
Abstract
Sleep for recovery is an essential factor for performance in athletes. One such group is recreational ultra-marathon swimmers (>10km). We aimed to compare measures of sleep before and after a sleep hygiene education intervention during a 16-week training programme. Using a prospective study design, the experiment was conducted in two phases (pre- and post-intervention), whereby pre- and post-intervention data were collected for 42 nights after the sleep hygiene education. This study had 24 masters’ swimmers (n = 13 females), aged 39 ± 11 years, and body mass index (BMI) of 26 ± 3 kg/m2 during a training squad for an ocean ultra-marathon swimmer (19.7 km) in Perth, Western Australia. Objective measures of sleep were obtained from a wrist activity monitor, the Readiband™ (Fatigue Science Inc., Canada). Participants underwent a 2-hour sleep hygiene education session. Generalised linear mixed models were fitted to examine relationships between predictor variables and sleep responses. Sleep onset and offset increased by 12 minutes post-intervention (p < 0.001). For nights before morning training, sleep onset increased by 12 minutes and offset by 24 minutes post-intervention. Females increased sleep onset by 18 minutes and delayed sleep offset by 12 minutes sleep (p < 0.05) post-intervention. The sleep hygiene education was insufficient in making meaningful improvements to measures of sleep. Individual sleep hygiene education and continuous reinforcement of sleep for recovery during a training programme may be required to observe improvements. Coaches should aim to design training schedules to minimise the impact on swimmer’s sleep opportunity and swimmers need to involve family in the planning of rest periods during a training programme.
Introduction
The importance of sleep for athlete recovery and performance has been a strong focus of research in recent years. 1 This research has primarily focused on elite or highly trained athletes; however, such athletes represent a fraction of people participating in sports. Whilst the number of committed recreational athletes participating in organised sporting events is increasing, 2 research on these athletes is limited. One such group is ultra-marathon swimmers participating in ultra-marathon or long-distance races >10 km. 3 In a previous study, 4 we reported that these swimmers consistently sleep <7 hours per night despite this age group requiring 7–9 hours of total sleep per night, 5 have a high risk of sleep apnoea and have less total sleep time (TST) the night before an early morning training sessions twice a week (<06:00). 4 Poor sleep outcomes in this population may reflect the impact of family, work, study and social commitments, which in addition to athletic training, may leave little opportunity for sleep. Such challenges are also present with youth athletes, with improvements in sleep with a sleep hygiene educational intervention. 6 Therefore, there is a need to examine whether interventions aimed at improving sleep are effective for recreational athletes.
Education is one such commonly employed intervention. Education programmes primarily focused on improving sleep hygiene and have demonstrated efficacy in improving the sleep of elite athletes; however, such programmes have not been tested on recreational athletes. Sleep hygiene education programmes may include information on sleep physiology, disorders and problems and the effects of caffeine, alcohol, exercise, routine and sleep environment on sleep. 7 For example, elite cricket players who underwent individualised sleep hygiene education sessions reduced their sleep latency (time to fall asleep) and advanced time at sleep onset resulting in a 5% improvement in sleep efficiency (SE). 8 In elite female netball players, a 1-hour group sleep hygiene education programme increased total sleep time (TST) by an average of 22 minutes per night and reduced time at wake variance in the mornings. 9 When using a combination of these interventions, a sleep hygiene education programme (∼2 hours) and individualised consultations (∼20 minutes) with an elite female basketball team and staff, only coaches showed significant increases in TST. In this study, players already slept >8 hours per night at baseline; therefore, the lack of increase in TST following the intervention may suggest players were already meeting their sleep needs (i.e. ceiling effect). 10 In professional rugby league, a sleep hygiene education seminar increased TST among players; however, after 1 month, sleep measures had returned to baseline values. 11 More targeted interventions have focused on those with high self-reported daytime sleepiness. For example, sleep education and personal feedback provided to elite Australian Football League players increased TST and efficiency. 12
Despite these findings in elite athletes and the sleep difficulties experienced by recreational athletes, 3 no studies have examined the effectiveness of sleep hygiene education for recreational athletes. Therefore, this study hypothesised that a group education programme on sleep hygiene would improve measures of sleep among ultra-marathon swimmers through earlier sleep onset, reduced sleep latency, decreased wake after sleep, a delay in sleep offset and an increase in TST. As such, this study aimed to compare measures of sleep recorded before and after a sleep hygiene intervention to determine the effectiveness of such interventions for recreational athletes.
