
Abstract
Background:
India accounts for 13.3% of global disability-adjusted life years (DALYs) lost due to stroke with a relatively younger age of onset compared to the Western population. In India’s public healthcare system, many stroke patients seek care at tertiary-level government-funded medical colleges where an optimal level of stroke care is expected. However, there are no studies from India that have assessed the quality of stroke care, including infrastructure, imaging facilities, or the availability of stroke care units in medical colleges.
Aim:
This study aimed to understand the existing protocols and management of acute stroke care across 22 medical colleges in India, as part of the baseline assessment of the ongoing IMPETUS stroke study.
Methods:
A semi-structured quantitative pre-tested questionnaire, developed based on review of literature and expert discussion, was mailed to 22 participating sites of the IMPETUS stroke study. The questionnaire assessed comprehensively all components of stroke care, including human resources, emergency system, in-hospital care, and secondary prevention. A descriptive analysis of their status was undertaken.
Results:
In the emergency services, limited stroke helpline numbers, 3/22 (14%); prenotification system, 5/22 (23%); and stroke-trained physicians were available, 6/22 (27%). One-third of hospitals did not have on-call neurologists. Although non-contrast computed tomography (NCCT) was always available, 39% of hospitals were not doing computed tomography (CT) angiography and 13/22 (59%) were not doing magnetic resonance imaging (MRI) after routine working hours. Intravenous thrombolysis was being done in 20/22 (91%) hospitals, but 36% of hospitals did not provide it free of cost. Endovascular therapy was available only in 6/22 (27%) hospitals. The study highlighted the scarcity of multidisciplinary stroke teams, 8/22 (36%), and stroke units, 7/22 (32%). Lifesaving surgeries like hematoma evacuation, 11/22 (50%), and decompressive craniectomy, 9/22 (41%), were performed in limited numbers. The availability of occupational therapists, speech therapists, and cognitive rehabilitation was minimal.
Conclusion:
This study highlighted the current status of acute stroke management in publicly funded tertiary care hospitals. Lack of prenotification, limited number of stroke-trained physicians and neurosurgeons, relatively lesser provision of free thrombolytic agents, limited stroke units, and lack of rehabilitation services are areas needing urgent attention by policymakers and creation of sustainable education models for uniform stroke care by medical professionals across the country.
Introduction
Worldwide, non-communicable diseases (NCDs) contribute to 70% of deaths. 1 Stroke is the second most common cause of death and disability with a much higher burden in developing countries.2,3 India accounts for 13.3% of global disability-adjusted life years (DALYs) lost due to stroke with a relatively younger age of onset compared to the Western population. 4 Studies have observed that timely management of stroke in the emergency is associated with lower hospital mortality and improved independent ambulatory status.5,6 India has introduced its own national stroke program and guidelines. These aim to change behavior with lifestyle modifications, prevention of stroke, and provision of optimized treatment at all levels of the healthcare. 7 However, barriers exist in implementing optimized stroke care at community level. Previous studies assessing infrastructure and barriers were either from a single medical center or a geographical area. Studies including multiple cities and states in India are lacking. 8
In India’s public healthcare system, stroke patients often seek care at tertiary-level medical colleges where an optimal level of stroke care is expected. 9 Assessing their infrastructure, resources, and adherence to protocols is crucial to improve stroke care and outcomes. However, there are no studies from India that have assessed the quality of stroke care, including infrastructure, imaging facilities, or the availability of stroke care units in medical colleges. We have no specific knowledge about the status of manpower, training gap, indoor stroke care, the extent to which guidelines are adhered, challenges in implementing such guidelines, or even the cascade leading to discharge and secondary prevention in medical colleges in India.
We designed the IMPETUS stroke study (Implementation of an evaluation and treatment package for uniform stroke care and outcomes in the medical colleges in India: An Implementation Research Study; https://impetus.icmr.org.in/) with the aim of improving stroke care from the time of recognition in the emergency, in patient management, secondary stroke prevention, and appropriate discharge planning. 10 As part of IMPETUS stroke study, we aimed to assess the current situation of acute stroke care in select 22 medical colleges across India, in terms of the infrastructural assessment and limitations. The objective of this study was to undertake a situational analysis of the current status of acute stroke care in select medical colleges in India.
