
Abstract
Objectives:
This study assessed the non-utilization of PNC services, identified factors associated with PNC non-utilization, and explored barriers to PNC utilization in the rural community.
Method:
A community-based mixed-cross-sectional study was conducted from 20 March to 20 April 2020 among 521 women who gave birth in the last 12 months prior to this survey. A multistage sampling and face-to-face interview techniques were used for the quantitative data collection, and a purposive sampling technique was used to select the study participants. In-depth interviews were used for the qualitative data collection. The quantitative data were entered into EpiData version 3.1 and then exported to SPSS version 25 for analysis. A binary logistic regression analysis was used to test the association between the independent and outcome variables. A p-value of <0.2 was used as the cutoff value to include variables in the multivariate analysis. Finally, a p-value of <0.05 was used to declare an independent association. The qualitative data were manually sorted, cleaned up, and labeled as themes. Every major theme was identified and enumerated, and the meaning units were cited together with the relevant participant’s socio-demographic details.
Result:
The non-utilization of postnatal care was found to be 75.4% in the area. Normal delivery, fewer than four antenatal care visits, inaccessibility to transportation, and poor knowledge of postnatal care were all identified as factors enhancing non-utilization of postnatal care. However, being informed about postnatal care positively influences postnatal care utilization. Poor awareness, information gaps, cultural and religious beliefs, service inaccessibility, and the unfriendly approach of healthcare workers were all explored as barriers in the qualitative study.
Conclusions:
The non-utilization of PNC services in this study was higher than the majority, but not all, of the previous comparable local and worldwide findings. Mode of delivery, hearing postnatal care information, the number of antenatal visits, transportation availability, and knowledge of postnatal care services were factors affecting the non-utilization of postnatal care. The clients’ poor awareness, information gaps, cultural and religious beliefs, service inaccessibility, and healthcare staff’s inauspicious approach were barriers explored. Therefore, counseling and transportation access need to be reinforced in the setting.
Introduction
Globally, nearly 300,000 maternal mortalities were caused by pregnancy and childbirth in 2017. Ninety-four percent of these deaths were recorded in underdeveloped countries. About 196,000 maternal mortalities occurred in the sub-Saharan regions alone. Maternal mortality in Ethiopia has decreased from 1030 deaths per 100,000 in 2000 to 401 deaths per 100,000 in 2017. Nevertheless, this figure falls well short of the sustainable development goal’s (SDG’s). 1
The postnatal period, also known as the postpartum period, is a time when most maternal deaths occur compared to the antepartum and intrapartum periods. These deaths are related to complications such as hemorrhages, infections, hypertension, and genital trauma.2,3 The postpartum period is the most susceptible time for both the mother and her baby. 4 In the first 24 hours after birth, around half of all maternal deaths occur. Furthermore, two-thirds of it happens during the first several weeks after childbirth. 5 Likewise, in 2019, about 47% of all deaths among children under the age of five happened during the newborn phase, which falls under the postnatal period. 6
The postnatal period starts immediately after childbirth and lasts up to 42 days. It is critical to uphold the hope of the mother, newborn, partner, and family. 3 According to the World Health Organization (WHO), all births (regardless of birthplace) need a minimum of four visits in the postnatal period. It is recommended that mothers and newborns receive postnatal care within the first 24 hours of childbirth, as well as visits on day 3, days 7 to 14, and 6 weeks. 5
Despite its valuable dual benefits, low- and middle-income countries have low uptake and poor quality postnatal care (PNC).2,7,8 In sub-Saharan Africa, nearly half of women do not utilize postnatal care. Eastern Africa, including Ethiopia, has the lowest utilization of PNC in this region. 9 In the last two decades, Ethiopia’s PNC utilization has shown better improvement. 10 Nevertheless, around two-thirds of women and newborns do not currently receive PNC. 11
According to evidence around the world, the magnitude of the non-utilization of PNC is tremendously high in rural communities compared to urban areas.12–15 In Ethiopia, about three-quarters of postpartum mothers in rural areas do not get postnatal care. 11
Disparities are frequently associated with various characteristics that influence PNC uptakes, such as knowledge deficits, 16 service inaccessibility, lack of decision-making power, 17 lack of support from family members, cultural views, and negative attitudes toward healthcare professionals.4,18 Furthermore, PNC utilization could be influenced by some obstetric and socio-demographic factors such as place of delivery,9,19,20 mode of delivery,9,19,20 knowledge of obstetric danger signs,16,17,19–22 maternal education,9,16,17,21–23 antenatal care visit,9,10,19 and media exposure.16,23
The Ethiopian Federal Ministry of Health (FMOH) has been firmly struggling to curb maternal and neonatal mortality by launching different global and local strategies such as training health extension workers (HEWs) who identify and provide antenatal and postnatal care. 24 The HEWs conduct home visits on days 2, 6, and 42 of childbirth. In addition, they are responsible for linking mothers and newborns to formal healthcare facilities. 25
Although many studies have been conducted in Ethiopia regarding PNC utilization, the majority of them are limited to the urban community. Moreover, the phenomenon’s ingrained barriers were less explored qualitatively than the hidden barriers of PNC utilization in rural women. Therefore, the goal of this study was to assess the non-utilization of PNC, to identify associated factors, and to explore barriers among women who gave birth in rural areas.
