
Abstract
Objectives:
To undertake an descriptive analysis of the health needs, healthcare practices and barriers to accessing healthcare faced by women in Lower Napo River Region, Peru, and to understand health literacy regarding cervical cancer and the need for more effective cervical cancer screening services.
Methods:
We performed a community-based needs assessment adapting Demographic and Health survey methodology with additional questions determining female health literacy on cervical cancer and assessing the availability and need for cervical cancer screening services. We surveyed women (N = 121) across all households in six communities along the Lower Napo River, Loreto, Peru, in May 2015. Data were collected as part of the larger Amazon Community Based Participation Cervical Cancer Screen-and-Treat Programme. Survey data were compared to national results from ENDES 2014.
Results:
Comparison between our findings and the ENDES 2014 survey highlighted considerable inequality between indigenous or mixed indigenous, rural populations in Loreto, Peru, and national population data averages over level of formal education, literacy, barriers to accessing healthcare and maternal and sexual health. Even though only 5.9% (N = 7/117) of women had no formal health insurance coverage, money was reported as the leading barrier accessing healthcare (N = 88/117, 75.2%). Health literacy regarding cervical and breast cancer was poor. A high proportion of women highlighted fear of screening processes (70.8%, N = 80/113) and lack of available services (53.6%, N = 60/112) as barriers to cervical cancer screening.
Conclusion:
Although progress has been made in improving healthcare access in Peru, such gains have not been experienced equitably and women living in remote communities face persistent marginalization regarding their health. There is a significant need for education related to and screening for cervical cancer in this region that is tailored to the reality of women’s lives in remote communities in Loreto.
Introduction
Globally, there is marked inequality between indigenous and non-indigenous populations in key socio-economic and health indicators. 1 Inhabitants of the rural communities of the Lower Napo River (LNR), in the Loreto Department of Peru, face persistent barriers to accessing health services, including limited health literacy, low rates of formal education, high levels of poverty and geographic barriers to health.2–4 While significant national economic growth since the turn of the century has led to reduction in national poverty levels and gross income inequality in Peru,5,6 rural and urban disparities in key indicators of health and healthcare access persist.7,8
Although much hearsay evidence suggests that women in rural Amazonian communities face high burden of disease, there are currently limited survey data to provide insights into the healthcare needs. Structural drivers of health inequity such as poverty, ethnicity and remoteness intersect with broader and culturally entrenched gender inequities to create significant barriers to health service use. 9 As women play a central role as care providers within these communities, understanding their health beliefs and healthcare practices is essential for the successful implementation of culturally and ethnically sensitive and effective health services. 10
To further understand the health needs of women in the LNR, the local healthcare organization DB Peru teamed up with a group of researchers at University College London (UCL), University of Birmingham, and University of Warwick to undertake a systematic evaluation of the demographic and health situation of women in the region. This study took place within the broader Amazon Community Based Participation Cervical Cancer Screen-and-Treat (ABCS) Programme, a cervical cancer prevention initiative which was the first of its kind in the region. The overall goal of the ABCS programme was to reduce death and disability from cervical cancer for women in the LNR. The project aimed to involve community members in a cervical cancer education and prevention programme, and encourage collaboration with the Peruvian Government, Iquitos Hospital and Mazan Health Centre. This was done through several steps including accurately quantifying women’s health needs and the burden of disease of cervical cancer in the region, providing education about the natural history, risk factors, and prevention strategies for cervical cancer and finally designing and delivering a sustainable cervical cancer screen and treat programme. In addition, concurrent vaccination against human papillomavirus (HPV) was provided in partnership with local government services. Two forthcoming papers will describe and evaluate, in detail, the impact of the ABCS education programme and the screening project itself. Prior to publication, additional information about the project can be found via the DB Peru website (http://dbperu.org/).
The primary aim of this article – which details the first part of the ABCS study – was to explore the health, healthcare practices and barriers to healthcare access faced by women within the LNR communities in rural Loreto and to draw comparisons with national health indicator data in Peru. The secondary aim was to explore female health literacy regarding cervical cancer and to determine barriers faced in accessing screening services.
Methods
Setting
Peru’s largest and northernmost region, Loreto, is covered almost in its entirety by the Amazon floodplains. The port city of Iquitos, the region’s capital and one of the least accessible cities in the world, is home to 45% of the region’s population 11 with the remaining inhabitants forming communities dotted along the Amazon River and its numerous tributaries. Those living within these remote river settlements are largely of indigenous or mestizo (mixed indigenous) heritage who identify as riberno (people of the river). Predominantly subsistence farmers, members of these communities have a rich cultural history centred around both the river and the jungle including a history of traditional medicine and plant-based healing.
DB Peru is a not for profit organization registered as a 501c3 non-profit charitable organization in the United States of America and as an organism no gubernamental in Peru. DB Peru was founded in 2003 and aims to provide healthcare, outreach and health education to the remote communities of the LNR, Loreto, Peru. At present, it serves over 5000 people living in 25 villages in the LNR. DB Peru has run health education programmes in the areas of infectious diseases and tuberculosis, antenatal care, breast and cervical cancer screening and dental health. Historically, their work has targeted the indigenous people of the LNR in the Peruvian Amazon jungle, who have limited access to healthcare. DB Peru works closely with the Ministry of Health and the local municipalities to augment their established programmes.
