
Abstract
In medical research, patients are increasingly recognized with ‘lay knowledge’ but their views are poorly researched. The study objective was to investigate patients’ attitudes to medical research. This is in comparison to lay and expert members on ethical review boards (ERB), as their task is to evaluate the risk−benefits of research, which are ultimately grounded in attitudes and values. From focus-group interviews with patients suffering from chronic inflammatory diseases, a postal questionnaire was developed and sent to patient members of the Swedish Rheumatism Association (n = 1195) and to all ERB board members in Sweden (N = 583). Response rates were 65 percent and the surveys were conducted in Jan−May 2011. Agreement across the groups included priority for medical research on diagnostic and early detection of disease. A key difference was expert and lay ERB members giving higher priority to basic research/research on lifestyle and prevention (primarily benefiting future patients), whereas patients prioritized research on daily function. On this significant point, lay members did not share the opinion of this patient group, indicating that they may be poor representatives for patients’ views. These results call for further research: how can patient perspectives be included in ERB discussions and in what way should patients’ values influence the research agenda.
Introduction
Patients are multiple stakeholders in medical research, primarily as end-consumers of medical care and sometimes as research participants. According to EU regulation, a competent body must assess research involving persons, both on the importance of aim and that any risks stand in proportion to potential benefits (Council of Europe, 1996: article 16). In Sweden this work is performed by ethical review boards (ERBs), where each regional ERB consists of ten members with scientific expertise, five members representing the interests of the general population and one chairman. Patients’ attitudes to medical research in this context are important for two reasons: (i) if the research agenda does not reflect or address priorities made by patients, there can be a mismatch between the needs of legitimate stakeholders and the direction of scientific research; (ii) if ERBs are unaware of patients’ values and priorities for research, the risk−benefit evaluation may not reflect what patients, as research participants, would deem as acceptable risks in relation to the research aim.
A novel way for patients to influence medical science is as research partners, defined as ‘persons with a relevant disease who operate as active research team members on an equal basis with professional researchers, adding the benefit of their experiential knowledge to any phase of the project’ (De Wit et al., 2011). The particular clinical trial can benefit from patient participation, but if future research priorities are decided without the input of patients and clinicians, the end product of research may be sub-optimal to the patient, e.g. mismatch in research on osteoarthritis (Tallon et al., 2000) and improved research outcomes for urinary incontinence after consultations (Buckley et al., 2010).
For patients suffering from chronic inflammatory diseases, priorities within research are particularly relevant given that these diseases are complex, meaning that the disease is caused by multiple genetic, environmental and lifestyle factors. The novel biological agents have been a great success to control the disease for a proportion of patients, but multiple approaches are necessary for these patients, who may meet specialists in, for example, rheumatology, physiotherapy, surgery and occupational therapy.
In order to gain deeper knowledge of public understanding of science, general surveys on attitudes to science are increasingly replaced by studies on more specific areas, e.g. biotechnology (Bates et al., 2005; Pardo et al., 2002; Sturgis et al., 2005). Similarly, the general public is broken down to more specific groups where for some, such as patients, the division of lay and expert knowledge may dissolve (Cunningham-Burley, 2006; Dixon-Woods et al., 2008; Yearley, 2000). In our background research for this work, we noted that little was known about patients’ priorities in medical research and about the (perceived) relationship between patients and researchers, despite patients being direct stakeholders in medical research. Although the necessity of communication between the public and the scientific community is recognized, there is little evidence that the latter is listening or is open to self-critique (Felt et al., 2009; Wynne, 2006). It may be argued that, as lay persons serve as members on ERBs, they provide this non-expert perspective on the ethical evaluation. However, there are no clear guidelines in Sweden for who qualifies to be a lay representative, and there is probably great variation on this point between countries. In the UK there are strict instructions for who can serve as scientific experts, so-called lay+ and lay representatives (NHS, 2009). According to the NHS guidelines, some of the lay representatives in Swedish ERBs would be disqualified on the basis of their self-reported occupations within health care services, such as nurse, midwife or physician (www.epn.se). This state of affairs may in part be explained by the fact that it is the county council − which runs the regional health care services − that recruits suitable persons to serve as lay representatives (pers. comm. registrar at ERB). The aim of this study was to explore patients’ attitudes to medical research and, in comparison to, attitudes held by members on ERBs. The project was conducted in close collaboration with the Swedish Rheumatism Association 1 (SRA) and included two research partners.
