the game.
“CHP + FR + CWI + CJ” intervention
Players drank 30 mL of CJ 35 and 250 mL of water with carbohydrates and protein within 30-min of completing the game; performed the foam rolling exercises using a polyvinylchloride pipe roller of 10.3-cm diameter and 0.3-cm thickness surrounded by a 1.5-cm thickness neoprene foam. 36 They were instructed and supervised to begin with the foam roller at the most proximal portion of the muscle and to roll as much body mass as tolerable from proximal to distal as smoothly as possible at a cadence of 1 s superior and 1 s inferior determined with a metronome. The foam roller activity was performed for 45 s, followed by a 15-s rest for each muscle group and in the same order (quadriceps, adductors, hamstrings, abductors, and gastrocnemius) in each lower extremity and repeated once. This protocol concluded with a cold-water immersion (CWI) where players immersed their lower body (up to the iliac crest) for 10 min in cold water (13–14°C) 37 inside a pool. Researchers closely monitored the water temperature every minute to maintain it.
“CHP + STR + ICWI” intervention
Players drank 250 mL of water with carbohydrates and protein within 30 min of completing the game. They performed 10 min of static stretching, involving two unilateral repetitions of 30 s, holding stretches to the quadriceps, adductors, hamstrings, abductors, and gastrocnemius muscles in each lower extremity. 38 An investigator supervised players during the stretching exercises. Intermittent cold-water immersion (ICWI) was the last recovery method used in this protocol. It consisted of five 2 min of intermittent immersions of the lower limb (up to the iliac crest) in a cold-water bath (13–14°C), separated by 2 min of rest in ambient air 39 using a fixed pool. Investigators closely monitored the water temperature every minute and monitored the 2-min immersions.
Statistical analyses
Data were presented as mean ± SD (or SE as stated) and 95% confidence intervals (CIs). Within-participant reliability of test measures (intra-session repeated efforts) was analyzed using the two-way random intraclass correlation coefficient (ICC) and coefficient of variation (CV). ICC values were >0.9 excellent, 0.9–0.75 good, 0.75–0.5 moderate, and <0.5 poor, and CV values were considered acceptable if <10%.
Independent samples t-test was used to check for baseline between-group differences in participants’ characteristics and GPS outcomes. Cohen's d (mean difference/pooled SD) was reported for the analyses and interpreted as follows: <0.2 trivial; 0.2–0.5 small; 0.5–0.8 medium; >0.8 large.
The relationships among variables were analyzed using a linear mixed model (LMM) for continuous data and a generalized linear mixed model (GLMM) for categorical data. Both models considered the individuals as a random effect, and the time of testing (time) and the recovery strategy used (group) as fixed effects. Mean and interaction effects were represented by the F for LMM and the chi-squared (χ2) for GLMM. The GLMM used gamma distributions with identity as a link function. Estimated marginal means from LMM and GLMM with 95% CI were used to consider the effect of each factor. For those significant factors (p < .05), a post hoc test with Holm adjustment was used to evaluate the interaction effect and the main effect of time or group. No missing data was present in the study. Still, two participants, one from each group, could not complete the study due to injuries that occurred during the game (see supplementary material II). Thus, 18 participants (CHP + FR + CWI + CJ = 9, CHP + STR + ICWI = 9) were finally included in the final analyses.
Pearson correlation coefficients were used to analyze the relationship between CK-III changes (pre- to post-game) and GPS game data. The magnitude of the relationships (r) was interpreted as follows: <0.1 trivial; 0.1–0.3 small; 0.3–0.5 medium; 0.5–0.7 large; 0.7–0.9 very large; and >0.9 extremely large.
Statistical analyses were conducted using the statistical package JASP for Macintosh (version 0.16.1, University of Amsterdam, Netherlands).
Results
Both groups had similar physical characteristics and game demands (p > .05; trivial to small effects, see supplementary material III). The reliability measures were for the CMJ (ICC = 0.90; 95% CI [0.82–0.95], CV = 4.6%; for the MVC (dominant) (ICC = 0.84; 95% CI [0.72–0.92], CV = 8.8%) and for the MVC (non-dominant) (ICC = 0.85; 95% CI [0.74–0.93], CV = 7.8%).