Methods
Study setting and period
The study was conducted in rural districts of the South Gondar Zone of Northern Ethiopia from 20 March to 20 April 2020. The capital city of the zone is Debre Tabor, which is found 98 km, in the east direction from Bahir Dar, the capital of Amhara Regional State, and 666 km from Addis Ababa, the capital city of Ethiopia. There are 15 total districts, two urban, and 13 rural.
Study design and participants
A sequential explanatory mixed-method design that included both quantitative (community-based cross-sectional) and qualitative study was conducted among women who gave birth in the last 12 months preceding this survey. In the qualitative study, postnatal women, husbands, religious leaders, and healthcare workers (HEWs, midwives, and district health officers) participated.
Inclusion and exclusion
All voluntary participants who lived more than six months in the study setting were included in this study, whereas participants who were severely sick during data collection were excluded from the study.
Sample size determination
For the quantitative part, a single population proportion formula was used to calculate the sample size. Assumptions such as a 5% margin of error with a 95% confidence level and a 19% population proportion 26 were used.

Finally, after considering a 10% non-response rate and a design effect of 2, n = 522, was used.
For the qualitative study, 20 interviewees were selected by considering data saturation. We approached six postpartum women and four women’s husbands from the postpartum care utilizer side; three HEWs, three midwives, and two district health officers from the service provider side; and two religious (an Orthodox and a Muslim) leaders from the religious institutions to make the sample inclusive.
Sampling technique
For the quantitative study, multistage sampling techniques were utilized. Of the thirteen rural districts in the zone, 25% (Ebinat, East Este, and Simada) were selected randomly. In the second sampling stage, 30 kebeles (the lower administrative units) were selected randomly from the selected districts, and a proportional allocation was made for each kebele. Finally, a lottery method was used to select the study participants by using the postnatal mothers’ registration book as a framework. The registration book was obtained from the HEWs who conduct house-to-house visits in the community. The registration book includes the full addresses of women and their full personal and obstetric history. Women who were not available at home or who had closed their homes on the first day of data collection were re-visited the following day.
The interviewees for the qualitative study were purposefully chosen in light of the interviewees’ knowledge and experiences about the utilization of PNC (women) as well as their communication skills, in accordance with Palinkas et al.’s justification for purposeful sampling techniques. 27
Study variables
Figure 1 describes the conceptual framework variables included in this study. The framework was developed after reviewing similar literatures.9,16,17,19,21–23,28–31 Non-utilization of PNC was the study’s main outcome of interest, whereas participants’ socio-demographic characteristics, obstetric factors, and characteristics of the health facilities were explanatory variables included in this study.

A conceptual framework of variables included in the study.
Data collection tools and procedures
An interviewer-administered structured questionnaire that was adapted from the previous studies was used for the quantitative study.17,22,26,29,32–35 The tools were tested for validity and reliability in most previous studies. Four data collectors and two supervisors each conducted a face-to-face interview through a house-to-house visit of randomly selected participants.
We have followed the consolidated criteria for reporting qualitative research (COREQ) guidelines developed by Tong et al. 36 to collect the qualitative data. A face-to-face in-depth interview (IDI) that was guided by a semi-structured questionnaire was conducted by four male MSc professionals (two midwives and two nurses) who fluently speak Amharic (a local language) and share similar culture and traditions with the interviewees were interviewed to ease deep understanding of the interviewees’ responses. The day and time of the interview session were arranged by phone calls to prospective participation. None of the data collectors had earlier contact with any of the interviewees, and none of the interviewees were given any incentive for their participation. The interviews were undertaken at the interviewees’ homes for women, husbands, and religious leaders; and at health posts, clinics, and offices for the HEWs, midwives, and district health officers, respectively. Moreover, the interviewees’ provided quit and free settings, and other nonparticipants’ individuals were restricted from the interview session to prevent possible interruptions. During the interview session, methods such as field note-taking and voice recording (using a mobile phone) were used. Each interview session was given 30 min.
Data quality control
For both sections of data collection, two-day training was given for data collectors and supervisors regarding the tool and procedures. Before 2 weeks of actual data collection, a pre-test was done on 5% of the total sample in one of the non-selected districts. Moreover, the English version of the questionnaire was translated into Amharic and then back to English by two language experts. Supervision was conducted on a daily basis to check for data completeness.
