
Abstract
Background and Purpose:
Cervical artery dissection (CAD) involving the carotid or vertebral arteries is an important cause of stroke in younger patients. The purpose of this systematic review is to assess the risk of recurrent CAD.
Methods:
A systematic review and meta-analysis was conducted on studies in which patients experienced radiographically confirmed dissections involving an extracranial segment of the carotid or vertebral artery and in whom CAD recurrence rates were reported.
Results:
Data were extracted from 29 eligible studies (n = 5898 patients). Analysis of outcomes was performed by pooling incidence rates with random effects models weighting by inverse of variance. The incidence of recurrent CAD was 4% overall (95% confidence interval (CI) = 3–7%), 2% at 1 month (95% CI = 1–5%), and 7% at 1 year in studies with sufficient follow-up (95% CI = 4–13%). The incidence of recurrence associated with ischemic events was 2% (95% CI = 1–3%).
Conclusions:
We found low rates of recurrent CAD and even lower rates of recurrence associated with ischemia. Further patient-level data and clinical subgroup analyses would improve the ability to provide patient-level risk stratification.
Introduction
Cervical artery dissection (CAD) refers to dissection of the carotid or vertebral artery in an extracranial segment. It is an important cause of stroke, particularly in young adults, in whom CAD is identified as the cause of stroke in 1 in 4 cases. 1 It has been associated with connective tissue disorders, hypertension, certain infections, major trauma, and physical activity (presumably due to mechanical trauma or stretching of the vessel).1–3
In some instances, CAD can recur in the same or another vessel. The prospect of recurrence is perhaps of greatest concern to a young, otherwise healthy, and physically active patient who has sustained an initial CAD with good functional recovery, and who wishes to resume exercise or recreational activities. This question has clear ramifications on quality of life. Recommendations on return to activity are made at the discretion of the individual practitioner, as there are no evidence-based guidelines to inform this discussion. An accurate estimate of the likelihood of recurrent CAD would be a valuable tool in assisting health care providers and patients in making decisions on risk assessment when considering return to activity. While there are individual studies examining the incidence of recurrent CAD, these are limited by small sample size and high degree of variability between studies, thus limiting generalizability. No previous systematic review exists on this topic.
Methods
This systematic review is registered with PROSPERO (registration number CRD42020166105), and methods are detailed in a published protocol. 4 Peer-reviewed search strategy outlined in the protocol was updated to include more recently published studies, up to March 2022, and is available in full in the supplementary files. Two independent reviewers screened articles in a two-level process using a pre-designed form, with screening of the title and abstract during the first phase and screening of the full text during the second phase. Disagreements were adjudicated by a third reviewer. Data extraction was also performed by two independent reviewers using a pre-designed form which was refined after a pilot exercise of the first three studies. Eligible studies included case series, observational studies, and randomized trials involving patients with radiographically confirmed spontaneous or traumatic CAD, provided that recurrence of CAD, defined as a new dissection in the same or another vessel, was reported. Studies of pediatric cohorts were not excluded. Recurrent ischemic events attributed to the initial dissection or from persistent vessel stenosis were not considered to represent recurrent dissection. Imaging modalities and radiologic diagnostic criteria used to confirm diagnosis of dissection were recorded for each study. To mitigate the risk of double counting of the same patient population captured in more than one report, we manually screened for articles written by the same first author, then carefully analyzed the Methods sections to determine possible overlap. Where there was significant overlap, the less recent study was excluded in favor of the study with more recent or more longitudinal data; in instances of only partial overlap, both studies were included.
The minimum follow-up duration was 1 month. The primary outcome is the proportion of patients with recurrent CAD overall, and stratified into predetermined early (at 1 month), intermediate (at 1 year), and late (at 5 years) time points. The latter 5-year recurrence was originally intended to be the primary outcome as specified in the protocol; however, this was revised to overall recurrence given many studies with shorter minimum follow-up periods. These measures were calculated by pooling incidence rates with random effects models weighting by inverse of variance. Individual study and pooled results are presented with their 95% confidence intervals (CIs). A continuity correction of 0.5 was added for studies with 0 events.
Subgroup analyses pre-specified in the protocol include studies with low risk of bias (as assessed using Hoy et al.’s tool for prevalence studies), 5 and subgroups based on sex, presence or absence of connective tissue disease (CTD), vessel involved in initial dissection, and spontaneous or traumatic mechanism of initial dissection. A post hoc subgroup analysis was added to examine recurrence in studies which did and did not include routine surveillance imaging as part of the follow-up protocol, as we hypothesized that there may be higher recurrence rates in some studies as a result of asymptomatic findings incidentally visualized on imaging.
