
Abstract
Background and aims:
In high-income countries, stroke incidence in the 21st century has increased or stagnated in young and middle-aged individuals. Assessing temporal trends in post-stroke outcomes is necessary to understand the impact of these changes in incidence.
Methods:
Embase and MEDLINE were searched from 1 January 1970 to 30 October 2024. Studies were included if they reported case fatality, 1-year or 5-year mortality, or stroke recurrence in patients aged up to 65 years. For studies reporting outcomes across multiple time periods, risk ratios (RRs) were calculated comparing the earliest and latest periods and pooled using inverse-variance random-effects models. The annualized change in the RR for case fatality was estimated using meta-regression.
Results:
Twenty-two studies reported case fatality across 28 populations after all strokes or ischemic stroke and intracerebral hemorrhage (14 population-based and 14 based on routinely collected data). The median (interquartile range (IQR)) duration between compared time points was 9 (7–13.3) years. Case fatality decreased over time (RR = 0.74, 95% confidence interval (CI) = 0.68–0.81), corresponding to a mean annual relative reduction of 3.2% (95% CI = 1.4–5.0). Results were consistent by age, sex, study design, geographical region, and stroke subtype (six studies; ischemic stroke: RR = 0.79, 95% CI = 0.75–0.83; intracerebral hemorrhage: RR = 0.77, 95% CI = 0.69–0.86). Trends were similar before and after 2000, with continued improvement after 2010 compared with 2000–2009 (six studies; RR = 0.70, 95% CI = 0.63–0.77). In addition, mortality decreased at 1 year (five studies; RR = 0.68, 95% CI = 0.52–0.87) and at 5 years after stroke (four studies; RR = 0.65, 95% CI = 0.45–0.95). In contrast, the 1-year cumulative incidence of recurrent stroke was unchanged after 2000 (three studies; RR = 1.04, 95% CI = 0.78–1.39).
Conclusion:
Early case fatality and long-term survival after stroke have progressively improved since the 1970s in high-income countries among young and middle-aged individuals, but stroke recurrence rates may have stagnated in the past two decades.

Keywords
Introduction
Stroke incidence has declined overall in high-income countries over the past 4 decades. 1 However, recent reports have shown an age-related divergence in stroke incidence, with less favorable trends and, in many settings, increasing or stagnating rates in young (<55 years) individuals.2–4 Population-based studies have also found that stroke incidence in middle-aged individuals (45–64 years) may have recently stagnated.3,5 Assessing temporal trends in post-stroke outcomes in young and middle-aged individuals is, therefore, needed to understand the impact of these changes in incidence.
Although studies have shown an improvement in early case fatality 6 and long-term survival after stroke overall, 7 several observations suggest that these trends may have differed by age. First, all-cause mortality rates in young and middle-aged adults have recently stagnated or increased in several high-income countries, which may adversely affect long-term survival after stroke. 8 Second, advances in secondary prevention may have preferentially benefited older patients (e.g. anticoagulation for atrial fibrillation), while treatments that are more commonly used in younger patients have only recently been widely implemented (e.g. patent foramen ovale closure). Third, the case mix of young stroke patients may have changed over time, with some studies reporting an increase in the proportion of ischemic compared with hemorrhagic stroke,3,9 a rise in cryptogenic ischemic stroke (IS), 3 and a decrease in stroke severity. 10 A recent study summarized rates of stroke recurrence in young adults, but whether these have improved over time remains unknown. 11
In the absence of similar data, we conducted a systematic review and meta-analysis to determine temporal trends in case fatality, long-term survival, recurrence, and vascular events after stroke among young and middle-aged individuals in high-income countries. We also assessed whether patient- and study-level characteristics explain observed trends.
Methods
Standard protocol approvals and registration
This systematic review was pre-registered on PROSPERO (CRD42051146314) and is reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analyses guidelines. 12
Search, study selection, and data extraction
Ovid Embase and Ovid MEDLINE were searched from 1 January 1970 to 30 October 2024, without language restrictions. The full search strategy is provided in Supplemental Table 1.