Statistical analysis
The quantitative data were edited and coded before being imported into EpiData version 3.1 and exported to SPSS version 25. Descriptive statistics such as tables and graphs were used to describe the findings. A multi-collinearity test was carried out to see the correlation between independent variables using standard error and co-linearity statistics (variance inflation factor [VIF]). The goodness-of-model fitness was tested by Hosmer–Lemeshow statistic test. A binary logistic regression model was used to test the association between the outcome and the explanatory variables. In the bivariate analysis, a p-value of less than 0.2 was used as the cutoff point to include variables in the multivariate analysis. Finally, the significant association was declared at a p-value less than 0.05.
For the qualitative data, two language experts who are fluent in both Amharic and English were translated and transcribed into words and phrases. Moreover, written field notes were reviewed several times to get a sense of how it all fits together. To ensure the data’s validity and reliability, the research team revised and double-checked all translations and transcriptions. Then data were coded into clear words and phrases that contained aspects related to each other regarding content and context to form meaning units. The data were then sorted, cleaned, and analyzed using content analysis. All the key themes were identified and listed, and the meaning units were quoted with the respective participants’ socio-demographic characteristics such as age and occupation.
Operational and term definitions
Postnatal care. a package of services that comprise physical examination, health education on child care, breastfeeding, treatment, physiotherapy, immunization, family planning, and counseling services given during the postpartum period (up to 42 days).
Postnatal care utilized. If the mother has at least one visit out of the three, such as the third day, seventh day, and sixth week after delivery (for health facility delivery), and at least one visit at any time before 42 days after delivery (for home delivery), by skilled healthcare professionals.
Non-utilization of postnatal care. if the mother has no at least one postnatal visiting within 42 days of childbirth.
Good knowledge. Those mothers scored greater or equal to five out of eight knowledge-related questions about PNC (⩾5 out of 8).
Poor knowledge. Those mothers scored less than five out of eight on knowledge questions related to postnatal care services. 37
Results
Socio-demographic characteristics
A total of 521 women participated in this study, with a response rate of 99.8%. The participants’ average age was 29.03 years (SD ±5.75). The majority of the respondents (93.3%) were housewives, with government employees (3.5%) following closely behind (Table 1). Twenty interview subjects in all participated in the qualitative investigation. Six (30.0%), four (20.0%), three (15.0%), three (15.0%), two (10.0%), and two (10.0%) of the interviewees were postpartum women, husbands, HEWs, midwives, religious leaders, and district health officers, respectively.
Socio-demographic characteristics of women who gave birth in the rural districts of South Gondar Zone, Northern Ethiopia (from 20 March to 20 April 2020).

ETB: Ethiopian Birr.
Labor workers and students.
Non-utilization of postnatal care services among the participants
In the study setting, 393 (75.4%; 95% CI: 71.8, 79.3) participants did not utilize the PNC services (Figure 2). Regarding the frequency of PNC visits, the majority (84%) of participants visited only once.

Non-utilization of postnatal care service among women who gave birth in the rural districts of South Gondar Zone, Northern Ethiopia (from 20 March to 20 April 2020).
Reasons for not utilizing postnatal care services
Of those who did not utilize the services, more than three-fourths (78%) reported not being appointed by healthcare professionals as a reason for not using the services (Figure 3). The reason for the non-utilization of PNC was also explored in the qualitative investigation. For instance, in the subtheme of poor awareness, most of the participants stated that they are unable to differentiate the PNC visit from a child immunization visit. In addition, they expressed that they were unaware of the frequency and timing of PNC visits.

Reasons for non-utilization of postnatal care service among women who gave birth in the rural districts of South Gondar Zone, Northern Ethiopia (from 20 March to 20 April 2020).
For example, two (21-year-old Para-1 and a 35-year-old Para-III woman) interviewees said: . . . I think postnatal care is for immunization after 45 days.
Another 20-year-old Para-1 woman added: . . . I don’t know when I should go to the health center for a postnatal care visit. I think only for immunization at 45 days.
The information gap was raised as a barrier to the non-utilization of PNC services in this study. Interviewees mentioned poor counseling by healthcare workers and poor information or misinformation about the PNC as the reasons that hindered their PNC utilization. The healthcare professional is expected to counsel the postpartum woman for subsequent visits. However, poor counseling on when to return (schedule) to the health facility following childbirth was raised as the most common reason for the non-use of the PNC. For example, a 30-year-old para-2 postpartum woman voiced this problem as follows: . . . the midwives didn’t let us wait more than 6 hours if we weren’t bleeding, and they didn’t advise us to come back after we gave birth for a visit. We only met with them on the 45th day for child immunization, but not for a checkup for us and our baby.
Another 30-year-old para-2 woman added: . . . what am I going to do if I don’t feel unwell or if I haven’t been notified to come?