Main effects and interaction effects
The results from the LMM and GLMM are shown in Tables 1 and 2 and Figure 2. The main effect of time was large (p < .001, F > 6.99; and χ2
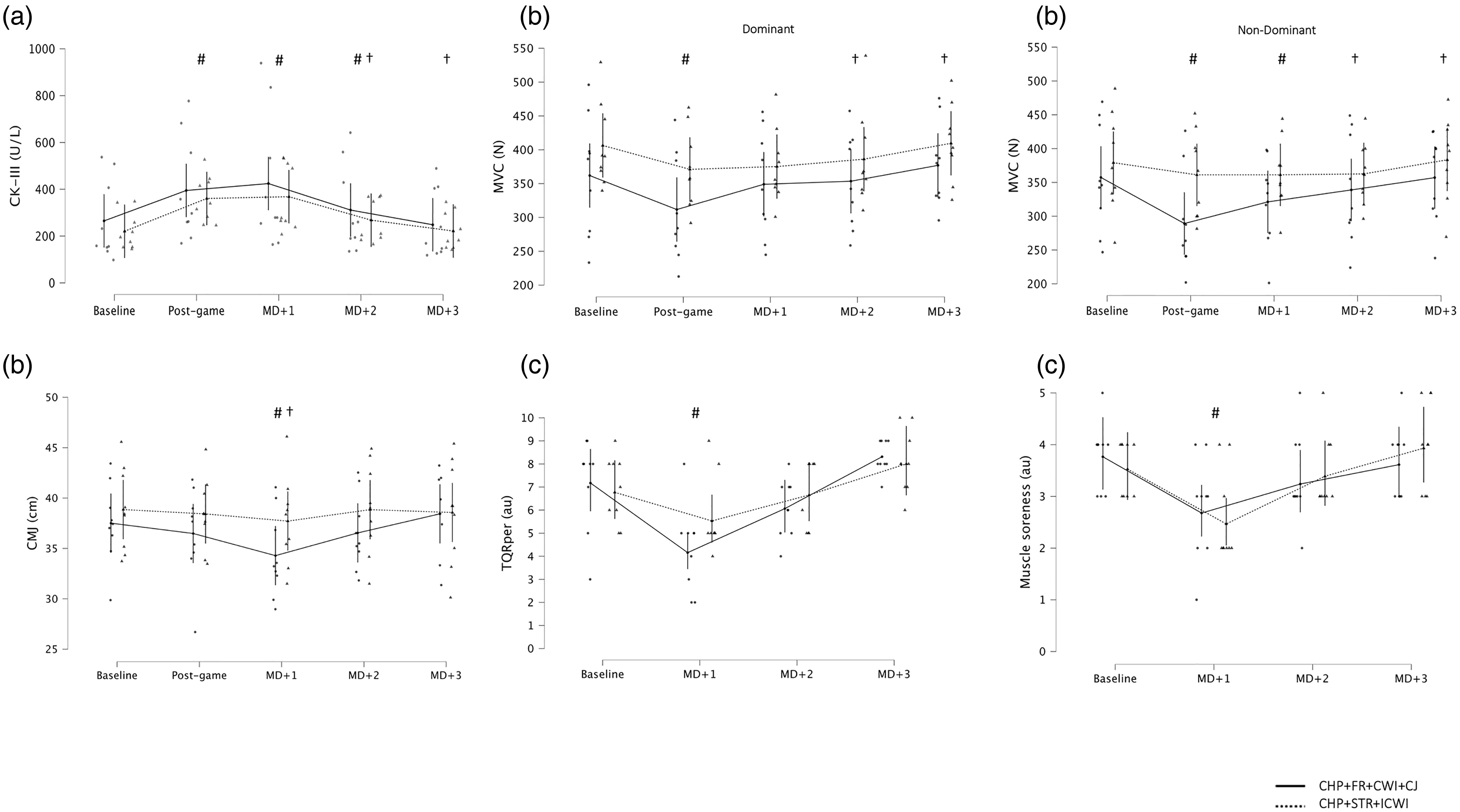
Physiological (a), neuromuscular (b), and perceptual (c) outcomes. CHP + FR + CWI + CJ: 250 mL of water with carbohydrate and protein, foam roller, cold-water immersion, and tart cherry juice concentrate; CHP + STR + ICWI: 250 mL of water with carbohydrate and protein, stretching, intermittent cold-water immersion; CK-III: creatine kinase muscular isoenzyme; MVC: hamstring maximal voluntary contraction; CMJ: countermovement jump; TQRper: total quality recovery perceived; MS: muscle soreness; MD + 1: 20 h after game; MD + 2: 44 h after game; MD + 3: 68 h after game; au: arbitrary units. Notes: # different from baseline. † different from post-game.