Methods
Participants
Twenty-four masters’ participants (n = 11 males, n = 13 females) volunteered to participate in this study. Participants were training for an ocean ultra-marathon swimmer (19.7 km) in Perth, Western Australia. The group had an average age of 39 ± 11 years, body mass index (BMI) of 80 ± 15 kg and height of 176 ± 1 cm, resulting in a BMI of 26 ± 3 kg/m2. Approval for the study was obtained from the Human Research Ethics Offices of the University of Western Australia. All participants were provided with information on the study prior to enrolment. Written informed consent was obtained from all before their participation.
Experimental design
This study examined the efficacy of a sleep hygiene education session for improving the sleep of masters’ swimmers undertaking a swim squad training programme (16 weeks, October to February) in preparation for an ocean ultra-marathon swimmer (19.7 km) in Perth, Western Australia, from Cottesloe to Rottnest Island.
All participants volunteered to participate in this training squad. A detailed examination of participants’ pre-intervention sleep and the lifestyle- and training-related factors that influence their sleep has already been published. 4 In summary, 8% were obese, 50% were overweight and 63% rated the importance of sleep as extremely important. The potential prevalence of obstructive sleep apnoea (OSA) was 21%, with 67% being moderate morning types (wake up at 07:24) (Supplementary Table 1).
Using a prospective study design, the experiment was conducted in two phases (pre-intervention and post-intervention), whereby pre-intervention (i.e. education session) data were collected for 42 nights and post-intervention data were collected for an additional 42 nights after the sleep hygiene education in late November (early summer). Across the data collection period, there were three scheduled training sessions each week: Monday 05:30–07:00, Thursday 19:00–20:30 and Saturday 06:00–08:00. Additionally, a wrist activity monitor was provided to consenting participants which they wore for the study duration.
Wrist actigraphy for objective measurement of sleep
Measures of sleep were obtained from a wrist activity monitor, the Readiband™ v5, and analysed using automated Readiband Sync™ with a 16Hz sampling rate (Fatigue Science Inc., Canada). Monitors were continuously worn on the non-dominant wrist 24/7 throughout the data collection period. Participants were instructed to remove the activity monitor when swimming to prevent malfunction due to potential water ingress.
When the Readiband device sleep/wake epochs are compared against the gold standard polysomnography (PSG) it has been reported as having an accuracy of 82%, sensitivity of 88% and specificity of 55% in 50 participants who underwent overnight sleep monitoring at a sleep laboratory. 13 The inter-device reliability of the automated scoring algorithm of the Readiband has been recommended for use in research settings. 14 Furthermore, it has been shown to compare favourably to PSG and another widely used and validated wrist activity monitor, the ActiGraph™ device 15 and is approved by the Food and Drug Administration 16 for measurement of physical activity and the extraction of measures of sleep. Sleep measures derived from the Readiband are described in detail in Table 1. On completion of the post-intervention phase, the wrist actigraphy devices were collected, and the data analysis was made using the proprietary automated Readiband Sync™ software. Data were extracted into excel form for statistical analysis.
Definitions of sleep measure as extracted from the Readiband™ (Fatigue Science Inc., Canada) device.
