
Abstract
Context:
Human papillomavirus coverage varies widely among women depending on their race, incomes, geographical location and education level.
Objective:
To evaluate whether reminder educative phone calls increase human papillomavirus vaccination rates in adult women aged 18–45 with high-risk factors of cervical cancer.
Design:
We conducted a single-blind randomized controlled trial in patients who consulted at a Canadian tertiary center in October 2019 during National Cervical Cancer Awareness Week.
Interventions:
We randomized women to receive three standardized educative phone calls or standard care.
Main outcome measure:
We assessed the immunization rate at 6 months.
Results:
A total of 130 patients were randomized of which 62 patients were randomized to the intervention. Eight patients (15.4%) got immunized at 6 months in the intervention group as compared to seven (11.7%) in the control group (p = 0.5645). The main barrier to vaccination reported by non-immunized patients at 6 months was the cost of vaccination (42.3%).
Conclusion:
Reminder educative phone calls did not increase human papillomavirus vaccination rates in adult women with risk factors of cervical cancer.
ISRCTN registration number: ISRCTN58518971
Introduction
Accounting for 569,847 new cases and 311,000 deaths in 2018, cervical cancer is classified as the fourth most frequent cancer in women worldwide. 1 Human papillomavirus (HPV), a sexually transmitted disease, is identified as the source of 99.7% of cervical cancers. 2 HPV is also related to vulva, vaginal, oropharyngeal, penis and anal cancers as well as genital warts. 3 With a 50% lifetime risk of affecting women and men, this viral infection is a real global burden. Available for more than a decade, HPV immunization is a very safe and effective primary prevention measure. 4 The third and last available HPV vaccine launched in 2014 is a nonavalent second-generation vaccine effective against five oncogenic HPV types. It offers a 90% cervical cancer protection. 5 It has been approved for females aged 9–45 years old and males aged 9–26 years old. 6 The World Health Organization (WHO) estimates that 80% immunization rate would reduce by two-thirds cervical cancer incidence. 7
Unfortunately, despite being a largely preventable disease, HPV coverage varies widely among women depending on their race, incomes, geographical location and education level. 8 Australia was the first country in 2007 to introduce a government-funded HPV immunization program for girls aged 12 and 13 years old. Since then, many other countries joined this initiative including Canada. In accordance with WHO, the Canadian Government as part of a nation immunization strategy set a goal of 90% HPV vaccination rate among teenagers by 2025. 9 As of today, in Canada, girls between 9 and 17 years old as well as immunosuppressed women between 18 and 26 years old have free access to HPV immunization. 10 Although proven efficacy is higher before the onset of sexual activity, immunocompetent adult women may also benefit from vaccination and are disadvantaged by these programs. 11 In fact, only a single dose is efficient and offers durable protection.12,13
Many studies have evaluated different strategies to optimize HPV vaccination rates such as informational or school-based interventions, government measures and recall methods particularly in teenagers and parents. 14 As for reminder strategies, two randomized controlled trials showed a significant increase of over 10% in HPV immunization rates of teenagers by using reminder phone calls, mail or home visits.15,16 A randomized controlled trial showed a significant increase in immunization rates in adults who received reminder letters. 17 However, one randomized controlled trial failed to demonstrate the beneficial effect of text messages in increasing vaccination completion rates in patients aged 19–26 who received a free first dose. 18 The authors postulated that one of the limitations of this study was not being able to send personalized messages.
Another interesting approach included an educational brochure and phone call reminders addressed to parents of pre-teen girls. This study showed a significant 10-fold increase in the completion rate compared to controls. 19 In addition, literature supports the use of reminders for multidose vaccines to increase infant immunization rates since 1984. 20 It was also well documented, in a systematic review of studies regarding HPV, that parents had a higher vaccine acceptance when it was recommended by their physician, when perceived ability to contract the infection was high and when they believed its efficacy. 21
As of today, no study has evaluated methods to increase HPV vaccination rates in adult women between 18 and 45 years. Most of these patients cannot benefit from free programs; others were negatively influenced by parents at an appropriate time of vaccination. 22 The need to address barriers to catch up immunization and efficient strategies to increase vaccination coverage rate is essential to reduce cervical cancer rates in this subgroup of population.