Results from the linear mixed models (LMM) and the generalized linear mixed models (GLMM).
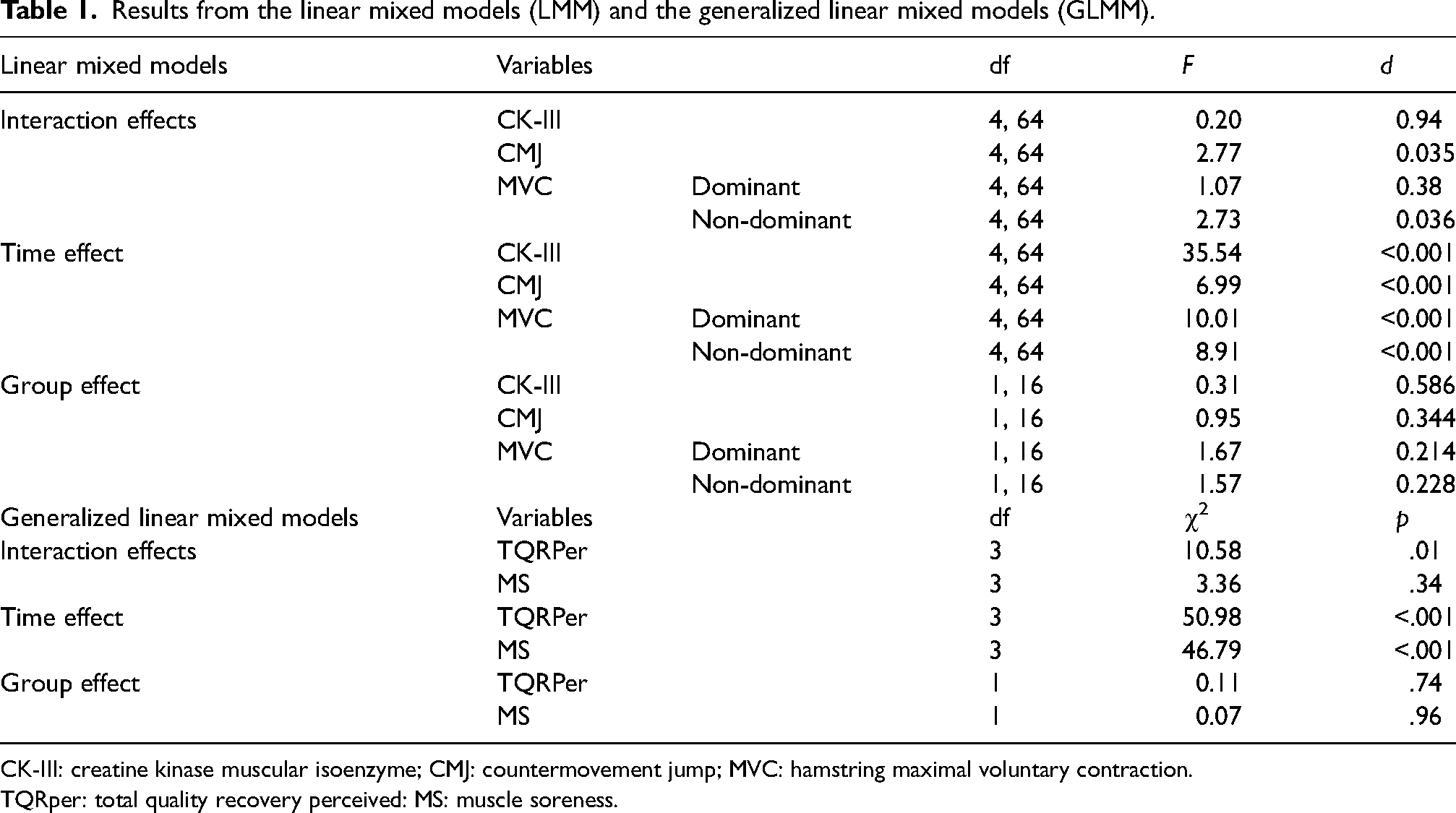
CK-III: creatine kinase muscular isoenzyme; CMJ: countermovement jump; MVC: hamstring maximal voluntary contraction.