This article addresses how patients’ attitudes differ from those of lay representatives and scientific experts on the topics of:
priorities in medical research
patient involvement in research projects.
Abbreviations
ERBexpert: members with scientific expertise serving on the ethical review board
ERBlay: chairmen and representatives of lay interests serving on the ethical review board
SRA: members of the Swedish Rheumatism Association.
Methods
A postal questionnaire was sent to patients (identified through the SRA) and to all members of ERBs for research on human subjects in Sweden. The questionnaire was based on results from three focus groups with the patient group (conducted during 2009) and contained questions on priorities in medical research, motives of researchers and animal testing (reported elsewhere). Two research partners from the SRA were involved in the focus groups (preparation, execution and analysis) and the development of the questionnaire. They provided a patient perspective throughout the project, with the intention to ensure relevance to the patient group.
A random sample of 1200 individuals with chronic inflammatory disease 2 was chosen from the member register of the SRA, 3 and the questionnaire was posted in January 2011, with two reminders including the questionnaire. Five individuals were excluded (one minor, two deceased, one self-reported support member and one double posting in the register), leaving a total of 1195 individuals.
The ERBs are located in six cities in Sweden: Gothenburg, Linköping, Lund, Stockholm, Umeå and Uppsala. There are 12 ERBs for medical research, six ERBs for other research and one central ERB for cases of appeal. An adapted questionnaire in terms of background information was posted to all 586 members (regular and alternate members) of Sweden’s ERBs (April 2011), with two reminders including the questionnaire. A total of 583 individuals were included in the study after three participants were eliminated (two deceased and one failure of delivery).
Patients with chronic inflammatory disease were selected because of their on-average long-term experience of health care, and it is a group that is often offered to participate in research. The ERBs were selected because of their task of protecting human subjects in research, and lay representatives in particular are included to safeguard other values than scientific advancement for human subjects in research. It is therefore of relevance to investigate the attitudes within the ERBs and how these reflect the attitudes of patients.
