
Abstract
About one-fourth of ischemic strokes occur in working-aged individuals in the high-income countries, with worldwide increasing incidence in this age group from 1980s to present. Recent evidence suggests that traditional vascular risk factors are more prevalent than previously suggested in young adult stroke patients and they accumulate with age particularly in men. Accordingly, relatively high rates of atherosclerotic changes have been detected in these patients. The strength of association of vascular risk factors has gone poorly studied, however. Many young patients with ischemic stroke have, in turn, no traditional risk factors, while they may harbor other conditions with weak or uncertain association with the stroke alone. These individual conditions often represent a risk factor that may be strictly young-age specific, more prevalent in younger than older stroke patients (e.g. patent foramen ovale), or more prevalent among the young in the population. Despite high rates of vascular risk factors and atherosclerotic changes, these findings do not translate to higher frequencies of identified classical stroke mechanisms. In fact, cryptogenic causes are markedly common and even more frequent among the very young patients. Limited randomized trial evidence exists to support secondary prevention decision-making in patients, yet they face an increased risk of death and future vascular events for years to come—dependent on risk factor profile and cause of the stroke. This review provides an overview of recent data on epidemiology, risk factors, and their strength of association in ischemic stroke in the young. Furthermore, the relationship between with the risk factors and cardiovascular outcomes and key features on the evidence related to secondary prevention will be discussed.
Introduction
Ischemic stroke is no longer a disease affecting just elderly people, since one-fourth of ischemic strokes occur in working-aged individuals in the high-income countries, new stroke striking an estimated 3.6 million young people each year. The burden of young stroke may be increasing further, since multiple recent studies have reported increasing incidence of ischemic strokes particularly at younger ages since 1980s, while incidence at older ages has been declining during the same period.1–5 Globally almost half of the entire stroke burden now affects young individuals given that they have a greater likelihood to survive their strokes with long life spans ahead and because strokes occur at younger ages in low- and middle-income countries. 6 Moreover, the overall population burden of cerebrovascular disease in the young may be underestimated, since clinically silent infarcts and white-matter changes have been shown to be prevalent even in young stroke patients.7,8
Approximately 10% of ischemic strokes occur in people aged less than 50 years, which is the age cut off most often used to define “early onset” or “young-onset stroke” or “stroke in young adults.”9,10 The age cut off is biologically arbitrary but is based on the differing clinical characteristics between younger and older stroke patients, in particular risk factors and etiology. 11
Recent evidence suggests that traditional vascular risk factors are highly prevalent in young adult stroke populations with distinct demographic characteristics,12,13 yet the strength of association of these risk factors has received scarce attention. On the contrary, there are also young patients without traditional risk factors, while these individuals may harbor other conditions with only weak or uncertain association with the stroke alone. These conditions often represent a risk factor that may be strictly young-age specific, more prevalent in younger than older patients, or more prevalent among young people in the population.
Although vascular risk factors among young stroke patients may be more common than previously suggested and relatively high rates of atherosclerotic changes have been detected, these findings do not translate to higher frequencies of identified classical stroke mechanisms.14,15 In fact, undetermined (or cryptogenic or hidden) causes are exceedingly common and even more frequent the younger the patients, the proportion exceeding 50% in patients younger than 30 years.16,17
This review first provides an overview of recent epidemiological findings on ischemic stroke in the young. Second, the current knowledge on the prevalence of modifiable traditional vascular as well as unconventional risk factors and their strength of association with early onset stroke will be discussed. The last part of the review will cover the relationship between with the risk factors and cardiovascular outcomes as well as key aspects on the evidence of secondary prevention in this patient population.
Literature search
References for this review were identified through searches of PubMed with the MeSH search terms “Stroke” and (“Young Adult” or “Adult,” or “Middle Aged”). Further search restrictions were done based on the review topics, including terms “Incidence,” “Risk Factors,” (“Etiology” or “Pathogenesis”), “Patent Foramen Ovale,” (PFO) and “Prognosis.” Relevant papers were also identified through searches of author’s files and by review of reference lists of the relevant articles. Congress abstracts were excluded and only full-text articles published in English were considered.
