
Abstract
Objectives:
The purpose of this cross-sectional study was to investigate the association between daily physical activity and sonographically measured bone status among women during the lactation period.
Methods:
Final participants were 152 women 4 months after childbirth. Bone status of the participants was measured using quantitative ultrasonometry of the calcaneus (speed of sound). Daily physical activity was assessed using the Japanese version of International Physical Activity Questionnaire short version. After getting the International Physical Activity Questionnaire results, we classified participants into three categories (low/moderate/high) according to a protocol. Participants categorized into the low group according to the International Physical Activity Questionnaire were considered to be in the low physical activity group and those categorized into the moderate and high groups were considered to be in the moderate to vigorous physical activity group.
Results:
Speed of sound was significantly higher in the moderate to vigorous physical activity group (moderate to vigorous physical activity versus low physical activity, 1533 m/s versus 1523 m/s, p = 0.03). Daily physical activity was significantly associated with speed of sound, even after adjustment for confounding factors and prognosticators (β = 0.195, p = 0.02).
Conclusion:
Sonographically measured bone status was significantly higher in women who were physically active than in those who were physically inactive, suggesting that daily physical activity might help to maintain good bone status.
Introduction
Bone mass and density increase till the age of around 20 years and remain stable until menopause, and thereafter, bone mass and density steadily decline. 1 Thus, it is required to preserve peak bone mass and density until menopause. During the period mentioned, women experience pregnancy and childbirth. Hormonal levels dramatically change during the perinatal period. In addition, bone density decreases because of puerperal amenorrhea or lactation in postpartum women, and this decrease is much greater than that in postmenopausal women. 2 Although the bone density of postpartum women generally returns to their before-pregnancy condition, some women do not recover their pre-pregnancy status. 3 Therefore, women should recognize that they are at a high risk of decrease in bone density not only during menopause but also during the lactation period.
Postpartum bone density has been shown to be associated with activity restrictions due to high-risk obstetric conditions, body mass index (BMI), previous lactation periods, exercise, and other such factors.4–6 However, the factors that can be intervened upon are still limited. It has been reported that an exercise program focusing on resistance exercise may be effective for preventing a decrease in bone density during the lactation period among women. 6 However, it is difficult for postpartum women to make time for exercise because they are often busy with housework and childcare. Therefore, it might be necessary to focus on daily physical activity (PA) rather than exercise. However, no previous study has appropriately investigated the association between daily PA and bone status during lactation.
The purpose of this cross-sectional study was to investigate the association between daily PA and sonographically measured bone status among women during the lactation period. We established the hypothesis that being physically active was associated with good bone status during lactation.
Methods
Participants
Data were collected from health checkups performed for 4-month-old babies living in a city, Hyogo, in Japan between February 2016 and December 2016. Figure 1 shows the flow chart of participant recruitment and screening. The study recruited 182 women 4 months after childbirth. The exclusion criteria for this study were as follows: (1) a history of thyroid or kidney disease, (2) no breastfeeding, and (3) incomplete data. Based on these criteria, 30 participants were excluded from the study. Eventually, 152 participants were included in the final sample. Data collection began after the approval of our proposal by the Research Ethics Committee of the Kobe University Graduate School of Health Sciences (authorization number: 449). All participants received written and verbal information about the study from researchers, and they signed written consent forms before participation in accordance with the Declaration of Helsinki.
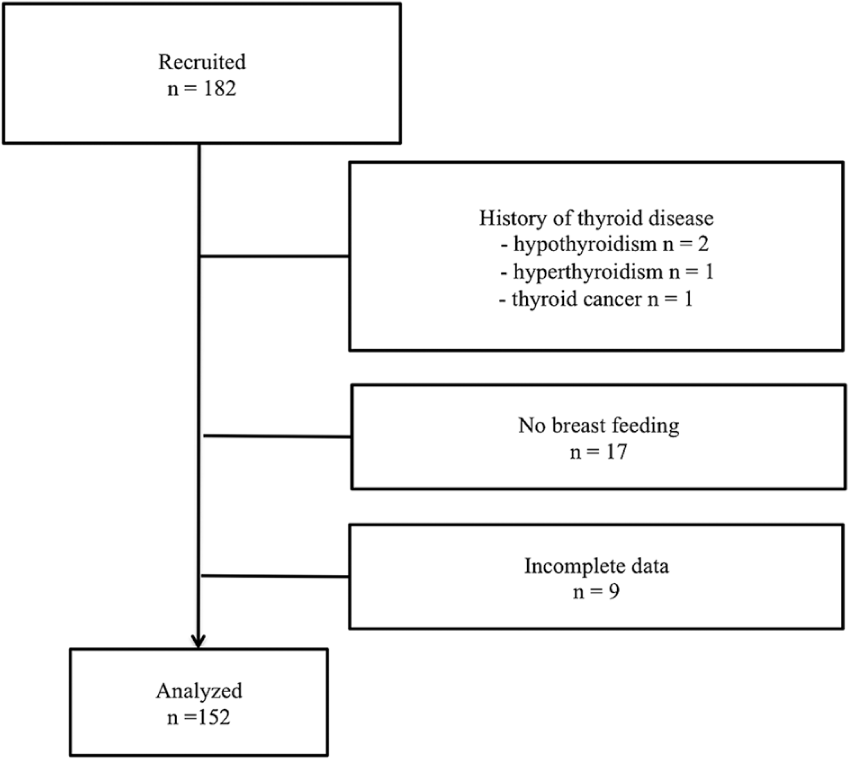
Flow chart of women recruited for and participating in this study.