Eligible studies were as follows: (1) prospective or retrospective cohort studies (including population-, registry-, administrative-, or records-based designs); (2) conducted in high-income countries (as defined by the World Bank); (3) including patients with any stroke, IS, or intracerebral hemorrhage (ICH); (4) reporting at least one of the following outcomes: case fatality, survival at 1 year or longer, stroke recurrence, myocardial infarction, composite major cardiovascular outcomes, venous thromboembolism, or major bleeding; and (5) in patients aged up to 65 years. The review was focused on high-income countries to improve comparability between stroke populations and study methodologies.
Studies were excluded if they were limited to subarachnoid hemorrhage, specific subpopulations (e.g. patients undergoing thrombolysis), pediatric populations, or if the minimum age for inclusion exceeded 40 years. Titles and abstracts were screened by one author (A.N.) and verified by a second author (L.L.). To identify additional studies, we hand-searched the reference lists of included studies, prior systematic reviews of similar outcomes across all ages,6,13–17 prior systematic reviews of temporal trends in stroke incidence,1,2,6 and other relevant publications known to us. Only peer-reviewed studies were included due to limitations in reporting quality in unpublished data.
If patient populations overlapped across several publications, we prioritized studies according to the following hierarchy: (1) those reporting outcomes for multiple time periods, (2) those with the largest sample size, and (3) unique subpopulation analyses. If a single study included results from different populations, data extraction and analysis were performed separately for each population. 18 If a study included patients with IS and transient ischemic attack (TIA), we extracted outcomes for patients with IS only, when possible.
Data were extracted by one author (A.N.) using a predesigned form and verified by a second author (L.L.). When data were presented only in graphical format, values were extracted using PlotDigitizer. If proportions were reported with 95% confidence intervals (CIs) but raw counts were unavailable, these were estimated from the reported proportion and CI width under the assumption of a binomial distribution. Authors were not contacted for data that were not reported in the original publications.
For each study, we extracted the inclusion period(s), number of stroke events, and number of outcome events. Early case fatality was defined as death within 28 days, 30 days, or during hospitalization. Mortality was also assessed at 1 and 5 years after stroke using proportions or cumulative incidence rates. Recurrence was extracted at any available time point during follow-up. When survival or recurrence data were presented only in graphical format (Kaplan–Meier or cumulative incidence curves), these were digitized, and Guyot’s method was applied to reconstruct pseudo-individual patient data. 19 If a study reported recurrent stroke and TIA, we extracted recurrent stroke only, when possible. When studies provided qualitative or summary measures of temporal trends (e.g. annualized percentage changes), these were extracted as presented.
As no validated quality appraisal tool exists for systematic reviews of temporal trends in disease outcomes, we used a domain-based approach adapted for stroke epidemiology, as previously reported 2 and adapted from van Asch et al. 20
Data synthesis and statistical analysis
Study outcomes were plotted for each reporting period, with 95% CI calculated using the Clopper–Pearson method.
For studies reporting outcomes across multiple time periods, risk ratios (RRs) were calculated by comparing the earliest and latest periods within each study and pooled using inverse-variance random-effects meta-analysis. Between-study heterogeneity was assessed using forest plots and quantified using the I2 statistic.
For case fatality, univariable meta-regression was used to estimate the annualized change in the RR and to determine whether study-level characteristics explained heterogeneity in temporal trends. Where feasible, prespecified subgroup analyses were conducted by age, sex, geographical region, stroke subtype (all strokes, IS, ICH, first-ever strokes), study design (population-based, routinely collected data), calendar period, sample size, outcome definition (28-day or 30-day, in-hospital mortality), duration between compared periods, and annualized change in stroke counts between compared periods. The latter was used as a proxy for changes in case ascertainment over time, under the assumption that larger increases in stroke counts may partly reflect improved detection or increased admission of milder events. For studies that also reported trends in older populations, these were extracted to determine whether the observed trends were specific to young and middle-aged individuals.
For 1- and 5-year mortality, given the limited number of studies reporting multiple time periods, we did not explore heterogeneity using meta-regression. To further evaluate temporal trends, we included studies reporting a single or multiple periods in an inverse-variance random-effects meta-analysis, with a double arcsine transformation for proportions or a logit transformation for cumulative incidence rates. Temporal trends were assessed using meta-regression with mid-period year as the independent variable and transformed proportions or cumulative incidence rates as the dependent variable, adjusting the study upper age limit and the type of event included (e.g. IS or IS and TIA).
