
Abstract
Introduction:
The impact of leptomeningeal collateralization on the efficacy of mechanical thrombectomy (MT) in patients with anterior circulation large vessel occlusion (aLVO) presenting in the 6-24 h time window remains poorly elucidated.
Patients and methods:
Retrospective multicenter study of aLVO patients presenting between 6 and 24 h after stroke onset who received MT plus Best Medical Treatment (BMT) or BMT alone. Leptomeningeal collateralization was assessed using single-phase computed tomography angiography (grade 0: no filling; grade 1: filling ⩽50%; grade 2: filling >50% but <100%; grade 3: filling 100% of the occluded territory). Inverse probability of treatment weighted ordinal regression was performed to assess the association between treatment and shift of the modified Rankin Scale (mRS) score toward lower categories at 3 months. We used interaction analysis to explore differential treatment effects on functional outcomes (probabilities for each mRS subcategory at 3 months) at different collateral grades.
Results:
Among 363 included patients, 62% received MT + BMT. Better collateralization was associated with better functional outcomes at 3 months in the BMT alone group (collateral grade 1 vs 0: acOR 5.06, 95% CI 2.33–10.99). MT + BMT was associated with higher odds of favorable functional outcome at 3 months (acOR 1.70, 95% CI 1.11–2.62) which was consistent after adjustment for collateral status (acOR 1.54, 95% CI 1.01–2.35). Regarding treatment effect modification, patients with absent collateralization had higher probabilities for a mRS of 0–4 and a lower mortality at 3 months for the MT + BMT group.
Discussion and conclusion:
In the 6-to-24-h time window, aLVO patients with absent leptomeningeal collateralization benefit most from MT + BMT, indicating potential advantages for this group despite their poorer baseline prognosis.

Introduction
Mechanical thrombectomy (MT) is the standard of care for anterior circulation large vessel occlusion (aLVO) within the first 24h of symptom onset in selected patients.1,2 Current European and American guideline recommendations for patient selection in the 6-24 h (“extended”) time window are still essentially based on perfusion imaging.3,4
Recent randomized trials have examined computed tomography (CT) based selection algorithms using ubiquitously available native and angiographic data.5–7 MR CLEAN-LATE was the only study to evaluate the efficacy of MT in the extended time window based on collateral flow on CT angiography (CTA) and included patients with poor (grade 1 (according to Tan et al. 8 ) with collateral filling ⩽50% but >0%), moderate (grade 2, collateral filling >50% but <100%), and good (grade 3, 100% collateral filling) collateralization on CTA, with a prespecified enrollment of 100 patients with poor collateral status. 9 A total of 113 patients with collateral grade 1 and 26 patients with absent collaterals (collateral grade 0, no collateral filling) were enrolled. 7 MT was superior to standard medical treatment alone (including intravenous thrombolysis) in patients selected based on collateral status, with the effect being independent of the degree of collateralization. 7 In addition, an effect modification of MT by collateral status was demonstrated, with the beneficial effect being greatest in the collateral grade 1 group and decreasing further across group 2 to 3. 7
These results support that the ischemic core growth rate influences the efficacy of MT, with fast core growth being associated with a greater benefit from MT. The group with the fastest core growth rate, based on collateral status as an imaging surrogate marker, are those with collaterals grade 0. However, the latter was underrepresented in MR CLEAN-LATE. One reason for a deliberate prespecified limited inclusion of these patients could be that those with absent collaterals may exhibit the least ischemic tolerance, potentially diminishing the effect of MT.
In a real-world multicenter cohort of adult patients with aLVO presenting in the extended time window, we aimed to investigate: (i) whether the beneficial effect of MT + BMT was preserved in a less preselected cohort with a higher proportion of individuals with absent leptomeningeal collaterals, and (ii) how the absence of collateralization influenced the treatment effect on functional outcome.
Patients and methods
Study design, setting, and data collection
This retrospective Swiss multicenter cohort study is based on data from six stroke centers from January 2014 to November 2022. It includes the RESCUE cohort,10,11 extended by data from the Cantonal Hospital St. Gallen (approximately 43% of the total current study cohort).
In RESCUE, we collected data from adult (⩾18 years) aLVO patients who either received MT + BMT or BMT alone (including intravenous thrombolysis) in the extended time window to examine treatment-related efficacy and safety aspects. Eligibility criteria were aLVO (imaging-confirmed occlusion of the internal carotid artery, M1 or M2 segment of the middle cerebral artery), admission between 6 and 24 h after symptom onset (or last-seen-well), and available cerebral perfusion imaging data (CT or MRI). Patient identification and clinical data extraction were performed via the Swiss Stroke Registry.