Eligible patients have been met initially as part of National Cervical Cancer Awareness Week (October 15–19, 2019). During this prevention week, our department meets more than 300 women in the gynecology outpatient clinic, providing an ideal setting to recruit high-risk patients and evaluating the barriers to vaccination. Therefore, our main objective in this trial was to evaluate if reminder educative phone calls increase HPV vaccination rates in adult women aged 18–45 years. Secondary objective was to evaluate if high-risk cervical cancer patients would benefit more of an educative reminder intervention than low-risk patients. We also aimed to determine different barriers to HPV vaccination.
Methods
Study design
We conducted a single-blind randomized controlled trial at Centre Hospitalier Universitaire de Sherbrooke from October 2019 to June 2020. This study was approved by the Comité d’éthique de la recherche du CIUSSS de l’Estrie—CHUS (registration number 2020-3319). The trial was registered retrospectively. The design of the submitted study is identical to what the institutional review board assessed when providing approval before the trial started. The protocol was not registered before the start of enrollment because there was a very short delay between the acceptance of our protocol by the ethics committee and the start of enrollment (a few days) and this step was therefore unfortunately forgotten at this time.
Study population
The study population was a sample of women aged 18–45 years old without prior HPV immunization. Women were eligible for study if they agreed to get a prescription of HPV vaccination and understood French. Women who did not know their HPV immunization status or refused vaccination were excluded. Patients were mainly recruited in free cervical cancer screening clinics during National Cervical Cancer Awareness Week held in October 2019. A minority of patients were recruited in colposcopy clinic at the Centre Hospitalier Universitaire de Sherbrooke and in a Mall kiosk held to promote prevention week activities. Initial contact of potential candidate patients was performed by study authors or a single research assistant who gave them a pamphlet with information on HPV infection and a vaccination clinics list and described the study (risks, benefits, voluntary participation). The vast majority of patients (more than 90%) consented to participate in the study by signing a written informed consent form prior to participation. If the patients were seen in one of the other screening clinics (outside the CHUS clinic or our medical clinic), they were offered information on the research project and they could decide if they then wanted to leave their contact details in order to be contacted by one of the co-researchers to explain the project. In order to limit travel for these patients, consent was obtained verbally by one of the co-researchers (J.R.-L. or M.-P.B.-G.).
This form of verbal consent (reading the consent form) has been accepted by our ethics committee. Participants were not informed regarding the aim of intervention. They were told that the objective of the study was to evaluate barriers toward HPV vaccination. In order to minimize deceptive ethical issues, subjects were fully informed of all objectives and intervention in a letter posted after final assessment.
Study interventions
Figure 1 outlines the trial time line. All eligible participants were given an initial recruitment questionnaire where risk factors of cervical cancer and immunization status were assessed. The risk factors of cervical cancer identified were based upon a clinical gynecology oncology reference book. 23 They received a file that contained a three-dose HPV vaccine prescription, vaccination clinics contact list and an HPV information brochure from the Society of Obstetricians and Gynaecologists of Canada. If a subject was assigned to the intervention group, she received a total of three standardized phone calls at 1, 3 and 6 months after randomization made by either the same author or one of the two research medical students involved. During the first two interventions, callers needed to follow the instruction of an educative script and at each intervention call, participants verbally informed research team if they got vaccinated and if not, investigators enquired what barriers they faced. If barriers identified concerned lack of patient knowledge about HPV or the vaccine, research team would provide a specific answer to any questions and assess any doubts or fear. If it concerned a logistical issue such as the loss of a prescription or not knowing where to get vaccinated, new prescription was directly made at the pharmacy and the vaccination clinic contact list was provided by email or discussed by phone. The control group received a phone call at 6 months to assess HPV immunization status and barriers to vaccination.

Study population inclusion/exclusion flow chart.
When patients did not answer a first phone call, a total of two callbacks were made and an email was sent with a short questionnaire. Patients who completed the study received a check by mail of 15 Canadians dollars each as a compensation for their participation.
Randomization
The randomization schedule was done in blocks of 6 in a 50:50 ratio. Allocation only occurred once the consent was obtained. A secured order list made by a computer generator determined the group allocation of each patient. 24 Only the two principal authors had access to the secured computer list. Randomized patients received all phone calls during the study period according to the group they were allocated. Given the nature of the intervention, study investigators and research coordinators were not blinded to treatment allocation.