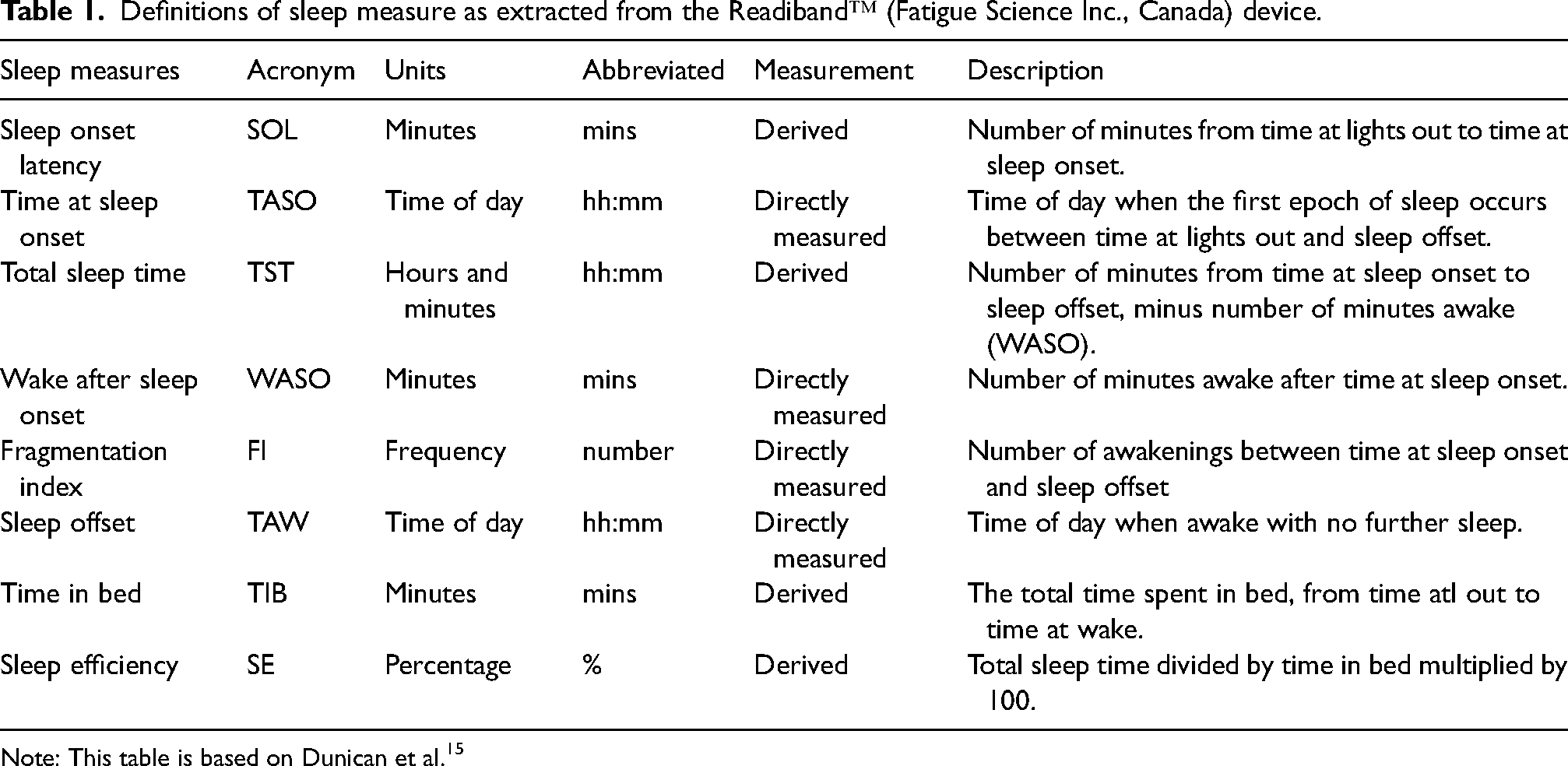
Note: This table is based on Dunican et al. 15
Sleep hygiene education session
A sleep hygiene education programme took place after the pre-intervention phase and consisted of a 2-hour presentation with 30 minutes of questions and answers in a group forum. This was delivered to all swimmers in the study. The topics included sleep physiology, chronobiology, sleep disorders, managing sleep environments, alcohol and caffeine use, anxiety and depression. Data from the pre-intervention phase was also presented at a group level (de-identified) to highlight trends, problems and potential areas for improvement. This included encouraging participants to better prioritise sleep the night before early morning training sessions, recommendations to reduce alcohol consumption, promoting efforts to reduce ‘sleep debt’ on the weekends, the highlighting the potential adverse effects of high body mass and sleep apnoea risk factors. The sleep education session was provided by an expert (PhD) qualified in sleep and performance in athletes.