Methodology
Study design
The following study was undertaken as part of the baseline assessment of the ongoing IMPETUS stroke study. 10 IMPETUS stroke is a multicentric, prospective, multiphase, mixed-methods, quasi-experimental implementation study, comprising three phases. The study was initiated in October 2021. Phase 1 is the pre-implementation phase, wherein a baseline survey assessment of the existing components of stroke care was performed. This study reports the existing infrastructure for stroke care among the study sites during the pre-intervention phase. During phase I, baseline data are collected on patients in a predefined structured case record form and focused group discussions were held to understand barriers and facilitators of stroke care. This is followed by the implementation phase where main intervention is periodic education and training of the staff, meetings with the site administrators, and education and training of caregivers. Following this implementation phase, data collection is continued to observe the level of implementation and sustainability. The outcomes of implementation shall be assessed on defined indicators of stroke care, mortality, and disability. 10
Study setting
We conducted the study in the collaborating 22 medical colleges and hospitals stretched across 14 different cities from 12 different states of India. All medical colleges are tertiary medical centers situated either in district headquarters or the state capitals.
Study participants
We sought responses to these questions from the neurology or medicine faculty of all study sites involved in the IMPETUS stroke study.
Study tool
The authors (R.B. and P.H.) formulated 85 questions after multiple rounds of discussions which seemed important and reasonable for the stroke care pathways in a hospital (supplemental material). We also reviewed the World Stroke Organization (WSO) action plan for optimizing stroke outcomes, the recommendation of the American Stroke Association (ASA) for the establishment of stroke systems of care and European expert survey to assess the main components of stroke unit care.11–13
Study variables and mode of question administration
Questions were sent through email-based electronic forms to neurology and medicine consultants from 22 different medical colleges via email. Questions were directed toward human resources and infrastructure involved in stroke care, emergency setting and in-hospital care, secondary prevention strategies, and discharge planning of stroke patients. Ethical issues: Study has been given ethical approval by the Institute Ethics Committee of the All India Institute of Medical Sciences, New Delhi, India (IEC-92/06.3.2020). The study adheres to the STROBE observational study guidelines. 14