TQRper: total quality recovery perceived: MS: muscle soreness.
Descriptive of the outcome variables for group and time.
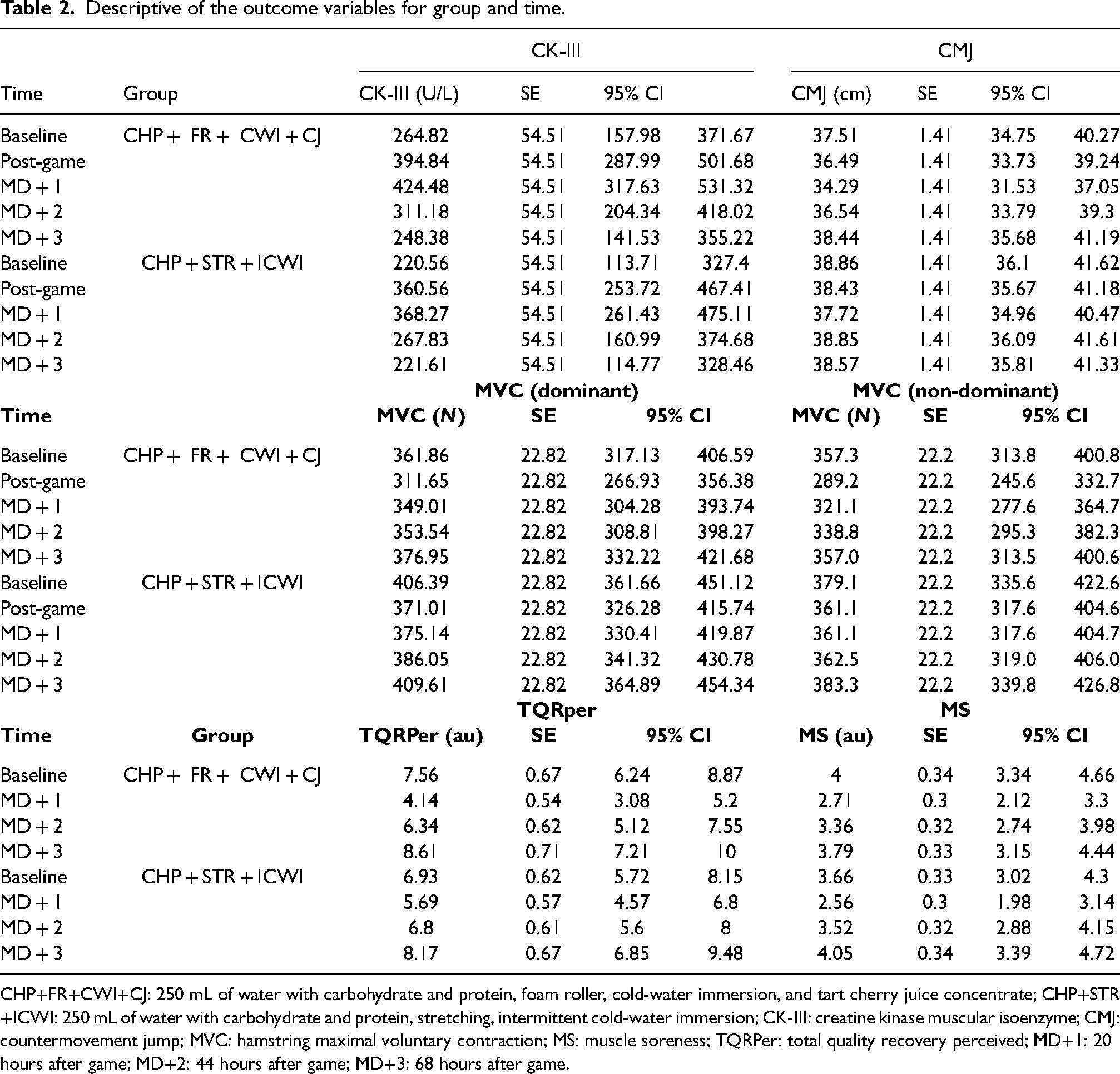
CHP+FR+CWI+CJ: 250 mL of water with carbohydrate and protein, foam roller, cold-water immersion, and tart cherry juice concentrate; CHP+STR+ICWI: 250 mL of water with carbohydrate and protein, stretching, intermittent cold-water immersion; CK-III: creatine kinase muscular isoenzyme; CMJ: countermovement jump; MVC: hamstring maximal voluntary contraction; MS: muscle soreness; TQRPer: total quality recovery perceived; MD+1: 20 hours after game; MD+2: 44 hours after game; MD+3: 68 hours after game.
