
Abstract
Background
Stroke is the fifth leading cause of death in young individuals globally. Data on the burden of sudden death by stroke are sparse in the young.
Aims
The aim of this study was to report mortality rates, cause of death, stroke subtype, and symptoms in children and young adults who suffered sudden death by stroke.
Methods
We conducted a retrospective, nationwide study including all deaths within Danish borders between 2000–2009 and 2007–2009 in persons aged 1–35 years and 36–49 years, respectively. Two physicians identified all sudden death cases through review of all death certificates. All available autopsy reports and records from hospitals and general practitioners were retrieved and a neurologist identified all sudden death by stroke cases.
Results
Of the 14,567 deaths in the 10-year period, there were 1,698 sudden death cases, of which 52 (3%) were sudden death by stroke. There was a male predominance (56%) and the median age was 33 years. The incidence of sudden death by stroke in individuals aged 1–49 years was 0.19 deaths per 100,000 person-years. Stroke was hemorrhagic in 94% of cases, whereof subarachnoid hemorrhage was the cause of death in 63% of cases. Seventeen (33%) cases contacted the healthcare system because of neurological symptoms, whereof one was suspected of having a stroke (6%).
Conclusions
Sudden death by stroke in children and young adults occurs primarily due to hemorrhagic stroke. We report a high frequency of neurological symptoms prior to sudden death by stroke. Increased awareness among healthcare professionals towards stroke symptoms in children and young adults may lead to earlier detection of stroke, and thereby potentially lowering the incidence of sudden death by stroke.
Introduction
Stroke is the fifth leading cause of death in people aged 15 to 59 years globally, and it is among the most common causes of sudden non-cardiac death in the young.1,2 Although rare, sudden unexpected death in the young is always a tragic and devastating event often occurring in apparently healthy individuals.3,4
Only a small amount of studies have investigated stroke subtypes in sudden death (SD) in the young, with a reported burden ranging from 4% to 14% of all SDs.5–12 However, the previous studies have been conducted on either selected patient populations, or studies only including autopsied patients.
We have previously conducted studies on both sudden cardiac death and sudden non-cardiac death in the young from 2000 to 2009 in an unselected and nationwide setting in Denmark.2,4,13,14 In our previous studies, the cause of death is cardiac in two-thirds of the SD cases and non-cardiac (e.g. stroke) in one-third of cases.
Aims
The aim of this nationwide study in an unselected population was to systematically investigate all sudden death by stroke (SD-S) cases by reviewing death certificates, autopsy reports, medical journals, and registry entries on previous known disease, and thereby describe mortality rates, cause of death, stroke subtype, and symptoms prior to death.
Methods
Study population
This is a nationwide retrospective study conducted using the availability of all death certificates to study SD cases. The methods used in this study have previously been described in detail.2,4,13–16 To get the phenotype well characterized, we used the registrations of all in- and outpatient activities in Danish Hospitals and emergency rooms together with access to all medical records and autopsy reports when performed. We included all deaths in individuals aged 1–35 years and 36–49 years in Denmark between 2000–2009 and 2007–2009, respectively.4,13 The study was approved by the Local Ethics Committee (H-KF-272484) and the Danish National Board of Health (7-505-29-58/6).
Danish registries
All Danish citizens are assigned a personal Civil Registration Number (CRN), which can be linked to national registries on an individual level. Using the CRN, we retrieved information on prior medical history from the National Patient Registry (NPR). Since 1978, the NPR has contained information on all inpatient (and outpatient contacts from 1995 onward) activity at Danish hospitals and emergency departments, using International Classification of Diseases diagnoses for each visit. 17
Death certificates
When a person dies within Danish borders a mandatory death certificate is completed by a medical doctor. If a Danish citizen is found dead or the death is sudden and unexpected, an external examination is mandatory by Danish law. The police and a medical doctor perform the examination. They are in possession of the deceased’s medical history (if any), the first responder (emergency medical service) records, the entire police record including witness statements, and the body of the deceased. This information is gathered and summarized on the death certificate in a section for supplementary information. This makes Danish death certificates highly suitable to identify sudden unexpected deaths 4 (see supplemental data). If the mode of death is not established from the external examination, a forensic autopsy is performed.