Results
All sites completed the questionnaire. The responses were provided by 19 neurologists and 3 internal medicine specialists. We observed a lack of stroke helpline numbers available for community (3/22;14%) among study sites. Although ambulance services are present in 18/22 (82%) hospitals, stroke prenotification systems were available in only 5/22 (23%) hospitals (Table 1). Non-contrast computed tomography (NCCT) facilities were available in all hospitals. However, other imaging modalities were available at a limited time of the day. Although on-call neurologists are available in 15/22 (68%) hospitals, only 6/22 (27%) hospitals have stroke-trained physicians available in the emergency (Table 1). Initial evaluation with blood sugar, blood pressure, and level of consciousness assessment is being done in almost all hospitals. However, routine National Institute of Health Stroke Scale (NIHSS) assessment is being done in only 13/22 (59%) during emergency evaluation (Table 1).
Stroke recognition and emergency area infrastructure.
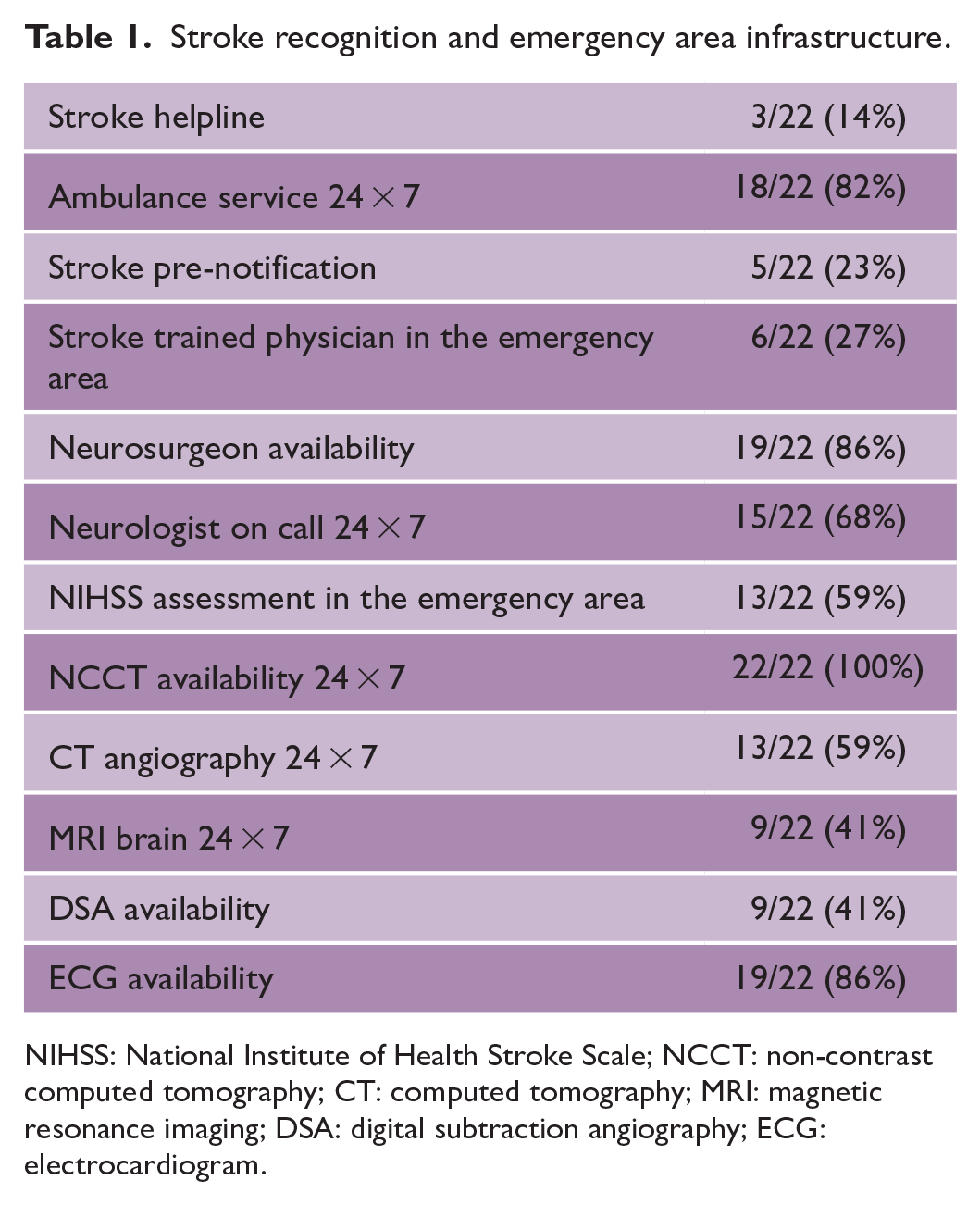
NIHSS: National Institute of Health Stroke Scale; NCCT: non-contrast computed tomography; CT: computed tomography; MRI: magnetic resonance imaging; DSA: digital subtraction angiography; ECG: electrocardiogram.
Intravenous thrombolysis (IVT) is performed in 20/22 (91%) hospitals among which 17/22 (77%) are providing it free of cost. Tissue plasminogen activator (TPA) is the most common agent used for IVT (Table 2). Endovascular therapy (EVT) services are available in 6/22 (27%) of the hospitals but only two hospitals are providing it free (Table 2). Lifesaving neurosurgical processes like decompressive craniectomy, 13/22 (59%), and hematoma evacuation, 11/22 (50%), are being performed in limited hospitals (Table 2). All hospitals have availability of CT angiography, carotid Doppler, and two-dimensional (2D)-echo (Table 3). Although Holter monitoring was available in all centers, its use for ischemic stroke evaluation was only done in 2/22 (9.1%). Routine swallow assessment is being done around three-fourths of the hospitals. In 19/22 (86%) hospitals, blood pressure monitoring is done at least twice daily (Table 4). Pneumatic compression and/or heparin is routinely used in 18/22 (82%) hospitals for deep vein thrombosis (DVT) prevention (Table 4). At the time of discharge, all hospitals are able to do risk profiling for diabetes mellitus, hypertension, heart disease, and smoking (Table 4). However, etiology identification (ischemic stroke subclassification) at the time of discharge is mentioned regularly in only 13/22 (59%) (Table 4).
Hyperacute stroke care.
