
Abstract
Introduction:
Although the efficacy and safety of endovascular treatment (EVT) for large-core ischemic stroke have been proven, most trials used perfusion imaging or included early-window patients, limiting generalizability to the late window, particularly in developing countries.
Aim:
We aimed to evaluate the safety and functional outcomes of EVT in large-core stroke patients treated between 12 and 24 h (late window) from last known well (LKW).
Methods:
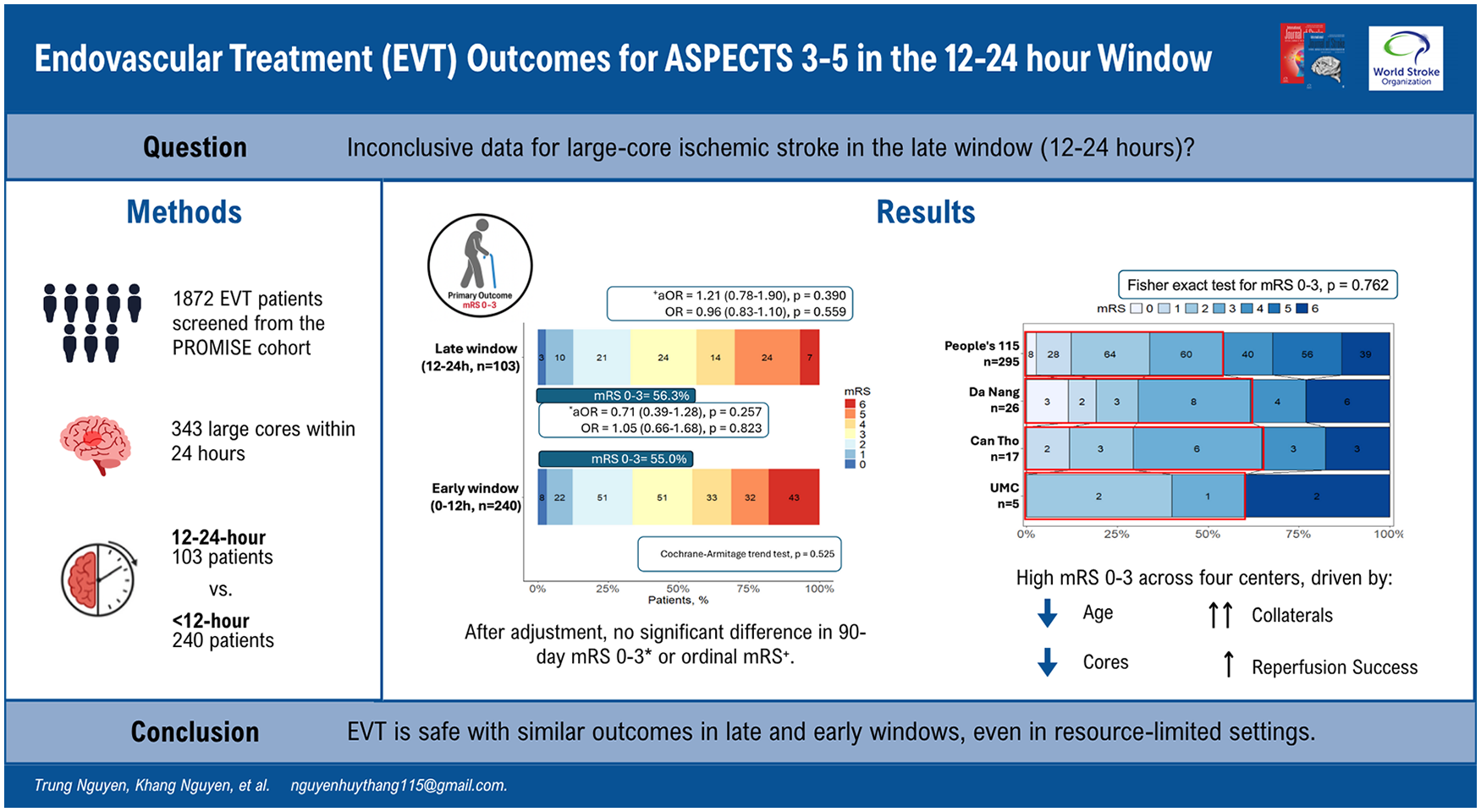
We conducted a prospective, multicenter observational study across four comprehensive stroke centers in Vietnam, enrolling consecutive patients who underwent EVT within 24 h of symptom onset between August 2023 and September 2024. Large core was defined by an Alberta Stroke Program Early CT Score (ASPECTS) of 3 to 5 on non-contrast computerized tomography (NCCT) or diffusion-weighted magnetic resonance imaging (DWI-MRI). Patients who underwent EVT within 12–24 h after LKW were compared to those treated before 12 h (early window). Primary and safety outcomes were independent ambulation (90-day modified Rankin scale (mRS) = 0–3) and symptomatic intracranial hemorrhage (sICH). Secondary outcomes were 90-day mRS 0–2, ordinal mRS, successful reperfusion (modified Thrombolysis in Cerebral Infarction score ⩾2b, early neurological deterioration (END)), and 90-day mortality.
Results:
Of 1872 patients receiving EVT, 343 with large ischemic cores (median age = 64.0 years, 33.8% female) were included, with 103 (30.0%) treated in the 12- to 24-h window. Compared to early-window patients, late-window patients had lower rates of intravenous thrombolysis (2.9% vs. 32.9%, p < 0.001), higher brain MRI use (51.5% vs. 16.2%, p < 0.001), and longer pre-treatment imaging-to-groin puncture times (106 vs. 77 min, p < 0.001). After adjusting for confounders, there were no significant differences in 90-day mRS 0–3 (56.3% vs. 55.0%, adjusted odds ratio (aOR) = 0.71, 95% confidence interval (CI) = 0.39–1.28, p = 0.26), ordinal mRS (aOR = 1.21, 95% CI = 0.78–1.90, p = 0.39), and sICH (aOR = 1.12, 95% CI = 0.32–3.50, p = 0.85). Other secondary outcomes were also similar.
Conclusion:
In patients with anterior circulation large vessel occlusion stroke and low ASPECTS, EVT at 12–24 h versus <12 h from symptom onset showed no significant differences in clinical or safety outcomes. Larger trials are needed to confirm these findings, especially in developing regions.
Keywords
Get full access to this article
View all access options for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.