
Abstract
The ‘What Being the Parent of a New Baby is Like-Revised’ (WPL-R) is an instrument designed to measure adaptation to parenthood. In the process of pilot testing and validating the WPL-R in a postpartum Dutch population, we became aware of the potentially sensitive nature of the measure. Despite the ethics committee waiving the invasive nature of the measure, we conducted a survey to explore its possible effect on women’s thoughts and emotions by using the Positive And Negative Affect Schedule (PANAS) to measure changes associated with completion of the WPL-R. Two hundred and fifteen questionnaires were returned. Our findings indicated a change in PANAS scores, implying an intervening effect when using the WPL-R, in research. This raises the question of whether it is acceptable to use a questionnaire with postpartum women without any knowledge of the possible effect it may have, even though the ethics committee has approved the study and considers the measure to be non-invasive.
Introduction
A mother’s 1 evaluation of the quality of her mothering is important to assess the adaptation to parenting her infant and for providing care that is specific to her needs for support. Self-reporting has been the major approach to learning about the quality of a mother’s caregiving and her satisfaction with it (Wittkowski et al., 2017, 2020). Individual mothers differ in how they evaluate the quality of their mothering (Botha et al., 2020; Pridham and Chang, 1989). Mothers’ evaluation of the quality of their mothering and adaptation to parenting their infant when completing a survey may prompt them to think about the quality of their mothering in ways they had not previously considered. Reflection on the quality of mothering stimulated by the survey questions may affect a mother’s mood. The change in mood may be positive if the mother is satisfied with how she is doing. If the change in mood is negative, however, the mother may feel less efficacious, competent and less engaged in her relationship with her infant as a direct result of completing the survey. Thus, survey instruments have ethical implications for researchers and clinicians who use them for assessment to consider when deciding to use the instrument.
Healthcare providers (or clinicians) could make use of mothers’ self-assessment and experiential knowledge of the quality of their mothering and their adaptation to parenting their infant to provide woman-centred care (Fontein-Kuipers et al., 2018). Knowledge of how well a mother perceives herself as knowing what her infant needs, for example, could lead to focussed intervention to support a mother’s development of knowledge of her baby’s needs. Dutch healthcare providers who work with mothers in antenatal, intrapartum and postnatal periods, and who could benefit from knowledge of mothers’ anticipated and perceived quality of mothering and adaptation to parenting their new infant, are the primary-care midwife, obstetrician and occasionally a general practitioner (GP) (Perined, 2020). Dutch care standards emphasise the importance of midwife and mother discussing topics such as the transition to parenthood and psychological wellbeing both pre- and postnatally, but do not specify how the delivery or reception of these topics should be assessed (De Boer and Zondag, 2018; De Boer et al., 2008; Tichelman et al., 2019). Using standardised self-report questionnaires could be of help to examine women’s thoughts on motherhood and adaptation to motherhood.
Self-evaluation instruments, including self-report survey questionnaires, although potentially useful for clarifying issues mothers may be experiencing in adapting to mothering their infant, may orient a mother’s thoughts and feelings towards negative perceptions of herself or her competence as a mother. The effect from participating in or completing a self-evaluation on the views of mothers’ regarding the quality of their mothering and adaptation to parenting warrants assessment. To date, this kind of assessment has not been provided despite its ethical implications for a mother’s psychological wellbeing and competent functioning in the mothering role.
Conducting research requires adherence to research protocols and ethics guidelines. Acquiring approval from a research ethics committee is routine practice. However, this approval is subjected to nonrational factors such as biases and heuristics, which can influence the process and the ultimate decision to approve or not approve the study conduct (Nuttgens, 2021). When a questionnaire is regarded as non-invasive and not too time consuming, ethical approval is likely to be granted. However, how do we know that asking questions about life-changing events such as becoming a parent is nonintrusive? The questions themselves may be seen as non-invasive, however the vulnerability of the target population also needs to be considered. Day-to-day life can make it hard to reflect and contemplate on recent experiences, adjustment to new roles and finding a new balance. So how does taking time to ponder these topics, for example when responding to a questionnaire, affect the respondent’s thoughts and emotions? Is there an effect from answering these questions, and if so, is this positive or negative? It is important to acknowledge that it can be difficult to determine potential harm at the outset of a study. However, researchers should endeavour to identify and assess potential harm, even after appropriate levels of ethics review have been sought and received. The purpose of the current study was to explore the possible effect of completing a questionnaire measuring adaptation to motherhood. The research question was as follows: Is there an effect of completing the WPL-R on postpartum women that can be detected as positive or negative affect?