Incidence of ischemic stroke at younger ages
Relatively few studies have assessed the incidence of ischemic stroke in the young, it is important to bear in the mind the varying upper age cut off and population when comparing the rates. From the last three decades the reported rates for individuals aged 15–45 vary from 3.4 to 21.7 per 100,000,18–23 the highest rate observed for Blacks in the Baltimore–Washington area. 20 For those aged 15–49, incidence ranges from 10.8 to 11.4 per 100,000 in people of Northern European origin.9,24
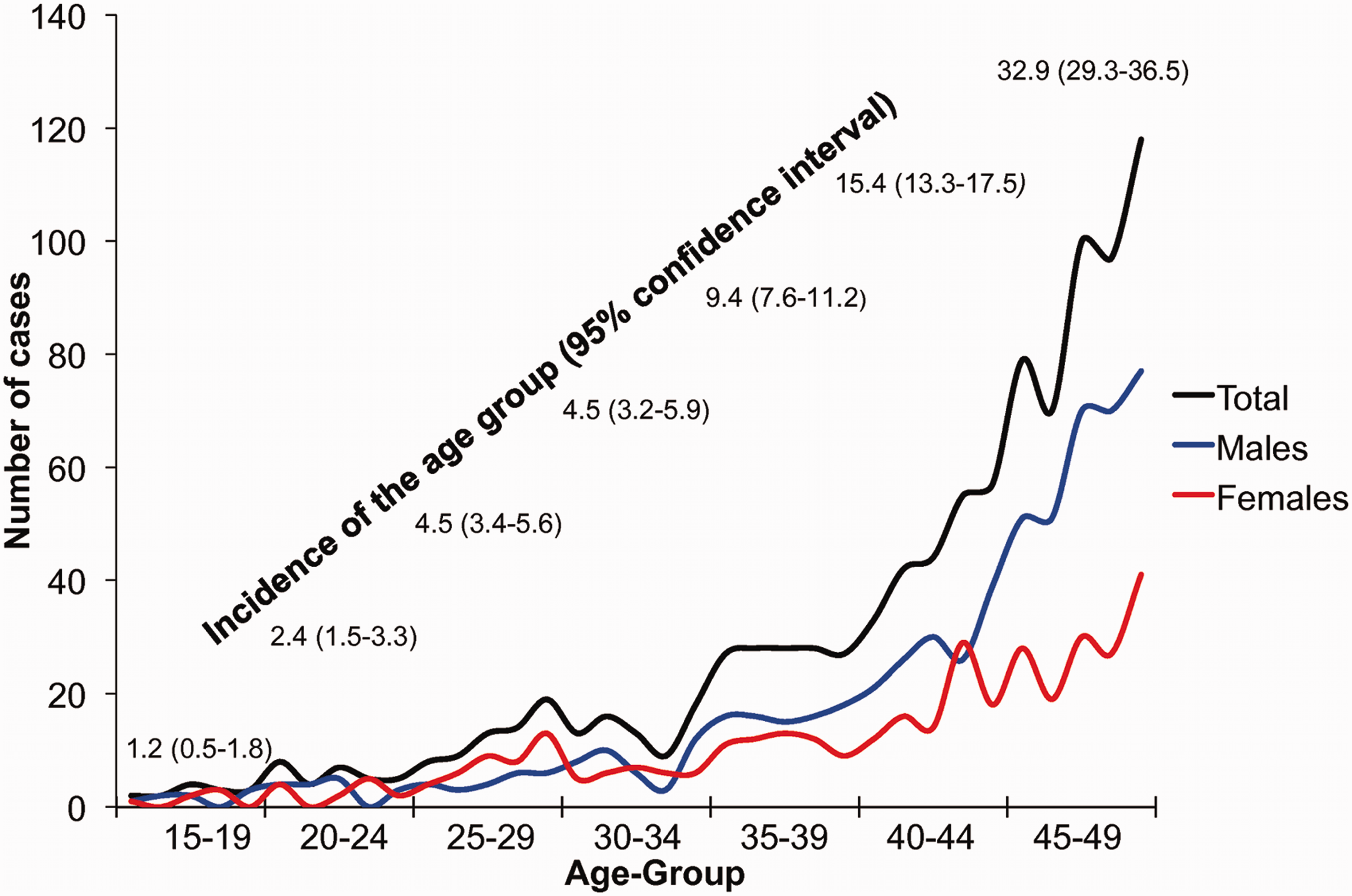
Incidence remains low among the youngest individuals, ranging from 1.2 to 4.5 per 100,000 in those aged <35 years, but then steeply increases with age, reaching 32.9 per 100,000 among those aged 45–49 years (Figure 1).
9
Generally in the young incidence for men is higher except for a few studies reporting higher incidence for women.23,25 There are notable gender differences in the occurrence of early onset stroke, as women outnumber men among those aged <35 years, whereas men outnumber women among those aged above 35 but less than 50 years (Figure 2).
13
The reasons for these sex discrepancies probably include gender-specific risk factors in reproductively active young women and clustering of traditional risk factors in middle-aged men, as discussed below.
Occurrence rates of ischemic stroke according to age and sex among individuals aged 15–49 years. Data are from the Helsinki Young Stroke Registry including 1008 consecutive patients with first-ever ischemic stroke.