Clinically, pooling across studies was appropriate given that the studies included addressed the question at hand in a relatively homogeneous way with respect to population and outcomes. Statistically, heterogeneity was assessed using I 2 , with thresholds based on the Cochrane Handbook for Systematic Reviews. 6
Results
A total of 1567 records were identified from databases, with 44 duplicate records removed before screening. In total, 1412 reports were excluded based on title and abstract screening. Reasons for exclusion at the level of full-text screening were outcomes (n = 37), study design (n = 35), patient population (n = 6), and language (n = 4). Cohen’s Kappa coefficient as a measure of inter-rater reliability at the level of full-text screening was 0.80.
Twenty-nine studies7–35 (n = 5898 patients) were eligible for inclusion in this systematic review, including 16 prospective observational studies, 11 retrospective observational studies, and 2 case series.7–35 Many studies reported recurrence of ischemic events (stroke or transient ischemic attack) in addition to recurrence rate (or absence of recurrence) of CAD (Table 1).
Results for included studies, including overall recurrence of cervical artery dissection (CAD), recurrence at 1 month and 1 year, and recurrent dissection symptomatic of ischemia.
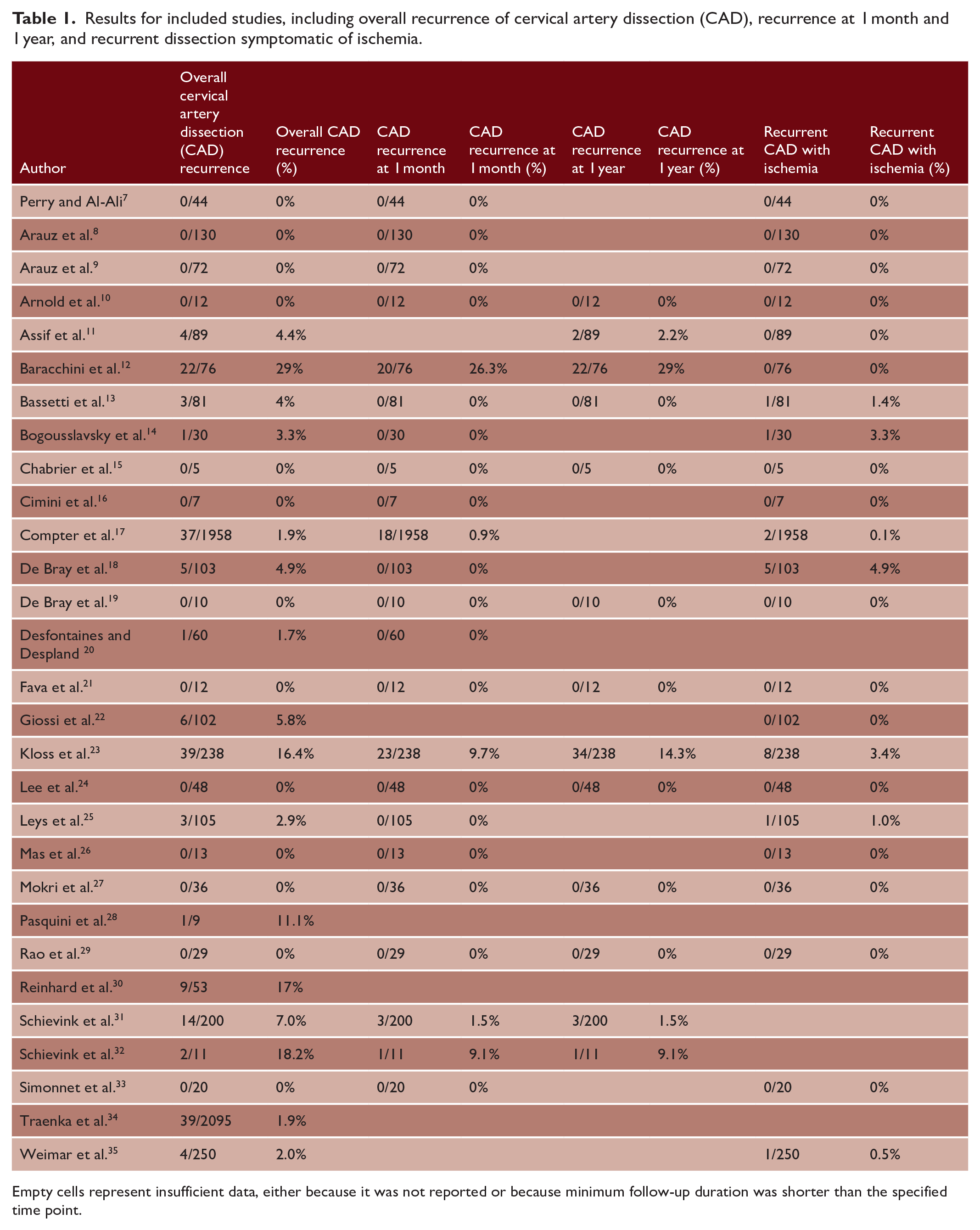
Empty cells represent insufficient data, either because it was not reported or because minimum follow-up duration was shorter than the specified time point.