Methods
This exploratory study used a cross-sectional online survey-based design.
Participants and procedure
Participants were recruited from February to April 2020 via social media platforms (Facebook, Instagram). We included mothers ⩾18 years of age, proficient in the Dutch language, who had given birth in the previous 12 months. In addition, they were included if they received maternity care in the Netherlands from a midwife, GP and/or obstetrician. We excluded nulliparous (pregnant) women. Participants completed an online survey via LimeSurvey, consisting of background variables, PANAS, WPL-R and again PANAS.
Measures
We collected the following socio-demographic factors and personal details: age, education level, occupational status, relationship status, parity, age of the youngest child in weeks and the maternity care provider (i.e. midwife, obstetrician, GP).
What Being the Parent of a New Baby is Like-Revised (WPL-R)
‘What Being the Parent of a New Baby is Like-Revised’ (WPL-R), developed by Pridham and Chang (1989), is a questionnaire that is used to evaluate adaptation to motherhood. The questionnaire consists of three subscales including 25 Likert-items and one open-ended question. The Evaluation subscale (11 items) asks the mother to assess her satisfaction in being the parent of a new baby, knowing what her baby needs, and meeting her own expectations as a parent. The Centrality subscale (8 items) focusses on how much the baby and caring for the baby are on the mother’s mind and on difficulties in leaving the baby behind with a partner or someone else. The Life Change subscale (6 items) contains items about changes in life, stressfulness of life, self-image and relationships with family members (Pridham and Chang, 1989). Each item is scored on a 9-point Likert scale ranging from ‘not at all satisfying’ (1) to ‘completely satisfying’ (9) or ‘very little’ (1) to ‘all of the time’ (9). The 25 Likert-items are followed by an open-ended question: ‘What else do you think is important to help us understand what being the parent of a baby is like for you?’. Internal consistency of the original scale was reported using alpha coefficients of subscales at 1 week, 1 month and 3 months postpartum: 0.87, 0.90 and 0.87 for Evaluation; 0.87, 0.80 and 0.88 for Centrality; and 0.77, 0.81 and 0.81 for Life Change (Pridham and Chang, 1989).
The WPL-R was translated into Dutch by authors EB and YK in consultation with the developer of the questionnaire and author KP. The items were subsequently back translated into English by a native English and native Dutch speaker. Discrepancies were reviewed and discussed with the back-translator, and authors EB and YK adapted items consisting of small changes in wording. The validation of the Dutch WPL-R will be described elsewhere.
Positive and Negative Affect Schedule (PANAS)
The Positive and Negative Affect Schedule (PANAS) was developed to measure two primary dimensions of mood: positive affect (PA) and negative affect (NA) (Watson et al., 1988). The PANAS is widely used to assess PA and NA and has been validated in several languages, including Dutch (Peeters et al., 1996). The PANAS (Watson et al., 1988) consists of 20 items: 10 words describing aspects of positive affect (being interested, excited, strong, enthusiastic, proud, alert, inspired, determined, attentive and active) and 10 words describing negative affect (being distressed, upset, guilty, scared, hostile, irritable, ashamed, nervous, jittery and afraid). Participants were asked to rate on a 5-point Likert scale – ranging from ‘very slightly or not at all’ to ‘extremely’ – how they felt at that moment (i.e. pre WPL-R, post WPL-R). High PA indicates a state of high energy, concentration and pleasurable engagement, while low PA is characterised by sorrow and lethargy. Low NA reflects a state of calmness and serenity, whereas high NA is characterised by subjective distress and unpleasurable engagement. The developers of the PANAS reported the mean score for momentary PA as 29.7 and momentary NA as 14.8 (min–max score 10–50 per scale).
