
Abstract
Poor nutrition habits have been reported in the childcare setting. While the literature advocates the need to carry out ‘Voice of the Child’ research, few studies have explored this methodology with regard to children and food, in particular in the pre-school setting. This article aims to outline the ethical issues raised by a research ethics committee and to discuss the impact of these issues on a study that hoped to determine the food perceptions of children (aged three to four years) within an ongoing nutrition and lifestyle pre-school project in Ireland. Ethical approval was granted for this study but only upon the clarification of two aspects: that only hedonic symbols previously used in the literature could be included in the study; and that parental consent be obtained from both parents of each child. Children were shown food pictures and asked to use the hedonic symbols to answer questions posed to them on the food. Owing to the ethical constraints imposed by the requirement for two-parent consent, seven children, from a potential sample of 85, were eligible to partake in the study. These children did not seem to understand the hedonic symbols recommended for use by the ethics committee, therefore preventing the collection of in-depth qualitative data. The ethical constraints placed on this study impacted on both its design and its methodology and are discussed in relation to national and international ethical guidance and legislation. Future research with children regarding food choice must balance the need for strict ethical standards with the need to explore children’s views on this subject.
Keywords
Introduction
Children have traditionally been viewed as the objects of research, with research being carried out on, rather than with them (Neill, 2010). Grover (2004) states that the strength of research will be affected if children are not participants in a process which allows them to tell their story. In recent times, children have been noted to be ‘active beings’; however, this does not always seem to translate into action research (Balen et al., 2006). The last decade has seen an increase in the literature highlighting the need for ‘Voice of the Child’ (VOC) research (Greene and Hogan, 2005). A policy document submitted to the Minister for Children by the National Children’s Advisory Council in Ireland (2010) noted that ‘the voices of younger children were not being heard’ and that ‘different methodologies must be explored and utilized to hear the voices of young children’.
In an editorial on medical research involving children, Gevers (2008) noted that while it is agreed that children need to be protected in a research situation, there are concerns that if regulation is too tight, this may prevent health research, that may be in their interest in the long term, taking place. In a review of the literature, Dixon-Woods et al. (2006) advocated an urgent need for social science study of children’s participation in research to inform legal and ethical frameworks.
In preparation for direct research with children, submissions for ethical approval are made to research ethics committees (RECs). These committees have a number of roles: the discouragement of unethical research; the provision of a public affirmation of ethical integrity for researchers, and the enhancement of sensitivity to ethical issues in research (Angell et al., 2007). While RECs are now evident in many health care settings to regulate and ensure ethical research; few sociologists have chosen them as a study option (Dixon-Woods et al., 2007).
The aim of this article is to outline the ethical issues raised by a REC, and discuss the impact of these issues on a study that hoped to determine the food perceptions of children (aged three to four years), within an ongoing nutrition and lifestyle pre-school project in Ireland.
Determination of the Voice of the Child in the HIP project
While many children are now cared for outside the home, inadequate nutrition practices in pre-schools have been reported (Benjamin et al., 2007; Jennings et al., 2011; Johnston Molloy et al., 2011). The Healthy Incentive for Pre-schools (HIP) Project is ongoing in the Midlands of Ireland and aims to develop an intervention scheme to incentivize pre-schools to improve their nutrition and health practices. With the interest and calls for VOC research from the literature (Grover, 2004), the National Advisory Group for the HIP project recommended an investigation to provide insight into children’s perception of food.
In preparation for direct research with children on the topic of food preference, a pre-study exercise was carried out to determine how best to capture the opinions young children have about food. To this end, two different symbolic systems were examined. This indicated that children seemed to understand a set of three smiley hedonic symbols from Microsoft Clip Art, correctly identifying the smiley symbols. However, when presented with a set of five facial hedonic symbols, described by Chen et al. (1996), they had difficulty explaining the meaning of the different symbols.