The interaction effect (group * time) was present for the CMJ, MVC (non-dominant limb), and TQRper models (p < .05, F > 2.74; and χ2
Post hoc tests or contrasts
The effect of time for all the outcomes is presented in supplementary material IV and Figure 2.
The interaction effect for the CMJ and TQRper only revealed changes for the CHP + FR + CWI + CJ group at MD + 1 (supplementary material IV, Figure 2).
The interaction effect for the MVC (non-dominant) only revealed changes for the CHP + FR + CWI + CJ group at post-game and MD + 1 (supplementary material IV, Figure 2).
Relationship between CK-III and GPS data
The changes in CK-III from baseline to post-game related to the GPS data were performed by Pearson correlations and can be seen in Figure 3.

Relationship between CK-III and GPS variables. CK-III: creatine kinase muscular isoenzyme; HSR: High-Speed Running distance.
The changes in CK-III were correlated to the number of accelerations (p < .001; very large effect), the number of decelerations (p = .003; large effect), HSR distance (p = .007; large effect), and sprinting distance (p = .04; large effect). Instead, total distance (p = .34) was not correlated to the changes in CK-III.
Discussion
The present study was designed to compare the effectiveness of two recovery protocols after a game on physiological, neuromuscular, and perceptual outcomes with elite U-21 soccer players. Both protocols had a positive time effect, indicating that both could be beneficial at providing accelerated recovery after a game at different time points (20–44-68 h) depending on the variable of interest. However, no differences were found between them; therefore, this study cannot report the superiority of one protocol over the other. Based on this study, practitioners and players may choose different possibilities to ensure recovery effectiveness. Large and very large correlations between CK-III and external load parameters such as accelerations, decelerations, HSR distance, and sprinting distance were observed.
Top-tier soccer players show low levels of muscle damage during official tournaments and have faster recovery before the next game. 40 In this sense, current scientific evidence demonstrates that CK normalization time courses are up to ≥72 h, despite physical performance recovery lasting up to ≥48 h. 7 These findings are like those reported in the present study, showing that neuromuscular outcomes (MVC and CMJ) recovered faster than CK-III, returning to similar baseline levels at MD + 2. However, CK-III baseline levels were reached between 48 and 72 h, 41 where the peak CK-III levels were obtained at MD + 1 in both groups, like what has been reported in previous research. 42 CK-III isoform inter-subject variability response should be considered when using it as a recovery-specific marker. 43 Furthermore, four GPS parameters, such as HSR and sprint distance, accelerations, and decelerations, showed large to very large correlations with CK-III and muscle damage immediately after the game. While this was not one of the study's primary aims, the possibility of determining recovery needs using noninvasive markers coming from GPS technology could provide a useful framework to individualize the recovery process in different soccer settings.12,15
No decrement was found when analyzing the CMJ performance immediately after the game. Instead, different trends were observed depending on the group at MD + 1. Considering a real change in performance in any value above the CV (4.6% = 1.7 cm), the CHP + FR + CWI + CJ group showed a decrement of 3.2 cm, while the CHP + STR + ICWI group reported no changes (−1.1 cm). Although some differences can be observed in the groups, they are not statistically significant. In a recent investigation by Romagnoli and colleagues, where no recovery intervention was applied, CMJ was compromised at 48-h post-game compared to the baseline level, 44 suggesting the need to perform recovery strategies such as the ones used in this piece of research. Hence, applying recovery strategies seems important when lower body performance needs to be recovered within 48 h, with the CHP + STR + ICWI protocol providing slightly better benefits (although not significant compared to the other protocol) for maintaining CMJ performance following a game. Future studies must be implemented to confirm this claim.