The data were analysed using SPSS (Statistical Package for the Social Sciences), version 19.0. Independent ANOVA and chi-squared comparison of means were used to analyse differences between groups, and Bonferroni analysis was used as post-hoc test. Significance level was set at a two-tailed p < 0.05.
Results
The response rates of the SRA and the ERB respondents were 65.2 percent and 65.0 percent, respectively. There were no statistically significant differences at the 5 percent level between respondents and non-respondents in terms of gender for any of the study groups or in terms of medical or non-medical ERBs.
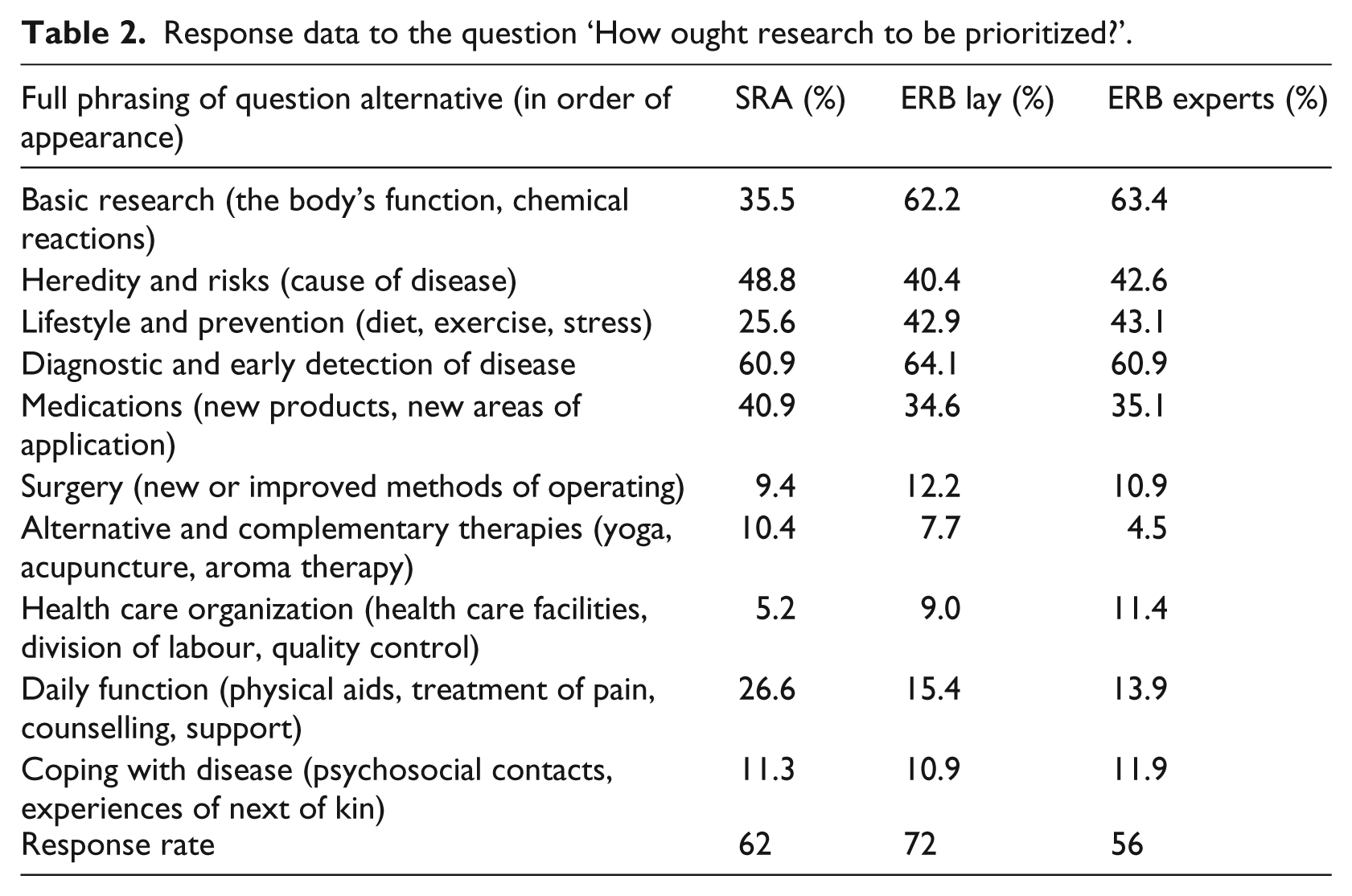
The majority of the SRA study population were women (reflecting the gender bias in disease load), and the mean age was 63.2 ± 11.8 years (Table 1). The most frequent diagnoses of respondents were rheumatoid arthritis (30%), fibromyalgia (20%) and Bechterew’s disease (10%), but also included polymyaliga rheumatic (PMR), psoriatic arthritis, Sjögren’s syndrome, systemic lupus erythematosus (SLE) and vasculities. The self-reported state of health was generally poor (mean of 3.78 ± 0.76 on a Likert scale, where 1 = excellent health and 5 = poor health). The mean age was high in both study populations, and a large proportion of the ERB respondents had served on the board for more than five years and a majority of SRA respondents had had their diagnosis for more than five years (Table 1). On the question of ‘How ought research to be prioritized?’, respondents could choose a maximum of three alternatives that they held to be areas of research that should be promoted (see Table 2 for full phrasing of question alternatives and response rates). Diagnostic and early detection of disease was a high priority to all groups, whereas heredity and risk were rated high by SRA and ERBexpert respondents. ERBexpert and ERBlay respondents agreed on giving priority to basic research and lifestyle and prevention, whereas SRA respondents were more likely to prioritize medications. There were statistically significant differences between the priorities of SRA to the members of ERB on basic research, lifestyle and prevention, and daily function.
Background data of respondents.

Response data to the question ‘How ought research to be prioritized?’.