9
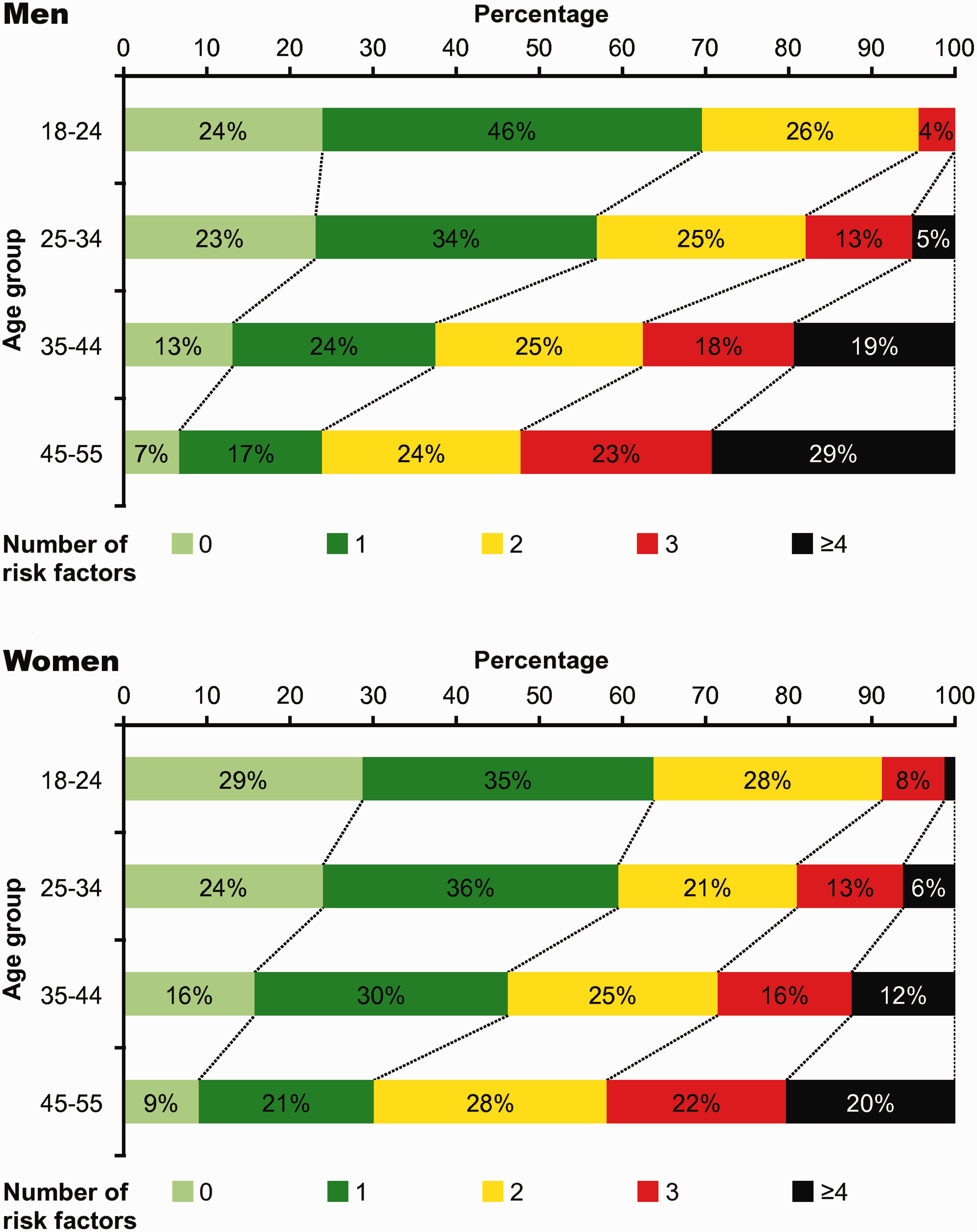
Prevalence of traditional vascular risk factors in young adults with ischemic stroke according to sex and age group. Adapted from von Sarnowski et al.
12
A number of recent epidemiological studies remarkably show that incidence of ischemic stroke at younger ages has been increasing since 1980s to present.1–5 Some of the studies showed more pronounced incidence increase in women,1,4 which challenges the current epidemiologic view of male preponderance in ischemic stroke. 26
Possible explanations for the increasing incidence include (1) artificial, i.e. improved awareness in the population or improved diagnostic accuracy; (2) growing prevalence of known stroke risk factors, e.g. increasing prevalence physical inactivity, obesity, type 2 diabetes mellitus, increasing use of alcohol and illicit drugs; (3) increasing prevalence of factors related to modern life style with limited scientific evidence and uncertain causality, e.g. 24/7 society syndrome including long work hours, shift work, long-haul flights, information overload, chronic stress, sleep deprivation; or (4) external reasons, such as increasing exposure to particulate matters in the air.