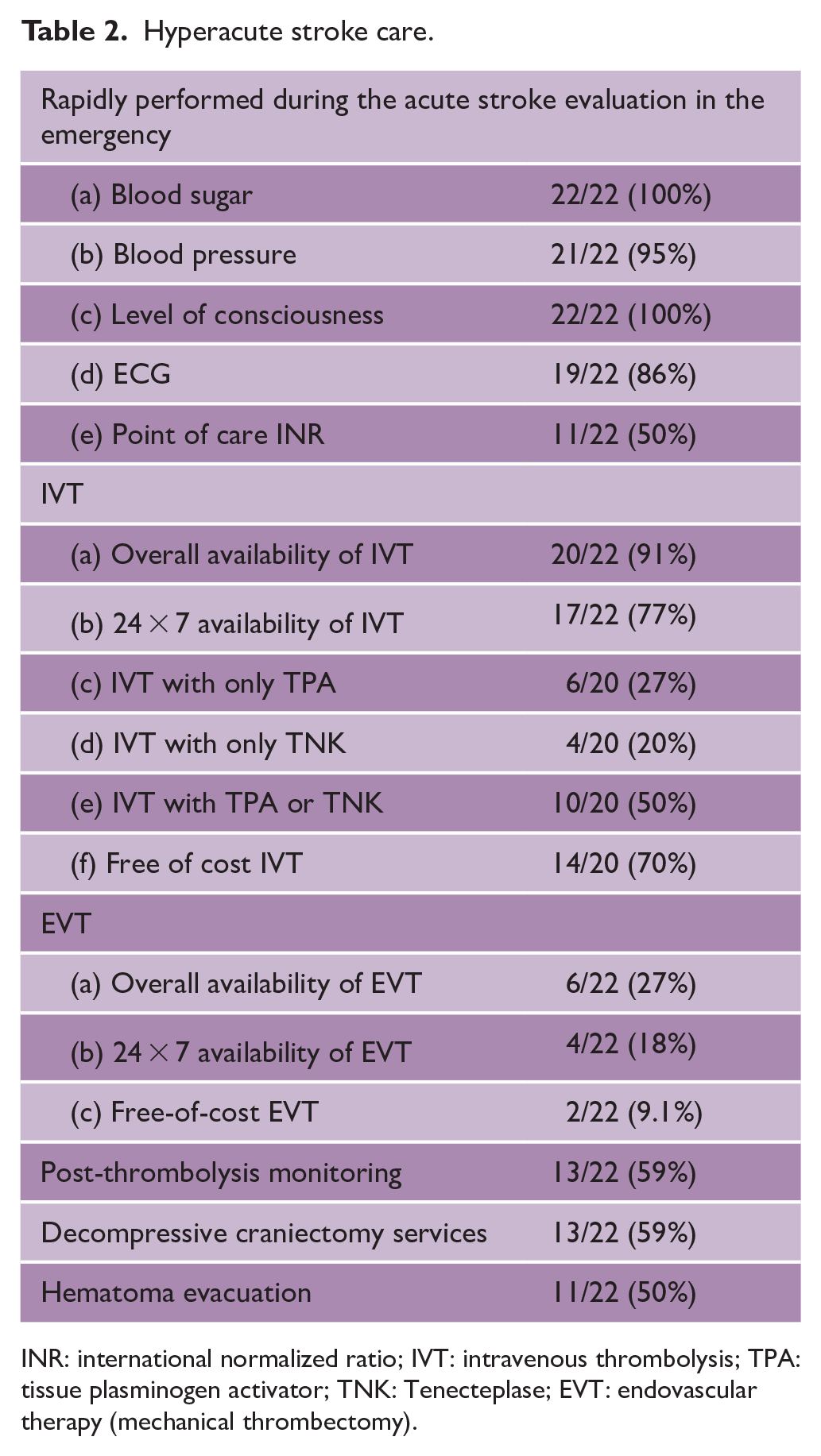
INR: international normalized ratio; IVT: intravenous thrombolysis; TPA: tissue plasminogen activator; TNK: Tenecteplase; EVT: endovascular therapy (mechanical thrombectomy).
Inpatient stroke care infrastructure.