We used the validated Dutch version of the PANAS (Peeters et al., 1996). Cronbach’s alpha was used to describe internal consistency with α = 0.79 for the PA-scale and α = 0.83 for the NA-scale. Norm scores were classified in seven groups from very low ⩽26 to very high ⩾42 for PA and very low ⩽12 to very high ⩾34 for NA. Average scores for PA were classified as 32–34 and as 17–20 for NA (Peeters et al., 1996).
Statistical analysis
We compared women who completed the survey (responders) with women who partially filled in the questionnaires (non-completers). Responders completed all questions about characteristics, the WPL-R, and the PANAS both pre and post WPL-R. When one or more of these questionnaire scales were missing, we regarded the questionnaire as incomplete. We used the Statistical Package for the Social Sciences (SPSS) version 26.0 for analysis (IBM Corp, 2019). Differences in socio-demographic and personal details were examined using T-tests and Kruskal-Wallis H tests, followed by Mann-Whitney U tests when significant differences were found. We performed the study during the COVID-19 pandemic, a time where relationships were affected due to social restrictions. After performing a factor analysis on the WPL-R data obtained in the COVID-19 period, within the original three factors established by Pridham and Chang (1989), we established that 17 of the 25 items could be included for analysis (items 2, 4, 9, 12, 14, 16, 21 and 22 were excluded). Spearman’s rank order correlations were computed to assess the relationship between the remaining 17 WPL-R items and post-Negative Affect scores.
We computed four PANAS score groups based on the PANAS scores before and after filling in the WPL-R: pre-Positive Affect (pre-PA), pre-Negative Affect (pre-NA), post-Positive Affect (post-PA) and post-Negative Affect (post-NA). Cronbach’s alpha ( α ) was calculated to measure internal consistency of each PANAS-scale and the results were considered to be good at α ⩾ 0.8 (Field, 2013). PANAS scores were compared between responders and non-completers using Independent Samples T-tests. The before and after scores of the responders, were compared using Paired Samples T-tests. A value of p < 0.05 was considered statistically significant. Answers to the open-ended question of the WPL-R were read and discussed among authors EB and YK to gain a better understanding of the collected data. We used an unconstrained matrix (Microsoft Word) to organise the data from the open-ended question (Polit and Beck, 2006).
Ethical considerations
This study received ethical clearance from the Medical Research Ethics Committees United (MEC-U) (Protocol Ref No. W20.020, February 2020) and from the Research Center Innovations in Care (Rotterdam University of Applied Sciences). Participation was voluntary and consent for participation and dissemination of the study results was obtained and recorded via box ticking before the questionnaires could be completed.
Results
Of the 216 received questionnaires, a total of 215 women met the inclusion criteria. One questionnaire was excluded because the participant was pregnant when filling in the questionnaire. The questionnaires were completed by 152 women (responders), while 63 questionnaires were incomplete (non-completers). Characteristics of responders and non-completers are presented in Table 1. We observed a difference in education level (H(2) = 9.09, p = 0.011), with more responders showing a high level of education and more non-completers a medium level (U = 3978, Z = −2.98, p = 0.003). Women also differed in their maternity care provider (H(2) = 6.35, p = 0.042), with reported differences in midwife led versus obstetric led care (U = 2974, Z = −1.99, p = 0.046), and in obstetric-led versus shared care (U = 582, Z = −2.22, p = 0.026).
Characteristics of responders and non-completers.