Only scarce systematic data are available thus far regarding the reasons for the increasing incidence of early onset stroke. Kissela and coworkers demonstrated a growing use of MRI in stroke diagnostics from early 1990s to 2005 correlating to improving diagnostic accuracy, but similar change in MRI use was seen across all age groups and with even greater magnitude for those aged ≥65 years. 3 National surveys suggest an increase in the population prevalence of obesity, hypercholesterolemia, and diabetes (www.cdc.gov/nchs/nhanes) and in young stroke patients smoking, alcohol drinking, and illicit drug use have been increasing during the same period as the observed increase of incidence. 27 Probably some of the increment might be explained by improved diagnostics and disease awareness, but the strong risk factors becoming more prevalent appear among the most robust potential explanations underlying the increasing incidence at younger ages.
Prevalence of traditional modifiable risk factors in young patients
The Stroke in Young Fabry Patients (SIFAP1) study was a prospective European multicenter study, which primary aim was to decipher the prevalence of Fabry disease in unselected 5024 young (age 18–55 years) stroke patients, recruited from 2007 to 2010. While definitive Fabry disease was diagnosed in 0.5% of the entire cohort, 16 the database also provided—for the first time in this scale—systematic information on the prevalence of well-documented vascular risk factors in young stroke patients. The four most frequent risk factors were current smoking (56%), physical inactivity (48%), hypertension (47%), and dyslipidemia (35%). One out of 10 had diabetes mellitus. 12
Obesity defined as body mass index (BMI) ≥ 30 emerged in 22% of the SIFAP1 study patients, yet if defined with waist circumference (≥94 cm for men, ≥80 cm for women), abdominal obesity was in fact the most prevalent risk factor in the cohort (i.e. 69%). 12 BMI ≥ 30 has been shown to be more prevalent among younger individuals in the population 28 and this measure of obesity has recently been associated with young-onset stroke in a case–control study. 29 However, the risk effect of BMI ≥ 30 may be mediated through associated conditions such as hypertension and diabetes mellitus since the association was greatly attenuated after adjusting for these factors. 29 Compared to BMI, anthropometric measures of abdominal fat including waist circumference, waist-to-hip ratio, and waist-to-stature ratio may, however, more accurately predict stroke risk and independent of other risk factors 30 and should be used in future studies addressing stroke risk.
In the SIFAP1 study, most of the modifiable risk factors, including current smoking, hypertension, dyslipidemia, diabetes, and excess alcohol drinking were more prevalent among men, while physical inactivity and high waist circumference were more prevalent in women. In addition, there was a notable clustering of these vascular risk factors with age in both sexes but significantly more pronounced in men (Figure 2). 12 Outstandingly, only 7% of men aged 45–55 and 9% of women of the same age group harbored none of the traditional risk factors in the study. Similar findings of risk factor clustering have been noted in other retrospective studies as well, with no differences in the risk factor profiles across European regions. 13
Strength of association of early onset vascular risk factors
For stroke in the young, the strength of association of risk factors is probably most solidly proven for smoking. Several studies with participants from multiple ethnicities have shown the association for smoking and early onset ischemic stroke, with odds ratios (OR) ranging from 1.6 to 7.7.31–37 A cumulative dose effect for smoking has been demonstrated with no significant heterogeneity between etiologic subtypes appeared. 37
In contrast to smoking, surprisingly scarce data are available regarding the strength of association of other well-documented risk factors in young adults. For hypertension, ORs have ranged from 1.6 to 8.9 in the few case–control studies including young adults.31–36,38 Interestingly, in the INTERSTROKE study OR for hypertension was 3.14 for ischemic stroke, but a substantial risk augmentation was observed for those ≤45 years (OR, 8.53), yet this estimate was for all stroke including ischemic and hemorrhagic stroke. 39
There is also other—yet limited and indirect—evidence that the association of traditional vascular risk factors may be stronger for younger individuals. For instance, the INTERSTROKE OR for diabetes mellitus was 1.6, but in young adults the few studies have suggested ORs ranging from 3.3 to 11.6, or even as high as 22.9 for white men in the Baltimore–Washington area.31,32,34,36 There is dearth of data regarding the diabetes subtypes in young adults with stroke, but it is reasonable to suggest that the strength of association would be stronger for type 1 juvenile diabetes mellitus than for type 2 diabetes mellitus. 40 Notably, a study that followed patients with type 2 diabetes mellitus found that the hazard of any macrovascular complication was twofold but the hazard stroke even 10-fold for those with early onset form of type 2 diabetes compared with patients with usual-onset type 2 diabetes despite similar average time to require insulin in the groups. 41 At least to some extent vascular comorbidities emerging at young age may thus represent earlier and more aggressive forms of the diseases—i.e. “early onset forms of older-onset risk factors,” leading to loss of the relative protection of youth. 41