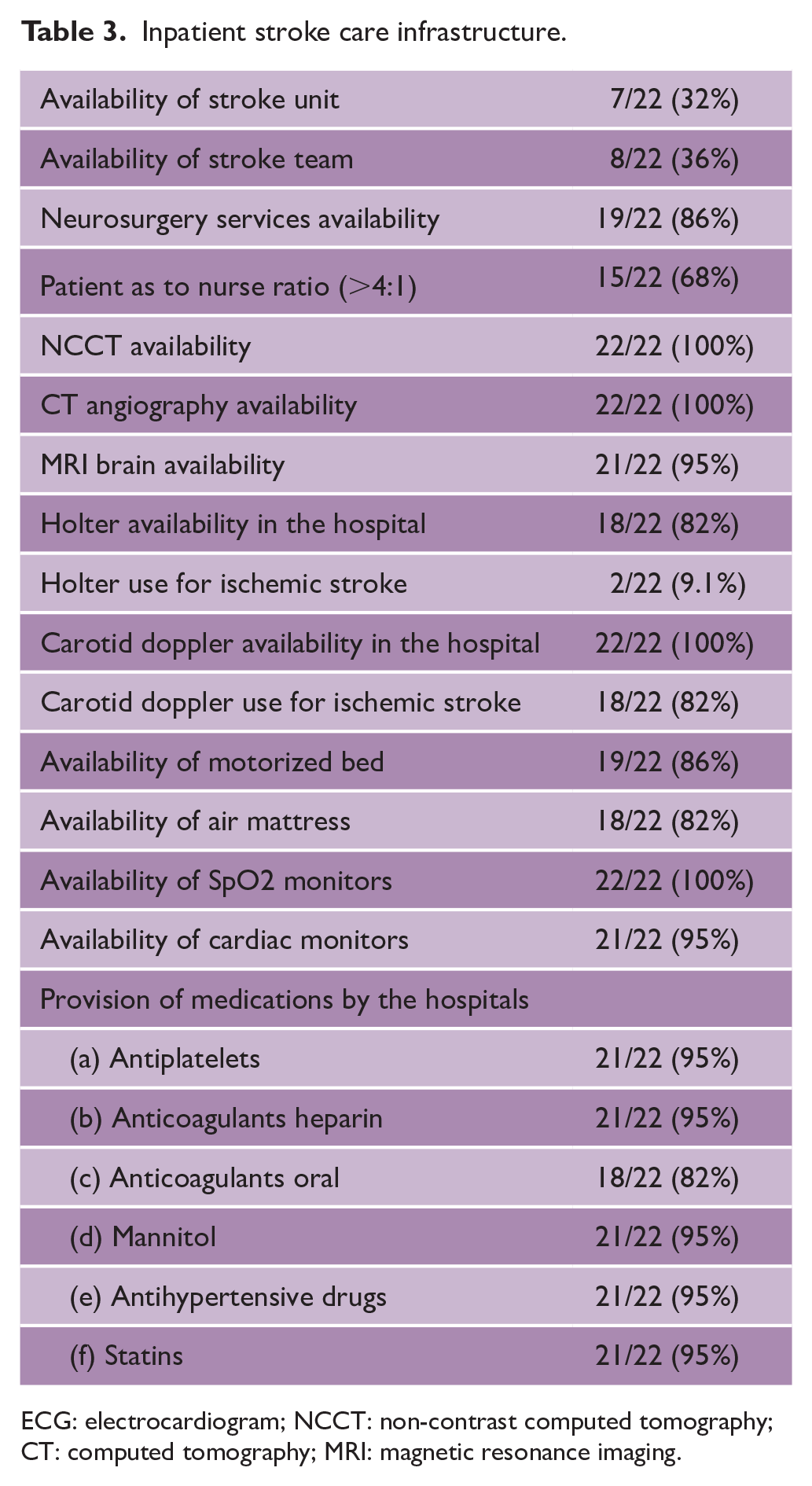
ECG: electrocardiogram; NCCT: non-contrast computed tomography; CT: computed tomography; MRI: magnetic resonance imaging.
Inpatient stroke care and secondary stroke prevention.
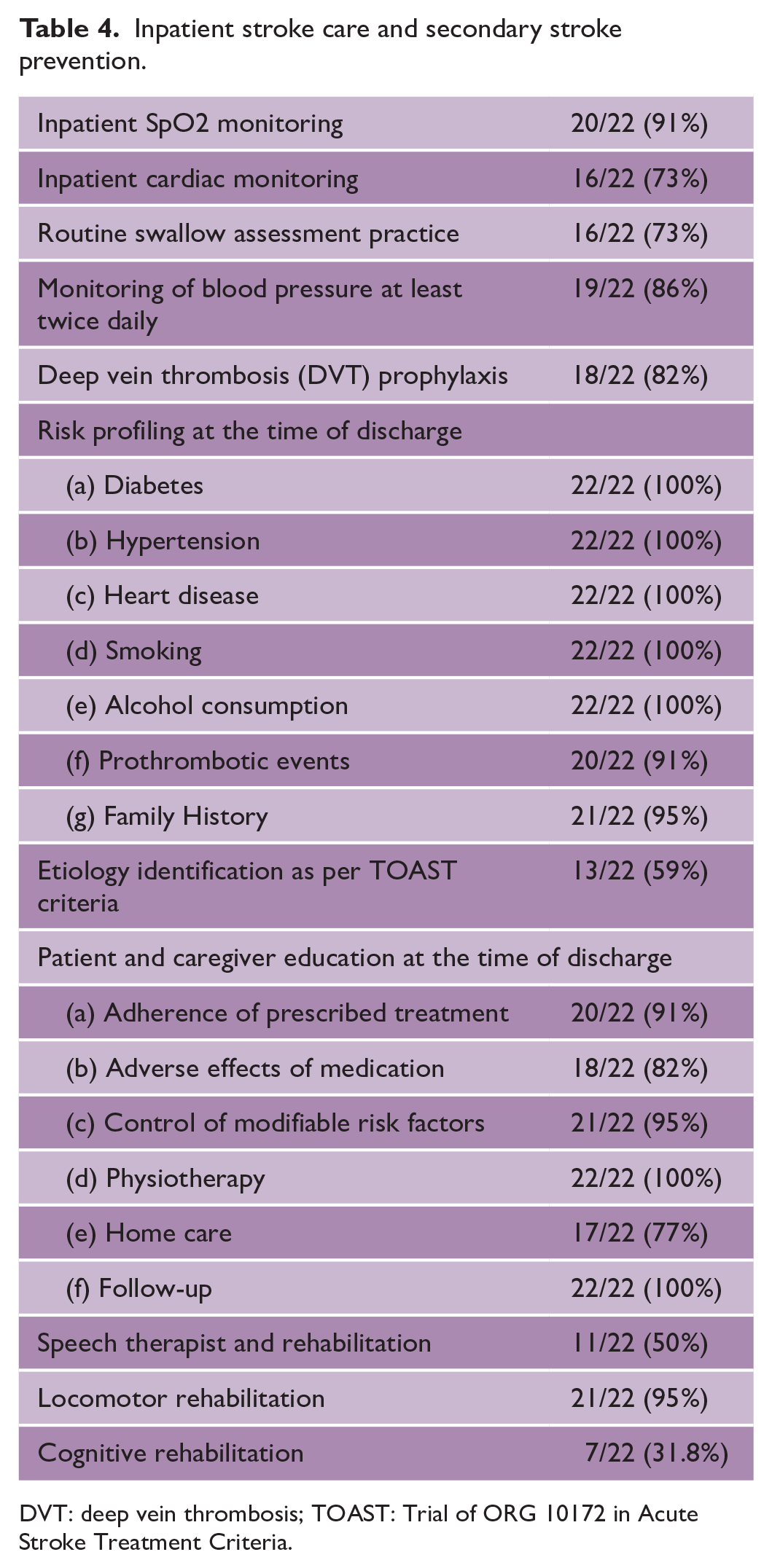
DVT: deep vein thrombosis; TOAST: Trial of ORG 10172 in Acute Stroke Treatment Criteria.
Discussion
Public hospitals face challenges in providing comprehensive care to acute stroke patients. This includes pre-hospital, intra-hospital, and post-hospital services such as evaluation, prevention, rehabilitation, and home care by caregivers. 9 This study assessed stroke management in 22 government medical colleges in India. We evaluated infrastructure, barriers, and facilitators. Previous studies identified multiple barriers in low-income countries, including limited resources, transportation, lack of experts, and rehabilitation services. 15
Public awareness of stroke recognition is low in lower middle-income countries (LMICs), including India. 16 Lack of structured prenotification systems and trained ambulance personnel still worsen the problem. 9 Ambulance services are available in 83% of hospitals, but their utilization by the public is limited not only in India but also in Ghana or Nigeria.16–18 Ambulance personnel may have inadequate training to recognize stroke symptoms. Use of alternative transportation methods may be more efficient in busy LMIC cities.
Scarce availability of stroke-trained physicians and neurologists is evident in India. Internists in the emergency area predominantly provide acute stroke care services due to the lack of neurologists. 17 Similar observations reported from a study from Ghana. 