For studies reporting temporal trends qualitatively or quantitatively but without raw data or CIs, the direction of the trend was recorded. A sign test (binomial test) was then performed to compare the number of studies reporting an increase versus a decrease or no change in the outcome over time.
Between-study variance (τ2) was estimated using restricted maximum likelihood. Reporting bias was assessed by visual inspection of funnel plots when ⩾10 studies reported multiple periods. If funnel plots were asymmetrical, trim-and-fill sensitivity analyses were performed. Analyses were conducted using R (version 4.3.1).
Results
The search of databases identified 67,845 records, with 682 full-text studies assessed for eligibility after title and abstract screening. Of these, 180 met the inclusion criteria. An additional 99 studies were identified through other sources, resulting in a total of 279 studies reporting at least one outcome (Supplemental Figure 1).
Case fatality
Two hundred and three studies reported case fatality across 223 populations: 151 (74.4%) for a single period, 31 (15.3%) across multiple periods, and 21 (10.3%) with qualitative or quantitative trends.
For all strokes or IS and ICH, 22 studies reported case fatality across multiple periods in 28 non-overlapping populations (21 all strokes and 7 IS and ICH; 14 population-based and 14 based on routinely collected data) (Figure 1, Supplemental Table 2).7,18,21–40 These studies encompassed 14 countries, with a median (interquartile range (IQR)) interval between the earliest and latest periods of 9 (7–13.3) years. Seven studies reported event counts by stroke subtype. The proportion of IS among all stroke events was stable or decreased over time in four studies and increased in three studies.26,29,32,34,35,39,40

Temporal trends in case fatality after all strokes in young and middle-aged individuals. Studies were plotted if they reported case fatality across more than one period after all strokes at ages ⩽65 years, stratified by study design. Studies reporting case fatality after ischemic stroke and intracerebral hemorrhage were not plotted. Case fatality was defined as death within 28 days, 30 days, or during hospitalization. Larger points represent more precise estimates (smaller standard errors) of case fatality.
Case fatality after all strokes or IS and ICH was lower in the latest compared with the earliest period (RR = 0.74, 95% CI = 0.68–0.81; I2 = 92%) (Figure 2). The mean annual relative reduction in case fatality was 3.2% (95% CI = 1.4–5.0), with corresponding reductions of 3.3% (95% CI = 0.6–11.7) in population-based studies and 2.8% (95% CI = 0.3–5.1) in studies based on routinely collected data.

Meta-analysis of the relative change over time in case fatality after stroke in young and middle-aged individuals. Risk ratios for each study were pooled using inverse-variance random-effects meta-analysis, stratified by study design. Case fatality was defined as death within 28 days, 30 days, or during hospitalization. Studies were included if they reported case fatality across more than one period after all strokes or after ischemic stroke and intracerebral hemorrhage at ages up to 65 years. A risk ratio < 1 indicates a lower risk of death in later compared with earlier time periods.
Temporal trends were consistent by age, sex, geographical region, stroke subtype, study design, sample size, and outcome definition (Figure 3 and Supplemental Figures 2 to 11). Greater reductions in case fatality were observed in studies with longer intervals between compared periods and in those with potential improvement in the ascertainment of mild events over time (Supplemental Figures 12 to 13). Trends were similar before and after 2000, with continued improvements after 2010 compared with 2000–2009.