Conduct of autopsies
All forensic autopsies are performed by a forensic pathologist and follow a protocol that requires thorough examination of all organs to establish the most probable cause of death. Toxicology screens are performed on adolescent and adult cases of sudden unexplained death. In Denmark, there are three forensic departments that conduct around 1200 autopsies per year.
Data collection
Death certificates were retrieved digitally and independently reviewed by two physicians to identify deaths that were sudden and unexpected. In case of disagreement, a consensus was reached after re-evaluating the death certificate and by reviewing the patient’s medical history. All available medical records were retrieved from general practitioners and relevant hospitals departments. Thus, we had information on the time surrounding the death, previous medical history, and descriptions of treatment and management in emergency rooms and/or hospital departments.
When reviewing autopsy reports, the most probable cause of fatal injurious mechanism was established. In non-autopsied cases, the same criteria were used in cases presumed to be of cerebrovascular origin based on the circumstances relating to the death including all information from death certificates, medical records, and medical imaging. In cases of uncertainty, all information regarding the patient in question was reviewed by an experienced neurologist to identify and validate the primary SD-S-diagnosis responsible for the death of the patient.
Definitions
We defined SD as a sudden, natural, and unexpected death: in witnessed cases as an acute change in cardiovascular status with time to death being <1 hour and in unwitnessed cases as a person last seen alive and functioning normally <24 hours before being found dead.4,13
SD-S was defined as the natural unexpected death of neurological cause concluded after autopsy or medical imaging, with the same time spans as for SD. This definition builds upon the World Health Organization’s definition of stroke, which is described as “rapidly developed clinical signs of focal (or global) disturbance of cerebral function, lasting more than 24 hours or leading to death, with no apparent cause other than of vascular origin.” 18
All traumatic brain injuries were excluded as well as hemorrhagic strokes in malignancy patients. For the purpose of this study, strokes were divided into hemorrhagic or ischemic origin in agreement with the definitions in the “American Heart Association/American Stroke Association (AHA/ASA) Expert Consensus Document.” 19 Hemorrhagic strokes were furthermore subdivided into intracerebral and subarachnoid hemorrhages (ICH and SAH, respectively). ICH was subdivided on the basis of whether the hemorrhage originated from a rupture of an arteriovenous malformation or not. SAH was subdivided on whether the hemorrhage originated from a cerebral aneurysm rupture or not. 19
Neurological symptoms were defined as focal weakness or numbness in face, arm, or leg, slurred speech or language problems, confusion or decreased level of consciousness, acute headaches, and visual abnormalities. All symptoms were registered within 12 months before death.
Statistical analysis
All calculations were performed using SAS software package version 9.3 (SAS Institute, Cary NC). Differences in proportions between groups were accessed using a chi-square test or Fisher’s exact test where appropriate. A two-sided p-value of <0.05 was considered statistically significant. Incidence rates were calculated using the mean age group population as a denominator.