Statistical analysis
Statistical analysis was conducted using the IBM Statistical Package for Social Sciences (v.27.0, IBM Corp., Armonk, NY, USA). All descriptive data are presented as mean ± SD. Generalised linear mixed models were fitted to examine relationships between predictor variables and sleep outcomes (sleep onset, sleep offset, time in bed (TIB), TST, SE, wake after sleep onset (WASO) and sleep onset latency (SOL)). The predictor variable set as a fixed effect in all models was the sleep education intervention, as data were coded as either ‘pre-intervention’ or ‘post-intervention’. Separate models were run to examine the potential influence of the intervention on all nights overall (1743 nights), nights of- and prior-to-rest days (1021 nights), nights before morning training (496 nights), nights after evening training (226 nights) and all nights for males (858 nights) and females (885 nights), respectively. For all models, participants were included as random effects. Model results are presented as the estimate (β), 95% confidence interval (CI) and p-value. The β-value represents the expected mean change in the outcome variable following the sleep education intervention. For all models, a p-value <0.05 was used for statistical significance.
Results
Overall
In the pre-intervention phase, there were a total of 886 nights and in the post-intervention phase, there were a total of 857 nights of sleep measures. The slight reduction in the post-intervention of 29 nights is attributable to failure to wear the device on that night.
When analysing all measures of sleep between pre- (886 nights) and post-intervention (857 nights), there were only statistical differences for sleep onset and sleep offset, with a 12-minute delay (e.g. later) in both variables following the intervention (p < 0.001 for both).
Nights before rest days
For nights of- and prior-to-rest days, sleep onset and offset were each delayed by 12 minutes, respectively, following the intervention (p < 0.05).
Nights before morning training sessions
For nights before morning training, sleep onset was delayed by 12 minutes, and sleep offset was delayed 24 minutes after the intervention (p < 0.05). The intervention had no statistical effect on sleep outcomes on nights following evening training.
Differences by sex
When considering biological sex, females recorded an 18 minutes delay in sleep onset, and a 12 minutes delay in sleep offset (p < 0.05), following the intervention (Table 2).
Modelled change in sleep outcomes following sleep hygiene education intervention. Includes models for all nights overall (1743 nights), nights of and prior-to-rest days (1021 nights), nights before morning training (496 nights), nights after evening training (226 nights) all nights for males (858 nights) and all nights for females (885 nights).
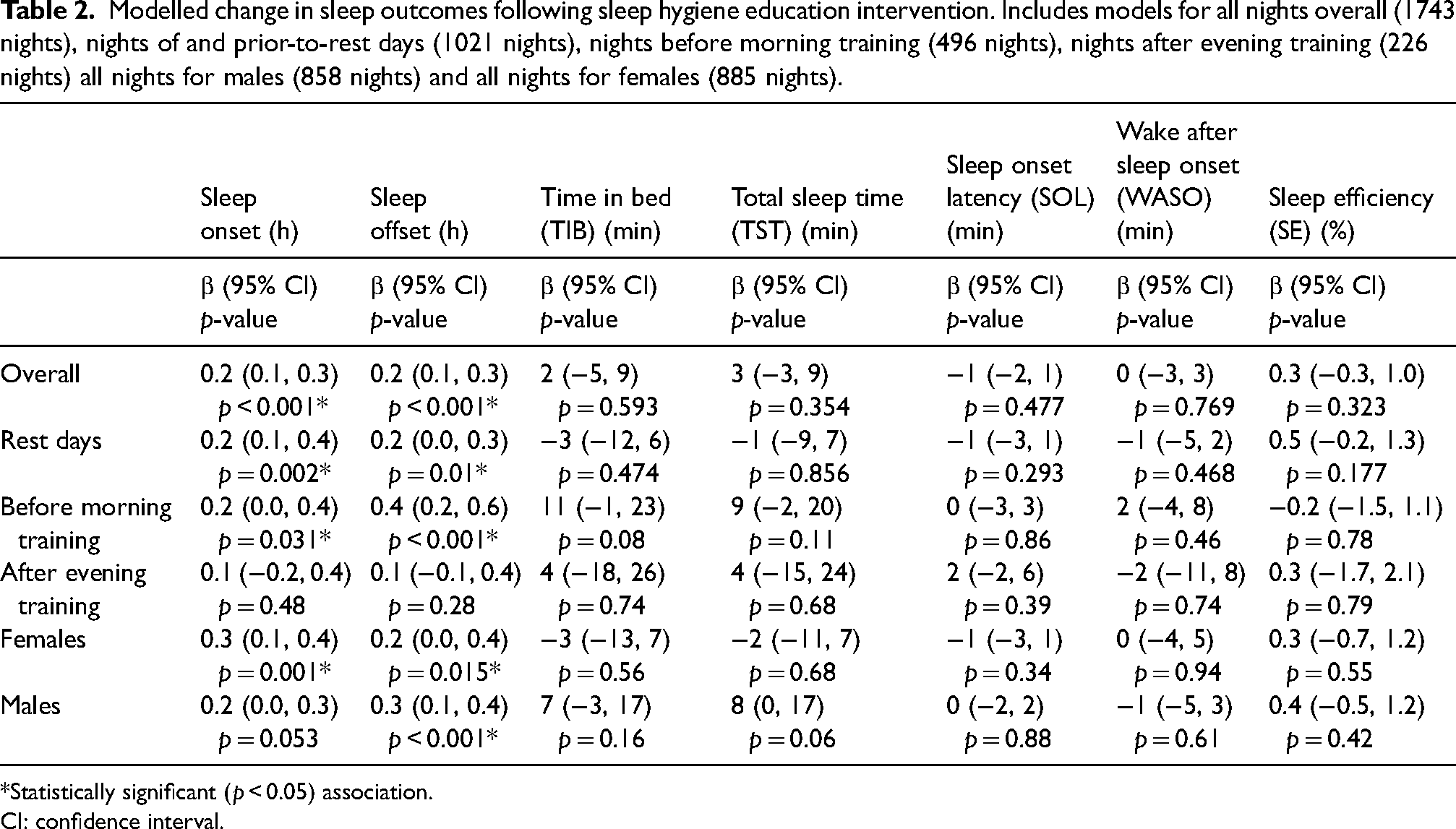
*Statistically significant (p < 0.05) association.
CI: confidence interval.
Discussion