Likewise, 25-year-old Para-2 woman said: . . . if midwives appoint us for a checkup at any time, we are free to return, and no family that is against them gets the services.
Unfortunately, the healthcare providers also raised the issue of poor counseling as a hindering factor for utilization of PNC services. For example, 24-year-old HEW stated: . . . most health care workers, including myself, do not counsel the mother adequately during her pregnancy and delivery regarding PNC visits.
Another 26-year-old, HEW added: . . . often I ask women, “Why do they not use the PNC service?” They respond by telling me their health professionals’ gaps in telling us when to return; for example, they didn’t educate us during antenatal care services and during delivery to get the PNC services.
Poor information or misinformation was another issue that was explored in this study as an obstacle to PNC utilization. The majority of participants stated that they were only told to return for immunization every 45 days or if they became ill at any time. For instance, a 21-year-old para-1 woman said: . . . I had four visits during my pregnancy; they didn’t tell me about the availability of PNC visits during that as well as when I delivered my child. I do not have information about the availability, frequency, and time of postpartum care for us, but I do know the immunization of my child; even if not told by them, I didn’t miss it.
Another a 30-year-old, Para 2 woman added, . . . I had no history of postnatal care up to 42 days after my delivery because I was not told about it and I did not know the time of visits.
The closest partners in a woman’s decision-making, the husbands, also displayed gaps in information about PNC services. For example, a 30-year-old husband expressed this issue as follows: . . . if my wife is advised to use postnatal care services, I am free to support and accompany her at any time; however, health professionals do not adequately advise about the issue during delivery.
An information gap was also mentioned by the healthcare providers, the main source of information regarding the PNC. They revealed that women did not have information about PNC service availability in the area. They pointed out that the problem was higher in the rural community. For instance, a 24-year-old female midwife stated: . . . most mothers, especially in the rural areas, had an information gap on postnatal care services and they did not expect the availability of PNC after they gave birth.
Moreover, a district health officer reported that there was an unorganized mothers’ conference in which women share information regarding PNC and other obstetric care services. For example, a 29-year-old district health officer was mentioned as follows: . . . as a limitation in our woreda, the mothers’ conference is not facilitated, not routinely given, and does not include the key informants from the community.
It was also investigated whether the unpleasant manner of the healthcare staff was a barrier to PNC utilization. Under this theme, the interviewees mainly mentioned false reassurance and a lack of sympathy. For example, a 40-year-old husband and postpartum women who were 28, 20, and 35 years old expressed how most professionals treat women unfairly by using phrases like: “. . . taking it as the care given to us depends on the professionals.” When I delivered the second child at the hospital, a midwife who was standing with me said to me, “Not today, not even tomorrow, you will not give birth.” What type of labor do you have? “When I delivered this child, I didn’t go to the hospital. The reason was to not see their bad faces.”
Another, a 20-year-old para-1 mother explained, Hmm . . . even cleaners abuse us when they see any blood falling down on the floor. They also see us with bad eyes. For example, they told one of my neighbors to discard the urine from the receiver, and she told her to not go if they did not discard the urine.
Another barrier preventing women from using PNC services was discovered to be the healthcare staff’s inadequate ability to establish confidence and dishonest assurances. A 35-year-old Para-3 woman, for example, stated: . . . the midwives told me with full confidence that my baby would not be delivered alive and that it would be delivered with deformity due to “
A 40-year-old husband also added: . . . my wife was abused by the health professionals when she delivered the last child. They were not voluntarily due to their work.
Another barrier to PNC use examined in this study was community’s cultural and religious concerns. The interviewees mentioned societal norms like the idea that new mothers shouldn’t leave the house right away. They believed that leaving the house put postpartum women at risk for bleeding, known as “seraqian” in the research community. For instance, a 21-year-old para-1 mother said: . . . after we gave birth, until 10 days we should be in the house with other people and we should hold steel, as I heard it keeps us from bad evil. For example, bleeding “seraqian” is the most known problem that might lead us to death.
A 30-year-old husband mentioned: . . . in our community, after delivery, the mother should stay indoors and should be with other people. Even if she becomes sick, she will be waiting up to the 8th day to seek treatment.
A 28-year-old HEW clarified that some individuals have a negative view of home visits. She mentioned: . . . when we went to the out of town community for a home postnatal visit, while we saw the child, if he was big, they would not allow us to see him. They thought you may evaluate his body.
Religious fathers were in favor of all medical experts’ maternal care. Going outside the house in the postpartum time for PNC use or child immunization, according to some interviewees, is an unacceptable religious doctrine. For instance, a 25-year-old husband voiced: . . . some women still believe in religion, do not need treatment, and are not allowed to see their baby before 40 days after delivery.
A 21-year-old para-1 woman mentioned: . . . as I heard from my family and neighbors, immunization is not good if the baby is not taking ‘qibaqidus or Kirstina’.