19 Structured training programs for stroke during residency are crucial for capacity building. Education of emergency staff can compensate for limited availability of stroke-trained physicians, improve stroke care, and enhance the availability of stroke-ready hospitals. Following stroke education of emergency resident doctors and nursing officers, a study demonstrated significant and sustained improvements in thrombolysis rates and time metrics after stroke education for emergency resident doctors and nursing officers. 18
Timely and accessible brain imaging services are critical for diagnosis and management of stroke. Availability, accessibility, functionality, reporting standards of CT or MRI may be limited and extremely variable among LMIC. A previous systematic review observed use of CT scans for diagnosis of stroke during admission in 90% patients and limited use of MRI, 20 while it is abysmally low at 13–26% in Africa. 21 In our study, all hospitals had NCCT imaging facilities available all day. However, door-to-CT time is crucial for assessing process quality. A tertiary institute study found that only 38.6% of patients achieved a door-to-CT time of less than 20 min. 22
Limited NIHSS assessment could be due to lack of awareness, training, unavailability of stroke-trained physicians, or skewed doctor-patient ratios in our emergency areas. Constant efforts to educate and enforce certification may help. IVT, an effective acute stroke intervention, has lower rates (3% and 19%, respectively) in low-income and LMICs compared to high-income countries (HICs) (50%), as per a meta-analysis.22,23 It has constantly increased in India, though is still underutilized. In a prospective study from southern part of India, financial constraints (76.7%) were one of the major barriers causing a delay in decision-making of thrombolysis; around 27.2% of patients with ischemic stroke reaching hospitals within 4.5 h of onset were below the poverty line. 18 The provision of cheaper thrombolytic agents like biosimilar Tenecteplase can overcome this barrier. We observed that 14/22 (63.6%) hospitals are using Tenecteplase.