For this study, only patients with available CTA were included. The identification of eligible patients treated at the Cantonal Hospital St. Gallen was performed based on the same eligibility criteria (except for the previous requirement of available perfusion imaging) as in RESCUE. Clinical data were also retrieved from the Swiss Stroke Registry. For the University Hospital Basel and the Cantonal Hospital St. Gallen, the data collection period was extended to November 2022.
This study was approved by the Ethics Committee Northwestern and Central Switzerland (EKNZ ID: 2020-00552, 2023-00268) in advance.
Treatment modalities
Treatment modalities included MT + BMT versus BMT alone. BMT included intravenous thrombolysis and other conservative therapeutic measures used in acute care (e.g. blood pressure lowering in cases of severe hypertensive derailment).
Leptomeningeal collateralization assessment
The leptomeningeal collateralization degree was assessed on baseline single-phase CTA (peak arterial phase) following a validated 4-point scale 8 (grade 0: no collateral filling; grade 1: collaterals filling ⩽50% of the occluded territory; grade 2: collaterals filling >50% but <100% of the occluded territory; grade 3: collaterals filling 100% of the occluded territory).
Two independent reviewers (TDD, TVS) blinded to cohort characteristics, treatment allocation, and functional outcomes interpreted each CTA. In case of discrepant ratings, a third independent reviewer (AMT) evaluated the collateral status to reach majority consensus.
Outcome measures
The efficacy outcome measure was defined as a shift on the modified Rankin Scale (mRS) score toward lower categories at 3 months. For the visual group comparisons (as patients with premorbid functional impairment [mRS score > 2] were also included), a stable mRS at 3 months was considered to be an excellent functional outcome. The modality of 3-month follow-up was left to the discretion of each participating center and included in-person clinic visits, telephone interviews, and medical record reviews.
Statistical analysis
Medians with interquartile ranges (IQR) were used to present categorical and continuous variables, whereas numbers with percentages were used for dichotomous variables. Comparisons between groups were performed using the Wilcoxon rank-sum test and Pearson’s chi-squared test, as appropriate. For the comparison of study cohort characteristics, the entire cohort was considered (N = 363).
First, we performed unweighted univariable ordinal logistic regression analyses in which we examined the influence of different covariables on the odds of a shift toward a lower mRS category.
We then performed inverse probability of treatment weighted (IPTW) analyses based on the propensity score as previously described 11 to examine: (i) the influence of treatment allocation (MT + BMT vs BMT) on functional outcome at 3 months, and (ii) a modification of observed treatment effects (MT + BMT vs BMT) by leptomeningeal collateralization (collateral grades 0–3). For IPTW, we used the following potentially outcome-relevant covariables: age, sex, diabetes, arterial hypertension, atrial fibrillation, premorbid mRS, National Institutes of Health Stroke Scale (NIHSS) score on admission, systolic and diastolic blood pressure on admission, blood glucose on admission, onset-to-imaging time, treatment with intravenous thrombolysis, symptomatic intracerebral hemorrhage (defined as an imaging confirmed hemorrhage that occurred within 7 days after the index ischemic stroke and was accompanied by a clinical deterioration of ⩾4 points in the NIHSS score). Multicollinearity diagnostics (using variance inflation factors [VIF]) were used to check for autocorrelation between covariables. We excluded patients without complete covariable set from the analyses. We used robust variance estimators and performed balance diagnostics (standardized differences and variance ratios) to assess the influence of weighting on between-group balance (MT + BMT vs BMT).
As a final step, we performed an interaction analysis based on IPTW models and calculated the contrasts of predictive margins to explore the differential treatment effects (MT + BMT vs BMT) on functional outcomes at 3 months (for all mRS subcategories) at different collateral grades. Level of significance was set at <0.05. We report 95% confidence intervals.
All analyses were performed using STATA version 17.0 (StataCorp LLC, College Station, TX).
Results
Study cohort characteristics
Of 363 patients included, 62% received MT + BMT (Figure 1). Patients with MT + BMT were less likely to have previous ischemic strokes (16% vs 25%, p = 0.049), had a lower premorbid mRS (median 0 vs 1, p = 0.001), and were clinically more severely affected at baseline (median NIHSS 14 vs 11, p = 0.03) compared to those who received BMT alone (Table 1). Figure 2 illustrates the mRS distribution at 3 months across different leptomeningeal collateralization grades. It shows a comparable proportion of patients with stable mRS after 3 months in the MT + BMT and BMT groups (14.9% vs 18.0%, p = 0.45).