Year of publication ranged from 1986 to 2021. The mean age of the population in each study ranged from 7.75 (in a study of pediatric patients) 15 to 50.3 years old. Twenty-one studies included patients with CTD; one study excluded these patients, and the remaining seven studies did not specify. Twenty-three studies reported the proportion of patients with traumatic versus spontaneous dissections. Average follow-up period ranged from 3.9 to 93.6 months. Five studies employed a specific antithrombotic protocol (anticoagulation in four studies and dual antiplatelet therapy in one study), while the remainder of studies deferred to the clinician’s discretion for antithrombotic selection. The extracted data for all included reports are available in full in the supplementary files.
Results of meta-analysis suggest that recurrent CAD occurred in about 4% of patients (95% CI = 3–7%) (Figure 1). Risk of recurrence was 2% at 1 month (95% CI = 1–5%) (Figure 2), and 7% at 1 year in the subgroup of studies with sufficient follow-up (95% CI = 4–13%) (Figure 3). Because only one study, which reported no recurrent dissections, had a minimum follow-up period longer than 5 years, we did not analyze data on late recurrences. That being said, late recurrences did occur and were reported in some studies in which some but not all patients had long-term follow-up. The latest reported recurrences occurred at 10 years.11,18 The risk of ischemia from recurrent dissections was approximately 2% (95% CI = 1–3%) (Figure 4).
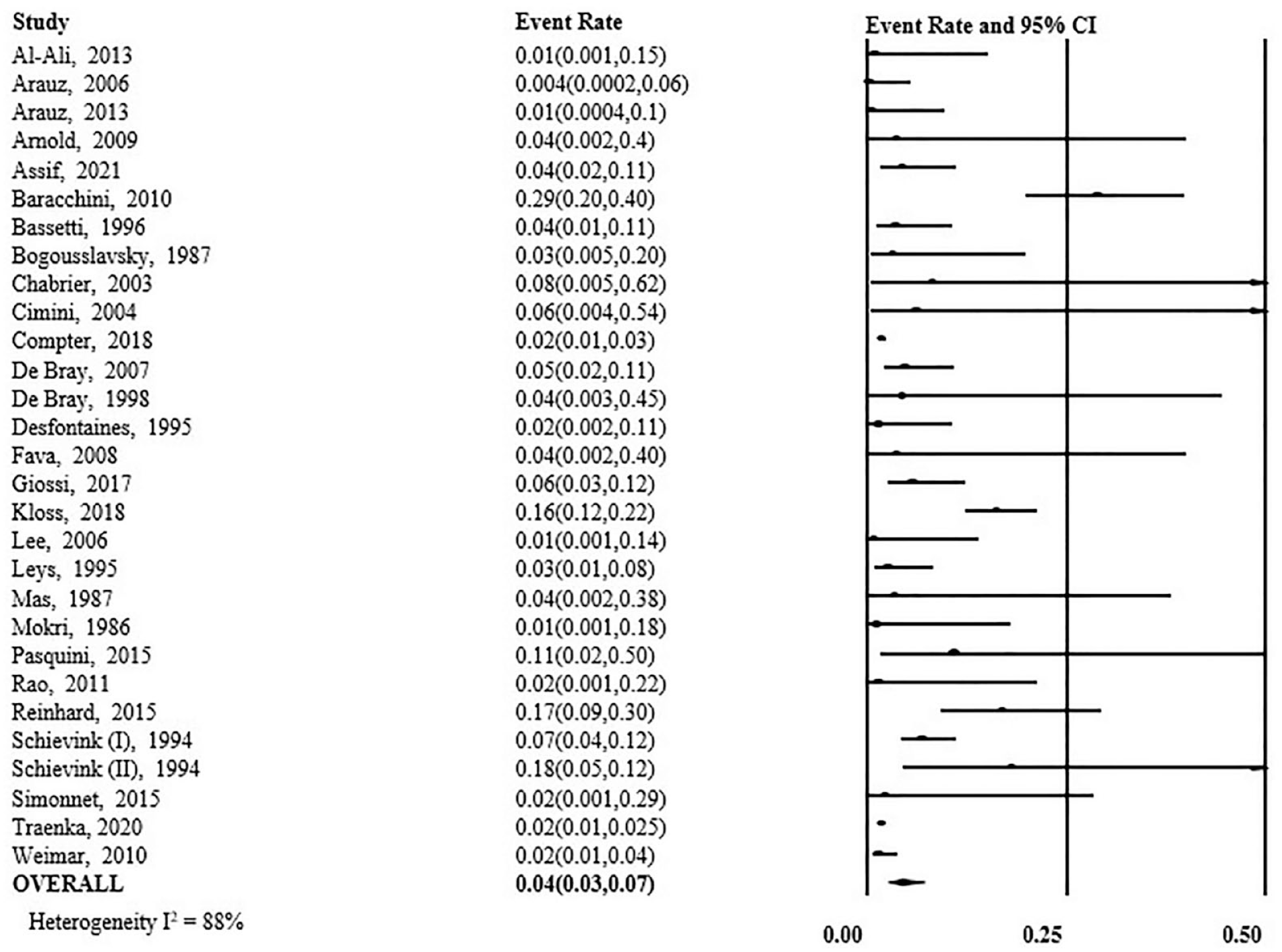
Overall incidence of recurrent cervical artery dissection for each study and overall, presented with their confidence intervals and measure of heterogeneity.