This study aimed to examine the efficacy of a sleep hygiene education session for improving the sleep of recreational ultra-marathon swimmers. The main findings were that swimmers delayed time at sleep onset with a commensurate delay in sleep offset the following day, resulting in no improvement in TST. Furthermore, this led swimmers to continually achieve less than the recommended 7–9 hours of sleep per night throughout the pre and post-intervention period. 17
Overall, in this study, we found no meaningful improvement in any measures of sleep; to our surprise, we found no improvement in TST after sleep hygiene education. Further analysis highlighted similar sleep behaviours on rest days as on training days with no specific changes. It was hypothesised that TIB and TST would have increased on rest days as early morning wake up were not required. In addition, when parsing the group into females and males, only meaningful changes were observed for females by delaying the time at sleep onset and offset the following day.
TST
This is the first study to investigate sleep behaviours in a middle-aged, recreational athletic population through a sleep hygiene education. Results indicate that sleep did not significantly improve following sleep hygiene education. In the present study, TST was only marginally below the recommended 7–9 hours of sleep per night, with swimmers averaging 6 hours 51 minutes of TST per night across the pre- and post-intervention periods. However, it must be noted that the activity monitors have a propensity overestimate TST due to the poor specificity of the devices 13 and as such the reported values of TST may be less. These estimates of sleep are similar to the average sleep time reported among other middle-aged recreational exercise participants. 18 When this is considered alongside evidence that regular exercise is known to promote healthy sleep in middle-aged populations. 19 It may be considered that the TST and efficiency had already been optimised in this cohort (i.e. ceiling effect). However, the current TST may be due to the constraints life commitments that may have prevented further improvements (e.g. work and family commitments limiting increases in sleep opportunity). Therefore, participants may not be achieving their maximal biological need for sleep as is required for 95% of adults (7–9 hours). 5
Given the suboptimal TST of 6 hours 51 minutes in this group, an opportunity exists to deploy strategic napping to increase sleep; whilst napping each day may not be achievable due to work and family commitments, consideration should be given to napping on the weekends or days off from work where time permits. Napping is an excellent strategy to minimise sleep debt and improve performance. 20 Participants in this cohort may benefit from prophylactic naps or sleep debt reduction naps. Such naps are recommended between 1:00 and 4:00 pm during the secondary circadian nadir known as the post-lunch dip. A nap between 20 and 90 minutes is recommended with a 30-minute window upon awakening to reduce sleep inertia. 21 A benefit of the timing of these naps is that they do not interfere with the scheduled training periods of the swim squad. However, caution should be exercised when using napping; napping will reduce sleep pressure thereby possibly further delaying the time at sleep onset and may exacerbate insomnia or other sleep-related problems.