Physical inactivity is among the most prevalent modifiable risk factors in young stroke patients, but its strength of association has remained nearly unstudied. A study performed on a Thai population aged 18–45 years found that history of no or irregular exercise increased stroke risk by eightfold after adjusting for confounders. This OR was of similar magnitude as for hypertension in that population. 38 Physical inactivity is linked to metabolic syndrome and its components and so an Indian study found the presence of three or more components of the metabolic syndrome to be associated with early onset stroke. 32
Regarding cholesterol and its components, an association between low high-density lipoprotein cholesterol and ischemic stroke at young age has been demonstrated,32,35,38 but no clear association has been shown for total cholesterol, low-density lipoprotein cholesterol, or triglycerides. A recent meta-analysis suggests that the association of lipoprotein(a) and ischemic stroke is stronger for young adults aged <55 years than for older individuals. 42
A few studies found rather modest association for a composite variable of heart disease with varying definitions.33,34,36 Association of early onset atrial fibrillation has not been assessed in young stroke patient populations, although its prevalence might be underestimated. 43 Regarding obstructive sleep apnea, one study suggests higher stroke risk for women aged ≤35 years compared to older age groups and relatively higher risk for women compared to men. 44
The associations of long-term 36 and recent heavy drinking34,45,46 and ischemic stroke have been demonstrated in young adults. The association of heavy drinking may also be stronger for younger adults.47,48 One study has also shown a protective effect of mild-to-moderate drinking in young women, 49 which is in accordance with the J-shape association found in nonselected populations. 48 Binge drinking pattern is more common in young individuals, 50 a risk factor for both ischemic and hemorrhagic stroke particularly in young adults.34,51
Are there risk factors specific for young stroke?
Risk factors for ischemic stroke that may be considered specific to young adults.

OR: odds ratio; RR: relative risk.
Pooled estimate of the risk if meta-analysis level of data available.
In the absence of antiphospholipid antibody syndrome or systemic lupus erythematosus.
Variability in the prevalence is primarily due to selection of cohorts and usually higher for cryptogenic cases.
Generally, the evidence base underlying the association of the risk factors presented in Table 1 is much weaker than for the well-documented vascular risk factors; the results have often been inconsistent between studies. Most of the original studies are small case–control studies prone to different sources of bias. Meta-analysis level of evidence is limited and virtually restricted to most extensively studied conditions such as migraine.54–56 Only very few of these risk factors have shown dose dependency and time dependency, which would be needed to increase the probability of causal link between the risk factor and studied endpoint. It remains largely speculative, how much of young stroke would be attributable to these risk factors.
A notable common feature for the less well-documented risk factors is that most of them are frequent in the background population. Therefore, it is plausible to hypothesize that several concomitant factors may be needed to cause the effect, endpoint stroke. Examples of such situations include antiphospholipid antibodies needing an external trigger or concomitant factor such as infection 80 or estrogen use. 59 Also for migraine with aura, additional factors may be needed including smoking and estrogen to aggravate the low independent risk. 81 PFO constitutes another similar condition with uncertain risk alone, as discussed below.
The high burden of risk factors does not translate into large proportion of definitive stroke mechanisms in young adults
The single most frequent cause of young-onset ischemic stroke in high-income countries is arterial dissection. 82 Dissection together with other generally rare causes considered the typical causes for young-onset stroke explains only about one-fourth or one-fifth of all causes. These rare causes include, e.g. Fabry disease, CADASIL (cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy), MELAS (mitochondrial myopathy, encephalopathy, lactic acidosis, and stroke), Moyamoya disease, reversible cerebral vasoconstriction syndrome, systemic or primary central nervous system vasculitis, cardiomyopathies, HANAC syndrome (hereditary angiopathy with nephropathy, aneurysms, and muscle cramps), Sneddon’s syndrome, sickle-cell disease, and specific coagulopathies. 83 Full account of the rare conditions is beyond the scope of this review.
Despite the recent studies showing a high prevalence of traditional risk factors in young adults with ischemic stroke, this fact does not translate into high frequency of patients classified as having typical older-onset causes for their stroke.9,16,17 The SIFAP1 study is the largest cohort to date of young stroke patients aged 18–55 with standardized diagnostic approach and brain MRI in all patients, and 3396 patients with ischemic stroke and 1071 with transient ischemic attack (TIA) enrolled.
16
According to Trial of Org 10172 in Acute Stroke Treatment (TOAST) classification,
84
the frequency of large-artery atherosclerosis in the SIFAP1 cohort was 18.6% and that of small-vessel disease 13.5%, with higher frequencies in men. Most patients with these diagnoses fell in the oldest age group of 45–55 years, while 33.4% of the entire cohort had undetermined cause. Notably, the proportion of cryptogenic strokes was larger among younger age groups. Another study that pooled data from 15 hospital-based registries of ischemic stroke at age of 15–49 (n = 3331) also showed increasing frequency of large-artery atherosclerosis and small-vessel disease with age and higher prevalence of these causes in men.