Data collection
At the health checkups performed for the 4-month-old babies, bone status of the participants was measured using quantitative ultrasonometry of the calcaneus, and the participants answered a self-reported questionnaire. In addition, we collected data from medical records. The self-reported questionnaire and the medical records were used to assess demographic characteristics, daily PA, and other data that are known to be associated with bone density or peak bone mass.
Demographic data
Demographic characteristics included age, height, weight, previous birth experience, and medical history. BMI was calculated as follows: BMI (kg/m2) = weight (kg)/(height (m))2.
Bone status
Speed of sound (SOS) was measured using Ultrasound Bone Densitometer CM-200 (Furuno Electric, Hyogo, Japan). The calibration was performed before the day of assessment on adopting the machine setting. After the calibration, we set the foot size of each participant. SOS is the velocity of a sound wave traveling through bone at the right side calcaneus, and it is influenced by the elasticity and density of bone. 7 Some studies have shown that SOS reflects bone density.8,9 Therefore, SOS was used as a parameter of bone density in this study. We measured SOS thrice and calculated the average value. A higher SOS indicates better bone status.
Daily PA
Daily PA was assessed using the Japanese version of International Physical Activity Questionnaire (IPAQ) short version.10,11 In this study, participants answered the IPAQ themselves. The IPAQ is one of the questionnaires for assessing daily PA in the postpartum period. 12 Respondents provide information on the frequency and duration of vigorous-intensity activities, moderate-intensity activities, and walking in the past 1 week, retrospectively. We calculated the combined total PA score and classified participants into three categories (low/moderate/high) according to a protocol. 13
Other factors related to bone status
Bone status–related data included the state of breastfeeding, the presence of menstruation, history of exercise, calcium intake, and the time of sun exposure. Participants provided information on the frequency of breastfeeding and powdered milk per day. Participants who only undertook breastfeeding were classified into the exclusive breastfeeding group. The history of exercise was assessed using the closed-ended question “When you were a junior high school or high school student, did you exercise?” In this study, we defined an exercise habit as club activities that were performed more than thrice a week apart from a physical education class. 14 Calcium intake was evaluated using a self-assessment table for calcium intake, 15 which includes 10 questions (score ranges from 1 to 37). A higher score indicates higher calcium intake. The time of sun exposure was assessed to estimate the production of vitamin D, according to a previous study. 16 We asked participants the question “How long do you bask in the sun during the day?” Participants were asked to select the most appropriate answer. A score of 1 was allocated to women who avoided sun exposure, while a score of 5 was allocated to women who were exposed to sunlight, on average, for more than 30 min per day.
Statistical analysis
Data are presented as mean ± standard deviation (SD) or median (minimum–maximum) for continuous variables and percentages for categorical variables. In this study, few participants were categorized into the high group according to the IPAQ. Thus, participants categorized into the low group according to the IPAQ were considered to be in the low physical activity (LPA) group and those categorized into the moderate and high groups were considered to be in the moderate to vigorous physical activity (MVPA) group. We first compared demographic characteristics, the state of breastfeeding, SOS, and daily PA between the analyzed and excluded groups. We then compared each variable between the MVPA and LPA groups using the independent t test (normal distribution) or Wilcoxon rank-sum test (non-normal distribution) for continuous variables, as appropriate, and the chi-square test for categorical variables. Subsequently, multiple regression analysis was performed to explore the influence of daily PA on SOS. Standardized β was calculated. The objective variable was SOS, whereas the explanatory variable was daily PA (MVPA = 1/LPA = 0). We selected the following relevant confounding variables from preceding studies: age and BMI. Prognosticators were previous birth experience (yes = 1/no = 0), exclusive breastfeeding (yes = 1/no = 0), and sun exposure.5,17,18 A p value < 0.05 was considered statistically significant. All analyses were performed using Stata 14.0 (StataCorp., College Station, TX, USA).
Results
Table 1 shows the results of comparisons between the analyzed and excluded groups. Only the rate of exclusive breastfeeding was significantly higher in the analyzed group than in the excluded group (analyzed group versus excluded group, 73.0% versus 28.6%, p < 0.01).
Comparisons of demographic characteristics, the state of breastfeeding, SOS, and PA between the analyzed and excluded groups.

SOS: speed of sound; PA: physical activity; SD: standard deviation; BMI: body mass index.
Statistical analyses were performed using the independent t test.
Statistical analyses were performed using the Wilcoxon rank-sum test.
Statistical analyses were performed using the chi-square test.
p < 0.05.