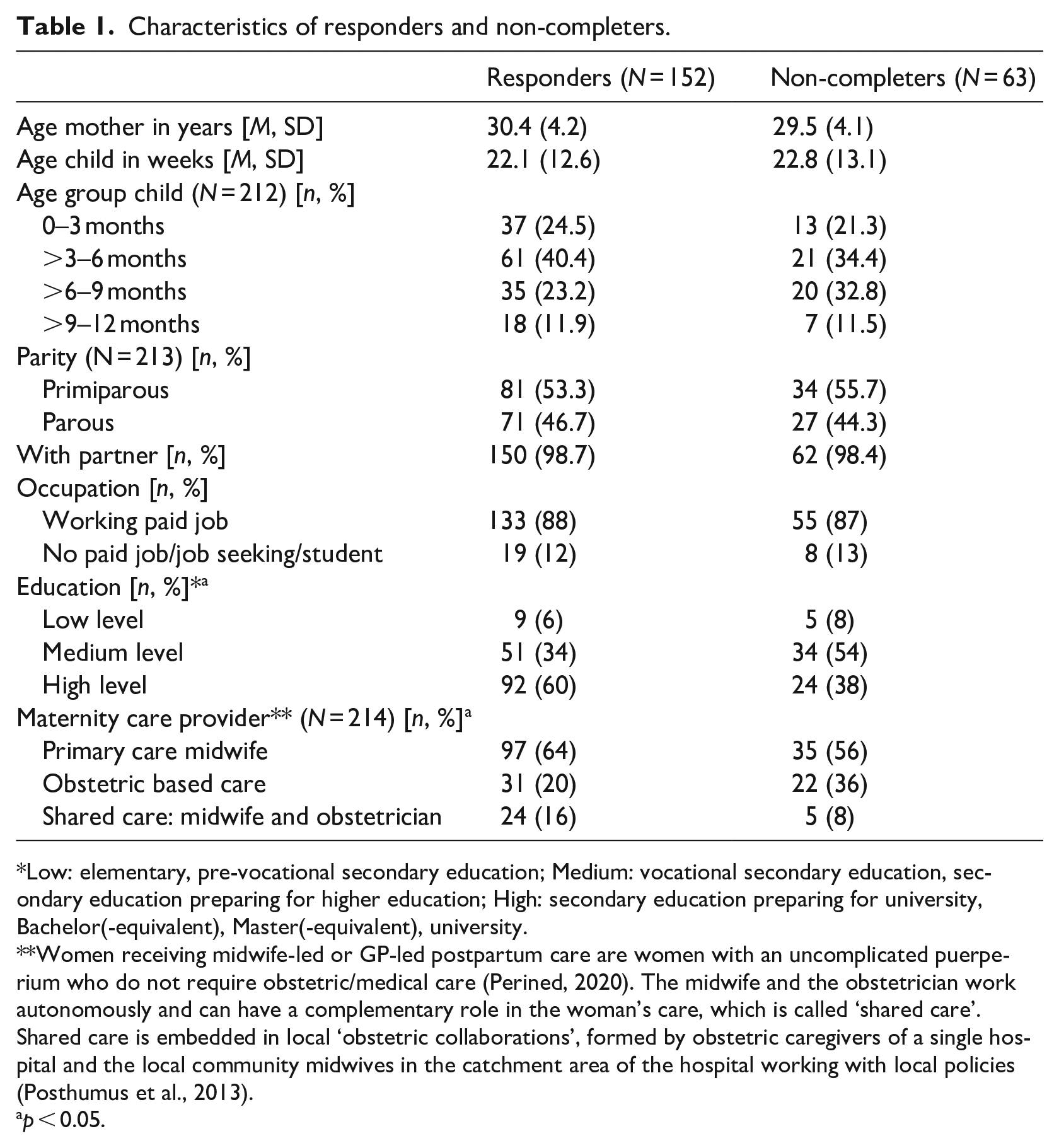
Low: elementary, pre-vocational secondary education; Medium: vocational secondary education, secondary education preparing for higher education; High: secondary education preparing for university, Bachelor(-equivalent), Master(-equivalent), university.
Women receiving midwife-led or GP-led postpartum care are women with an uncomplicated puerperium who do not require obstetric/medical care (Perined, 2020). The midwife and the obstetrician work autonomously and can have a complementary role in the woman’s care, which is called ‘shared care’. Shared care is embedded in local ‘obstetric collaborations’, formed by obstetric caregivers of a single hospital and the local community midwives in the catchment area of the hospital working with local policies (Posthumus et al., 2013).
p < 0.05.