Study outcomes
The primary outcome was to assess whether non-HPV immunized adult women would have a higher rate of HPV vaccination by using reminder educative phone calls. We followed patients for 6 months after their randomization and assessed their vaccination status.
As secondary outcomes, we evaluated whether high-risk cervical cancer patients would benefit more of an educative reminder intervention than low-risk patients. We recorded rates of vaccination at 6 months for high-risk patients in intervention and control groups. High-risk patients were categorized as presenting one or more of these risk factors: smoker or past smoker, more than two sexual partners in the past 12 months and low education status (high school or less, history of abnormal pap smear or if they had their last pap smear more than three years ago). This information was derived from eligibility questionnaire.
As tertiary outcomes, we examined the different barriers to HPV vaccination. Barriers to vaccination in intervention and control groups mentioned by non-vaccinated patients were recorded. Barriers to vaccination in intervention group mentioned at 1 and 3 months which were overcome by educative phone calls were also recorded.
Sample size and statistical analysis
Despite the fact that very little literature is available on the subject, we considered that our intervention could double to triple the vaccination rate in women in our intervention group. Published literature on vaccination shows that effective interventions can double, triple, or even more, vaccination rates.14–17 We considered a vaccination rate of 13% in the control group (which represents the prevalence of HPV vaccination in Canada among women aged 26–45), and a vaccination rate of 32.5% in the intervention group (multiplying factor of 2.5). 24 We needed 71 women in each study group to have a power of 80% and an alpha level of 0.05. This calculation was performed using ClinCalc software. 25