REC ethical constraints on project work
Ethical approval for the VOC study was sought from the research ethics committee of the Health Service Executive Dublin Mid-Leinster, and the Ethics Committee of the Dublin Institute of Technology, Ireland. While ethical approval was granted by the research ethics committee of the academic institution, the health services research ethics committee noted that ethical approval would only be granted if two conditions were met: firstly, that only a specific set of hedonic symbols from the literature could be used (Chen et al., 1996); and secondly, that parental consent was obtained from both parents of each child that was to take part in the process. Co-ordination between dual ethics committees at a management level may have prevented this variance in approval from occurring; however, there was no co-ordination in place and, therefore, the research dietitian believed she could only proceed with the research by following all the conditions laid down by both committees. The stipulations imposed on the researcher, however, impinged on both the design and methodology of the present study.
Ethical conditions and effect on study sample
HIP project pre-schools that had been visited previously by the researcher (n = 48) were excluded from the sampling process as such visits may have had an influence on practice and children’s views in these settings. The remaining pre-schools (n = 15) were divided according to the number of full day care children attending and their deprivation score (Small Area Health Research Unit, 2009). Each service identified in the sampling process was contacted by telephone. A verbal explanation of the VOC process was detailed. Settings were advised that, informed pre-school manager, and informed two-parent consent would be necessary. Information and consent forms were sent to each pre-school manager at least one month prior to the arranged visit date. A follow-up telephone call was made to each manager just prior to the scheduled visit to confirm visit details and ensure that parental consent had been obtained.
Nine of 15 pre-schools (n = 85 children, aged three to four years) agreed to take part in this element of the overall study. It became apparent upon attending each pre-school to carry out the VOC work, that pre-schools had experienced difficulty in collecting consent from both parents of each prospective child. Table 1 outlines the numbers of children and consent for the present study.
Number of pre-schools and parental consent
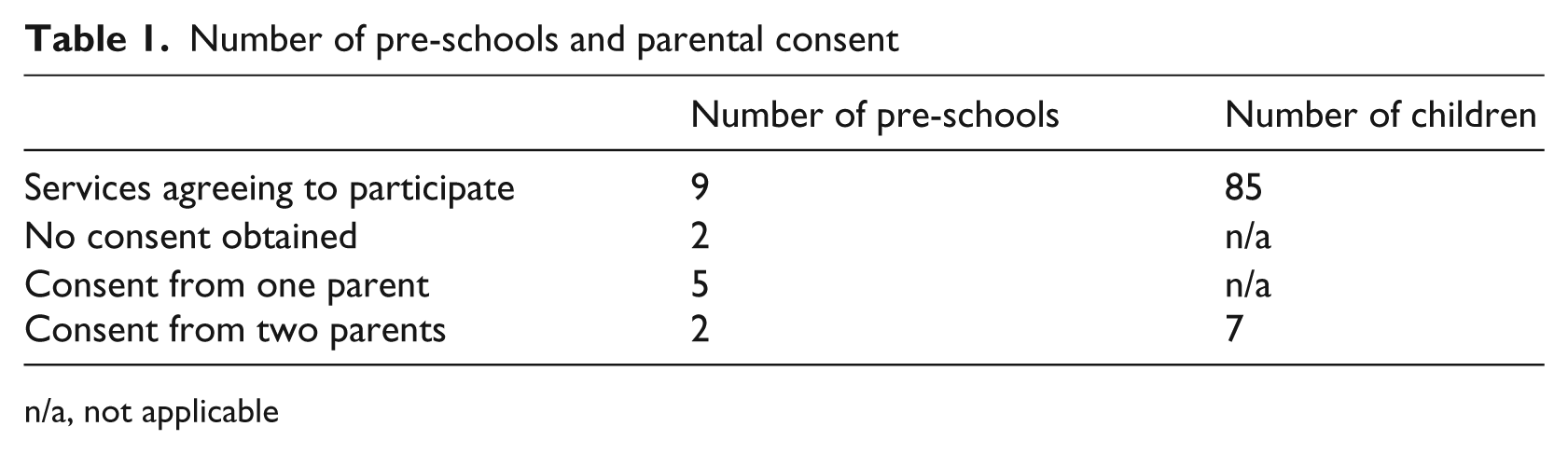
n/a, not applicable
In hindsight one may hypothesize as to why ‘two-parent consent’ was required by the health service REC; there may have been a number of factors that influenced this decision. The possible reasons for this will now be outlined.