17
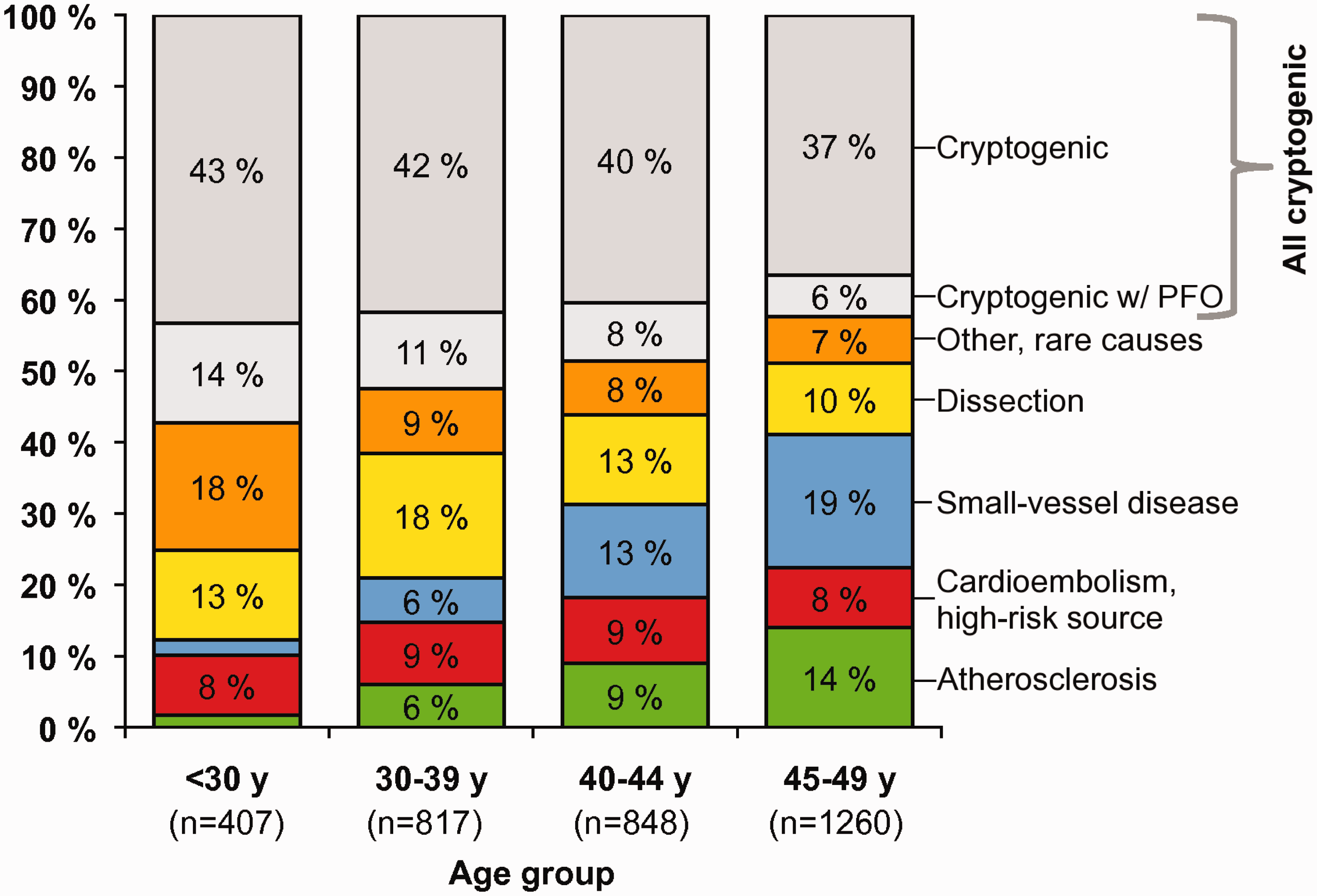
In accordance with SIFAP1 study, the frequency of cryptogenic strokes in that study was substantial and larger among the youngest age groups, being up to 57% among those aged < 30 years if PFOs were included in the count (Figure 3).
17
Distribution of etiologic subgroups in young adults with ischemic stroke according to TOAST classification in pooled data from 15 hospital-based registries. Data adapted from Yesilot Barlas et al.
17
Regardless of the large proportion of unknown causes, recent findings, however, challenge the traditional view about low prevalence of atherosclerosis in young stroke patients. Another analysis based on the SIFAP1 cohort showed overall prevalence of extracranial stenoses of 8.9% and of intracranial stenoses of 11.8%. Together with nonstenotic plaques, one-fifth of the cohort had symptomatic or asymptomatic atherosclerotic findings. 14
How do the etiologic classification schemes perform in young stroke?