Statistical evaluation was performed using nQuery advisor and Microsoft Excel 2019 software. Univariate analyses were used to describe the characteristics of the population in each group. The primary outcome of interest was the proportion of patients who got HPV immunized in the intervention and the control groups. This proportion was calculated as those who have received at least one dose of HPV-9 by the end of the 6-month evaluation period divided by the total number of subjects in the intervention or the control groups. Another outcome of interest was to determine the risk factor profile of patients who got vaccinated. We calculated the proportion of high-risk patients who got immunized in the intervention and control groups. In order to analyze these data, we used the chi-square test or the Fisher exact test for all of our dichotomous values such as vaccination at 6 months and the Mann–Whitney U test for continuous variables such as age. Probability levels (p-value) below 0.05 were considered statistically significant. Not all reminder phone calls were successfully delivered or emails responded but our analyses were made on the intent-to-treat principle.
Results
Patients
A total of 141 eligible patients were identified and 130 patients were randomized (Figure 1). The population is composed of 62 patients randomized to the intervention and 68 patients in control group. Groups were comparable for baseline characteristics, including age, education, smoking status and number of sexual partners in the past 12 months (Table 1). In the intervention group, 44.1% did not have a pap smear in the past 3 years as compared to 58% for patients in the standard group (p = 0.083).
Baseline characteristics. a
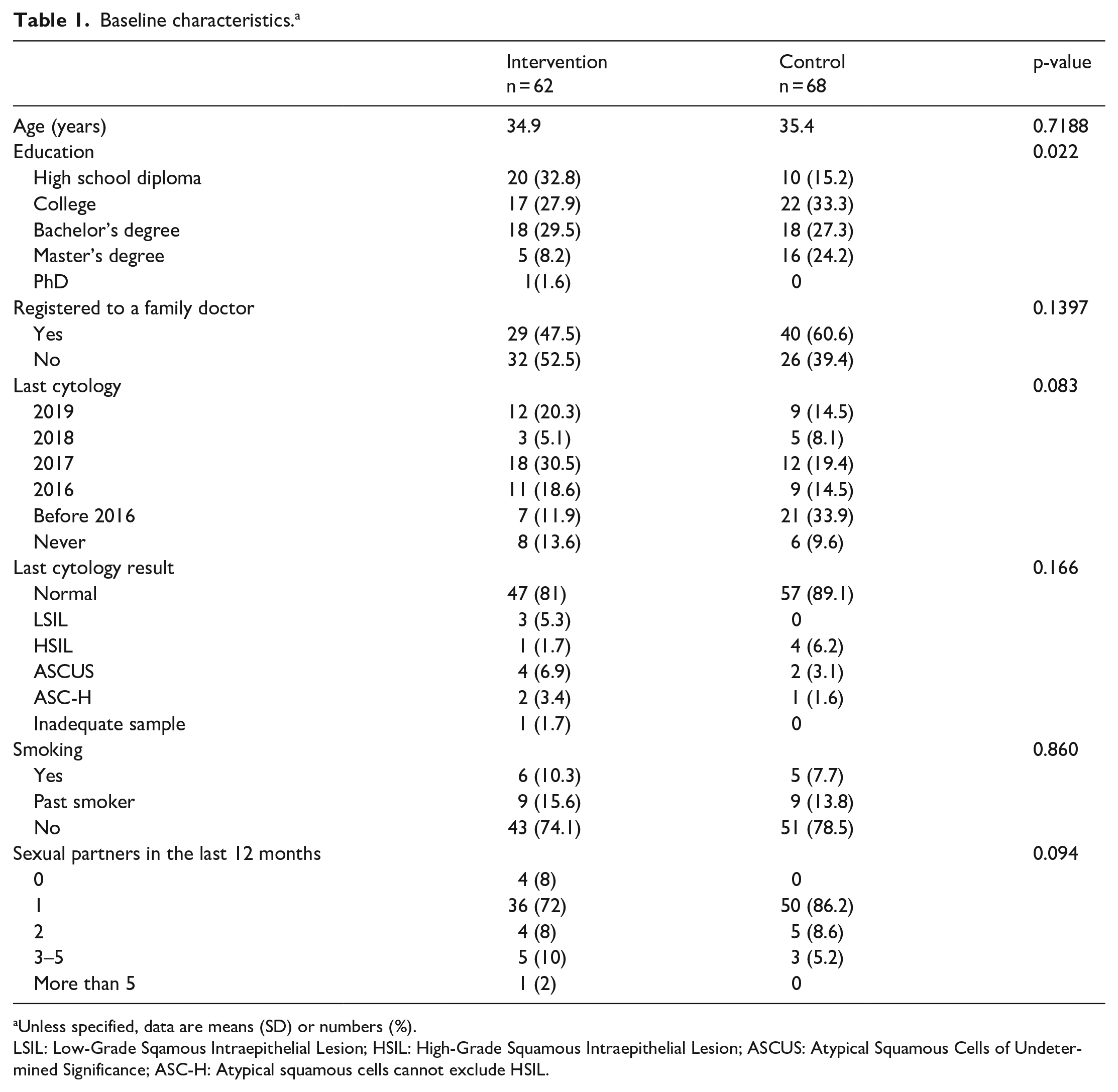
Unless specified, data are means (SD) or numbers (%).
LSIL: Low-Grade Sqamous Intraepithelial Lesion; HSIL: High-Grade Squamous Intraepithelial Lesion; ASCUS: Atypical Squamous Cells of Undetermined Significance; ASC-H: Atypical squamous cells cannot exclude HSIL.
Primary outcome
Eight patients (15.4%) got immunized at 6 months in intervention group (n = 52) as compared to seven (11.7%) in control group (n = 60) (p = 0.5645) (Table 2, Figure 2).