Results
In the 10-year study period, 14,567 deaths occurred within 27.1 million observed person-years. We identified 1,698 SD cases of which 61 persons died suddenly and unexpectedly due to stroke. Nine persons had a possible traumatic brain injury and were excluded according to the AHA/ASA definitions. 19
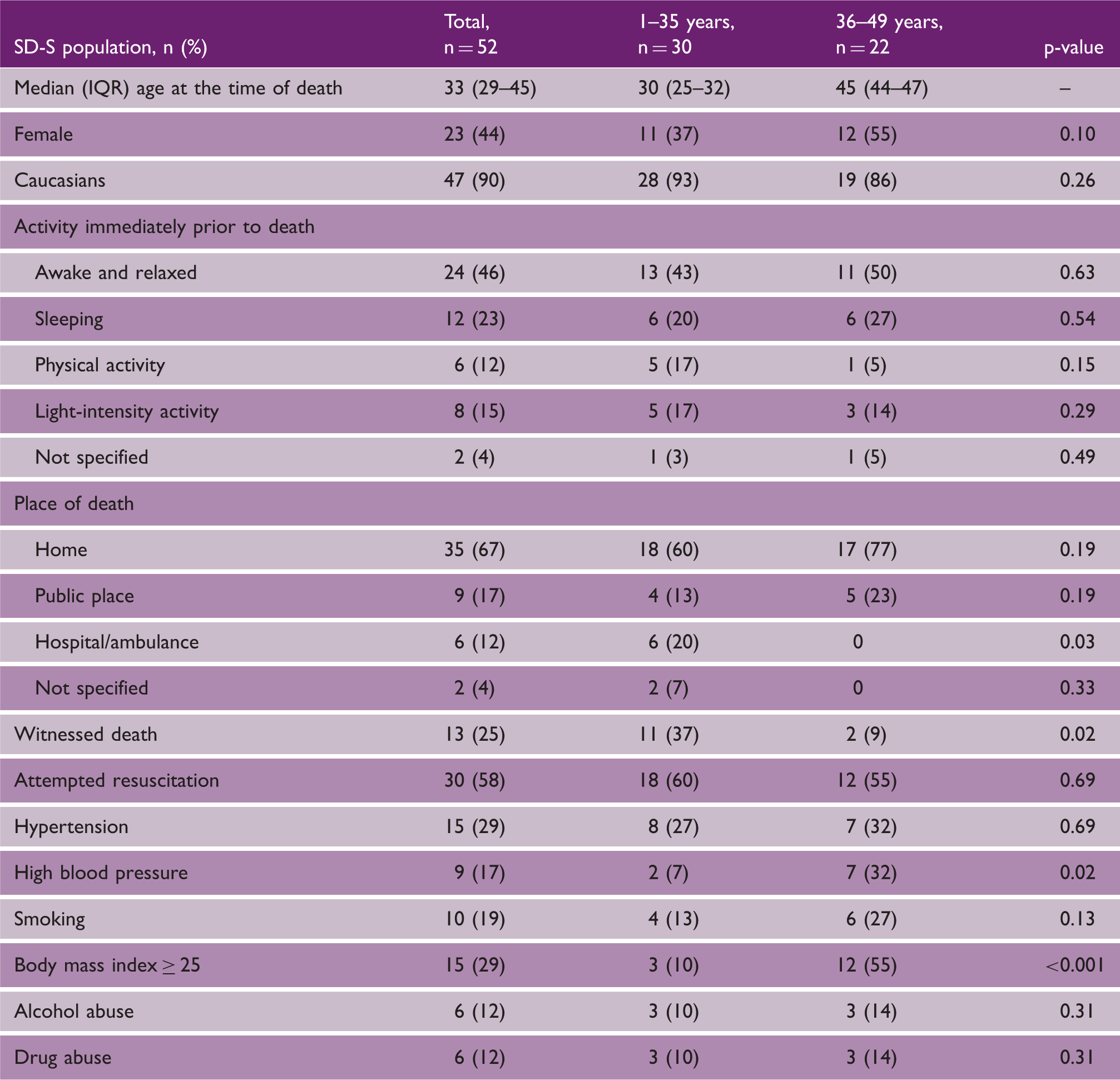
Overall, 52 cases (3% of all SD) were categorized as SD-S, making it the fourth most common cause of SD (Figure 1). Clinical characteristics are shown in Table 1. Three cases were aged <20 years. In 20 of the SD-S cases (38%), no previously known medical history was known. The most common known diseases were psychiatric disorders (n = 11, 21%). Medical history and use of medication among cases is shown in Supplementary Table 1.