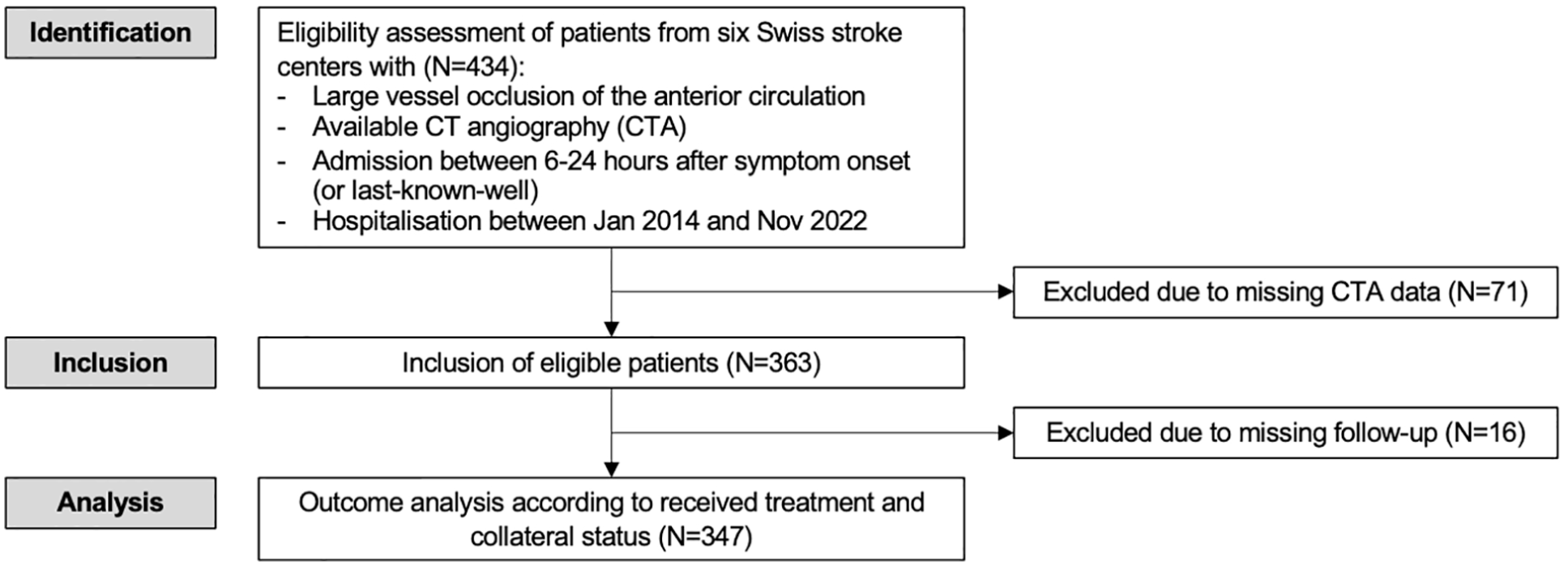
Study flow chart.
Study cohort characteristics.
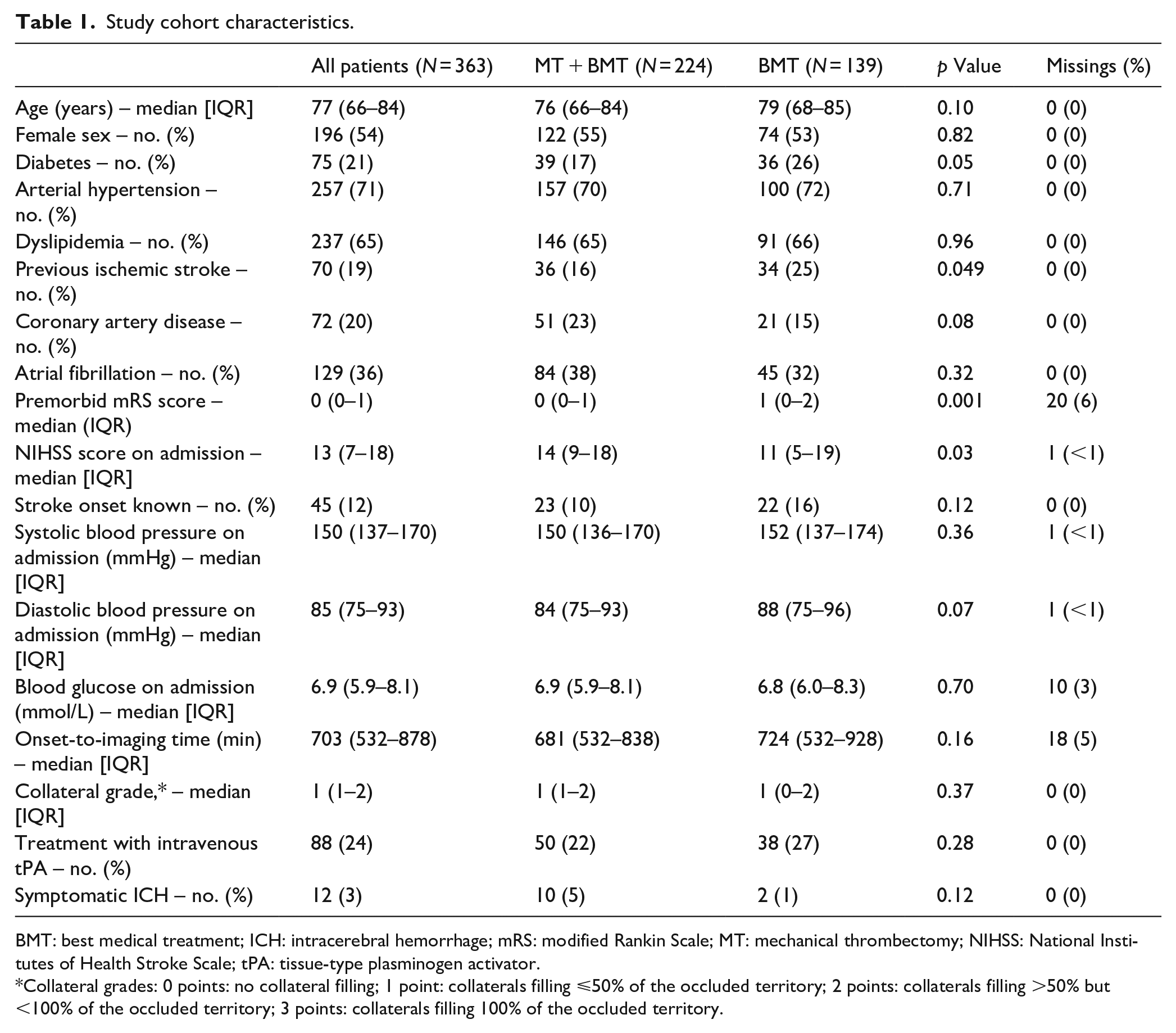
BMT: best medical treatment; ICH: intracerebral hemorrhage; mRS: modified Rankin Scale; MT: mechanical thrombectomy; NIHSS: National Institutes of Health Stroke Scale; tPA: tissue-type plasminogen activator.
Collateral grades: 0 points: no collateral filling; 1 point: collaterals filling ⩽50% of the occluded territory; 2 points: collaterals filling >50% but <100% of the occluded territory; 3 points: collaterals filling 100% of the occluded territory.
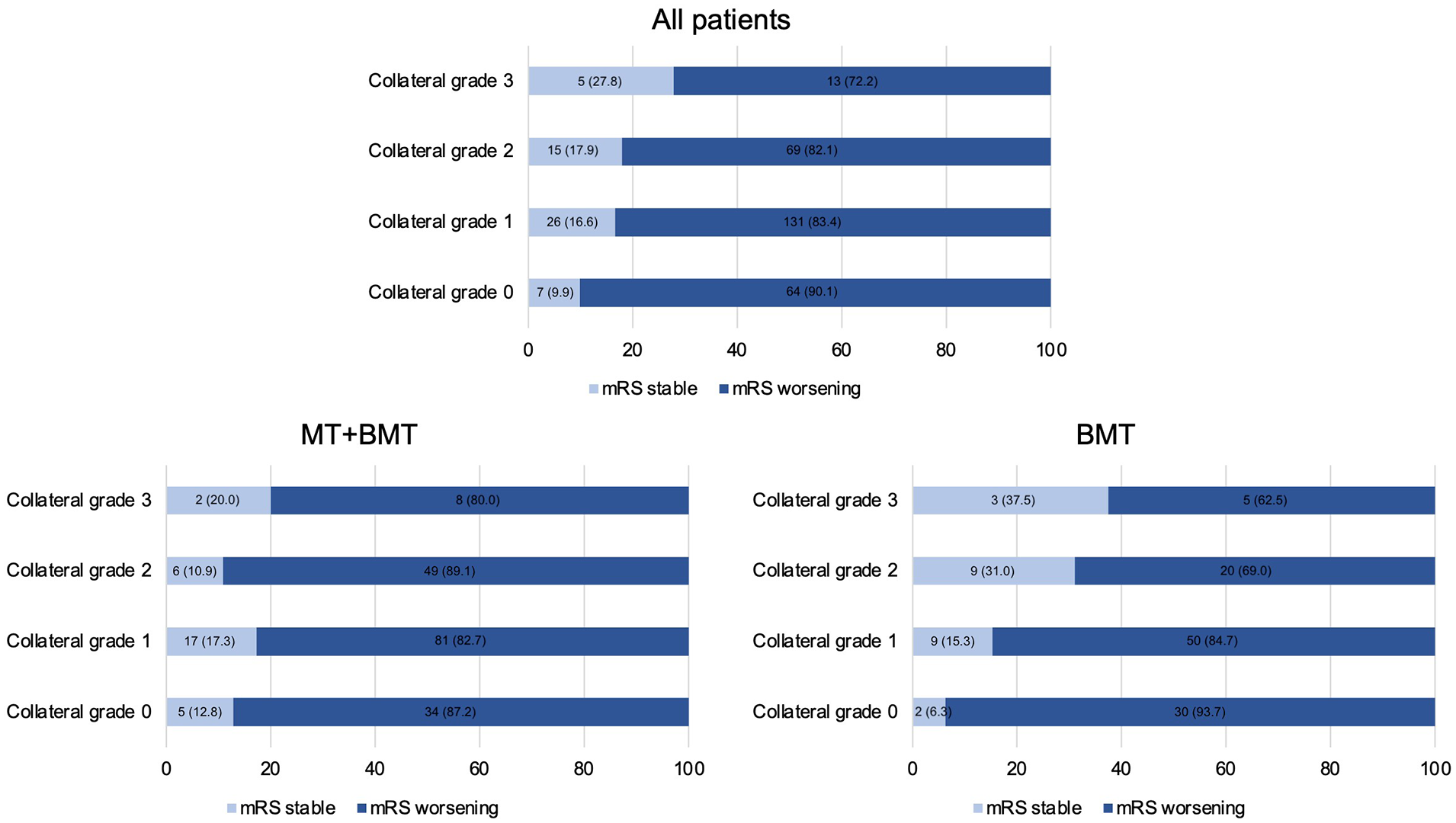
Distribution of functional outcomes at 3 months across different leptomeningeal collateralization grades.
Association of treatment modality and functional outcomes at 3 months