EVT is provided to very few patients despite the fact that it can be used in selective patients up to 24 h from the onset of stroke. The EVT availability is limited across LMIC.15,19,22,23 Only 3.4% of patients received mechanical thrombectomy in the Indo-US stroke Collaborative National Stroke Registry. 4 Across the country, approximately 100 centers have the facility for EVT and are gradually increasing.9,24 These are limited to large urban cities in either tertiary referral public institutes or privately funded corporate medical centers. In a recent survey by the mission thrombectomy (MT) 2020 plus global network among 75 countries, global MT use was poor and LMIC had 88% lower mechanical thrombectomy access when compared to HICs. 25 Infrastructural needs, limited trained manpower, and significantly high cost will limit its implementation across LMIC. Low-cost indigenously manufactured devices, reducing device cost, and integration of hub and spoke models could help overcome this limitation. 24 Providing training to radiologists, neurologists, and neurosurgeons will help increase the available manpower. 26 The National Board of Examination (NBE)-accredited fellowship program in India is one step in this direction (https://natboard.edu.in/fellowship.php; accessed 17 May 2023). We found that 40% of hospitals cannot routinely perform lifesaving surgeries like hematoma evacuation and decompressive craniectomy. Timely surgical intervention can reduce mortality in the case of intracerebral hemorrhage (ICH) and malignant middle cerebral artery (MCA) infarction. 27 In India, one neurosurgeon is available per one million population. This unmatched need results in limited access to surgical treatment with spontaneous intracerebral hemorrhage (SICH). 28 No well-described data are available for such interventions from LMICs in previously published literature.19–21
A multidisciplinary stroke team and admission to stroke units improve outcomes. 29 Availability of stroke units is limited in LMIC with patients generally admitted in general medical or neurology wards.16,19,21 Stroke unit admissions were reported in 25% of patients admitted in Thailand, 12% in Brazil, and 6% in Argentina. 20 Presently, in India, stroke units are limited and available predominantly in super specialty tertiary care academic hospitals, private sector, and metropolitan cities. 9
Stroke subtyping is crucial for treatment and secondary prevention due to variations in recurrence and mortality rates. In South Asia (15.1%), a significantly lower percentage of stroke patients undergo vascular imaging compared to Western countries (84.3%). 30 Limited availability of CT angiography services during working hours hampers timely diagnosis and subtyping. Stroke of undetermined etiology, including cardioembolic that requires optimum evaluation, was the second most common cause (27.3%) of ischemic stroke in a registry study. 31 In our study, only 59% of hospitals were using the TOAST (Trial of ORG 10172 in Acute Stroke Treatment Criteria) etiology classification at the time of discharge.
Provision of optimal inpatient rehabilitation improves the quality of life and motor function of stroke patients. 32 Availability of rehabilitation expertise, although assessed in our study, could be influenced by additional factors. LMICs provide post-discharge rehabilitation services to a smaller proportion (31%) of patients compared to HICs (92%), leading to higher rates of functional disability. 33 A significant number of years lost due to stroke in rural India occur in the age group of 30–70 years. 34 There is a communication gap in post-discharge rehabilitation needs, with caregivers expressing a need for more information. 34 LMICs have a shortage of skilled rehabilitation practitioners (<10 per 1 million population), mainly concentrated in tertiary care centers, necessitating innovative and accessible stroke rehabilitation services, including tele-rehabilitation. 35 The IMPETUS project aims to enhance rehabilitation services and promote tele-rehabilitation for patients and caregivers in hospitals and homes. Video modules and low-cost assistive devices improve outcomes.