PANAS scores
The Positive Affect (PA) and Negative Affect (NA) scores are presented in Table 2. Internal consistency in our sample was good with Cronbach’s alpha varying from α = 0.87 to α = 0.90. We observed no differences in pre-PA and post-PA scores among the responders. Both pre-PA and pre-NA scores did not differ between responders and non-completers. There was a significant difference between pre-NA and post-NA scores among the responders (t(151) = 6.77, p < 0.001). All PA-scores were above average (classified as 35–37) according to the norm scores, while pre-NA scores were average (classified as 17–20) and post-NA scores were below average (classified as 15–16) (Peeters et al., 1996).
Positive Affect (PA) and Negative Affect (NA) scores for responders and non-completers.
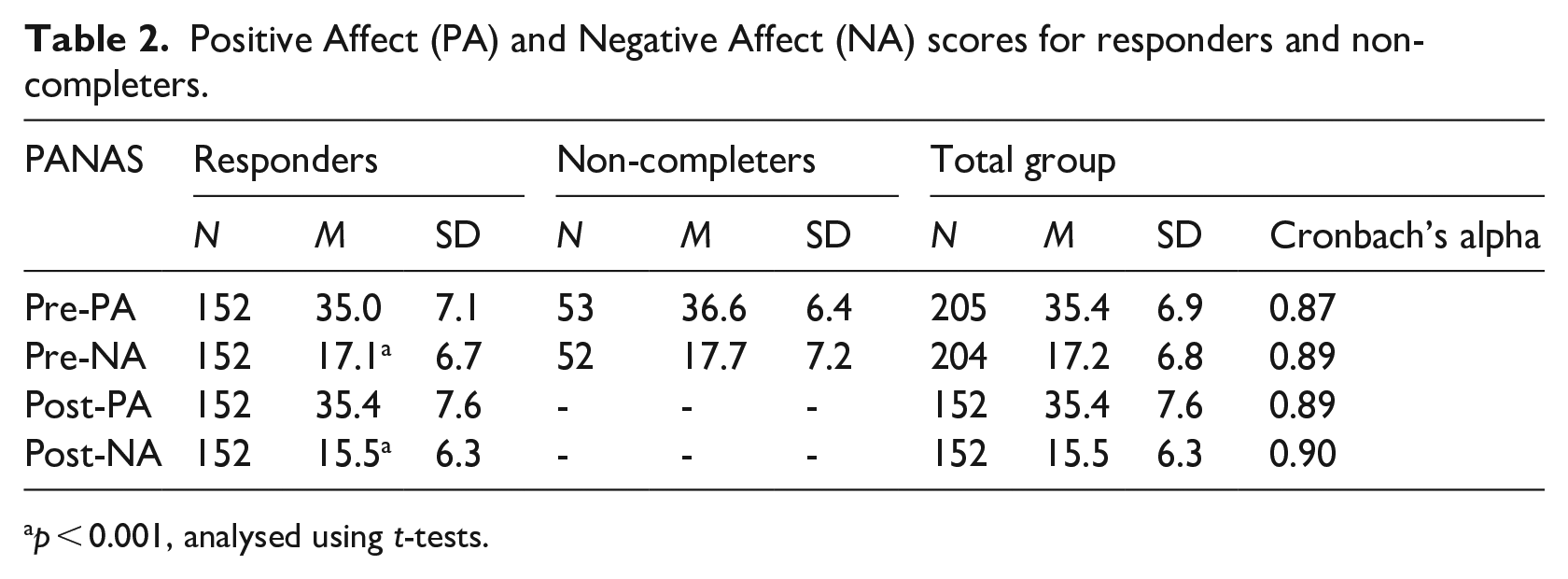
p < 0.001, analysed using t-tests.