In the unweighted analyses, the univariable model showed higher odds for a shift toward a lower mRS category for the MT + BMT group without reaching statistical significance (cOR 1.18, 95% 0.80–1.72, p = 0.41; Supplemental Table S1). In the IPTW analysis, adjusted for confounders (exclusive leptomeningeal collateralization grades), there was a significant benefit of MT + BMT over BMT alone in terms of higher odds for a shift toward lower mRS categories at 3 months (acOR 1.70, 95% CI 1.11–2.62, p = 0.02) with consistent results after additional adjustment for leptomeningeal collateral status (acOR 1.54, 95% CI 1.01–2.35, p = 0.047; Supplemental Table S2). There was no evidence of multicollinearity, as indicated by VIFs below 10 (Supplemental Table S3). Balance diagnostics showed that weighting improved balance between groups (MT + BMT vs BMT), as reflected by standardized differences closer to zero after weighting for 12 of 13 variables (Supplemental Table S4).
Association between degree of leptomeningeal collateralization and functional outcomes at 3 months
In both treatment groups, highest collateralization grade was associated with highest odds of favorable functional outcome at 3 months (BMT alone group [grade 3 vs 0]: acOR 20.90, 95% CI 1.93–225.84, p = 0.01; MT + BMT [grade 3 vs 0]: acOR 10.03, 95% CI 2.89–34.83, p ⩽ 0.001). Within those with absent collateral flow (i.e. collateral grade 0), MT + BMT was associated with higher odds of favorable functional outcome at 3 months (Supplemental Table S5).