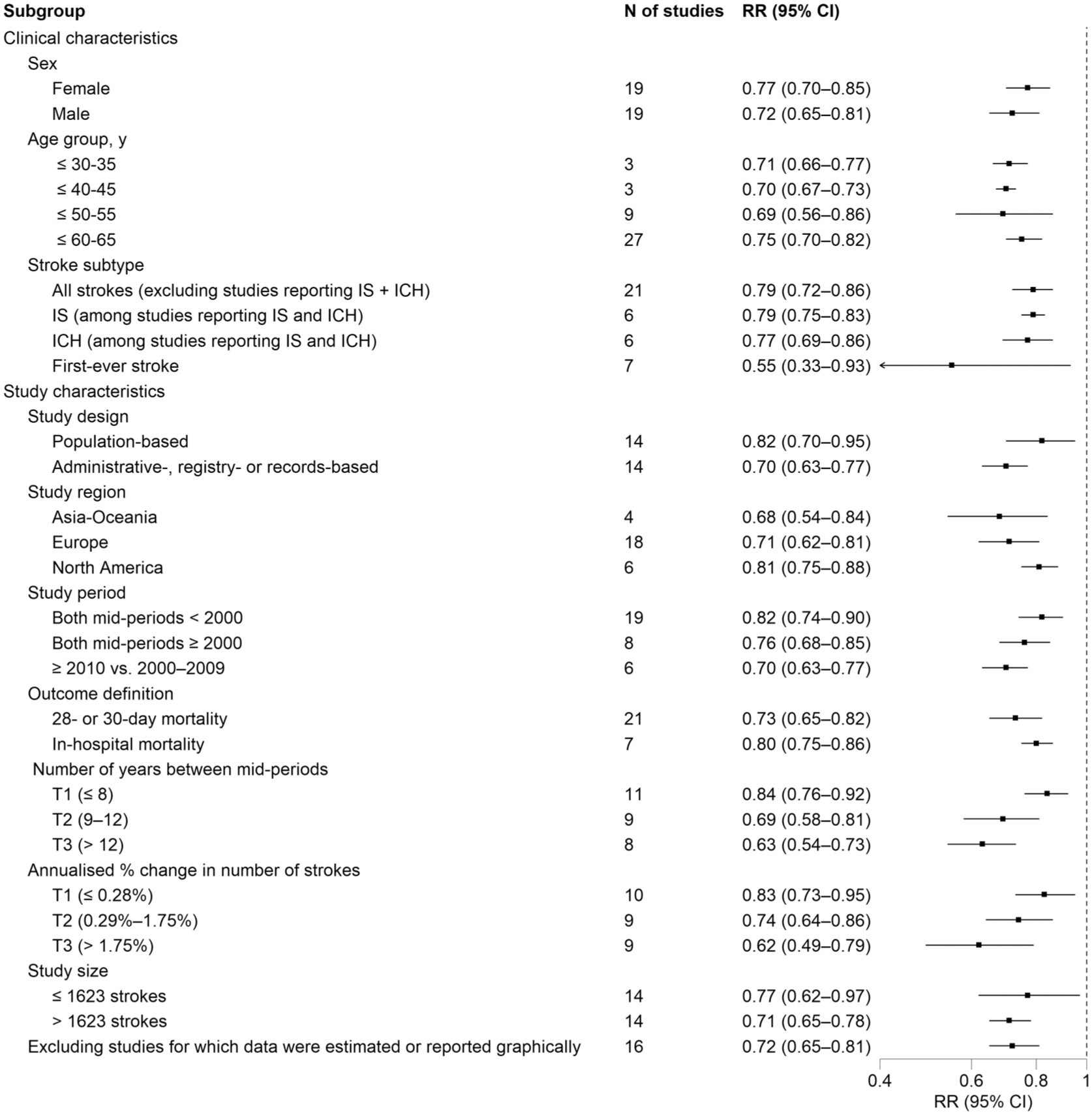
Subgroup analyses of the relative change over time in case fatality after stroke in young and middle-aged individuals. Risk ratios for each study were pooled using inverse-variance random-effects meta-analysis, stratified by clinical and study characteristics. Case fatality was defined as death within 28 days, 30 days, or during hospitalization. Studies were included if they reported case fatality across more than one period after all strokes or after ischemic stroke and intracerebral hemorrhage at ages up to 65 years. The number of years between mid-periods and annualized changes in stroke counts were stratified by tertiles (T1 to T3). A risk ratio < 1 indicates a lower risk of death in later compared with earlier time periods.
Thirteen studies also reported case fatality in older populations, showing similar reductions at ages ⩽65 years (RR = 0.73, 95% CI = 0.63–0.85; I2 = 89%) and >65 years (RR = 0.78, 95% CI = 0.69–0.89; I2 = 99%).21–27,29,31,32,36–38 There was no evidence of small-study effects (Supplemental Figure 14). Among 12 studies reporting qualitative or quantitative trends, 11 showed decreases and 1 no change in case fatality (p < 0.01) (Supplemental Table 3).