Timing of sleep
Evidence that sleep onset and offset times were delayed (i.e. delayed sleep phase) following the sleep hygiene intervention may not reflect the effects of the intervention, as it would be expected that sleep onset would advance (i.e. earlier) after participants received advice on the impacts of evening light, caffeine and bedtime routines on sleep onset. Instead, the delay in sleep in the present study may reflect changes in environmental natural light conditions. Whilst pre-intervention data collection occurred during spring in Australia, post-intervention data collection occurred in the late spring and early summer, when daylight hours are greatest during the year. Exposure to more evening light in the summer post-intervention period may explain the slight phase delay observed in this study. Interestingly, a sleep phase advance was not observed post-intervention when examining nights after evening training. This may reflect that the sleep phase was already delayed – likely due to training effects – in the pre-intervention period. Indeed, as reported in our previous study examining sleep in this cohort, sleep onset after evening training typically occurred after 10:30 pm, whereas sleep onset on rest days or before morning training was typically before 10:30 pm. Interestingly, this study's average sleep onset time of 10:29 pm highlights that participants were primarily moderate morning chronotypes, as previously reported. 4
In our study, the intervention was conducted in late November and post-intervention measures were collected in December. A potential factor impacting the inability to increase sleep is the increase in daylight hours. From the commencement of the pre-intervention to the end of the post-intervention period, there was an increase in daylight hours from 12 hours 58 minutes to 14 hours 12 minutes with the earliest sunrise time of 05:03. Over the duration of this study, there was a change in seasons. The study started in the spring and concluded in summer. Other research has reported that sleep is highest in the winter and gradual declines through spring, with its lowest during summer 22 and thereby may be impacted by the ability to increase sleep time. In addition, the month of December in Australia is a period of school summer holidays and an increase in festivities in the lead-up to Christmas, all of which may impact the ability to achieve additional sleep for the recreational athlete who may have children and may attend work of family festivities. An increase in alcohol 23 during this period and overeating may lead to fragmented and disrupted sleep, thereby reducing TST.
Sleep hygiene promotion and knowledge
A challenge with such recreational athletic cohorts is the ability to continually reinforce and promote the importance of sleep through sleep hygiene education. Our study consisted of a single 2-hour session with all swimmers, and no longitudinal reinforcement of the educational material occurred. In a study of professional rugby league, the players reverted to previous poor sleep habits within 1 month of the sleep hygiene education session, highlighting the importance of the sustainability of such programmes. 11 This is a challenge for athletes and coaches and one that may be exacerbated as a season or competitive period progresses. This is supported by recent recommendations that stated, ‘Sleep education should occur multiple times throughout the season’, with frequent check-ins with the athlete about their sleep and the use of presentations, informal sessions and information sheets to be used as health promotion. 17 Therefore, educating coaching and sports science staff to support sleep behaviours in more of a health promotion manner may be a sustainable option in the future to promote sleep hygiene practices. To do this, we must consider the current knowledge and skills of coaches and sports science staff. Overall, sleep hygiene knowledge in coaches and sports science staff has been assessed as only adequate, and knowledge of sleep–wake behaviours and thoughts and attitudes about sleep is inadequate. Furthermore, less than half of coaches and sports science staff promote sleep hygiene within their teams, groups, or athletes, with a lack of knowledge in sleep science being one of the main factors. 24 Considering that athletes will interface and communicate with coaches and sports science staff on a regular basis, a focus on a higher level of education to these coaches and sports science staff who can continually educate, promote to athletes may be a more effective approach for sustainability over time. Specifically, resources such as videos, online courses, seminars, podcasts and infographs can be utilised to engage recreational swimmers.