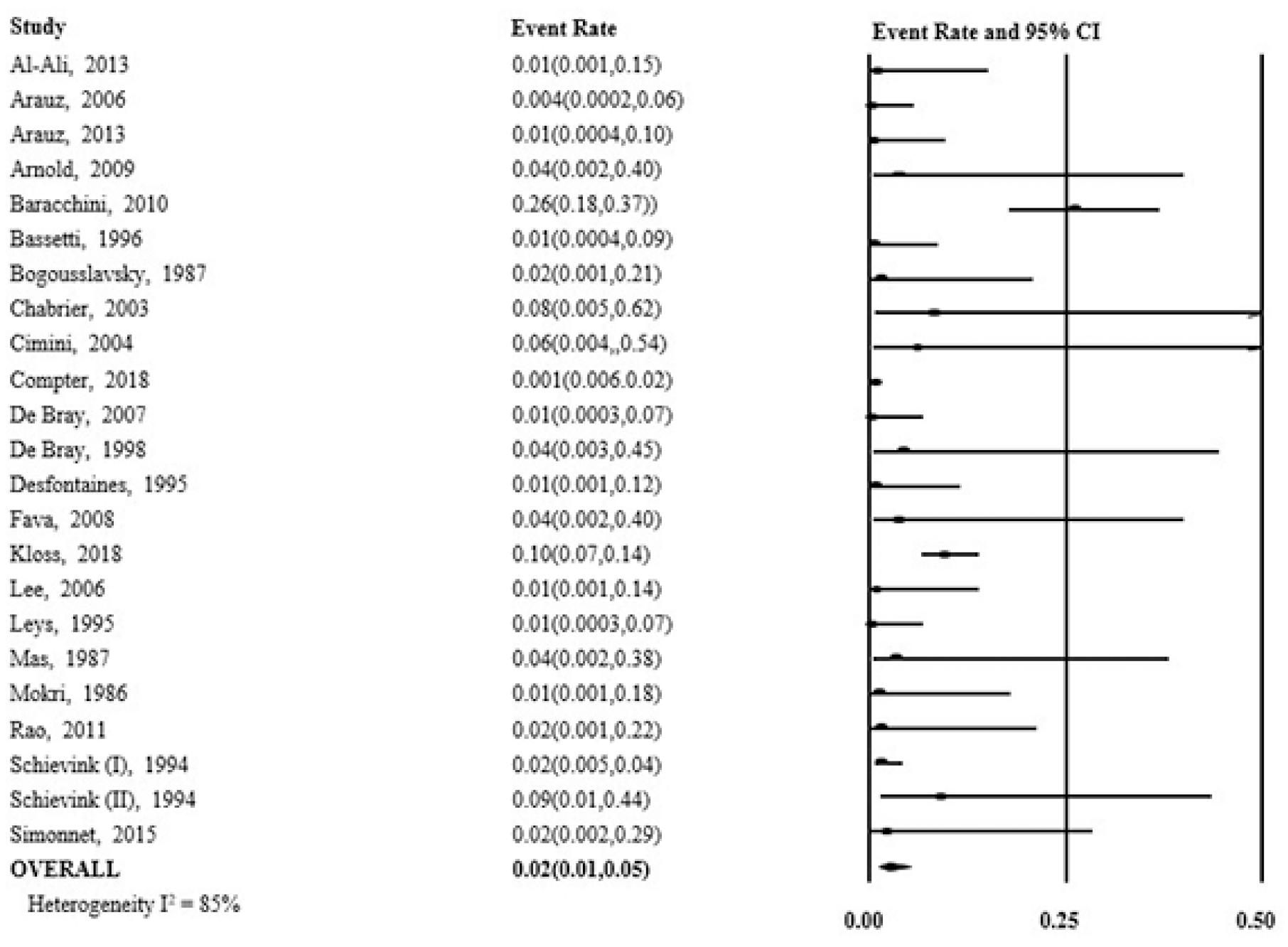
Incidence rates for secondary outcome of recurrent cervical artery dissection at 1 month for each study and overall, presented with their confidence intervals and measure of heterogeneity.