Fortunately, religious leaders were enthusiastic about the PNC services. They clarified that, generally speaking, religious restrictions did not apply to maternal health services. For example, according to a 70-year-old orthodox priest (father), . . . women need adequate nutrition to relieve their bodies of weakness due to loss of blood and fatigue caused by labor. In addition to this, they need health professionals to provide the support needed.
A 55-year-old Sheikh (a Muslim father) added, . . . women are barred from religious activity for a few days after delivering, but not from health institutions. They can require medical help from professionals.
The characteristics of health facilities
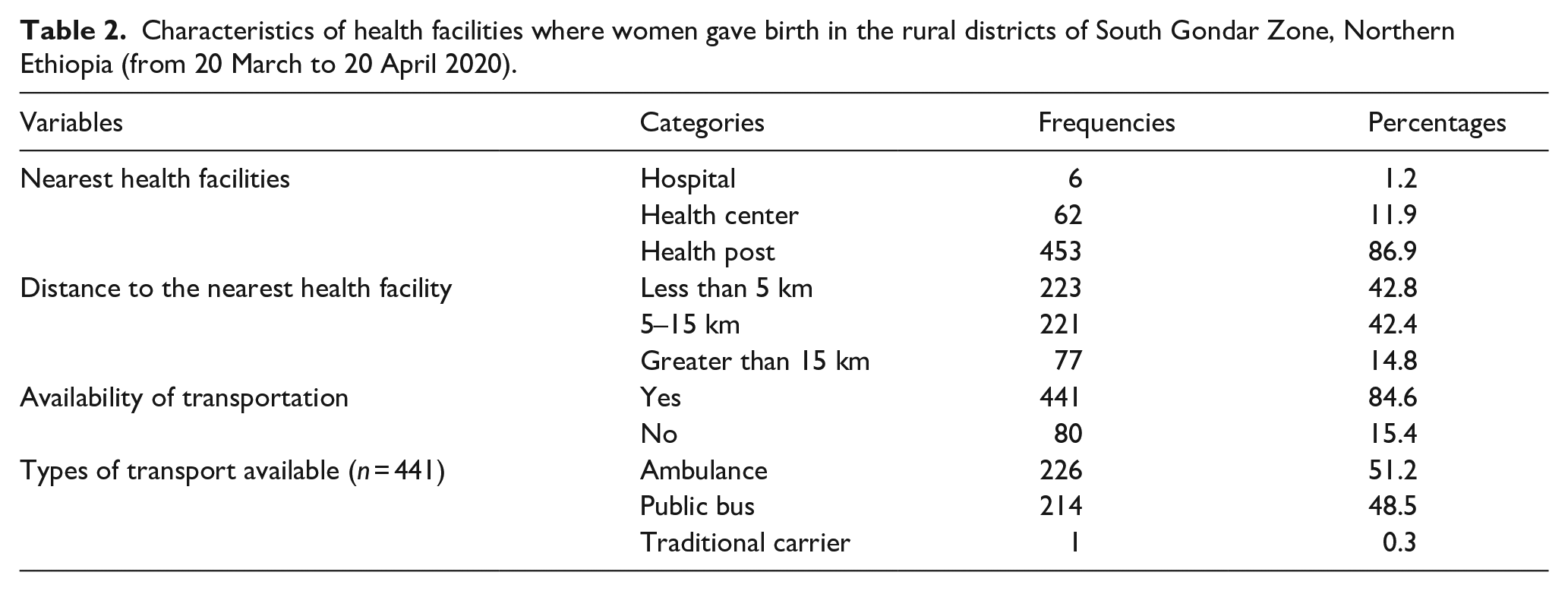
About 453 (86.9%) of the participants have health posts within a reasonable distance from their houses. Of those, 223 (42.8%) were located less than 5 km away from the health facilities. About 441 (84.6%) got a transport service. Of those, 226 (43.4%) respondents got traditional transportation and 214 (41.1%) got ambulance service. In the majority, 467 (89.4%) of participants gave birth at a health facility (Table 2).
Characteristics of health facilities where women gave birth in the rural districts of South Gondar Zone, Northern Ethiopia (from 20 March to 20 April 2020).
In the qualitative investigation, service inaccessibility was identified as one of the factors that obstructed PNC utilization. The PNC service’s inaccessibility in the setting was reported by both beneficiaries and service providers. The interviewees reported transportation problems, including a shortage of ambulances and drivers’ recklessness in the area, as reason the for PNC non-utilization. . . . before 3 years, I was working in a pool house. During that time, many drivers played pool. One ambulance driver responded to a woman who called on his phone, “The ambulance has no gas, so I cannot come,” but he was told to call his friend, “as his ambulance has gas, but he didn’t want to go.”