Strengthening caregiver knowledge and empowering them to assist during inpatient care is extremely relevant to LMICs due to shortage of nursing manpower. 36 This is an untapped strategy that leads to poor knowledge transfer that may affect patient outcomes, especially once discharged to home.34,35 One of the important components of the IMPETUS project is to enhance caregiver knowledge using training strategies for patient care.
Potential solutions to these limitations are possible and various models can be explored to improve stroke services in LMIC.16,37 The WSO Global Stroke Services Guidelines and Action Plan framework proposes three tiers of stroke services (minimal, essential, and advanced), depending on the availability of multidisciplinary expertise, diagnostic infrastructure, and capacity for acute reperfusion therapy and should guide improvement of services in small steps that can yield significant results as was observed from a minimal stroke unit set up in Conakry, Guinea, Africa. 38 The Brazilian Stroke Project initiative and National Stroke Policy Act is an excellent example of implementing stroke services, including pre-hospital notification, creation of stroke centers, reimbursement of thrombolysis, rehabilitation. 39 The line of stroke concept ensures each city or region to comprehensively provide stroke services at all levels.
A simple smartphone-based tele-stroke model using was a successful attempt to facilitate acute stroke care in the state of Himachal Pradesh, India. 40 In the ongoing National NCD Programme (https://ncd.nhp.gov.in/) and Ayushman Bharat Health and Wellness Centres (https://ab-hwc.nhp.gov.in/) of India, screening and treatment is the strategy to reduce disease burden. The Ayushman Bharat Pradhan Mantri Jan Arogya Yojana (PMJAY) is a national public health insurance scheme that supports treatment for low income populations in India. Implementing NPCDCS (National Programme for Prevention and Control of Cancer, Diabetes, Cardiovascular Diseases & Stroke) program and standardizing and homogenization of stroke care services will be essential for optimal care.
Education and training for medical, nursing, and rehabilitation graduates improve stroke patient management. Including checklists and algorithms for stroke care would encourage uniformity of care. Capacity building should include residents, nurses, and step-down centers, accompanied with engagements with administrators for sustenance.
Strengths and limitations
The study provides a brief insight into the current status of stroke care services that needs focus for improvement. India is a large country with infrastructural, social, and economic diversity like other LMICs, including Brazil and Africa, and should not lead to a speculation that these data represent the entire country. Since this study includes only medical colleges in urban settings, area and economic bias are likely. Since the respondents were only medical leads, information bias is possible. There has been significant progress in training and improvement in stroke services in the country. Interviewing multiple physicians or doing focused group discussions involving physicians, paramedics, and stakeholders of medical services will provide more detailed information on current stroke care services.
Conclusion
This study could highlight the current functioning of publicly funded hospitals with acute stroke management and secondary stroke prevention. Lack of prenotification, a limited number of stroke-trained physicians and neurosurgeons, relatively lesser provision of free thrombolytic agents, a limited number of stroke units, and lack of rehabilitation services are areas where we need urgent attention by policymakers and creation of sustainable education models for uniform stroke care by neurologists across the country.
Supplemental Material
sj-pdf-1-wso-10.1177_17474930231189395 – Supplemental material for IMPETUS Stroke: Assessment of hospital infrastructure and workflow for implementation of uniform stroke care pathway in India
Supplemental material, sj-pdf-1-wso-10.1177_17474930231189395 for IMPETUS Stroke: Assessment of hospital infrastructure and workflow for implementation of uniform stroke care pathway in India by Manish Salunkhe, Partha Haldar, Rohit Bhatia, Deepshikha Prasad, Shweta Gupta, M V Padma Srivastava, Sanjeev Bhoi, Menka Jha, Priyanka Samal, Samhita Panda, Sucharita Anand, Niraj Kumar, Ashutosh Tiwari, S Gopi, Garuda Butchi Raju, Jyoti Garg, M P S Chawla, Biman Kanti Ray, Amit Bhardwaj, Alok Verma, Nikhil Dongre, Gurpreet Chhina, Raminder Sibia, Rupinderjeet Kaur, Paresh Zanzmera, Thomas Iype, Sulena, Ravinder Garg, Ashok Kumar, Abhay Ranjan, Vijay Sardana, Dilip Maheshwari, Bharat Bhushan, Alvee Saluja, Pramod Darole, Kiran Bala, Surekha Dabla, Inder Puri, Shalin Shah, Gajender Singh Ranga, Smita Nath, Shishir Chandan and Rupali Malik in International Journal of Stroke
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The IMPETUS study is supported by research grant from Department of Health Research (DHR), Indian Council of Medical Research (ICMR), New Delhi, India.
Data accessibility statement
The data are available on reasonable request, with the corresponding author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.