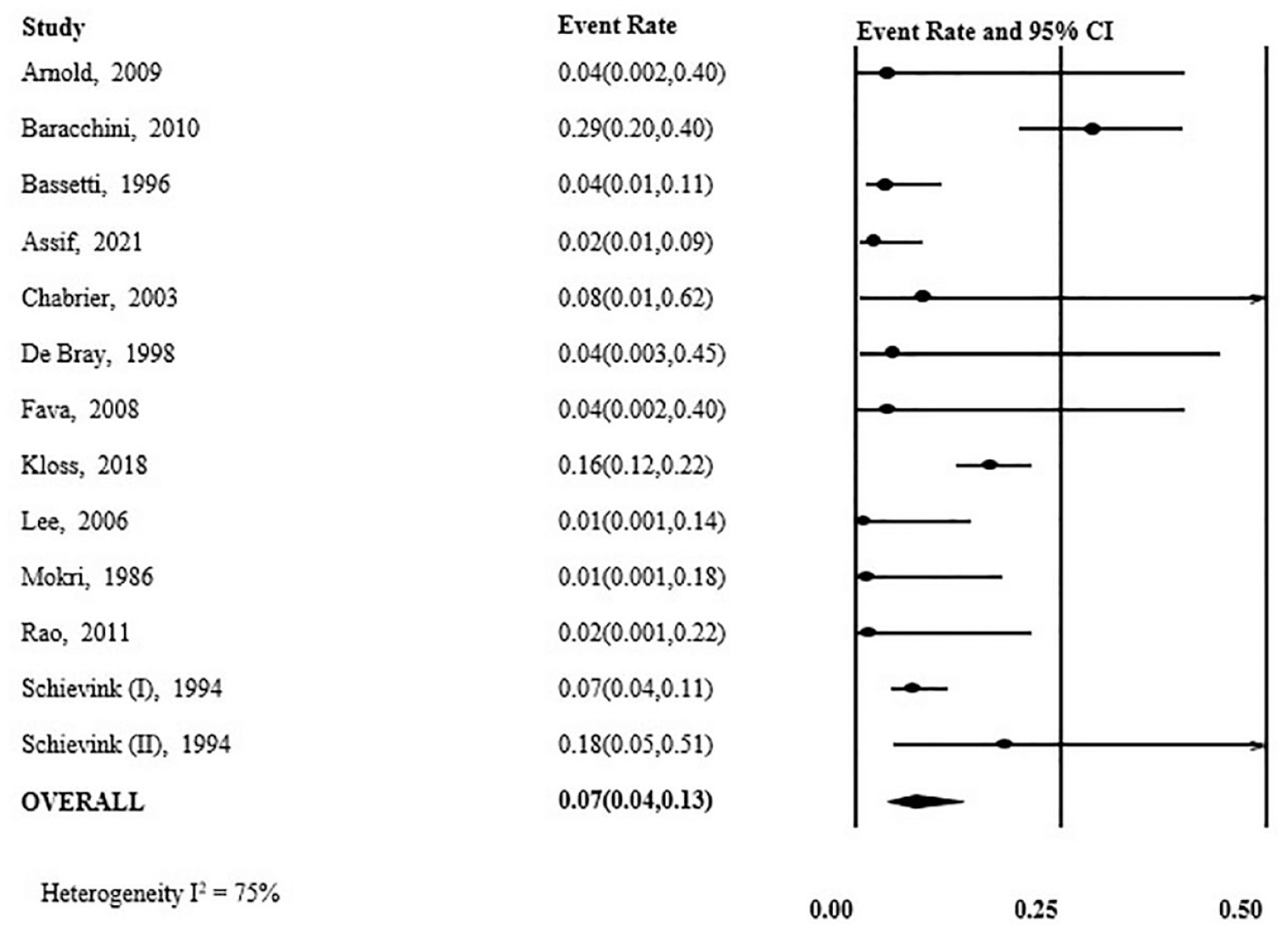
Incidence rates for secondary outcome of recurrent cervical artery dissection at 1 year for each study with sufficient follow-up duration, and overall, presented with their confidence intervals and measure of heterogeneity.