Comparisons of demographic characteristics, bone density–related data, and SOS between the MVPA and the LPA groups are presented in Table 2. BMI and calcium intake were presented as median (minimum–maximum) because of their non-normal distribution. The number of multiparous women was higher in the MVPA group than in the LPA group (MVPA versus LPA, 75.6% versus 54.1%, p = 0.02). In addition, SOS was significantly higher in the MVPA group than in the LPA group (MVPA versus LPA, 1533 m/s versus 1523 m/s, p = 0.03).
Comparisons of demographic characteristics, bone status–related data, and SOS between groups classified according to PA (moderate to vigorous versus low).

SOS: speed of sound; PA: physical activity; MVPA: moderate to vigorous physical activity; LPA: low physical activity; SD: standard deviation; BMI: body mass index.
Statistical analyses were performed using the independent t test.
Statistical analyses were performed using the Wilcoxon rank-sum test.
Statistical analyses were performed using the chi-square test.
p < 0.05.
The results of multiple regression analysis are shown in Table 3. Daily PA was significantly associated with SOS, even after adjustment for confounding factors and prognosticators (β = 0.195, p = 0.02). Exclusive breastfeeding was negatively associated with SOS (β = −0.216, p < 0.01).
Associations between PA and sonographically measured bone status using multiple regression analysis.

PA: physical activity; BMI: body mass index.
p < 0.05.
Discussion/conclusion
In this study, we investigated the association between daily PA and sonographically measured bone status among women during the lactation period. We found that daily PA was associated with sonographically measured bone status even after adjustment for confounding factors and prognosticators.
Among preceding studies of subjects during lactation, Lovelady et al. 6 reported that participation in exercise programs, such as resistance and aerobic exercise, can prevent bone density decrease. On the other hand, Little and Clapp 19 showed that self-selected recreational exercise (walking, running, aerobics, and so on) did not influence bone density. These preceding studies focused on a mode of exercise and duration. Little and Clapp 19 reported that self-selected exercise did not stimulate bone remodeling in women during the lactation period, whereas an intervention program involving resistance and aerobic exercise was effective for bone growth in the lumbar spine and femur. 6 However, postpartum women currently have to perform housework and childcare by themselves because of the trend of nuclear families in Japan. In such a situation, it has been assumed that postpartum women do not participate in some exercise programs habitually, and therefore, we focused on daily PA, including exercise, in this study. A previous study has reported on the association between PA and sufficient bone density among postmenopausal women. 20 Our results build on the findings of this preceding study and show that PA is suitable for postpartum women. 20
The risk of a decrease in bone density due to puerperal amenorrhea or lactation in the postpartum period has been reported in a previous study. 2 In addition, the incidence of thin young women has been increasing every year in Japan. 21 Considering the correlation between BMI and bone density, 22 we believe that Japanese women have inadequate bone density before pregnancy. Thus, it is important for women to be physically active in the lactation period to preserve bone status.
In this study, exclusive breastfeeding was negatively associated with sonographically measured bone status. This result would be presumed because babies can consume calcium from their mothers through breast milk. Moreover, breastfeeding is extremely good from an immunologic point of view. Particularly in Japan, breastfeeding is generally recommended. Accordingly, we should think that the positive association between sonographically measured bone status and PA is important particularly in lactating women. Information on the association between exercise and bone status or between daily PA and bone status among women during the lactation period remains scarce. Thus, further longitudinal studies should be conducted in the future to obtain a consensus.
This study has several limitations. First, this study had a cross-sectional design, and we did not describe a causal relationship. In addition, the SOS immediately after childbirth was not measured. However, considering the logic of mechanical stress and bone formation, 23 habitual PA may have some influence on sonographically measured bone status. In future, the longitudinal studies should be carried out. Second, the sample sizes were small. However, despite the low statistical power conditions, the difference in SOS was significant between the PA groups. Thus, future studies should be conducted in larger sample sizes. Third, daily PA and exercise habit history were retrospectively assessed using a self-reported questionnaire in this study. A subjective assessment may result in measurement and recall bias. Future studies should use objective assessments for daily PA to enhance reliability. Fourth, calcium and vitamin D levels were measured using questionnaires. Although the questionnaires used showed the validity or correlation with 25(OH)D levels,15,16 calcium and vitamin D levels should be assessed through a blood examination in future studies. Fifth, the bone status was assessed using the SOS; however, it was not assessed individually. Dual-energy X-ray absorptiometry (DXA) is used as the standard device to diagnosis of osteoporosis. In the future, bone status should be evaluated using DXA to determine bone density. Despite these limitations, to the best of our knowledge, this is the first study to clarify the association between daily PA and sonographically measured bone status during the lactation period.
In conclusion, sonographically measured bone status was significantly higher in women who were physically active than in those who were physically inactive, suggesting that daily PA might help to maintain good bone status. Longitudinal studies are needed to examine the influence of daily PA on bone status, and objective evaluations of daily PA are needed to provide recommendations to women during the lactation period for bone status maintenance.
Footnotes
Acknowledgements
We would like to thank all study participants for taking their time and for their willingness to respond by means of the questionnaires. We would also like to thank the staff of the city for their assistance with this project.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.