For IS, 12 studies reported case fatality across multiple time periods (2 population-based and 10 based on routinely collected data), with a median (IQR) interval of 9 (7.8–13.3) years between the earliest and latest periods (Supplemental Table 4 and Supplemental Figure 15).26,29,32,34,35,39–45 Case fatality was lower in the latest compared with the earliest period (RR = 0.74, 95% CI = 0.64–0.87; I2 = 82%) (Supplemental Figure 16). Results were consistent across subgroup analyses (Supplemental Figure 17), with no evidence of small-study effects (Supplemental Figure 18). Among 14 studies reporting qualitative or quantitative trends, 12 showed decreases, and 2 showed no change in case fatality (p = 0.01) (Supplemental Table 5).
For ICH, 11 studies reported case fatality across multiple time periods (2 population-based and 9 based on routinely collected data), with a median (IQR) interval of 9 (8–10.5) years between the earliest and latest periods (Supplemental Table 6 and Supplemental Figure 19).26,29,32,34,35,39–41,46–48 Case fatality was lower in the latest compared with the earliest period (RR = 0.78, 95% CI = 0.72–0.85; I2 = 88%) (Supplemental Figure 20). Reductions were found for both sexes but were greater in females (Supplemental Figure 21). There was evidence of small-study effects (Supplemental Figure 22), but case fatality remained lower after trim-and-fill adjustment (RR = 0.83, 95% CI = 0.74–0.93; I2 = 86%). All seven studies reporting qualitative or quantitative trends showed decreases in case fatality (p = 0.02) (Supplemental Table 7).
When all studies reporting case fatality across multiple time periods were pooled, temporal trends were heterogeneous (RR = 0.74, 95% CI = 0.67–0.80; I2 = 91%). The duration between the compared mid-periods explained 55% of the between-study heterogeneity. Other factors associated with heterogeneity in separate univariable models included case fatality definition (15%), geographical region (7%), upper age limit (6%), and study design (6%).
One-year mortality
Sixty-seven studies reported 1-year mortality. Of these, 15 were excluded (Supplemental Figure 23), leaving 52 studies for analysis: 35 (67.3%) reporting a single period, 9 (17.3%) multiple periods, 7 (13.5%) qualitative or quantitative trends, and 1 (1.9%) both a single period and quantitative trends.
Among the nine studies reporting multiple periods, 1-year mortality decreased over time for all strokes or IS and ICH (five studies; RR = 0.68, 95% CI = 0.52–0.87; I2 = 70%),7,21,22,24,35 IS (four studies; RR = 0.58, 95% CI = 0.48–0.69; I2 = 69%),35,44,45,49 and ICH (two studies; RR = 0.72, 95% CI = 0.53–0.99; I2 = 82%)35,47 (Supplemental Table 8 and Supplemental Figures 24 to 26). Reductions were also observed among 28/30-day survivors for all strokes or IS and ICH,7,21,22,24,35 IS,35,44,45 but not for ICH35,47 (Table 1).
Temporal trends in 1-year mortality, 5-year mortality, and recurrence after stroke in young and middle-aged individuals.

ICH, intracerebral hemorrhage; IS, ischemic stroke; RR, risk ratio.
Risk ratios quantify temporal changes in outcomes by comparing the latest with the earliest (reference) reporting period.
The reported pooled proportions or cumulative incidence rates excluded three studies reporting mortality for patients with IS and TIA. Results including these studies were as follows: 1-year mortality, IS, ⩽60–65: <2000: five studies, 10.0%, 95% CI = 5.6–15.4; 1-year mortality, IS, ⩽40–55: <1990: six studies, 10.0%, 95% CI = 8.1–12.2; 1990–1999: nine studies, 5.2%, 95% CI = 3.1–7.7; ⩾2010: eight studies, 3.7%, 95% CI = 2.9–4.6; 5-year mortality, IS, ⩽58–65: 1990–1999: four studies, 15.1%, 95% CI = 8.8–24.5; 5-year mortality, IS, ⩽45–55: 1990–1999, four studies, 8.7%, 95% CI = 4.2–17.3; ⩾2000: five studies, 9.9%, 95% CI = 7.1–13.6.