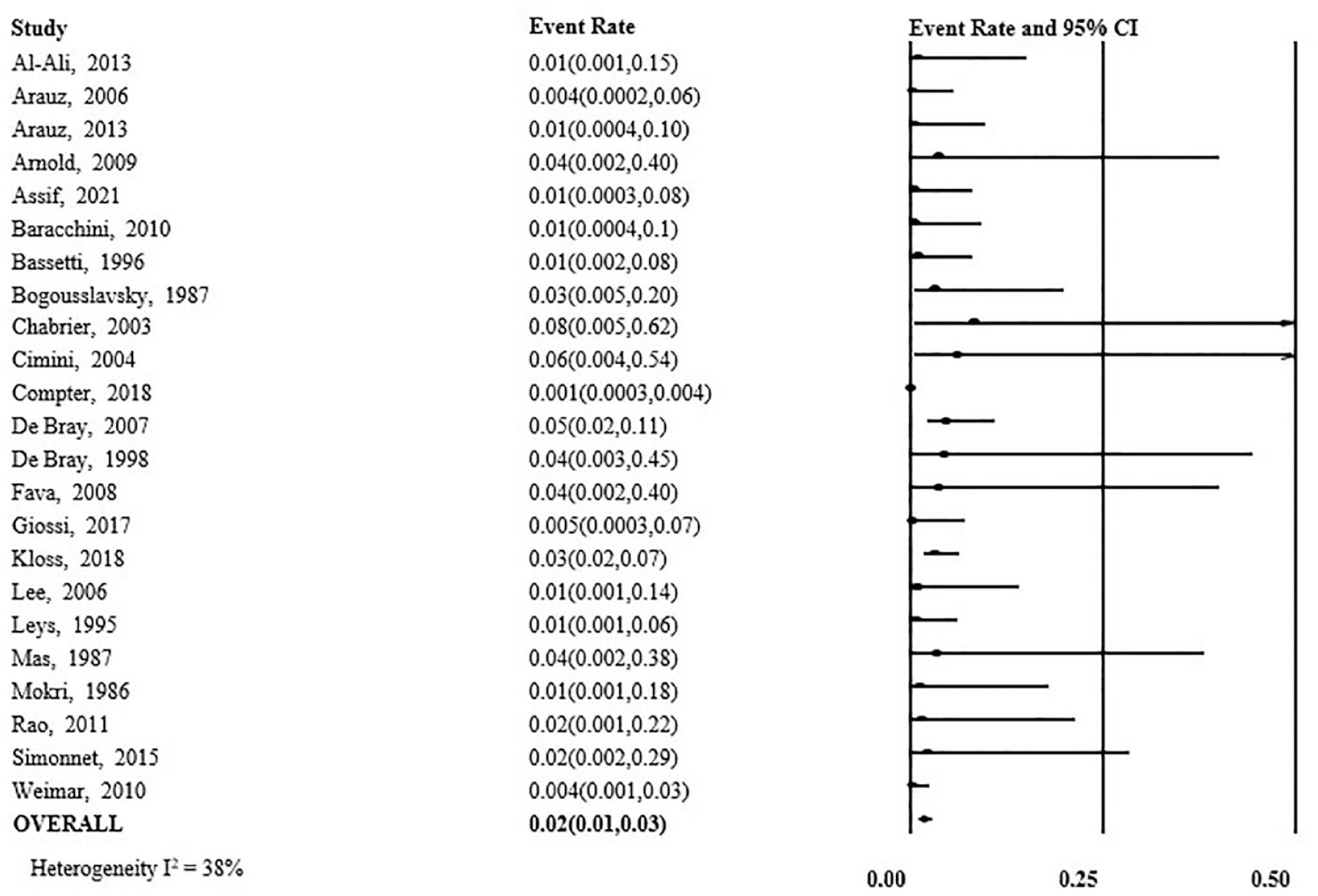
Incidence of recurrent cervical artery dissection symptomatic of ischemia for each study in which this outcome was reported, and overall, presented with their confidence intervals and measure of heterogeneity.
In the subgroup of studies that included routine surveillance imaging, recurrence occurred in 5% of patients (95% CI = 3–9%), and in studies without routine imaging, recurrence occurred in 3% of patients (95% CI = 2–7%) (Figure 5). There were insufficient data to be able to collect or analyze recurrence rates in any of the pre-specified clinical subgroups. In individual studies, the following variables were associated with statistically significantly higher recurrence rates: fibromuscular dysplasia, arterial tortuosity, younger age, longer follow-up period, and family history of arterial dissection.
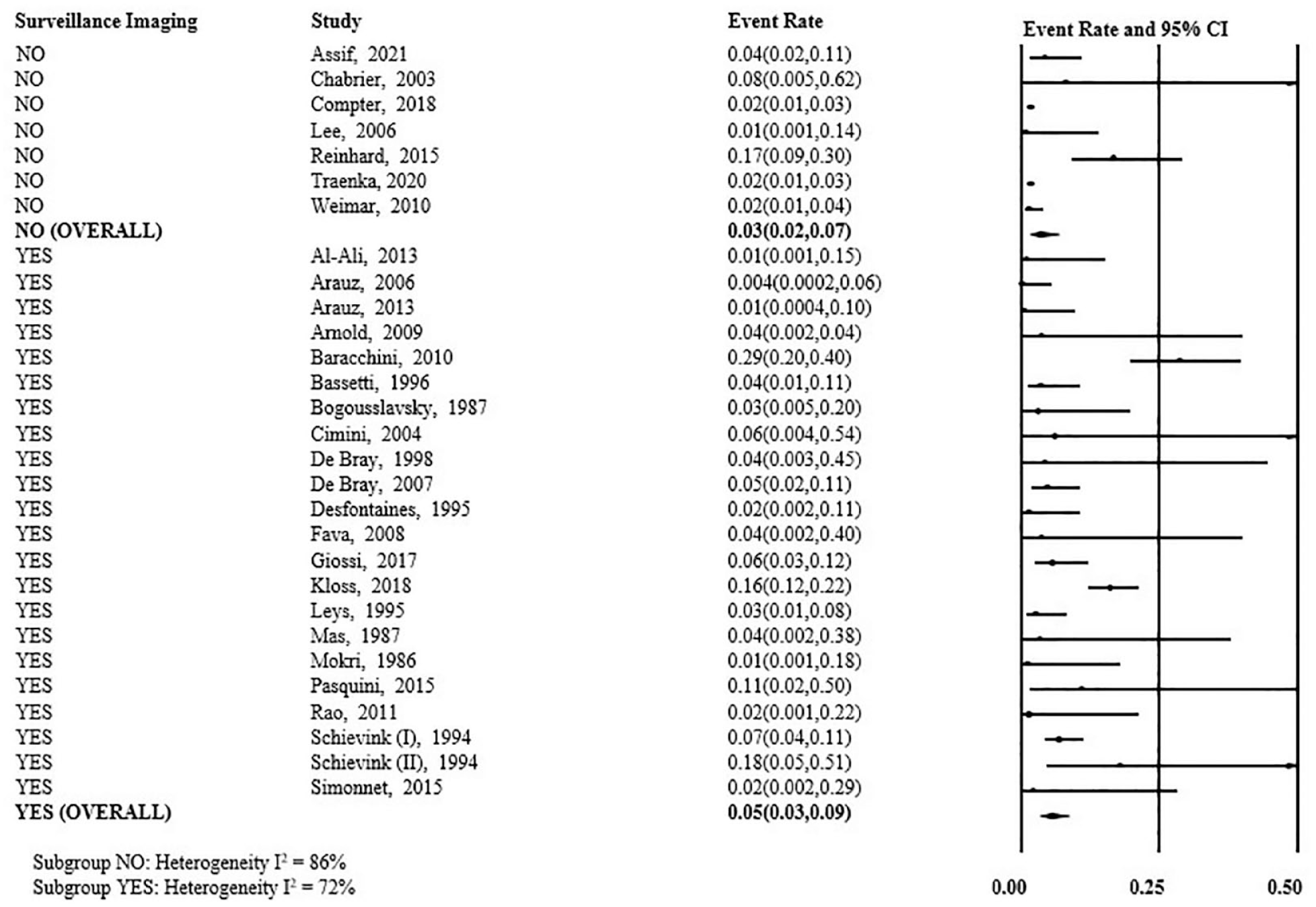
Subgroup analysis of the primary outcome of overall incidence of recurrent cervical artery dissection in studies that did and did not include routine surveillance imaging as part of their follow-up protocol, presented with their confidence intervals and measures of heterogeneity.
Low risk of bias was identified in 22 of the 29 included studies (75.9%). Within this subgroup, recurrence occurred in 5% of patients (95% CI = 3–8%) (Figure 6). A sensitivity analysis was also performed by excluding the studies that most significantly influenced the I 2 . In the remaining studies, recurrence occurred in 3% of patients (95% CI = 2–4%) (Figure S1).
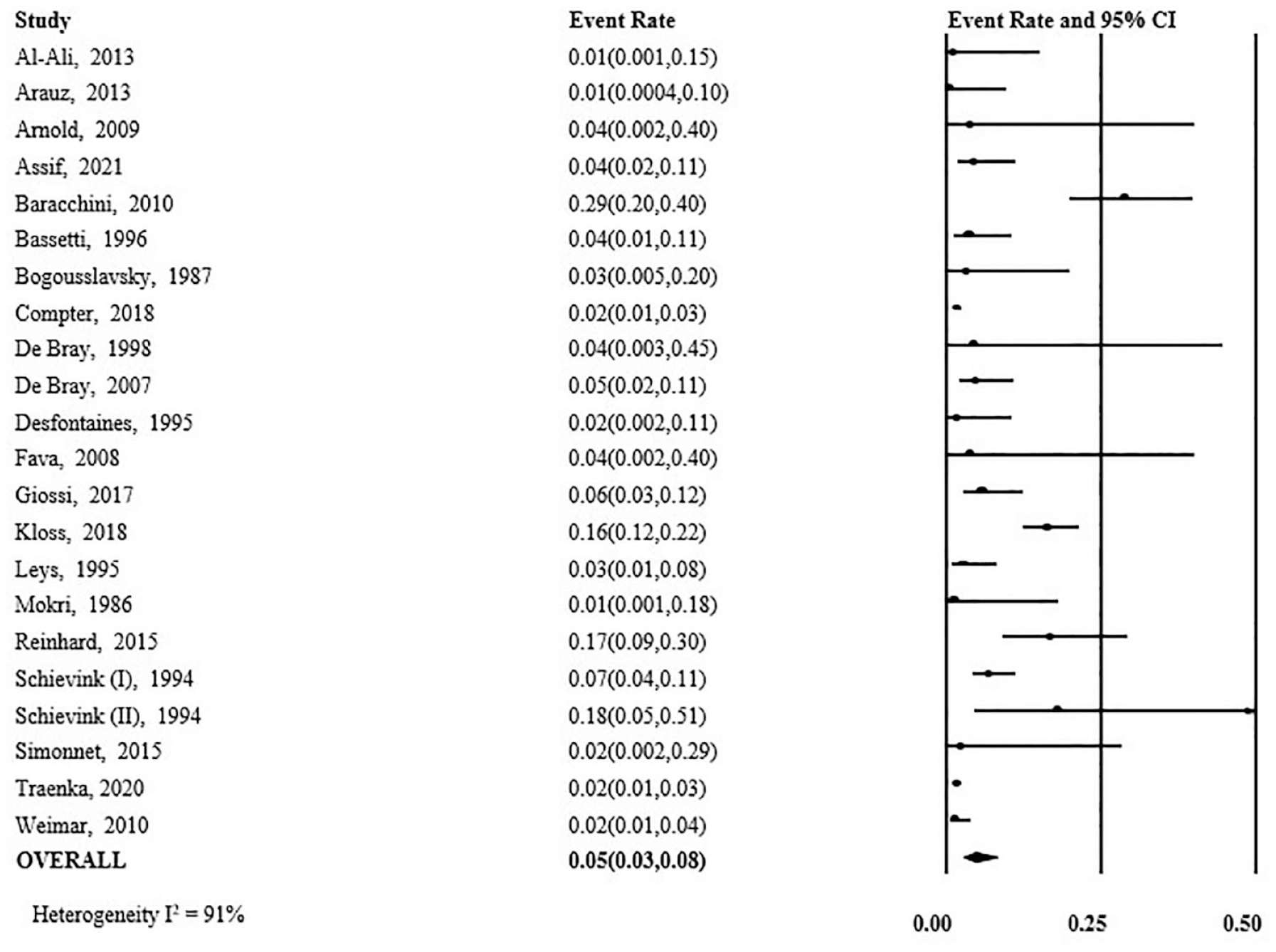
Primary outcome of overall incidence of recurrent cervical artery dissection for the subgroup of high-quality studies only, presented with their confidence intervals and measure of heterogeneity.