Flowchart identifying all cases of sudden death by stroke in individuals aged 1–35 years and 36–49 years between 2000–2009 and 2007–2009, respectively. Clinical characteristics and medical history in cases of SD-S in persons aged 1–49 years in Denmark by age SD-S: sudden death by stroke; IQR: interquartile range.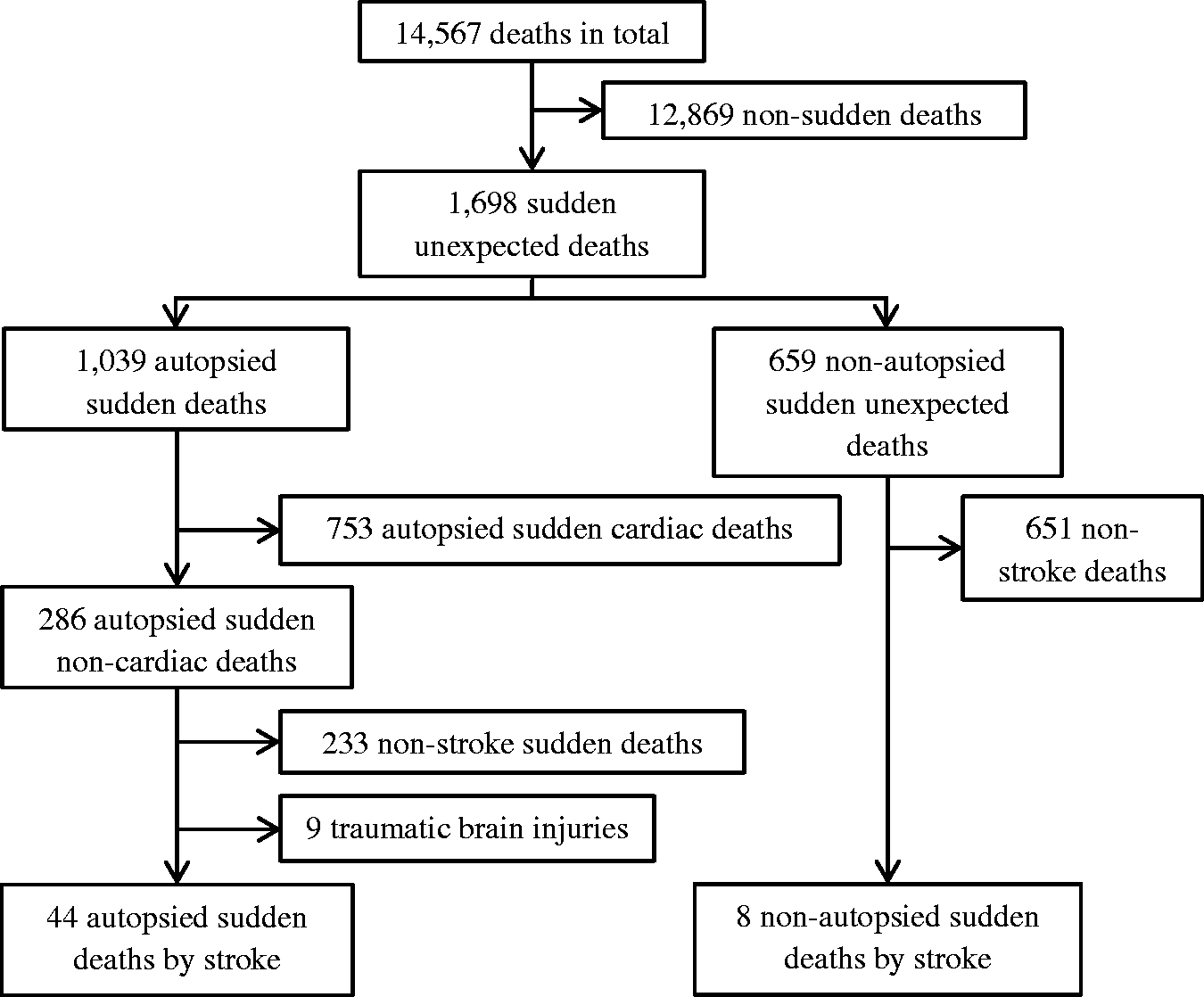
Incidence of SD-S
The incidence of SD-S was 0.19 (95% confidence interval (CI) 0.14–0.25) per 100,000 person-years in individuals aged 1–49 years. The incidence rate was 0.13 (95% CI 0.09–0.18) in persons aged 1–35 years and 0.66 (95% CI 0.43–1.00) in persons aged 36–49 years per 100,000 person-years, with an incidence rate ratio of 5.2 (p < 0.01). Incidence of SD-S for the age groups 1–17, 18–45, and 46–49 are shown in Supplementary Table 2.