Among eight studies reporting quantitative trends, seven showed decreases, and one showed no change in 1-year mortality (p = 0.07) (Supplemental Table 9). Meta-regression analyses, including the 45 studies reporting one or multiple periods, showed lower 1-year mortality over time overall and by stroke subtype, age, sex, study design, and geographical region (Supplemental Tables 10 to 13 and Supplemental Figures 27 to 29). Comparisons across time periods showed progressively lower 1-year mortality after all strokes or IS across all age groups (Table 1).
Five-year mortality
Sixty-nine studies reported survival beyond 1 year after stroke. Of these, 48 were excluded (Supplemental Figure 30), leaving 21 studies for analysis: 5 (23.8%) reporting 5-year mortality across multiple periods, 14 (66.7%) for a single period, and 2 (9.5%) with quantitative trends.
Among the five studies reporting multiple periods, 5-year mortality decreased over time for all strokes or IS and ICH (four studies; RR = 0.65, 95% CI = 0.45–0.95; I2 = 77%),7,22,35,50 IS (two studies; RR = 0.63, 95% CI = 0.37–1.06; I2 = 82%),35,51 and ICH (one study; RR = 0.69, 95% CI = 0.55–0.88) 35 (Supplemental Table 14 and Supplemental Figures 31 to 32). Reductions were also observed among 28/30-day survivors for all strokes or IS and ICH,7,22,35 IS, 35 but not ICH 35 (Table 1).
Both studies reporting quantitative trends showed improvements in long-term survival after stroke (p = 0.50) (Supplemental Table 15). Meta-regression analyses, including the 19 studies reporting one or multiple periods, showed lower 5-year mortality in more recent periods (Supplemental Tables 16 to 19), although data for ICH were limited.
Stroke recurrence
Seventy-eight studies reported stroke recurrence. Of these, four provided cumulative incidence estimates across multiple periods: three at 1 year after IS45,52,53 and one at 5 years after all strokes 54 (Supplemental Table 20).
Temporal trends in the 1-year cumulative incidence of recurrence after IS were heterogeneous (RR = 0.82, 95% CI = 0.41–1.65; I2 = 96%) (Supplemental Figure 33). Only one study showed a reduction in recurrence, based on follow-up using ICD codes and comparing 2002–2006 with 1987–1991. 52 Restricting the analysis to more recent comparisons (2002–2006 vs 1997–2001 in this study, and late 2010s vs early 2010s/2000s in the other two studies) reduced heterogeneity and indicated a stable 1-year risk of recurrence (RR = 1.04, 95% CI = 0.78–1.39; I2 = 69%). The remaining study, which also used ICD codes for follow-up, reported no change in the 5-year cumulative incidence of recurrent stroke after all strokes when comparing 1998–2001 with 1986–1989 (RR = 0.94, 95% CI = 0.85–1.03). 54
Of the four studies described above, two also reported trends in stroke recurrence across all ages. In the Danish Stroke Registry, between 2004–2006 and 2016–2018, the age- and sex-adjusted 1-year recurrence rate after IS decreased by 25% across all ages, whereas the 1-year cumulative incidence of recurrence remained unchanged among adults aged 18–49 years. 53 In an administrative data-based study from Scotland, between 1986 and 2001, the adjusted 5-year rate of hospitalization for recurrent stroke decreased by 27% across all ages, whereas the 5-year cumulative incidence of hospitalization for recurrent stroke was unchanged among individuals aged <65 years. 54
Additional studies reporting stroke recurrence are summarized in Supplemental Table 21. The annualized rate of recurrent IS after IS ranged from 0% to 8.0% across 23 studies with follow-up durations of 2 to 17 years. The annualized rate of recurrent IS or TIA after IS and/or TIA ranged from 3.1% to 11.7% across four studies with follow-up durations of 1 to 6 years. The annualized rate of recurrent ICH after ICH ranged from 0.3% to 1.5% across four studies with follow-up durations of 3 to 17 years.