Discussion
This meta-analysis provides our best estimate of the incidence of recurrent CAD. Recurrence appears to be infrequent, and stroke related to recurrent dissection is even rarer. This distinction suggests that many recurrent dissections may be associated with local symptoms only or may be entirely asymptomatic. It is interesting to note that the study reporting the highest recurrence rate by far, at 29%, 12 also employed the most rigorous follow-up imaging protocol, including initial daily ultrasounds for all patients, followed by monthly imaging for 6 months, then every 6 months thereafter. The frequency of follow-up imaging for each study is available in the extracted data. It should be noted for the interest of the reader that the Cervical Artery Dissection in Stroke Study (CADISS) did not include recurrent dissection as an outcome and thus was not eligible for inclusion.
This study has several limitations. The duration of minimum follow-up for most studies reduced the available data on long-term recurrence rates. Variable reporting of patient characteristics also precluded clinical subgroup analysis which limits the ability to provide patient-specific estimates of risk. We identified high statistical heterogeneity in most of the analyses, which was not clearly explained by the subgroup analyses above. Despite the statistical heterogeneity, the studies included were uniform enough in their clinical and methodological characteristics to justify pooling for meta-analysis.
Conclusion
Ultimately, the low rates of recurrent dissection should be of great interest to patients and clinicians, particularly as this patient population tends to be young and active, making conclusions on future risk particularly vital. While these studies captured a broad