When CJ was used for two consecutive days in combination with the other methods of the protocol (CHP + FR + CWI), this intervention did not significantly improve any variable analyzed compared to the CHP + STR + ICWI. Nevertheless, when using it as a unique recovery method for eight consecutive days and compared to a control group, neuromuscular outcomes (CMJ, MVC) recovered faster such as MS indicators were lower and inflammatory response was attenuated. 45 Although these beneficial effects, no effects on oxidative stress or CK were observed. 45 The intake frequency used in the protocol (only 2 days) and synergistic or additive possible effects when combining several recovery methods could attenuate CJ's impact.
The present study used two ways of applying immersion in cold water and other recovery methods. Both obtained similar results in terms of physiological, neuromuscular, and perceptual outcomes. CWI significantly affects delayed onset muscle soreness (DOMS), perceived fatigue and recovery, muscular power performance, and serum CK. 46 However, these effects were only observed 24 h after high-intensity exercise and not after eccentric loads. CWI was only effective for positively influencing muscular power but not muscular strength performance. 46 A moderate difference in favor of this recovery method (CWI) was observed in soccer at 48 h when analyzing CMJ and MVC. 47 Nevertheless, in a recent review, Schons and colleagues 48 found beneficial effects of CWI on muscle strength but no effects on jumping and running performance. Additionally, CWI and active recovery after a game did not improve jumping performance 22 in youth players. However, according to a recent study, 46 the duration and temperature of CWI can play a crucial role in enhancing recovery. For instance, lowering the time and temperature may improve the efficacy of CWI after high-intensity exercises, such as removing CK and incrementing endurance performance.
The literature lacks evidence supporting the muscular and physiological effects of stretching after physical activity or competitive soccer games on reducing MS. 49 Moreover, some authors concluded that it might even lead to an increase in DOMS and CK levels, 50 while others 49 found a CK reduction after performing static stretches. Therefore, the existing evidence is quite conflicting. However, when stretching exercises were combined with other recovery techniques, such as massage (after a competition), 51 it induced a lower perception of leg soreness and better CMJ values. 52 Previous research has found that CMJ values were significantly higher 24 h after a training session when using a combination of recovery methods consisting of submaximal running and static stretching. 21 These findings are similar to the ones in the present study, where stretching within a recovery protocol induced positive changes in the variables studied; yet, it is impossible to state that these improvements were caused by stretching or other recovery strategies.
A recent review has reported ambiguous conclusions and recommendations about foam rolling when analyzing the use among different-level athletes. 53 In another recent study, after a typical soccer session, foam rolling had a large effect on the recovery of agility, TQRper, and perceived MS compared to a passive recovery. Nevertheless, and according to the current study findings, similar perceptual and neuromuscular outcomes were found when comparing two protocols that combined different recovery methods. Nonetheless, and due to these non-conclusive results, foam rolling may be recommended as a recovery tool for this typology of athletes.
Despite the lack of definitive scientific evidence, some recovery methods, such as stretching or foam rolling, are widely used by elite soccer teams after training and competition. 17 One of the reasons could be that these recovery methods can influence players’ perceptions and may increase adherence to the protocols. 21 Therefore, practitioners should consider their use when planning and designing multimethod recovery protocols. Based on this study's findings, we recommend including different recovery methods based on several criteria, such as scientific agreement, but first, considering players’ preferences and perceptions based on wellness, especially at elite levels.
This study found a time effect on recovery parameters in both interventions. Specifically, CK-III was normalized at MD + 3 and neuromuscular and perceptual outcomes at MD + 2. However, no differences between protocols were found, except for the interaction effect found in the CHP + FR + CWI + CJ group at post-game and MD + 1 in neuromuscular and TQRper outcomes. Therefore, based on these results, this paper's authors consider both protocols similarly effective. Practitioners could combine the recovery methods proposed in this study as post-competition recovery strategies and adjust the interventions to meet elite soccer players’ requests and team contexts based on their fixtures or training schedule.