WPL-R scores
After obtaining 17 of the 25 original WPL-R items, we used Spearman’s rank order correlation to examine the relationship between the WPL-R items and post-NA scores (Table 3). For seven items there was a negative correlation between the item and post-NA score. For example: a higher score on item 1 (How satisfying has being the parent of a new baby been for you?), correlates with a lower post-NA score, r(150) = −0.21, p < 0.01. Four items were positively correlated to post-NA scores. For example: a higher score on item 10 (On the whole, how stressful is your life, being the parent of a young baby and perhaps having other things to deal with?), correlates with a higher post-NA score, r(150) = 0.47, p < 0.01.
Spearman’s rank correlations between WPL-R items and post-NA scores (n = 152).
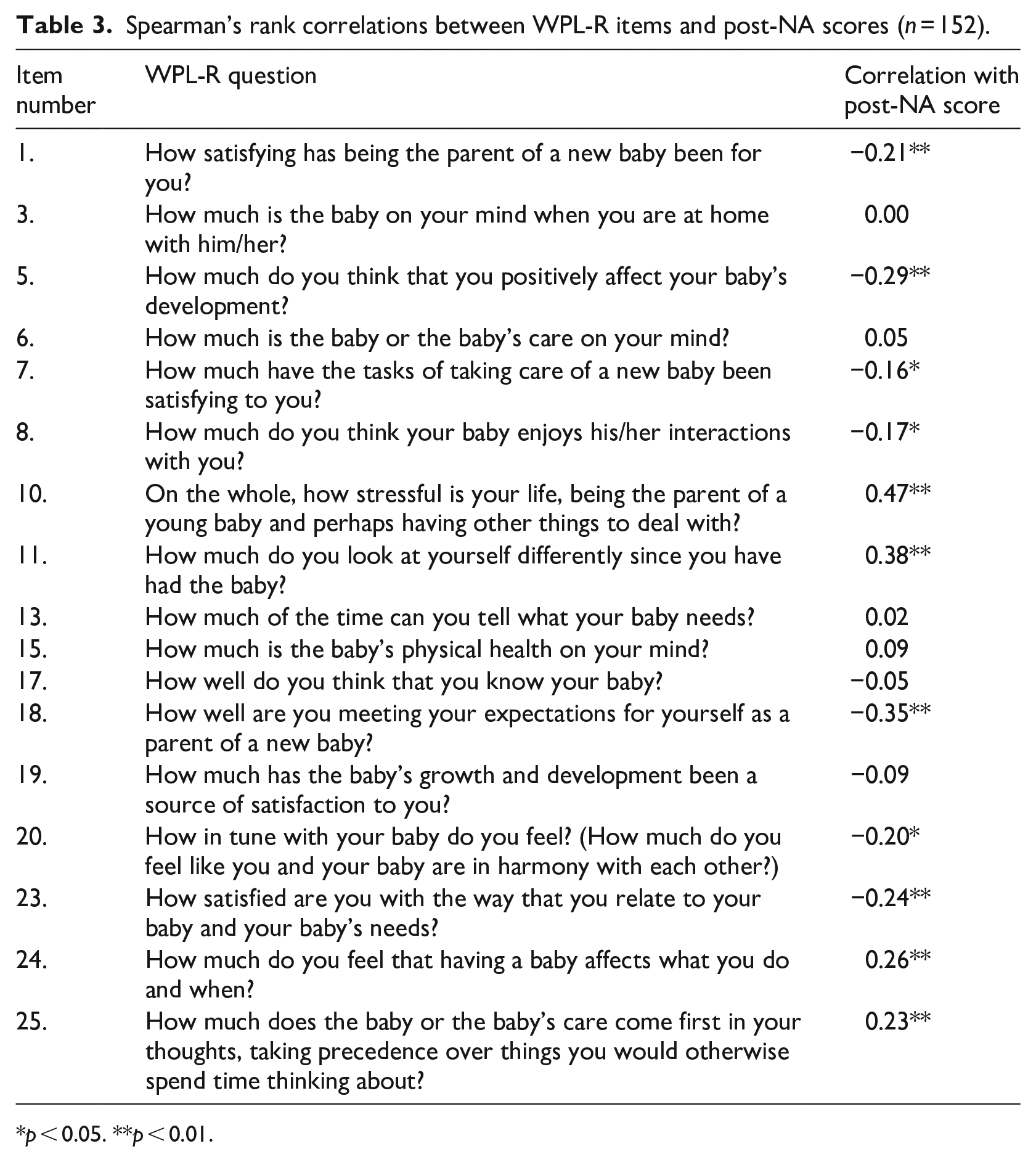
p < 0.05. **p < 0.01.