Another 25-year-old Para-2 woman stated, . . . the midwives gave us an ambulance phone number, but while we call it is not available and not answered sometimes.
Regarding the ambulance shortage, a 35-year-old husband said, . . . ambulance service is poor and ambulances are scarce. It is difficult to say “there’s an ambulance in our area.”
The interviewees also mentioned obstacles related to health facilities, such as inadequate postpartum admission rooms, a shortage of beds, and a scarcity of other important resources, under the service inaccessibility theme. The study’s healthcare interviewees indicated that a lack of resources made it difficult for them to give PNC services to everyone who needed them. From the beneficiary’s perspective, a 25-year-old husband said: . . . due to a lack of beds and space, the health institution is unable to provide all of the essential resources for postnatal care services. Our wives are discharged after six hours, rather than 24.
A 26-year-old midwife voiced: . . . we have not enough beds and waiting rooms for all mothers to give immediate postnatal care for the first 24 hours.
Another diploma midwife of 25 years old added: . . . materials are limited and other challenges exist, so we can’t give the postnatal care service.
Moreover, a 26-year-old HEW mentioned: . . . from delivery to the 7th day, postnatal care services are given by me at home. I couldn’t address all mothers for different reasons, such as lack of kits, but only for those critical or sick ones.
Obstetrics characteristics of participants
Two hundred seventeen (41.7%) of the participants had one to two children. The majority (493, or 94.6%) of participants’ last pregnancy was planned. Regarding the antenatal care (ANC) follow-ups of the last pregnancy, 490 (94%) had ANC visits. Of these, 419 (85.5%) had their follow-ups at the health center. Unfortunately, only twenty-one (4.3%) participants were counseled about PNC service during ANC follow-ups. In terms of pregnancy complications, 39 (7.5%) participants developed pregnancy complications. The majority, 467 (89.6%), of participants gave birth at a health institution, and of these, 394 (84.4%) were delivered through spontaneous vaginal delivery (SVD). About half of the participants were discharged within 6 to 24 hours after delivery. Regarding knowledge of PNC services, 308 (59.1%) of participants had poor knowledge of the services (Table 3).
Obstetrics characteristics of women who gave birth in the rural districts of South Gondar Zone, Northern Ethiopia (from 20 March to 20 April 2020).
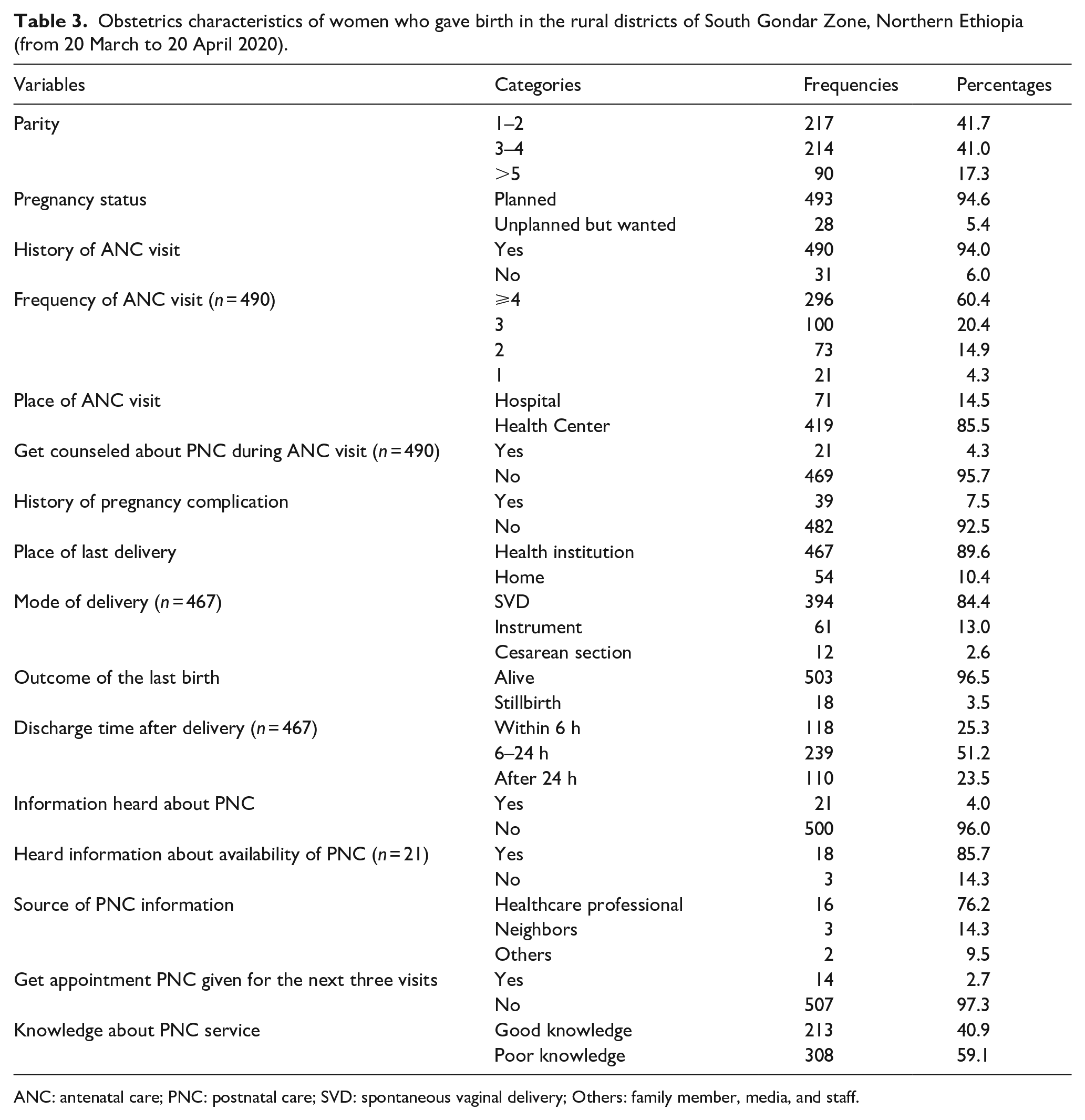
ANC: antenatal care; PNC: postnatal care; SVD: spontaneous vaginal delivery; Others: family member, media, and staff.