Considering family, work and time
Research is scarce concerning sleep among recreational athletes who must contend with work, family and training for their specific discipline. Whilst this is normal for many athletes, the research has not investigated the interaction between these variables that may reduce sleep. One potential factor may be the home and family environment, whereby family-to-work conflict and parents’ lack of time for self-care were associated with sleep complaints. 25 This poorer sleep quality is higher in males and dual-parent single-income families. 26 Whilst family and lifestyle data were not captured within this study; it is a potential factor that may need to be addressed through pre-screening or personal interview techniques to identify contributing factors to sleep-related problems. Such factors may also include the type of work the recreational athlete is employed in; the stress incurred during working hours may impact sleep quality, all of which will reduce TST and should be considered. 27 Another component that should be considered is ‘time’; there are only 24 hours in a day, and when an athlete exercises, eats, works and spends time with family and friends, there is often reduced opportunity for sleep; in addition, early morning wake ups to attend training further curtail sleep opportunity. 28
Potential limitations of this study
The lack of sleep disorder assessment and its potential prevalence may impact their ability to improve their sleep. Psychological characteristics were not included within this study such as anxiety and depression that may be impacting sleep problems or disorders. The inclusion of daytime napping was not included and may be impacting the assessment of TST in a 24-hour period. This study did not aim to quantify sleep staging and sleep quality due to cost and resource limitations, further studies with appropriate funding may wish to examine this. In addition, the time frame in which our study took place is somewhat limited by the 16-week swim squad. As discussed earlier, long-term group and individual sleep hygiene education and optimisation may be required to observe meaningful changes.
Future research
Future research should evaluate the potential presence of undiagnosed sleep disorders at the commencement of a training season. This may be achieved through alternative home-based ambulatory PSG methods that may also be used to assess sleep stages and sleep quality. 29 In addition, investigating the external factors that impact recreational athletes’ sleep, such as family, work, study, or other commitments, is vital in future studies as these may be the most significant modifiable factors. Finally, studies may wish to educate coaching staff on sleep science and provide a communication plan to reinforce sleep behaviours throughout the training season.
Conclusion
In conclusion, middle-aged recreational swimmers require a sustained focus on sleep habits and behaviours through a training programme. This study also provides evidence that coaches need to consider sleep hygiene education and continuous reinforcement of sleep for recovery during a training programme. Training schedules should be designed to minimise the impact on swimmer’s sleep opportunity and swimmers need to involve family in the planning of rest periods during a training programme.
Practical applications for coaches
Coaches should consider designing training schedules based on swimmers’ sleep habits, behaviours and chronotypes to support sleep extension may result in more meaningful changes.
Coaches should consider the time of year when a training season is occurring as external factors such as school holidays and seasonal holidays such as Christmas or Easter may impact recreational athletes’ sleep and recovery practices.
Individual athletes may need to involve their families in changes arising from sleep hygiene education sessions to promote meaningful improvements to sleep.
Supplemental Material
sj-docx-1-spo-10.1177_17479541231152196 - Supplemental material for Sleep hygiene education for improving sleep in ultra-marathon swimmers: Guidance for coaches and swimmers
Supplemental material, sj-docx-1-spo-10.1177_17479541231152196 for Sleep hygiene education for improving sleep in ultra-marathon swimmers: Guidance for coaches and swimmers by Ian C Dunican, Emma Perry, Gemma Maisey, Elena Nesci and Spencer Roberts in International Journal of Sports Science & Coaching
Footnotes
Acknowledgements
The authors would like to thank Fatigue Science, Vancouver, British Columbia, for the supply of Readiband™. Second, to Elena Nesci and the swimmers at eSwim, Western Australia for participating in this study.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Ian C Dunican is the Chair of the Scientific Advisory Board for Fatigue Science, Canada, and received no financial or other incentives related to this research project. In addition, Ian C Dunican is the Director and Chief Adviser of Melius Consulting Pty Ltd and Sleep4Performance.
Funding
The author(s)received no financial support for the research, authorship, and/or publication of this article: This study was fully funded by Sleep4Performance https://sleep4performance.com and the athletic business of Melius Consulting Pty LTD ![]() .
.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.