Vaccination. a
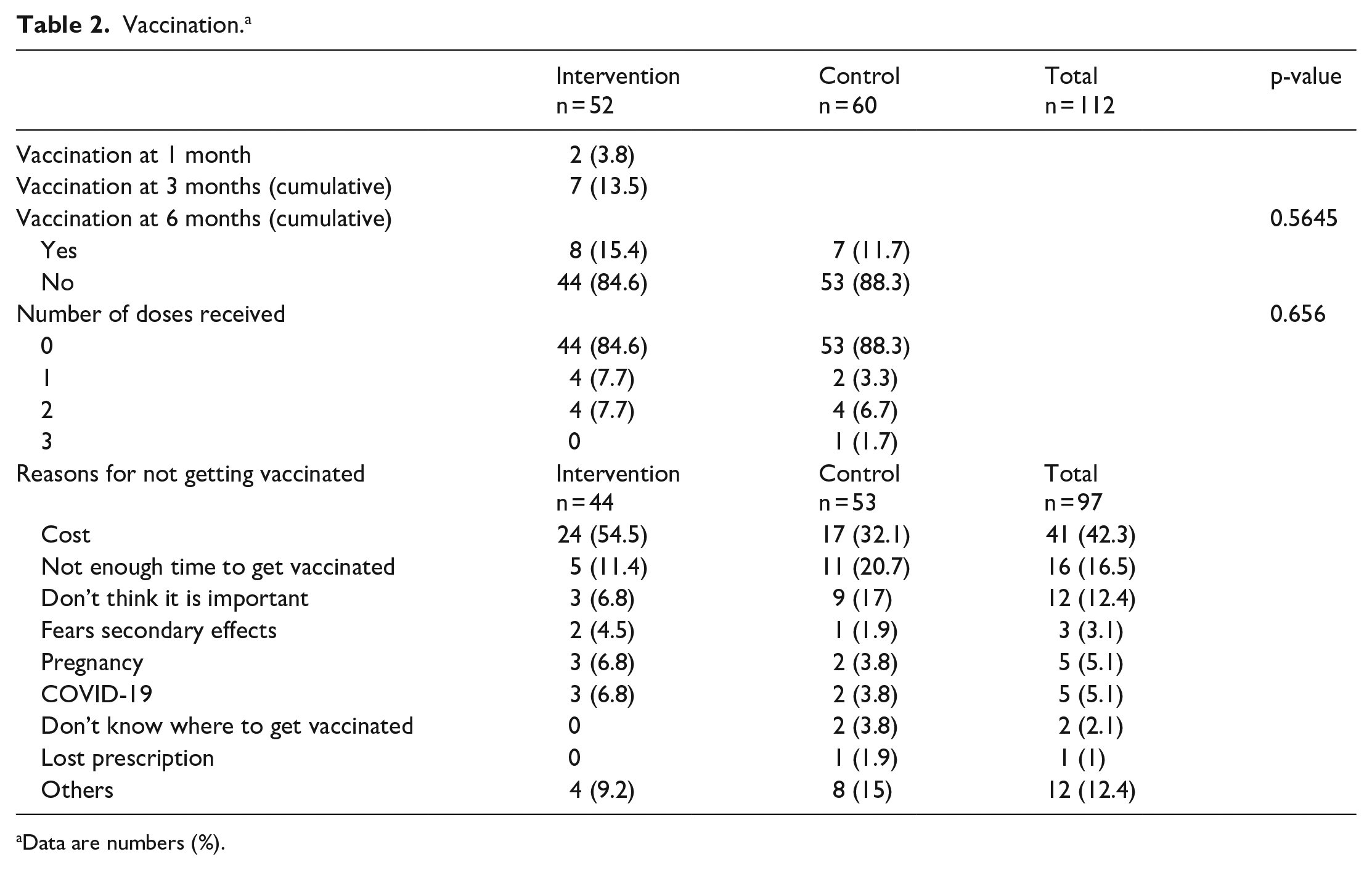
Data are numbers (%).

Percent of patients who received at least one targeted dose.
Secondary outcomes
Subgroup analyses of high-risk patients in intervention and control groups (smoker or past smoker, more than two sexual partners in the past 12 months, low education status, history of abnormal pap smear, last pap smear more than 3 years ago) did not show any difference in immunization rates (Table 3). No statistically significant differences were noted between groups for the number of doses received (Table 2). Barriers to vaccination reported by non-immunized patients at 6 months include the cost of vaccination (42.3%), the lack of time to go to vaccination clinics (16.5%) and the lack of importance of being vaccinated perceived by patients (12.4%) (Table 3). Six patients out of eight (75%) who got immunized in the intervention group got vaccinated after one or two educational calls (Table 4).
Risk factors of vaccinated women. a

Unless specified, data are means (SD) or numbers (%).
Barriers to vaccination mentioned at 1 and 3 months which were overcome by recall calls. a

Data are numbers (%).
Adverse events
There were no adverse events observed in either group.
Discussion
This study evaluated the use of reminder educative phone calls in women aged between 18 and 26 to address the persistent problem of low HPV immunization. While evidence in other settings showed a higher rate of vaccination completion with reminder interventions, our randomized controlled trial failed to demonstrate any difference between intervention and control groups.