Factors associated with postnatal care service utilization
Table 4 presents both the bivariate and multivariate analysis of factors associated with the non-utilization of PNC. Of all the variables included in the bivariate logistic regression analysis, mode of last delivery, information about PNC, transport availability, frequency of ANC visits, and knowledge of PNC services were shown to be associated with non-utilization of PNC services.
Bivariate and multivariate analysis of factors associated with non-utilization postnatal care among women who gave birth in the rural districts of South Gondar Zone, Northern Ethiopia (from 20 March to 20 April 2020).

CI: confidence interval; ANC: antenatal care; PNC: postnatal care; Ref.: Reference category.
Postnatal care.
Crude odds ratio.
Confidence interval.
Adjusted odds ratio.
Spontaneous vaginal delivery.
Cesarean section.
Antenatal care.
p-value < 0.2
However, after controlling for potential confounders in multivariate analysis, mode of delivery (AOR: 0.46; 95% CI: 0.27–0.85), number of ANC visits (AOR: 0.21; 95% CI: 0.12–0.36), transport availability (AOR: 0.48; 95% CI: 0.23–0.99), information about PNC (AOR: 10.70; 95% CI: 8.07–23.54), and knowledge of PNC services (AOR: 0.47; 95% CI: 0.30–0.73) were shown to have a significant association with utilization of PNC services.
Discussion
This study assessed the non-utilization of PNC services, identified factors associated with PNC non-utilization, and explored barriers to PNC use in the rural community. As a result, the proportion of non-utilization in our study was found to be 75.4% (95% CI: 71.8–79.3), which was higher than the finding from the Ethiopia Mini Demographic and Health Survey. 11 Similarly, this finding is higher than the previous studies conducted in Sri Lanka (38.6%), Morocco(69%), Malawi (43.4%), Nigeria (68%), Tanzania (50.5%), South Sudan(56%), Debre Tabour Town (42.5%), Debre Markos Town (66.6%), East Gojjam zone (65.4%), Jimma Town(40.5%), Halaba kulito Town (52.1%), and Benchi-Maji Zone (48.8%).14,22,28,29,32–35,38–41 The most likely cause of this inconsistency is a difference in the places of residence. The majority of the previous studies were conducted in urban communities, whereas the current study was conducted in a neglected rural community. The other possible reason might be socio-cultural and religious beliefs in the area, which were also attested in the qualitative segment of this study.
The finding of this study is lower than studies conducted in rural Bangladesh (82.0%) and Mertule Mariam district (81%).26,42 This discrepancy could be attributed to time variations and socio-demographic differences between the current and previous study populations.
The recent study also identified the reasons for the non-utilization of PNC. Accordingly, 78% of participants reported being not appointed to PNC as a reason for non-utilization. This result is quite higher than a previous study conducted in Debre Tabour Town and Mertule Mariam district.26,33 This finding was also supported by the qualitative finding, where poor counseling was mentioned by the interviewees. Poor canceling might be due to a lack of training of healthcare providers and a shortage of human power in the setting. A study by Berhe et al. 43 supported this elaboration.
Favorable cultural and religious beliefs, adequate information, and good awareness regarding PNC services are key tools for women’s decision-making to use the service. These are by far the most important tools for avoiding the first delay in obstetric care. 44 Nevertheless, our study explored negative cultural and religious beliefs, inadequate information, and poor awareness of PNC services in the community.