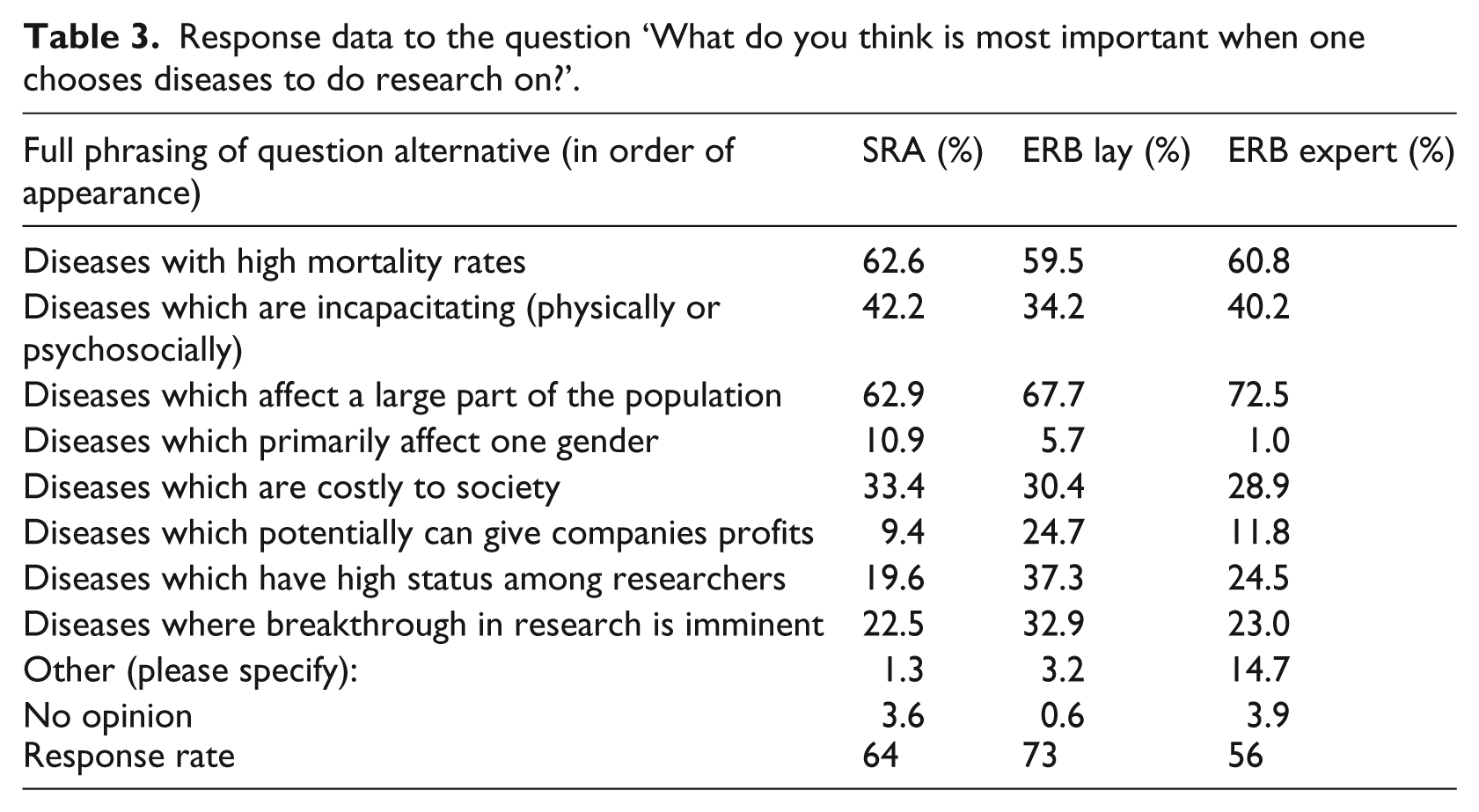
A maximum of three response alternatives could be chosen for the question ‘What do you think is most important when one chooses diseases to do research on?’ (see Table 3 for full phrasing of question alternatives). There was agreement across the groups on a number of aspects, particularly diseases which affect many people in society and diseases with high fatality rate, but also for diseases which involve incapacity and diseases incurring high costs to society. Compared to ERBexpert and SRA, ERBlay gave a considerably higher priority to diseases where research breakthrough is likely, diseases that have high status among researchers, and if the research results are potentially profitable. On these three alternatives the differences in opinion by ERBlay were tested against those of SRA respondents, and all were statistically significant. The SRA respondents believed to a higher degree that gender bias in the disease load was a factor that could influence which disease to study. The ERBexpert respondents more frequently gave other reasons than the given alternatives, which included responses such as chance, existing research at the hospital/university, where funding was most likely to be secured, and possibility to make a difference (e.g. in terms of treatment options).