Firstly, although it would not be possible to know the actual membership representation of the REC at the time of the study ethical application, the Research Ethics Review Guideline (Health Service Executive Midlands Area, 2012) notes that the REC should include: hospital physicians; hospital and community nursing staff; hospital and community senior allied health professionals; a general practitioner; a solicitor; a lay person; and a public health physician. With this representation in mind, one may postulate that this membership would not reflect the socio-economic status of the local community and that this may have contributed to the REC being out of step with the parental arrangements of children in the wider community. Based on national Irish figures for one-parent families, requesting the inclusion of two-parent consent precluded one-third of the potential population from becoming involved in the study, as 35.2% of Irish families are noted to be lone-parent families (Central Statistics Office, 2007).
The second possible reason for requesting ‘two-parent consent’ may have been apprehension. In the United Kingdom (UK), Angell et al. (2010), in reviewing 80 randomly sampled letters issued by NHS (National Health Service) RECs, determined that some evidence existed that RECs were concerned about what may happen if only one parent were to sign a consent form. This concern is evident despite the fact that, as Angell et al. note, there is no problem with this issue in the eyes of the UK law, as clinical trial regulations only require one parent to provide signed consent.
A possible third reason for requesting two parents to sign consent forms may have been due to confusion in the REC on the issue of appropriate consent for minors in clinical and non-clinical trials in Ireland.
The two-parent consent requirement of the Irish Health Service based REC in this study was outlined in their response letter as being ‘a legislative requirement’. However, nationally, lack of clarity amongst RECs was apparent; this may be due to the absence of one body overseeing the governance of RECs in Ireland. In 2008, a national review of REC practice (Health Service Executive Research Ethics Committees Review Group, 2008) was undertaken, with participants suggesting that ‘there is a legislative vacuum and there is no clarity for non-clinical trials research. Some RECs operate to their own SOPs and some follow the guidelines available from the Irish Council for Bioethics’ and that ‘the clinical trials act was brought in for a specific purpose but what it has done, or appears to have done, is (it) has forced people into a way of thinking, that maybe, could be replicated with research that’s not of a clinical trials nature’.
The European Communities (Clinical Trials on Medicinal Products for Human Use) Regulations 2004, which govern clinical trials and the establishment and direction of ethics committees (Irish Department of Health and Children), outline that ‘every person with parental responsibility for the minor’ should be consulted, and give their consent to a minor taking part in a trial. The Irish Council for Bioethics (2004) guidelines state that ‘parental or guardian’s consent must be sought’, and Sheikh (2008) maintains that all research, apart from a clinical trial, is not governed by legislation in Ireland, concluding that ‘where a minor is concerned, decisions in relation to its welfare are decided by the parent / legal guardian’. It is possible that the issue of consent in this study, when considered by the REC, was treated as consent for a clinical trial.
It is very welcome to note that in response to the REC practice review (Health Service Executive Research Ethics Committees Review Group, 2008), a comprehensive package of consultations was undertaken to develop a standard national REC application form and guidance document for use in Ireland. This document was introduced in 2011 (Molecular Medicine Ireland, 2004), and in it the chairperson, in her introduction, states that the standardised approach was introduced in response to the fact that ‘the ethical review process had become an obstacle to research rather than a facilitator of it’. It is interesting to note that the standard guidance now specifically outlines the requirement for minors with regard to consent: ‘persons under the age of 16 cannot give consent to take part in most research studies, and (if consent is being sought) it should be sought from one parent or one legal guardian. It is recommended however that persons under the age of 16 be assented to participate in a manner appropriate to their age and level of understanding’ (Molecular Medicine Ireland, 2004).
Fine and Sandstrom (1988) suggest that ‘in some ways, the idea of informed consent with preschoolers would seem like a laughable conceit’, but go on to say that ‘children should be afforded some explanation’ and that ‘this simple explanation might be sufficient to provide a measure of informed consent consistent with the informants’ understanding’. The issue of assent with minors is an important consideration, particularly when one is aiming to give children a voice. In this study, while those children partaking in the study were asked for verbal assent, there were other children (whose parents had not consented) who specifically asked why they could not partake in the study exercise and expressed disappointment when they were not able to do so.