population and are highly generalizable, there remains an opportunity to collect further patient-level data to inform more tailored estimates of risk. Further well-designed studies examining CAD recurrence, including analysis of recurrence rates in different subgroups, would be of great clinical utility. Ultimately, discussions regarding return to activity after CAD will need to remain individualized, factoring in patient factors, values, and preferences. However, we do hope that the findings of this study will allow for a more empirically sound foundation upon which to base decision-making, and we feel that citing a baseline recurrence risk of 4% for all-comers is tangible for patients and is a helpful starting point in framing these discussions.
Supplemental Material
sj-jpg-1-wso-10.1177_17474930231201434 – Supplemental material for Recurrence of cervical artery dissection: A systematic review and meta-analysis
Supplemental material, sj-jpg-1-wso-10.1177_17474930231201434 for Recurrence of cervical artery dissection: A systematic review and meta-analysis by Elizabeth Lounsbury, Naomi Niznick, Ranjeeta Mallick, Brian Dewar, Alexandra Davis, Dean A Fergusson, Dar Dowlatshahi and Michel Shamy in International Journal of Stroke
Supplemental Material
sj-xlsx-2-wso-10.1177_17474930231201434 – Supplemental material for Recurrence of cervical artery dissection: A systematic review and meta-analysis
Supplemental material, sj-xlsx-2-wso-10.1177_17474930231201434 for Recurrence of cervical artery dissection: A systematic review and meta-analysis by Elizabeth Lounsbury, Naomi Niznick, Ranjeeta Mallick, Brian Dewar, Alexandra Davis, Dean A Fergusson, Dar Dowlatshahi and Michel Shamy in International Journal of Stroke
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.