Treatment effect modification by degree of leptomeningeal collateralization
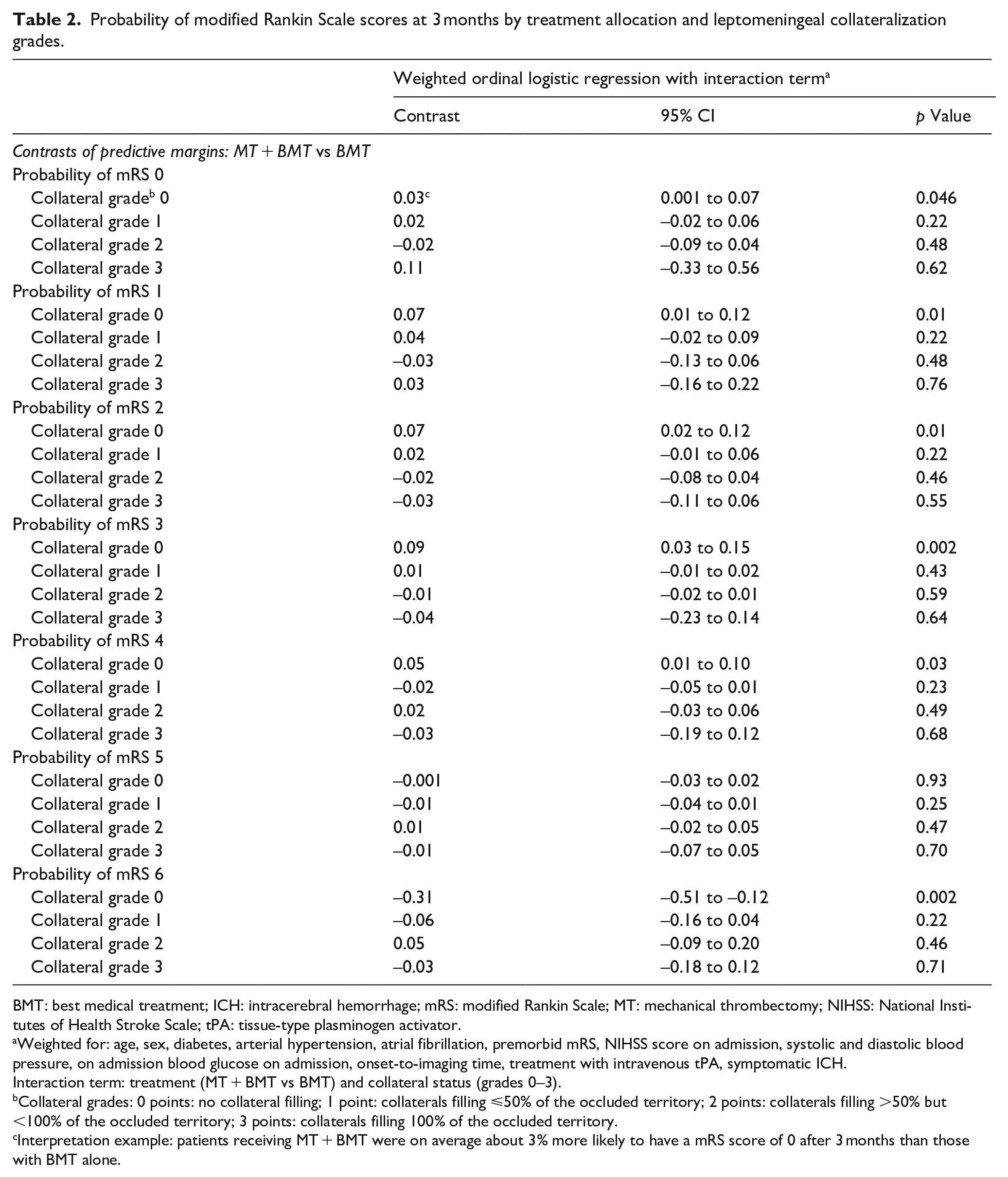
Overall, there was evidence for a significant interaction between treatment allocation and leptomeningeal collateralization (dichotomized collateral score [0 vs 1–3]; pinteraction = 0.03). Within the group with collateral grade 0, consistently higher probabilities for a mRS of 0–4 were found for the MT + BMT group (Table 2). Patients receiving MT + BMT were on average about 3% more likely to have an mRS of 0 after 3 months than those with BMT alone. Conversely, at the other end of the mRS spectrum, MT + BMT patients with collateral grade 0 were on average about 31% less likely to have died (as indicated by an mRS of 6) compared to patients with collateral grade 0 that received BMT alone. For the collateral grade 1 group, we saw effect estimates (except for the mRS 4 subgroup) trending toward the same direction as for the collateral grade group 0 but without reaching statistical significance.
Probability of modified Rankin Scale scores at 3 months by treatment allocation and leptomeningeal collateralization grades.
BMT: best medical treatment; ICH: intracerebral hemorrhage; mRS: modified Rankin Scale; MT: mechanical thrombectomy; NIHSS: National Institutes of Health Stroke Scale; tPA: tissue-type plasminogen activator.