The protocol used a convenience sampling technique to select players from the U-21 Mexican National Team. Consequently, the sample size (N = 20) is relatively small, which could have limited the statistical power and affected the significance of some comparisons (between effects). 24 However, using “sample quality criteria,” the specificity of the players enrolled (elite young soccer players) may have increased its representativity. Moreover, the players in the study were only male; therefore, these protocols should be replicated in female populations of a similar competitive level before their implementation. Finally, the lack of a control group in the study limits the possibility of concluding our investigation by understanding if any experimental conditions were more effective than controls in a similar population. However, this is a common limitation when professional players are enrolled.
Practical applications
Elite soccer players could combine different recovery methods after games, such as the two combinations used in this study that reported a positive effect on recovery.
Both protocols used in this study had a positive time effect, but since no differences were found between them. Practitioners could use the ones more suitable for their players.
It is suggested that practitioners and players be given a choice among different options based on their preferences and the perceived effectiveness of recovery.
Since large and very large correlations between CK-III and external load parameters such as accelerations, decelerations, HSR, and sprint distance were observed. Practitioners are invited to monitor these parameters to manage the recovery strategies better.
Supplemental Material
sj-doc-1-spo-10.1177_17479541231155585 - Supplemental material for The effectiveness of two comprehensive recovery protocols on performance and physiological measures in elite soccer players: A parallel group-randomized trial
Supplemental material, sj-doc-1-spo-10.1177_17479541231155585 for The effectiveness of two comprehensive recovery protocols on performance and physiological measures in elite soccer players: A parallel group-randomized trial by Albert Altarriba-Bartes, Jordi Vicens-Bordas, Javier Peña, Fernando Alarcón-Palacios and Luis A Sixtos-Meliton, Martí Matabosch-Pijuan, Enric Giménez-Martínez, Marco Beato, Julio Calleja-González in International Journal of Sports Science & Coaching
Supplemental Material
sj-doc-2-spo-10.1177_17479541231155585 - Supplemental material for The effectiveness of two comprehensive recovery protocols on performance and physiological measures in elite soccer players: A parallel group-randomized trial
Supplemental material, sj-doc-2-spo-10.1177_17479541231155585 for The effectiveness of two comprehensive recovery protocols on performance and physiological measures in elite soccer players: A parallel group-randomized trial by Albert Altarriba-Bartes, Jordi Vicens-Bordas, Javier Peña, Fernando Alarcón-Palacios and Luis A Sixtos-Meliton, Martí Matabosch-Pijuan, Enric Giménez-Martínez, Marco Beato, Julio Calleja-González in International Journal of Sports Science & Coaching
Supplemental Material
sj-docx-3-spo-10.1177_17479541231155585 - Supplemental material for The effectiveness of two comprehensive recovery protocols on performance and physiological measures in elite soccer players: A parallel group-randomized trial
Supplemental material, sj-docx-3-spo-10.1177_17479541231155585 for The effectiveness of two comprehensive recovery protocols on performance and physiological measures in elite soccer players: A parallel group-randomized trial by Albert Altarriba-Bartes, Jordi Vicens-Bordas, Javier Peña, Fernando Alarcón-Palacios and Luis A Sixtos-Meliton, Martí Matabosch-Pijuan, Enric Giménez-Martínez, Marco Beato, Julio Calleja-González in International Journal of Sports Science & Coaching
Supplemental Material
sj-docx-4-spo-10.1177_17479541231155585 - Supplemental material for The effectiveness of two comprehensive recovery protocols on performance and physiological measures in elite soccer players: A parallel group-randomized trial
Supplemental material, sj-docx-4-spo-10.1177_17479541231155585 for The effectiveness of two comprehensive recovery protocols on performance and physiological measures in elite soccer players: A parallel group-randomized trial by Albert Altarriba-Bartes, Jordi Vicens-Bordas, Javier Peña, Fernando Alarcón-Palacios and Luis A Sixtos-Meliton, Martí Matabosch-Pijuan, Enric Giménez-Martínez, Marco Beato, Julio Calleja-González in International Journal of Sports Science & Coaching
Footnotes
Acknowledgments
The authors sincerely thank all the players and staff members from the U-21 Mexican National soccer team for their help and cooperation during the study. They also want to express their gratitude to all Mexican National Team Federation department members, especially Gerardo Torrado and Ignacio Hierro.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.