An important issue that may artificially increase the proportion of both young and old cryptogenic strokes is the nature of classification systems. The most widely applied classification, TOAST, was developed for more than two decades age for the purposes of a clinical trial and may be simply too robust and unspecific for young patients. Furthermore, it has an overall rather modest reliability between raters. A recent study on young ischemic stroke patients 85 utilized a new online classification system developed based on the old TOAST, the Causative Classification for Stroke, which uses certain sophisticated rules to guide the rater and has greater inter- and intra-rater reliability. 86 Utilizing careful and extensive diagnostic workup, that study 85 suggested that causal etiology could not be determined in only 11% of patients. However, a large proportion of cardioembolic strokes had only isolated PFO, with no proof of its causality.
The new ASCO (A for atherosclerosis, S for small-vessel disease, C for cardiac source, O for other cause) classification characterizes patient phenotype in a more comprehensive manner, considering relevant underlying diseases and grades of evidence of the causative pathology as follows: grade 1, definitive cause; grade 2, causality uncertain; grade 3, unlikely a direct cause but the disease is present. Nevertheless, attempts to classify young patients with ASCO may lead to even larger proportions of undetermined causes, as exemplified by a study by Larrue and colleagues where 52.7% of their subcohort aged 16–44 years and 39.0% of those aged 45–54 years had no definite cause (grade 1 pathology). 87 Reclassification of the SIFAP1 patient population led to an even larger proportion of those without definitive grade 1 cause, 70.7%. Absence of grade 1 or 2 pathology was detected in 45.9%, but about 50% of patients in that study had more than one finding with uncertain causality and high prevalence of findings compatible with concomitant atherosclerosis in the large arteries or findings supportive of small-vessel disease. 15
PFO—An example of a simple structure with a complex role in the chain of causality
Much of the uncertainty in classifying the potential cause considers PFO, constituting a significant proportion of undetermined young-onset strokes. PFO can serve as a conduit for paradoxical embolism originating in deep vein thrombosis, but as simple as it appears in case reports, PFO in fact exemplifies the entire complexity of determining the potential pathogenetic mechanism for stroke in the absence of a definite cause. As many other risk factor with uncertain causality, PFO is common (≈25%) in the general population, 88 which leads to high probability that PFO is just an innocent bystander. 89 Although case–control studies demonstrate an association for PFO and stroke, 57 no association appears in strictly population-based studies. 58 Proving the definite causality in clinical practice remains a challenge as it requires that the venous thrombosis be diagnosed prior to stroke, which is rarely the case. It is therefore reasonable to argue there must be other concomitant factors—persistent or transient, recent or remote—predisposing to paradoxical embolism in individuals with suggested PFO-related stroke. These include transesophageal echocardiography features—such as PFO length and size, presence of atrial septal aneurysm, and right-to-left shunt at rest90—as well as precipitants elevating the risk for venous thrombosis (e.g. bed rest, long travel, immobilization, trauma, lower extremity caster), infections, prothrombotic conditions, 91 and recent physical activity, particularly those inducing Valsalva maneuver.
Most studies have applied no criteria for adjudicating PFO as causal or incidental, so the decision has merely relied on the individual physician or investigator. A recently developed Risk of Paradoxical Embolism (RoPE) score may help to identify those PFOs that would be causally relevant. The score, ranging from 0 to 10, is composed of age (0–5 points: 5 points if age 18–29 years, 0 point if age ≥70 years), presence of cortical infarct, and lack of traditional risk factors (one point for each of the following: no hypertension, no diabetes, no history of stroke or TIA, nonsmoker). 92 It was further evaluated whether the transesophageal echocardiography characteristics were associated with the clinical features assessed with the RoPE score suggesting that PFO would be pathogenic—but no evidence of such association was found. 93 Therefore, additional measures for determining the pathogenetic role of PFO are needed and alternative causes to paradoxical embolism, such as vulnerability to atrial arrhythmia 94 and thrombosis generation in PFO itself should be explored. In addition, venous thrombosis in the pelvic veins or pulmonary embolism might be underestimated sources for embolism as suggested by a few rather small prospective 95 and retrospective96,97 studies, albeit some of the results are conflicting, 98 warranting larger prospective investigations.