Biggs (2009) notes that in the UK there are a number of conflicting issues on consent between the law and ethical guidance and that the autonomy of minors is better protected by ethical guidance than by law. Biggs further suggests that ‘Obtaining the assent of those who lack the legal capacity to give valid consent is an important acknowledgement of their individual autonomy and self-determination’, and notes that if a minor is not able to provide legal consent, parental consent should only be sought and be seen to be legal when a child’s assent is in place. Considering this, it is a welcome sign that assent is now included in the national standard REC application form.
Ethical conditions and effect on data collection
The second condition imposed on the study was the requirement to use only published hedonic symbols (Chen et al., 1996), as they were ‘valid and reliable’.
For the study a schedule of questions and pictures relating to food was developed; the food pictures used were a collection gathered from Microsoft Clip Art, specifically for this study. The researcher met with a small group of three to four children (for whom ‘two-parent consent’ had been obtained) in their settings. Children were not taken from their pre-school room, but were asked to move as a group to one side of the room and asked to give their verbal assent to take part in the exercise. When in the group with the researcher, the children were shown the pictures of different foods and food situations, questions about the pictures were asked, and children requested to point to hedonic symbols (Chen et al., 1996) to answer the questions.
When the first picture of food was shown to the children in the group situation and they were asked the first question about this picture, it became apparent to the research dietitian that the children were unable to relate their feeling about the food picture they were being shown to the hedonic symbols they had been given.
After a number of unsuccessful attempts, the researcher then asked the children to point to the hedonic symbols and asked them what they thought each symbol portrayed. It became apparent that the children’s perceptions of the symbols were at odds to that which had been outlined in the literature (Chen et al., 1996). Table 2 outlines the children’s responses in this study, and the description given by American children, of similar age, in the study carried out by Chen et al. (1996).
Hedonic symbols; literature and children’s explanation
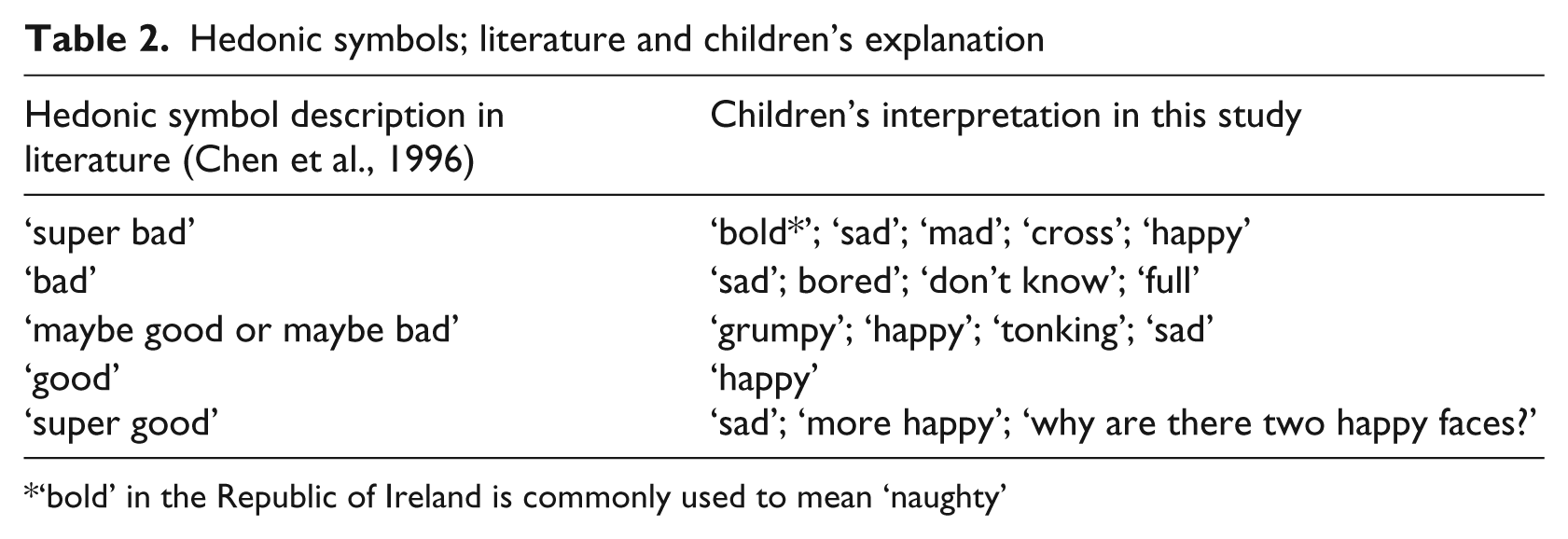
‘bold’ in the Republic of Ireland is commonly used to mean ‘naughty’
The inclusion of the published symbols may have had a negative impact on the children’s understanding of the study methodology, especially as the pilot pre-study demonstrated that the use of developmentally appropriate symbols led to a successful outcome, with children of this age correctly recognising the symbols. There is a need to recognise that tools that may be shown to be correct for use in a certain context may not be the most appropriate tools if used in a different scenario. While the researcher submitted Microsoft Clipart symbols with the REC application, it became clear through two rounds of correspondence with the REC on this issue that they required that only validated symbols were to be used.