Myocardial infarction, composite vascular events, venous thromboembolism, and bleeding
Due to the limited number of studies and variability in outcome definitions, temporal trends could not be assessed quantitatively for myocardial infarction, composite vascular events, venous thromboembolism, or bleeding. Studies reporting these outcomes are described in the Supplemental Material. The annualized incidence of myocardial infarction or acute coronary syndrome ranged from 0% to 1.6% across 15 studies with follow-up durations of 2 to 12 years (Supplemental Table 22). In a study from the Helsinki Young Stroke Registry, the 5-year cumulative incidence of composite ischemic arterial events (of which >80% were IS) remained stable between 1994 and 2004, with risks of 11.1% between 1994 and 1999 and 12.0% between 2000 and 2004. 55 The annualized incidence of venous thromboembolism ranged from 0.2% to 0.5% across two studies with follow-up durations of 3 to 10 years. Three studies reported bleeding risk with heterogeneous outcome definitions (Supplemental Table 23).
Discussion
In this systematic review and meta-analysis, we found that early case fatality after stroke in young and middle-aged individuals has steadily declined since the 1970s in high-income countries. This improvement was consistent across patient (age, sex, stroke subtype) and study characteristics (design, sample size, outcome definition, geographical region) and was sustained at 1 and 5 years after stroke. In contrast, temporal trends in stroke recurrence were heterogeneous and appeared to plateau after 2000.
Our finding of improved early case fatality at younger ages is consistent with studies reporting temporal trends across all ages.6,14 Unlike for incidence, the magnitude of decline in case fatality was similar in younger and older individuals, with no evidence of an age-specific divergence. These improvements were most likely driven by the advances in acute stroke care over the past 30 years, including the widespread implementation of stroke units in the 1990s, decompressive craniectomy in the early 2000s–2010s, and mechanical thrombectomy in the mid-2010s, all of which reduce stroke-related mortality.56–58
Although improvements in acute stroke care likely contributed to the observed decline in case fatality, changes in ascertainment cannot be excluded, especially because a large proportion of strokes at younger ages are mild. 59 Over the study period, increased access to magnetic resonance imaging (MRI) and the transition from a time- to a tissue-based definition of IS may have led to a higher proportion of mild strokes being diagnosed, potentially influencing case fatality estimates, especially after 2000.10,60 Even so, case fatality also declined in population-based studies, which consistently ascertained patients using the time-based definition of IS, and after ICH, for which diagnosis is less dependent on MRI. However, the reduction in case fatality was greater in studies with larger increases in stroke counts over time. While such increases may reflect changes in population size or stroke incidence, these may also indicate improved detection or increased hospital admission of mild events, particularly for IS and in studies based on administrative data. We were unable to pool temporal trends in case fatality by stroke severity. A study from the Danish Stroke Registry (2005–2018) showed that the incidence of IS among individuals aged 18–49 years increased only for mild strokes, whereas case fatality declined primarily for moderate and severe strokes. 10 Together, these findings suggest that both increased detection of mild strokes and improvements in acute care may have contributed to the observed decline in case fatality. Future studies should continue to monitor these trends and should report outcomes stratified by stroke severity.
We also observed improvements in survival at 1 and 5 years after stroke in young and middle-aged individuals. Importantly, gains were also seen in 28/30-day survivors for all strokes and IS, indicating that improvements in long-term survival were not solely driven by reductions in early case fatality. Although the cumulative incidence of 5-year mortality after stroke was lower in more recent time periods, long-term survival plateaued after 2007 in South London (UK) and 2010 in Cincinnati (US).51,61 In the included studies, most long-term deaths after stroke were secondary to cardiac causes, recurrent stroke, or malignancy, highlighting the need for further improvements in secondary prevention strategies.35,62
Few studies have evaluated temporal trends in stroke recurrence at younger ages, and results were heterogeneous. We observed no clear change in recurrence rates after 2000. However, these findings should be interpreted with caution. Definitions of recurrence were often unclear or inconsistent across studies, and such differences are strongly associated with early recurrence risk. 63 Only one study reported a reduction in recurrence across multiple periods, but this analysis relied on ICD codes alone for case ascertainment, 52 which may miss early recurrences and introduce bias trends if coding accuracy changes over time. 64 Improved access to MRI, the transition from a time- to a tissue-based definition of IS and changes in care-seeking behavior may have increased the detection of mild recurrent strokes in more recent time periods. Two studies reported that recurrence rates stagnated at younger ages and improved at all ages.53,54 Potential age-related differences in temporal trends in stroke recurrence should be explored in future studies stratified by stroke etiology and accounting for changes in case mix.