Weighted for: age, sex, diabetes, arterial hypertension, atrial fibrillation, premorbid mRS, NIHSS score on admission, systolic and diastolic blood pressure, on admission blood glucose on admission, onset-to-imaging time, treatment with intravenous tPA, symptomatic ICH.
Interaction term: treatment (MT + BMT vs BMT) and collateral status (grades 0–3).
Collateral grades: 0 points: no collateral filling; 1 point: collaterals filling ⩽50% of the occluded territory; 2 points: collaterals filling >50% but <100% of the occluded territory; 3 points: collaterals filling 100% of the occluded territory.
Interpretation example: patients receiving MT + BMT were on average about 3% more likely to have a mRS score of 0 after 3 months than those with BMT alone.
Discussion
We conducted a retrospective multicenter cohort study of adult aLVO stroke patients presenting between 6 and 24 h after stroke onset to investigate the degree to which collateral status influenced the treatment effects of MT + BMT (vs BMT alone). Our key findings were: (i) MT + BMT was associated with better functional outcomes at 3 months – regardless of the leptomeningeal collateral status; (ii) the favorable effect of MT + BMT varied depending on the degree of collateralization; (iii) patients with absent leptomeningeal collateralization exhibited the greatest benefit from MT + BMT.
Our study builds on the findings of MR CLEAN-LATE, adding novel insights by providing more extensive information on patients with absent leptomeningeal collaterals – a group that was previously underrepresented (MR CLEAN-LATE: 5% of the total cohort [26/535] compared to 20% in the MT + BMT group and 25% in the BMT group in the present study). Patients with absent collaterals had the largest proportion of those with poor (mRS score 3–6) functional outcomes at 3 months. Remarkably, the absence of collaterals did not diminish the beneficial effect of MT but was, on the contrary, the greatest for this group. The observed effects were independent of possible differences in the time between onset (or last-known-well) and performance of CTA between collateral status groups. The comparable proportion of those with excellent functional outcome at 3 months (stable mRS score) between the MT + BMT and BMT alone groups should be interpreted with caution. Patients with stable 3-month mRS score had a higher premorbid mRS score. It should be noted that the distance between mRS categories 0 and 1 may not be clinically equivalent to the distance between categories 1 and 2. For example, a shift from mRS score 0 to 1 is already reached once any residual deficit is detected. In contrast, a more extensive impairment of pre-stroke activities is required for a formal mRS deterioration with a premorbid mRS score of 1.
For the collateral grade 1 group, the effect directions across mRS categories were largely congruent with those of the grade 0 group, albeit lacking statistical significance. We saw a consistent trend toward wider 95% confidence intervals with increasing collateral grades. The increase in estimation imprecision could be due to a higher variability within higher collateral groups or the different collateral group sizes. At least for the groups with collateral grades 2 and 3 (which accounted for 27% and 6%, respectively), it is conceivable that the analyses were underpowered given an expected smaller effect size than in the lower categories based on the results of MR CLEAN-LATE and our current analyses. Furthermore, an uneven distribution of occlusion sites and, thus, of baseline (and expected final) infarct core sizes is possible. In RESCUE, occlusion sites were determined based on angiographic data, and perfusion imaging was evaluated by automated software. Performing perfusion imaging was not mandatory for patients included in this study. However, given that the aLVO definition was relatively restrictive, we consider a significant confounding unlikely.
Our findings may have implications for future trial designs: Patients presenting between 6 and 24 h with absent collateralization should not necessarily be excluded from trials in which CTA-based MT selection algorithms are applied. Despite the potential unfavorable prognostic implications of absent collateral flow, these patients may potentially benefit most from MT compared with BMT alone. One reason for the limited data on patients with absent collateralization might be their comparably (to collateral grades 1–3) low ischemic tolerance due to a faster core growth rate, which could cast doubt on the efficacy of MT for these patients in the extended time window of up to 24 h after stroke onset.
The time between stroke symptom onset and treatment initiation is a crucial factor for the efficacy of MT. 12 In DEFUSE-3, the clinical benefit of MT was comparable to that of perfusion imaging selected patients within the first 6 h. 1 An explanation for this observation might be an interindividual variation in the ischemic core progression rate, as patients with poor collaterals develop large core volumes more rapidly than those with good collateralization.13,14 Within the first 4.5 h after symptom onset, fast core growth has already been found to be associated with a greater benefit of MT (compared to intravenous thrombolysis alone). 15 For the extended time window, an analysis of the DAWN trial population showed that good collateralization was associated with slower stroke progression and resulted in better functional outcomes. 16 However, no significant interaction between MT and the degree of collateralization was shown. 16 In MR CLEAN-LATE, the effect estimates (MT + BMT vs BMT) decreased steadily from collateral grade 1 to grade 3. 7
Our findings add to the existing but limited body of evidence that patients with absent collaterals on CTA (i.e. fastest core progression) might benefit most from MT + BMT compared with standard medical care, even though they may initially have larger ischemic cores and demonstrate worse 3 months functional outcomes. However, it should be noted that overall, the proportion of those with poor outcome remains relatively high even in the MT + BMT group (76% with mRS 3–6 at 90 days).