In the current study setting, more than one-half of participants did not get ambulance services. This finding was also supported by the qualitative finding where interviewees revealed a lack of transportation as a barrier to PNC utilization. In light of delay models, this transportation-related problem fall into the second delay that could hinder postpartum women from getting the service by averting reaching the health facilities. 44
Moreover, our study explored barriers relating to the third delay model, including inadequacy of postnatal admission rooms, shortage of beds, and healthcare providers’ negative. This finding is in line with a study from the Tigray Region of Ethiopia. 43 The scoping review from Sub-Saharan Africa also concurs in the same way. 45
Regarding factors affecting the non-utilization of PNC, mode of delivery was significantly associated with the non-utilization of PNC. The participants who gave birth through spontaneous vaginal delivery (normal) were 46% less likely to utilize PNC than those who delivered through an instrument and/or cesarean section. This association was supported by the previous evidence from Sri Lanka, Northern Shoa, Debre Makos Town, and East Gojjam zone.29,31,32,41 This might be a result of users’ inadequate understanding of the likelihood of sickness or other difficulties during routine labor.
The odds of PNC utilization were 21% lower among participants who had less than four ANC visits compared to those who had at least four visits. This finding is consistent with Sri Lanka, Ethiopia’s demographic and health survey (EDHS 2016), and Mertule Mariam.23,26,41
In our study, participants who had no transport for a PNC visit were 48% less likely to utilize PNC service compared to those who had transport. Despite the fact that transport availability is a significant factor for postnatal care utilization, no study identified it previously.
The likelihood of PNC utilization was 11 times higher among participants who were informed about PNC utilization compared to those who were not. This result is congruent with studies from Morocco, Malawi, Nigeria, and the Mertule Mariam district.14,26,28,39 This entity was also raised by the interviewees in the qualitative section of the study.
Consistent with the empirical evidence that poor health knowledge compromises the intention and behavior of healthcare utilization, 46 participants who had poor knowledge of PNC were 47% less likely to utilize PNC in this study. This association is also compatible with findings from Nigeria, Mertule Mariale Mariam District, Jimma Town, and Demba Gofa rural district.22,26,30,39
As a strength, this study was conducted in a rural community and utilized a mixed-method design that explored barriers to PNC utilization. However, recall bias might be its shortcoming. Moreover, postnatal women who were not registered in the postnatal registration book (our sampling framework) could be accidentally excluded from this study.
Conclusion and recommendation
In comparison to the majority, but not all, of the prior comparable local and international findings, the non-utilization of PNC services in this study was higher. The mode of delivery, the frequency of antenatal visits, the availability of transportation, and knowledge of PNC services were all significantly associated to the non-utilization of PNC. The barriers to PNC utilization, including users’ poor awareness, information gaps, cultural and religious beliefs, service inaccessibility, and healthcare staff’s unfavorable approach, were explored. Hence, we recommend healthcare providers and stakeholders to reinforce antenatal and intrapartum counseling and work to solve the transportation problems.
Implications for practice and policymakers
Healthcare professionals, including midwives and HEWs, need to enhance clients’ counseling regarding PNC utilization because it commences during ANC visits and in the delivery room. Thus, programs such as training of healthcare providers and information dissemination through social media could break the barriers to PNC utilization. To halt clients’ negative beliefs toward PNC service, community mobilization, including arranging mothers’ conferences via HDA and HEWs, needs to be reinforced. We are also hopeful that the current findings will help the government and other interested parties to address the service inaccessibility issues.
Supplemental Material
sj-docx-1-whe-10.1177_17455057221125091 – Supplemental material for Non-utilization of postnatal care and its associated factors among women who gave birth in rural districts of Northern Ethiopia: A community-based mixed-method study
Supplemental material, sj-docx-1-whe-10.1177_17455057221125091 for Non-utilization of postnatal care and its associated factors among women who gave birth in rural districts of Northern Ethiopia: A community-based mixed-method study by Getu Amsalu, Asmare Talie, Wubishet Gezimu and Abdissa Duguma in Women’s Health
Supplemental Material
sj-docx-2-whe-10.1177_17455057221125091 – Supplemental material for Non-utilization of postnatal care and its associated factors among women who gave birth in rural districts of Northern Ethiopia: A community-based mixed-method study
Supplemental material, sj-docx-2-whe-10.1177_17455057221125091 for Non-utilization of postnatal care and its associated factors among women who gave birth in rural districts of Northern Ethiopia: A community-based mixed-method study by Getu Amsalu, Asmare Talie, Wubishet Gezimu and Abdissa Duguma in Women’s Health
Footnotes
Acknowledgements
The authors express heartfelt gratitude to all study participants, data collectors, supervisors, and language translators for their invaluable efforts in securing data quality. The authors are also pleased with all the individuals who provided us with important information about study setting.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.