WPL-R: Open-ended question
The open-ended question of the WPL-R ‘What else do you think is important to help us understand what being the parent of a baby is like for you?’ was answered by 72 women (33%). The following topics were described as having an influence on the experience of motherhood: (a) first versus subsequent child (parity); (b) health and temperament of the child; (c) getting to know your baby takes time; (d) you can’t prepare for motherhood but must experience it yourself to understand what it is like; (e) (lack of) sleep; and (f) achieving a new balance in the family and in life. Women also mentioned the influence the restrictions related to the COVID-19 pandemic had on their answers, for example to questions about their relationships with extended family or leaving their child with someone else than their partner. The answers given were not representative of how they would have responded without COVID-19 restrictions.
Discussion
To our knowledge, this is the first study exploring the possible intrusive or harmful effect of completing the WPL-R on positive or negative affect of postpartum women. Our results suggest that positive affect (PA) does not change while completing the WPL-R, but negative affect (NA) declines significantly after completing the questionnaire. Fortunately, in our case, the WPL-R did not have a negative or harmful effect on maternal affect, but that does not absolve us from the obligation to consider the potential effect of the WPL-R from the standpoint of the participants in our research. Moreover, this is an issue for researchers to consider or to examine when administrating questionnaires of a sensitive nature, for example, questionnaires aiming to examine psychosocial wellbeing. The Code of Human Research Ethics and Conduct of The British Psychological Society (2014) defines harm as potential physical or psychological harm, discomfort or stress to human participants, including personal beliefs, relationships and/or disclosing deviant behaviour. Some of these elements are included in the WPL-R, such as item 1 and 10 which ask about satisfaction and life stress. However, when the risk of harm is not greater than encountered in day-to-day life, no measures are required to obviate, minimise or manage the risks of harm (The British Psychological Society, 2014). In our study the WPL-R measures exactly that, the day-to-day life of a woman being a mother. Although our study was exploratory in nature and had a small sample size, our results indicate that by completing the WPL-R items women are not exposed to harm. The PANAS showed a decrease in negative affect after completing the survey. Future research including a larger sample of women is needed to confirm our explorative findings.
Our results suggest that women do not become more positive about being a mother after filling in the WPL-R, but they do become less negative. Reflecting on one’s quality of mothering may thus have a positive effect by reducing negative affect. This in itself is a positive observation; the alteration in maternal affect suggests that completing the WPL-R can serve as a form of personal awareness, reflection, or evaluation for new mothers, in particular, because the negative correlations between WPL-R items and NA scores are related to the evaluation subscale of the WPL-R (Pridham and Chang, 1989). The positive alteration in maternal affect might even indicate the questionnaire functions as a screening, intervention or therapeutic measure for maternal self-perception or evaluation. This possibility is important especially in times of constant comparison of oneself with picture-perfect parents on social media, which can lead to role overload and lower levels of perceived parental competence (Coyne et al., 2017). Parents experience a culture of comparison, competition and judgement which can be harmful to their emotional wellbeing but might be mitigated by the application of critical reflection (Sanders et al., 2021). Self-evaluation could provide helpful reflection for mothers, in our case a positive confirmation of satisfaction (Pridham and Chang, 1989).
The positive correlations between WPL-R items and NA scores are related to the WPL-R items about stressfulness of life, self-image and ‘putting the baby first’. These elements are part of the transition to motherhood (Prinds et al., 2014). Our results indicate that these experiences require the attention of healthcare professionals whilst being involved in the care of mothers and infants. Evidence suggests that discussing motherhood in terms of meaningfulness, manageability and comprehensibility is an adequate way of helping women understand what being the mother of a baby is like (Van Den Branden et al., 2022). Additionally, using the WPL-R in practice, either as an evaluation or screening tool, can benefit mothers themselves, but it can also be of merit for healthcare practitioners to use the WPL-R scores as a tool for starting a dialogue.