Strengths and limitations
Our study has several strengths and limitations. Strengths include that: (i) we obtained standardized clinical data from a prospectively maintained national stroke registry; (ii) we used propensity-score-based analyses to address the risk of selection bias (inherent to the retrospective design) as best as possible. Limitations include: (i) the nonrandomized study design with a residual confounding risk due to unobserved or unmeasured confounders; (ii) the lack of imaging-based tissue outcome parameters. Especially the missing information on core sizes on baseline imaging is a limiting factor, particularly concerning whether patients with missing collaterals also had larger ischemic cores compared to patients with higher collateral grades, as might be expected; (iii) the limited generalizability of the results to other regions or countries with different structural prerequisites concerning acute stroke care; (iv) the ASPECTS and exact site of vessel occlusion were not systematically recorded for the present cohort.
Conclusion
Among adult stroke patients with aLVO presenting between 6 and 24 h after stroke onset, the combination of MT and BMT was associated with improved functional outcomes at 3 months, independent of collateral status. Moreover, patients with absent leptomeningeal collateralization exhibited the greatest benefit from MT with BMT, suggesting that these individuals might derive substantial advantages from the intervention despite their overall poorer prognosis.
Supplemental Material
sj-doc-1-eso-10.1177_23969873241239208 – Supplemental material for Absent leptomeningeal collateralization is associated with greatest benefit from mechanical thrombectomy in the 6-24 hour time window
Supplemental material, sj-doc-1-eso-10.1177_23969873241239208 for Absent leptomeningeal collateralization is associated with greatest benefit from mechanical thrombectomy in the 6-24 hour time window by Tolga D Dittrich, Tennessee von Streng, Anna M Toebak, Annaelle Zietz, Benjamin Wagner, Martin Hänsel, Raoul Sutter, Mira Katan, Nils Peters, Lars Michels, Zsolt Kulcsár, Grzegorz M Karwacki, Marco Pileggi, Carlo W Cereda, Susanne Wegener, Leo H Bonati, Marios Psychogios and Gian Marco De Marchis in European Stroke Journal
Supplemental Material
sj-docx-2-eso-10.1177_23969873241239208 – Supplemental material for Absent leptomeningeal collateralization is associated with greatest benefit from mechanical thrombectomy in the 6-24 hour time window
Supplemental material, sj-docx-2-eso-10.1177_23969873241239208 for Absent leptomeningeal collateralization is associated with greatest benefit from mechanical thrombectomy in the 6-24 hour time window by Tolga D Dittrich, Tennessee von Streng, Anna M Toebak, Annaelle Zietz, Benjamin Wagner, Martin Hänsel, Raoul Sutter, Mira Katan, Nils Peters, Lars Michels, Zsolt Kulcsár, Grzegorz M Karwacki, Marco Pileggi, Carlo W Cereda, Susanne Wegener, Leo H Bonati, Marios Psychogios and Gian Marco De Marchis in European Stroke Journal
Footnotes
Acknowledgements
None.
Declaration of conflicting interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: MK received speaker honoraria from Medtronic. GMK is on a scientific advisory board of Bayer AG. CWC is member of the Medical and Scientific Advisory Boards of iSchemaView. LHB received personal fees from Claret Medical and InnovHeart. GMDM received speaker honoraria from Medtronic. The remaining authors report no conflicts of interests relevant to this study.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by the Ethics Committee Northwestern and Central Switzerland (EKNZ ID: 2020-00552, ID 2023-00268) in advance.
Informed consent
Patients were informed about the use of their routinely collected data for research purposes. Patients who refused the use of their data were excluded from the analysis.
Guarantor
TDD.
Contributorship
TDD, TVS and GMDM planned the work. TDD and TVS acquired the data and drafted the manuscript. TDD performed the analyses. All authors interpreted the results and substantially contributed to the final manuscript.
Data availability
Anonymized records may be provided upon reasonable request by the corresponding authors.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.