Cause of death
Hemorrhagic subtypes in cases of SD-S in persons aged 1–49 years in Denmark by age
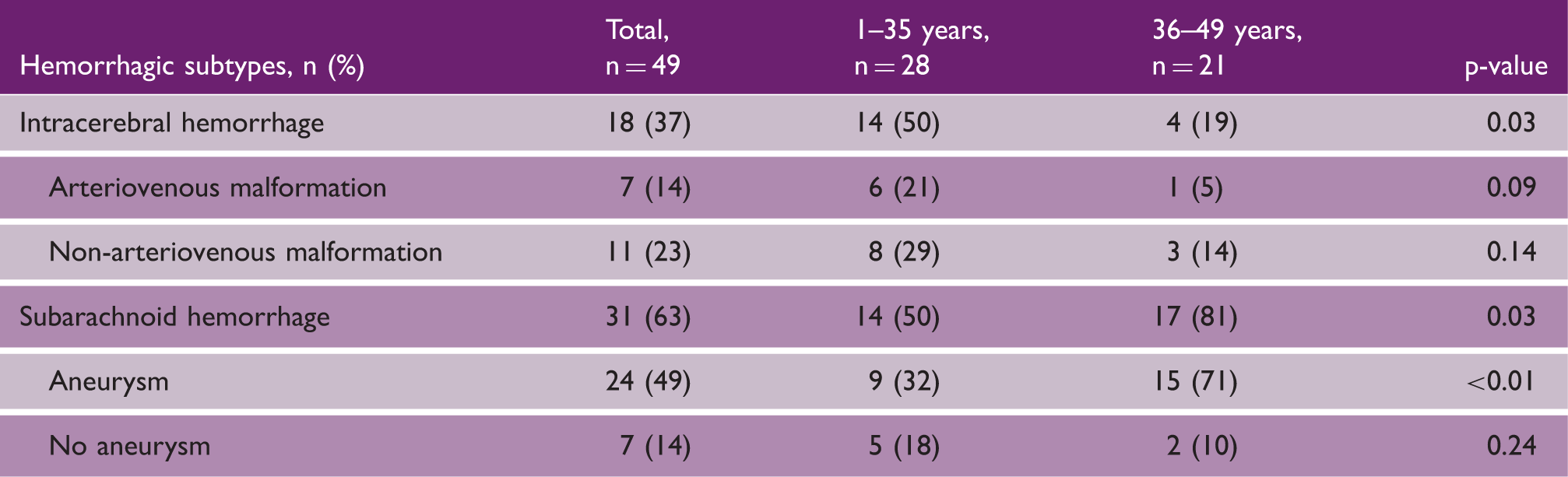
SD-S: sudden death by stroke.