Using the WPL-R to support discussion with mothers about what being the mother of a baby is like needs a sensitive, knowledgeable and responsive clinician as mothers’ answers to the WPL-R items could otherwise result in labelling or categorisation of mothers (The British Psychological Society, 2014). The use of the WPL-R in practice requires education and adequate communication and coaching skills of professionals. It is unethical to not have the necessary skills and qualifications required when asking sensitive questions concerning emotive topics (Crowther and Lloyd-Williams, 2012). Additionally, when maternal responses to the WPL-R items indicate therapeutic interventions seem necessary, the healthcare professional needs to ensure that adequate help and support is available and accessible. This is relevant and important for midwives, because it is known that when there is a lack of follow-on care midwives do not discuss complex personal issues with women (Fontein-Kuipers et al., 2014).
Limitations and future research
We measured momentary affect using the PANAS, establishing the short-term effect of the WPL-R. We do not know whether participants experienced lasting effects or prolonged personal discomfort. It could very well be that a mother’s perception of her efficacy or competence in performing mothering function, altered in a negative direction after completing the WPL-R, remained persistent in negative affect or thought. We should consider whether using the WPL-R is legitimate if long-term negative self-perception or discomfort might occur. In order to explore this, longitudinal research is recommended. Another limitation is that the PANAS deals only with affect. Another consideration in use of the WPL-R is the support a mother might need to bolster her evaluation of herself in respect to the quality of her mothering and her adaptation to mothering her infant. We did not exclude mothers with premature children or children with health issues.
The WPL-R may need modification in its construction, delivery and analysis to take into account the age of the baby, the kind of temperament the baby has, how much sleep the mother has been getting, how much support from family members she is getting, and how balanced mothering the baby and family life is. In addition, we need to consider whether all items of the questionnaire are suitable to be asked during times of the COVID-19 pandemic, as some of the questions (e.g. regarding support from family members) were reported by mothers to have been answered differently due to COVID-19 restrictions. This may have influenced the cultural and time appropriateness and sensitiveness of the questionnaire to mothers’ true feelings. The WPL-R would be more useful if responses could be compared to normative values. It is therefore recommended to repeat this study when COVID-19 has waned, or to repeat the study including COVID-19 questions to potentially adjust for the WPL-R scores.
We observed differences between our responders and non-completers. Compared to the non-completers, our responders had higher levels of education and were more likely to have received primary midwifery care, implying they were healthy postpartum pregnant women (De Boer et al., 2008). The self-selective nature of our recruitment strategies might have led to selection bias, affecting the generalisability of the findings. It could also be that, for example, health and temperament of the child (lack of) sleep and the child’s age may have affected our results. The sample size was too small to perform subgroup analysis to establish the effect of these variables. We recommend repeating the study with a larger sample of postpartum women and to examine possible associations.
Conclusion
Although we found a positive change (the decline in negative affect) for responders in PANAS scores after completion of the WPL-R, the changes in affect might imply an intervening effect when using questionnaires such as the WPL-R in research. This raises the question of acceptability of use of questionnaires with postpartum women without any knowledge of the possible effect it may have, even when an ethics committee approves the study and considers the measure to be non-invasive. Further research is needed to explore and confirm our findings.
Footnotes
Acknowledgements
We would like to thank Dr. Vicki Erasmus for her work on the translation of the WPL-R and VAR midwifery students for their assistance in collecting the data.
Data availability statement
The dataset generated and analysed during the current study is available from the corresponding author on reasonable request.
Funding
All articles in Research Ethics are published as open access. There are no submission charges and no Article Processing Charges as these are fully funded by institutions through Knowledge Unlatched, resulting in no direct charge to authors. For more information about Knowledge Unlatched please see here: ![]() .
.