There were insufficient data to assess temporal trends in other outcomes, including major bleeding and cardiovascular events, which are important for determining the overall burden of stroke at younger ages. Future studies should assess these trends using standardized definitions and consistent methods of ascertaining outcomes.
Our findings have important clinical and research implications. First, the combination of increasing stroke incidence and declining case fatality implies that the number of young stroke survivors is likely rising, justifying the need for dedicated clinical services and additional research to address the specific impacts of stroke in the young. Further increases in prevalence are also expected with continued improvements in the management of ICH and acute stroke recanalization therapies. Second, the sustained improvement in survival up to 5 years after stroke suggests that advances in stroke care truly improved outcomes rather than simply delaying death. However, we did not measure temporal trends in disability, return to work, quality of life, or cognitive impairment, which are important elements of stroke burden at younger ages and should be evaluated in future studies. Finally, the potentially stagnating recurrence rates emphasize the need to improve control of traditional risk factors, which is frequently suboptimal in younger patients. 65 Future trials should aim to include young patients, who more frequently present with cryptogenic stroke and for whom etiology-specific treatments are often lacking.
Limitations
This analysis has several limitations. First, there was a high degree of statistical heterogeneity for temporal trends in case fatality, as measured by the I2. However, directions of effect were qualitatively consistent across studies, and high I2 values likely reflect the large sample sizes and narrow CIs of administrative-based studies, as well as differences in the number of years between the compared time periods. Second, data on stroke severity were unavailable in most included studies. We used changes in stroke counts as a proxy measure for potential improvements in the ascertainment of mild strokes, but this approach requires further validation. Similarly, we were unable to adjust for other differences in case mix (e.g. stroke etiology), which may have contributed to residual confounding in the observed temporal trends. Third, the restriction of this review to high-income countries limits generalizability to low- and middle-income countries, where an estimated 89% of strokes at younger ages occurred in 2021. 4 In addition, although the incidence of young stroke varies by ethnicity, there were insufficient data to assess temporal trends across ethnic groups. Fourth, we did not contact study authors for additional data and relied on reported time periods, using midpoints as a proxy for time. We attempted to minimize reporting bias by extracting data from graphs and summary results when possible and by including studies that only reported qualitative trends. Fifth, most of the identified studies for ICH had administrative or hospital-based designs and provided limited data regarding long-term survival and stroke recurrence.
Conclusion
The age-related divergence in stroke incidence since the early 21st century has been accompanied by improvements in early case fatality and long-term survival among young and middle-aged individuals. These trends likely reflect advances in acute stroke care and potential changes in stroke severity. In contrast, stroke recurrence in this population may have stagnated over the past 2 decades, underscoring the need for further research using standardized methods to define and ascertain recurrence, as well as for improved secondary prevention strategies in younger populations.
Supplemental Material
sj-docx-1-wso-10.1177_17474930261447879 – Supplemental material for Temporal trends in case fatality, long-term survival, and vascular events after stroke in young and middle-aged individuals: A systematic review and meta-analysis
Supplemental material, sj-docx-1-wso-10.1177_17474930261447879 for Temporal trends in case fatality, long-term survival, and vascular events after stroke in young and middle-aged individuals: A systematic review and meta-analysis by Ahmad Nehme and Linxin Li in International Journal of Stroke
Footnotes
Acknowledgements
None.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr Nehme is funded by the Oxford University Clarendon Scholarship and the Fonds de Recherche du Québec (![]() ); Dr Li is funded by the NIHR Advanced Fellowship and the Oxford Brain Science Fellowship. The funders had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the article; and decision to submit the article for publication.
); Dr Li is funded by the NIHR Advanced Fellowship and the Oxford Brain Science Fellowship. The funders had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the article; and decision to submit the article for publication.
Ethical Approval
Not applicable.
Data availability statement
The data included in this systematic review are available in the source manuscripts.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.