Neurological symptoms
Neurological symptoms a prior to sudden death by stroke caused by a hemorrhage in persons aged 1–49 years in Denmark
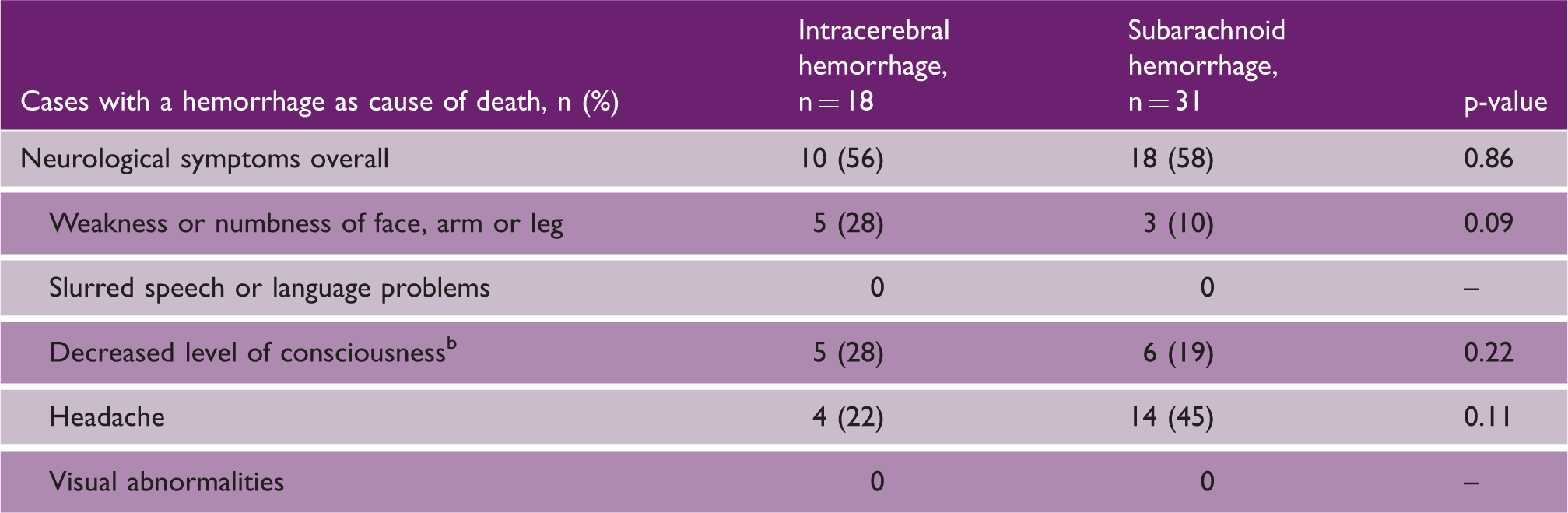
Within one year prior to death.
Including confusion.
In total, 17 patients (33%) contacted the healthcare system on basis of their neurological symptoms; six cases had contact with their general practitioner, nine with an emergency department, and two contacted both. Among the 17 patients who sought medical attention, 7 (41%) had two or more neurological symptoms whereof one was headache. Stroke was suspected in one of the 17 patients who sought medical attention.
Discussion
We present the first nationwide study on SD-S in the general population aged 1–49 years. Our main findings were: (1) SD-S occurs with an incidence rate of 0.19 per 100,000 person-years, (2) persons aged 36–49 years have a five-fold increased risk of SD-S compared to persons aged 1–35 years, and (3) hemorrhagic strokes are by far the most frequent cause of death in SD-S cases (94%).
Incidence and cause of death
Even though SD-S is a rare phenomenon, it remains one of the leading causes of sudden non-cardiac death and an estimation of the overall burden is pivotal. We found SD-S to be the cause of death in 3% of all SD cases in children and young adults, which makes it the fourth most common cause of SD after sudden cardiac death, SD by pulmonary embolism, and infectious diseases. Previous studies have suggested cerebrovascular disease to be the cause of SD in 4% to 14% of cases.5–12 However, these studies have either been conducted on selected patient populations (e.g. military recruits) or based on findings from one forensic department or region of a country, thereby potentially not reflecting the true incidence of SD-S in the general population. Furthermore, the studies are often based on data from low-income countries that have higher risk of stroke than high-income countries, in large explained by a difference in patterns of risk factors for stroke (e.g. smoking). 20
As this study is the first to estimate incidence rates of SD-S in a nationwide and unselected setting the lower incidence of SD-S found is probably a better reflection of the true incidence rate in the general population in high-income countries.