Response data to the question ‘What do you think is most important when one chooses diseases to do research on?’.
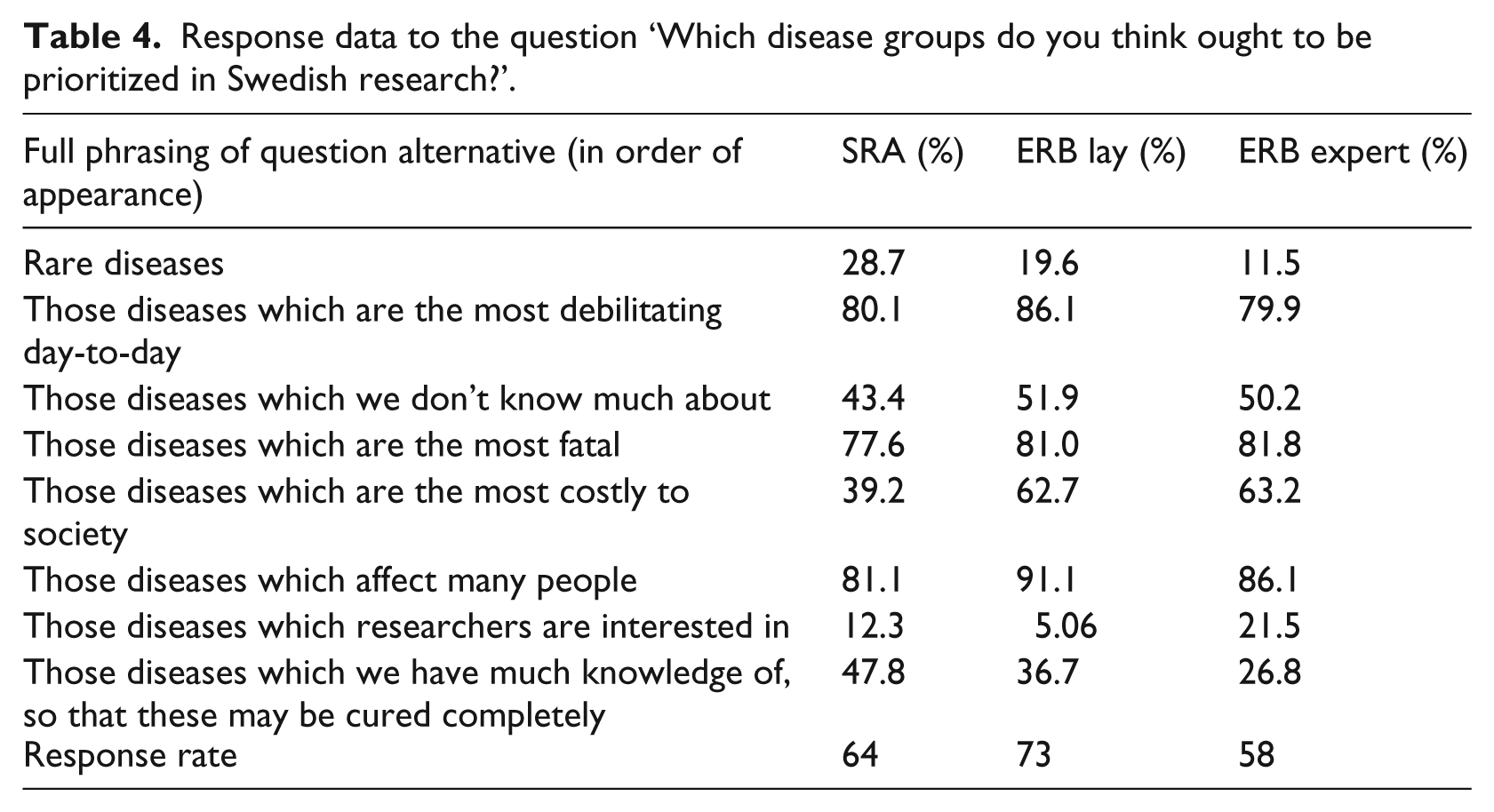
Respondents were asked to give high or low priority to disease groups to the following question: ‘Which disease groups do you think ought to be prioritized in Swedish research?’ (see Table 4 for the disease groups). Presented here is how many of the total number of respondents rated an alternative as a high priority. There was agreement across the groups for the top three priorities: number of affected patients, debilitating diseases, and diseases with high mortality rates. Of medium priority to the SRA respondents were: (i) diseases where there is hope for a cure; (ii) so far unexplored diseases; and (iii) high cost to society. In contrast, both ERB groups had the same priority list but in reverse. On the alternatives of diseases with hope of cure and disease with high costs, there were statistically significant differences between the SRA and the ERBexpert and the ERBlay.