Several factors could be implicated in this low immunization rate. Forty-two percent of patients mentioned “cost” as the most important barrier to HPV immunization. Forty-three percent of patients currently living in the state of Quebec do not have access to private health insurance coverage, which sometimes covers partial or total cost of HPV vaccination. 26 Public insurance does not offer coverage of HPV immunization cost. We did not assess insurance information in our trial, but patients who mentioned “cost” as a barrier to vaccination were asked if they had a private insurance and, if so, to check their vaccine coverage. These results are consistent with a national survey of US physicians on HPV vaccine, which showed that cost posed a barrier to vaccination. 27 This is also in accordance with pediatrician national survey where 70% of physicians believed that financial concern was a burden to HPV vaccination rate. 28
Another barrier to vaccination that was reported by 16% of patients was the lack of time. Although subjects were provided with an easy tool contact list of vaccination clinics, some still had difficulty to manage the vaccination appointment in their schedule. An interesting solution would be to offer HPV vaccination in a post-partum setting when women are actively engaged with the health care system. A prospective study evaluating this solution showed that 95% of women received at least the first dose and that satisfaction was very high. 29
The characteristics of our population may also be involved in low immunization rates. The population study was highly educated. Around 30% of the population had at least a bachelor’s degree. The educational aspect of the intervention had potentially a lesser impact in this subgroup population who might already be well informed. In fact, only 12% of the population did not seem to understand the importance of HPV vaccination while in other studies lack HPV knowledge is doubled. 30 Also, in our intervention group, 44% of patients did not have a pap smear in the last 3 years as compared to 58% in control group. These patients may have a more difficult health care accessibility or might be less concerned with their health. This could explain the difficulty to increase immunization rates in intervention group.
We needed a total of 142 patients to have a power of 80%. Unfortunately, by the end of the Awareness Week, only 141 patients were eligible and 130 were randomized. It is possible that a sizable effect of reminder calls was not detected because of a lack of power. Patients with higher risk of cervical cancer did not have a higher immunization rate. However, the sample of high-risk patients who got vaccinated (n = 12) was probably too small to achieve a reasonable conclusion in this subgroup of the population. If we look at the six patients in intervention group who got immunized after the third call, 50% had initially lost their prescription. A great alternative would be to send the prescription directly to their pharmacy. Once the prescription is received by the pharmacy, patient would receive a call and this could limit logistical problems.
The onset of COVID-19 pandemic during our research period has limited impact on our trial. Patients had already had their first and second call by that time, but we had to assess the impact of the pandemic on the possibility of getting vaccinated. Only 4.4% of all group population could not get immunized because of COVID-19.
The population selected was mainly from Sherbrooke City, which is a predominantly Caucasian area. The majority of our patients had one sexual partner in the last year, did not smoke, had a normal cytology result, had a regular cervical screening and had at least a college degree. The results of our study could easily be transposable to any low-risk Caucasian population.
The design of the study is very innovative since it includes personalized reminders and educative methods. Also, little data is available in literature evaluating adult HPV immunization interventions. Although no increase in immunization rates was noted, we were able to determine that financial concerns and logistical time issues were important barriers to vaccination. We also noted that loss of prescription is easily modifiable by sending prescription directly to patients’ pharmacies. A government financial aid directed toward a vaccination program in post-partum setting could be an interesting way to address the low rate vaccination in adult women.
Conclusion
In conclusion, reminder educative phone calls did not increase HPV vaccination rates in adult women aged 18–45 with risk factors of cervical cancer. It is possible that a sizable effect of reminder calls was not detected because of a lack of power. However, this study shows that multiple barriers to vaccination remain. The main barrier to vaccination is the cost of the vaccine. More study is needed on strategies that could overcome barriers to HPV vaccination in adults.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: Funding for this trial was provided by a grant funding from the research team at Sherbrooke University and from MERCK company. The financial aid was used to pay the two research medical students and to finance patient reward. The funders of the study had no role in study design, data collection, data analysis, data interpretation, and preparation, review or approval of the manuscript. The corresponding author had full access to all the data in the study and had final responsibility for the decision to submit for publication.
Data access and responsibility
The principal investigators, Marie-Pier Bernard-Genest and Jessica Ruel-Laliberté, had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.