We observe a significantly higher incidence of SD-S in the 36–49 year age group, which most likely is a consequence of the age-related increased risk of stroke. 21
The low proportion of ischemic strokes in our study (n = 3, 6%) implies a more severe pathology in the hemorrhagic strokes within the first 24 hours in the young. Our observations are in accordance with Pekmezovic and colleagues, who found hemorrhagic stroke to be a more common cause of death than ischemic stroke for both sexes in all age groups up until 59 years of age. 22
Neurological symptoms
A previous study of hospitalized stroke patients aged 45–64 years showed a high frequency of stroke symptoms before admission. 23 They found that 56% of cases with hemorrhagic stroke, and 22% of patients with an ischemic event, presented with headache at admission. However, as the authors state, their results were limited to hospitalized patients and data on cases experiencing strokes resulting in out-of-hospital death were unavailable. Our data which includes out-of-hospital and in-hospital deaths supports that neurological symptoms prior to stroke (58%) are common and that headaches are the most frequent symptom. Together, this shows that neurological symptoms prior to stroke are common in both those who survive and those who die suddenly.
It is unlikely that preventive actions can be undertaken in patients with only prodromal symptoms minutes prior to SD, as the time window for intervention is very narrow. However, 50% of cases reported neurological symptoms earlier than 1 hour prior to death and 33% of cases contacted primary and/or secondary healthcare providers before death. The low incidence of SD-S combined with the high incidence of headache in the general population make identification of patients at risk difficult. Koivunen and colleagues found hemiparesis and headache as the most common symptoms upon arrival at the hospital in persons aged <50 years with first-ever ICH, and that the symptoms in the young were milder compared to a cohort of ICH patients >50 years of age. 24 This emphasizes the difficulty in identification of patients at risk. Nonetheless, our data highlight that general practitioners and other first responders should be aware of patients with an unexpected onset of severe headache without an apparent explanation, especially if the headache is accompanied by other neurological symptoms, but studies comparing symptoms in hemorrhagic strokes versus controls are warranted.
Study strengths and limitations
The strength of our study is its comprehensive inclusion of all deaths in a 10-year period in a nationwide setting followed by a thorough investigation of cause of death and characterization of the cases. We retrieved information from medical journals from hospitals and general practitioners, Danish death certificates, autopsy reports, and registries. Only 0.6% of all 14,567 deaths were excluded due to incomplete death certificates.
Our study on SD-S was limited by the retrospective study design. A prospective study design would be superior regarding the registration of relevant data. However, the conduction of a prospective study is complicated by the low incidence of SD-S. We only included SD-S cases verified by autopsy or imaging and therefore we most likely have missed some cases of SD-S. However, autopsies in Denmark are performed relatively often in SD-cases and, in the study period, an autopsy was performed in 80% and 50% of all cases of SD in patients aged 1–35 years and 36–49 years, respectively, thereby limiting the problem.
Although we extracted information from all possible sources, the frequency of symptoms might have been underestimated, as 75% of the SD-S cases were unwitnessed at time of death.
Conclusion
Hemorrhagic stroke was the most common cause of death among young persons aged 1–49 years suffering SD-S. In those aged 1–35, ICHs were more prevalent, while SAHs were more predominant in persons aged 36–49 years. We found a high frequency of neurological symptoms prior to SD-S. Increased awareness among healthcare professionals and researchers towards stroke symptoms in the young may lead to earlier detection of stroke, and thereby potentially lowering the incidence of SD-S.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Novo Nordisk Foundation and the European Union’s Horizon 2020 research and innovation programme under the acronym ESCAPE-NET, registered under grant agreement no. 733381.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.