Response data to the question ‘Which disease groups do you think ought to be prioritized in Swedish research?’.
The response rates for the following statements ranged between 57 percent and 70 percent (Table 5). SRA respondents had statistically significant different means on all statements compared to either one or both groups in the ERBs, whereas no significant differences were found in the replies within the ERBs. A majority in all groups tended to agree that there is more research on some diseases than others, which leads to injustices in Sweden (Table 5). The SRA respondents were more likely to agree, whereas the ERBlay respondents only had a slight tendency to agree with the statement (statistically significant). There was consensus across the three groups that medical research tends to benefit patients, but the SRA respondents were less convinced compared with the ERB respondents. Statistically significant differences were confirmed in the replies by SRA compared to ERBexpert and ERBlay.
Response data on views on patient participation.
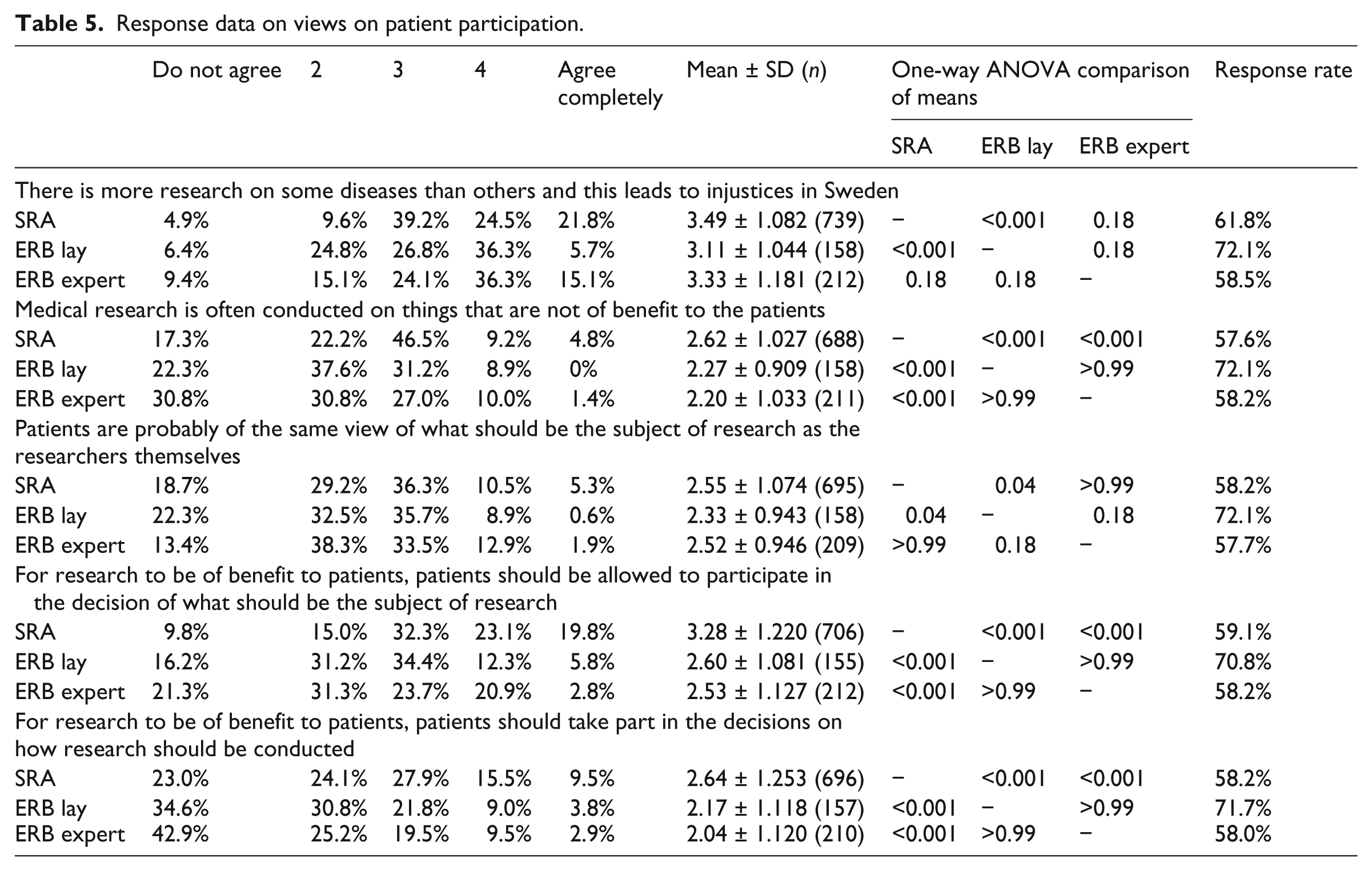
A majority of respondents tended to agree that patients and researchers have different views on what should be the subject of research. Lay representatives held a stronger belief in this difference of opinions, whereas patients and researchers only tended to agree. The ERBlay response was statistically significantly different from the responses of SRA and ERBexpert. Although all groups agreed that patients and researchers had different views on what should be the subject of research, it was only patient respondents who were positive about patient involvement in the research process. Researchers and lay representatives in ERB tended to disagree that research could be made more beneficial to patients if patients could be involved in deciding what should be the subject of research. In contrast, there was general agreement that patients should not participate in the decision of how research should be conducted, but members of ERBs were more negative than patients, and differences were statistically significant for SRA respondents compared to both ERBlay and ERBexpert.