The relationship of clustering risk factors and dismal cardiovascular prognosis after stroke in the young
Although it may seem favorable as compared to older stroke patients, recent follow-up studies have challenged the traditional view, which considered the prognosis of young adult stroke generally favorable. A Dutch study showed a fourfold higher mortality for young patients with stroke compared to age- and sex-matched background population, with excess mortality present across all age groups, but particularly for those aged 35–50 years. 99 In the most recent studies on long-term mortality in young adult stroke, cumulative mortality has ranged from 1.9 to 5.2% at one year, 9 to 11% at five years, 12 to 17% at 10 years, and 27% at 20 years, with the highest annual rate in the first year.99–105 Importantly, more than half of the deaths in the long term seem to occur due to vascular causes, of which majority are other than strokes.99,101 Regardless of stroke etiology and demographic factors, increasing number of vascular risk factors has been shown to be an independent marker of elevated risk of death in the long term.106,107 Of the TOAST categories, large-artery atherosclerosis carries the highest risk for death. 106
Cumulative risk of recurrent stroke in young stroke survivors is nonnegligible, ranging from 9.4% at five years to 19.4% at 20 years in the largest of the recent consecutive series.108,109 Composite of any vascular event occurred at a rate of 11.5% at five years, 108 30.4% at 10 years, 100 and 32.8% at 20 years. 109 As for mortality, the risk for recurrent stroke and vascular events is highest during the first year but remains high for years after the index event. Increasing number of vascular risk factors independently predict as well recurrent vascular events in these patients.106,109,110 Compared with undetermined causes and other determined rare causes, the highest risk for recurrent stroke and vascular events emerge for large-artery atherosclerosis, cardioembolism, and small-vessel disease, yet recurrences occur across all etiologic subgroups.108,109
Scarcity of evidence is guiding secondary prevention
General guidelines are adopted for the treatment of early onset strokes, despite young patients typically are underrepresented in randomized trials and so the results may not be directly translated to apply all young patients. The virtually only randomized data for secondary prevention that considers specifically younger patients or causes that are common among young patients come from the Patent Foramen Ovale in Cryptogenic Stroke Study (PICSS), 111 the Cervical Artery Dissection in Stroke Study (CADISS), 112 and from the recently completed three trials comparing transcatheter closure of PFO with best medical treatment. 113 PICSS was a subcohort to a larger study and showed no difference in the risk of stroke or death in rather young patients (mean age 59 years) between those treated with aspirin or warfarin. There was, however, a nonsignificant trend in favor of warfarin in the subgroup of cryptogenic strokes, yet of similar magnitude in patients with and without PFO. 111 CADISS study showed a very low rate of recurrent strokes in patients aged 49 years with cervical or vertebral artery dissection and so managed to show no difference between aspirin and anticoagulation. 112 Finally, after none of the individual trials comparing transcatheter closure of PFO with best medical treatment showed a treatment effect favoring either one of the treatments, a Cochrane meta-analysis of the three trials concluded that closure might in fact be harmful due to increased risk of atrial fibrillation. However, there might be benefit from the closure using a device with a high rate of success in carefully selected patients, yet further studies are warranted. 113
Conclusions
The impact of early onset stroke is becoming more important in the population due their increasing incidence from 1980s to present, with young stroke causing now almost half of the entire stroke burden globally.
One of the main reasons for the increase in incidence may be that vascular risk factors have become more prevalent in the population. Recent findings are thus challenging the traditional view that classical risk factors would play a minor role in young stroke. As opposite, vascular risk factors are highly prevalent and in parallel with the clustering of vascular risk factors with distinct demographic patterns, mortality and risks of recurrent stroke and other vascular events are increased for years after the index stroke, exceeding the corresponding risks in the background population.
Regarding stroke subtypes, the highest risk of recurrent events appears in subtypes considered typical for older-onset stroke. There may be special features in the vascular risk factors that manifest early in life and associate with early onset stroke endpoint. As an important practical implication, the identified high-risk patient groups should be subjected to more close follow-up and aggressive management of the underlying diseases.
As more knowledge has been accumulating on the traditional risk factors, a very large proportion of young patients still remain without elusive pathophysiology for their stroke. In such situations the evidence base for secondary prevention is very thin and the patients have to live in uncertainty for years. These individuals also face increased risks of death and recurrent vascular events suggesting active underlying pathologies. A number of less well-documented risk factors with generally weak associations and poorly known role in the chain of causality often are present in young patients with ischemic stroke.
There are now strong incentives to initiate large prospective collaborative studies to explore the specific features and pathogenetic roles of both early onset forms of known vascular risk factors and the less-well documented risk factors considered specific to young adults. Furthermore, the utility of novel diagnostic modalities, e.g. for cardiac and vessel-wall imaging should be investigated, 114 as well as collect samples particularly for studies of coagulopathies 115 and genetics 116 in order to establish new risk factors and causal disease mechanisms leading to early onset strokes. All this should eventually lead to developing next-generation phenotyping schemes that better fit young individuals and allow for personalized treatments and better care for young stroke patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work received support from the Helsinki and Uusimaa Hospital District.
Informed consent
N/A
Ethical approval
N/A
Guarantor
JP
Contributorship
N/A