Fine and Sandstrom (1988) have noted there are challenges to creating research tools for use with pre-school aged or pre-literate children; perhaps it is for this reason that the REC felt that a pre-published instrument may yield better results than something created at a local level.
The poor outcome of this study, however, does not reflect badly on the hedonic symbols from the literature that were used. The inability to collect data in this study, with a tool developed for research carried out in another country, more than a decade previously, is quite unsurprising, and rather than the researcher challenging the published literature, this result should further add to an information base which recommends the need to have situation specific tools with which to work with young children, to enable them to narrate their story (Fine and Sandstrom, 1988). Moreover, it is important that specific research applications for work with minors be dealt with by RECs on an individual basis, especially if there are no recent studies of a similar nature within the same cultural context.
Approaching RECs regarding ethical constraints imposed
In retrospect, it may have been possible to consider the ethical conditions prescribed and predict the type of problems that might be encountered when endeavouring to undertake the study under these ethical constraints. However, as Dixon-Woods et al. (2007) suggest, ‘the proper role of applicants is one of docility; in responding to letters they must make displays of obedience and deference. In particular, unless they are to resort to the appeals mechanism, applicants are obliged to accept judgements which are inherently contestable and indeterminate as incontestable and final.’ Dixon-Woods et al. also note that applicants’ hands are effectively tied when it comes to receiving REC letters with recommendations, as to disagree would mean taking a huge risk of an unfavourable ethical opinion.
Perhaps if there had been the opportunity to discuss the ethical issues raised by the REC in a face-to-face interview, this may have helped to allay the concerns of the REC and, therefore, may have resulted in a different endpoint with regard to this study. It would appear that there is the possibility to do this in the UK; Dixon-Woods et al. (2007) note that researchers may now attend REC meetings and that this can have an influence which may be seen in subsequent REC decision letters.
Perhaps this facility is also possible in an Irish context; however, this possibility is not clearly evident. In this study, all correspondence with the REC was by postal letter. It is interesting to note that, even within the new national standard application guidance manual (Molecular Medicine Ireland, 2004), there does not appear to be any information on how a REC can be approached in a face-to-face manner to discuss its decisions.
Conclusion
With increased numbers of children spending significant time in early years’ settings, it is important that children are consulted regarding the potential impact of this on their food intake and preferences. There is a dearth of studies focusing on the VOC in this age group, and no study could be found which aimed to ascertain perceptions of food among children of this age group. Although this study took place in Ireland, the lack of published literature in this area probably indicates that this may be an issue on a wider scale.
It was agreed that the limitations of the final sample and the poor response to the hedonic symbols rendered the results from this element of the study invalid. Little meaningful data were obtained from this study, which is hugely disappointing. However, it is important to delve into the ethical issues that surround research with children. Gathering an understanding of the issues of consent and assent, and contemplating the importance of developing age and culturally appropriate information collection tools, is very important to equip those who hope to undertake such research in the future. Researchers should be cognisant that the important need to maintain strict ethical standards must be balanced with the need to give due regard to determining the child’ voice in research.
Footnotes
Funding
This material is based upon works supported by safefood, The Food Safety Promotion Board, under safefood Grant No. 01-2008, in association with the Health Service Executive.
Competing interests
None of the authors have any conflicts of interest to declare.