Discussion
The role of patients in research is changing, and the concept of ‘lay knowledge’ or ‘lay expertise’ is both applied (Griffiths et al., 2007) and critiqued (Prior, 2003) in the scientific literature. This study indicates that patients believe that their perspective can contribute to making research more relevant to the end-consumer, i.e. themselves. Most of the differences between patients and members of ERBs were in the strength of response rather than opposing attitudes, but it is consistent with previous findings that researchers are less persuaded about the benefits of research partners in the process of research (De Wit et al., 2011). Lay representatives were convinced of a difference in opinion between patients and researchers to a greater extent than patients and scientific experts themselves believed there to be. This study shows that neither lay representatives nor researchers in ERBs shared the attitudes of this patient group on some core issues, and that ERB respondents, including lay representatives, were generally sceptical about patient participation as research partners. Only careful evaluation of projects with research partners can show if, when and how patient experience can contribute to making research more relevant to the intended group, but unless researchers believe that it can be beneficial to communicate with patients, there can be no true co-operation. Our results indicate that researchers need to be aware of their own critical position toward research partners if a patient is to ‘operate […] on an equal basis with professional researchers’ (De Wit et al., 2011), and these researchers need to be open to critique (Felt et al., 2009). Obviously, if patient research partners are included purely for window-dressing purposes, that is a waste of resources for everyone involved.
The relatively new formation of ERBs can be seen as one arena where questions in biology and medicine are discussed with members of the public (Council of Europe, 1996: article 28). The constitutions of ERBs vary, but the Swedish system is comparable to the British NHS Research Ethics Committee, where one-third of the board members are lay representatives (Dyer, 2004; NHS, 2009). In the EU directive on ethics committees, a significant reason for lay representation is public representation (2001/20/EC), indicating that they provide an outsider perspective − someone without personal investment in the pursuit of science and who remains critical to possible sacrifices. This description suggests that lay representatives have a role as potential whistle-blowers and as important observers of the system. That lay representatives serve to contextualize the scientific discussions to social and moral values fits Dyer’s model of ‘extra-scientific public participation’ (Dyer, 2004). The Government proposition 2002/03:50 to the Swedish law 2003:460 highlights that ‘[t]he point of reference must be respect for the research participant’s or the patient’s values, since the person who risks being harmed also is the one to make a final evaluation. To weigh the risks for the research participants against the benefits of doing the research here become central.’ (Swedish Ministry of Education and Research, 2002: 39; authors’ translation).
The underlying assumption for the need of lay representatives is that science and society have different goals, with different and possibly conflicting values (Allen and Waters, 1983). The validity of this assumption can be questioned, especially in relation to different sections of the public. In an interview study with families with a child afflicted by childhood cancer on perceptions of biomedical practice, there was a strong view of shared values and research goals (Dixon-Woods et al., 2008). Instead of the patients and their next-of-kin experiencing being separate from the medical world, they thought of themselves and the medical staff as being part of the ‘childhood cancer community’. Our results show a great degree of consensus for the top priorities in medical research (prioritizing diseases that affect a large number in the population, diseases that cause incapacity, or diseases with high rates of fatality). However, there were also areas where attitudes differed, which call for debate. Of course there may be bias among researchers and affected parties (including affected patients) to approve projects, and an important role of lay representatives may be to ‘[check] the natural enthusiasm of doctors’ (Allen and Waters, 1983: 64), but that role is more about having an unbiased position and a dispassionate perspective rather than to represent ‘the social values’. In a study on parents’ willingness to allow their child to participate in research, that independent role was found in the attending physician whose aid parents highly valued in estimating risks and benefits for their child (Rodriguez et al., 2006). The trend to involve the public in decision-making at different levels may not be what the public wants, partly because of their (perceived) lack of knowledge. In a study by Litva et al. (2002), interviewed citizens wanted to be heard, for the process to be open and that decisions could be adequately explained, but they did not want to be co-responsible for the decisions. The risk is that lay representatives, who by definition do not have scientific expertise, serve a symbolic role on ERBs owing to the framing of the discussion in scientific terms combined with a ‘desire for consensus’ (Ideland, 2009).
Given the emphasis in medical ethics on the priority of the individual over societal or scientific goals (Council of Europe, 1996), it is surprising how negative the ERB as a whole, and lay members in particular, are in this study to patients having increased opportunity to influence the research agenda. Our results indicate that the lay representatives are poor representatives for this patient group and that patients and ERBs seem to be at odds on significant points, e.g. on patient participation in research. As only the attitudes of one patient group have been included in this survey, it is not yet possible to draw any general conclusion on possible congruent or incongruent views between lay representatives and the many patient groups. However, there is no obvious reason for why the high priority of ‘research on daily function’ would be a specific interest of this particular patient group as opposed to a general interest of many patients. Additionally, the reluctance of lay representatives to support patient participation in research calls for further investigation. One possible reason may be that lay representatives exaggerate the differences in opinions between researchers and patients and therefore do not think that co-operation would function. Another possible reason is that ERBs are not up-to-date on how patient research partners have improved research. Either way, the question arises on how ERBs can include patient perspectives, which they must, as it is the task of ERBs to protect patients and healthy volunteers in medical research and to ensure that the risks stand in proportion to the expected scientific benefits. It is of moral significance when the end-consumers of research hold a different view of what constitute scientific benefits from those doing the risk−benefit analysis.
Conclusion
Overall, there were shared core values between patients and members on ERBs for priorities in medical research, but with some important points of differences. One difference, relevant for the research agenda, is the stronger focus among the medical community and non-patients to prioritize research that is either of benefit to future patients or reduces costs for society. In contrast, patients prioritized research to relieve suffering for now-living patients. Another difference is that patients were alone in seeing the benefits of patients as research partners, and lay representatives were poor advocates for the patient perspective in this instance.
This calls for clarification of the role for lay representatives and how patient perspectives can be included in the work of ERBs. The question for the scientific community in general is if, when and how patient perspectives should influence medical research, whether for the individual research project or in setting the research agenda.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.