Community access and ethical approval
We gained access to the communities through existing DB Peru activities. Our work was facilitated by a team of community health workers (promotores). We were given permission to undertake research and the ABCS programme by community leaders.
Ethical approval for the fieldwork was secured by the Institutional Review Board of the Universidad Peruana Cayetano Heredia (Codigo SIDISI: 63685). All research was also formally approved by the Board of DB Peru. All participants were consented in writing and verbally, due to anticipated low literacy rates. Interview participants were reassured that their participation was completely voluntary. We also discussed the issues of anonymity and privacy, as well as how the data would be handled and stored after collection. Although there were no overt problems encountered when signing the consent documents, some women who were less literate preferred to make an ‘x’ mark instead of a full signature.
The overall ABCS project employed a community-based participatory (CBP) project model, incorporating local community meetings, consultations and involvement at each stage of the process. Education sessions around women’s health, cervical cancer and cervical screening were drafted in collaboration with the community and identified needs. The ultimate Screen-and-Treat programme was delivered between October 2015 and October 2016.
Survey
We performed a locally adapted demographic and health survey in 6 of the 25 LNR communities. These communities were selected as a representative sample of the wider LNR region because of both their population size and demographic characteristics. Furthermore, all six communities had previously been host to DB Peru and were logistically feasible for the study. The survey consisted of women’s health questions based on internationally standardized and locally validated Demographic and Health Survey (Encuesta Demogafica y de Salud Familiar, ENDES). 12 We added context-specific questions to evaluate women’s health needs, and focused on women’s knowledge and unmet needs in breast and cervical cancer (Supplementary material 1).
We recruited women aged above 15 years via promotores from every household within each community and invited all women who were interested to a group meeting prior to collecting data. We were present in the villages before and after the survey to raise awareness and respond to any concerns. Inclusion criteria were as follows: women aged above 15 years, a permanent resident of the selected village and cognitive ability to consent to the survey. Exclusion criteria were as follows: women or girls outside of this age range, those who are temporary residents or who are visitors and those who are unable to provide informed consent.
The surveys were conducted in May 2015 by a team of 10 trained volunteers working with DB Peru. Each survey was anticipated to last up to 2 hours, including verbal information and consent (given the anticipated low literacy rate in the region). We collected 121 surveys and visited six communities. The participation rate varied between 55% and 82% of women estimated to be present in each community on the day of the survey.
Results
Survey participants
In the 121 women surveyed, the mean age of respondents was 42 (range 21–76) years. We defined women of childbearing age within our sample as being aged between 15 and 49 years. This definition is also used within the ENDES survey and allowed us to draw comparisons between these two populations. In total, 91 women of childbearing age (N = 91/121, 75.2%), whose ages ranged between 21 and 49 years, were included. The women surveyed were mainly subsistence farmers or small-scale agricultural labourers (N = 112/121) or service providers (N = 9/121). Table 1 details the characteristics of the survey population.
Study participants characteristics.

We compared the results of our survey with ENDES data from 2014. Table 2 shows a comparison of results between the women of childbearing age within this sample and the average ENDES 2014 results.
Comparison between women of childbearing age in the LNR and national ENDES Data (2014).

LNR: Lower Napo River.
Education/literacy
Formal education was limited with most women having only received incomplete primary education (42.1%, N = 51/121). Only 12.1% of women of childbearing age in our sample had completed secondary education or higher, considerably fewer than national ENDES average of 59.7%. 7 Similarly, illiteracy levels in the survey population were nearly double the national average at 11.1% within the surveyed population.
Partnerships and empowerment
Most women (89.7%, N = 105/121) reported being married or part of a consensual union. In partnered women, average reported education levels of male spouses were higher than the women themselves: 20.2% reported their partners had completed secondary education or higher (N = 20/99) compared to 6.7% of interview respondents. Seventy-two percent (N = 88/121) of women listen to the radio but only 19% (N = 23/121) used a mobile phone and very few (3.3%, N = 4/121) had access to Internet.
Access to healthcare and traditional medicine
Six percent (N = 7/117) of women were uninsured, 83.8% (N = 98/117) were covered by Peru’s national comprehensive health insurance (Seguro Integral de Salud, SIS) and the remaining were covered by another form of medical insurance (N = 12/117). In the national Peruvian population, 68.6% of women are covered some form of health insurance, of which 40.6% are covered by SIS and 31.4% remain uninsured. 7 Despite a generally high coverage of insurance within the LNR, over two-thirds of women stated that money acted as a barrier to accessing healthcare (N = 88/117, 75.2%). This may indicate direct costs associated with seeking healthcare that are not adequately covered by the SIS insurance, such as the cost of transport between the river and healthcare facilities. Other barriers to healthcare access include transport (54.7%, N = 64/117), childcare (42.7%, N = 50/117) or not wanting to go alone (39.3%, N = 46/117). While the ENDES survey results demonstrated significant barriers to access, including finical barriers (59.7%), transport (35.4%) and not wanting to go alone (38.8%), 7 these were notably lower than reported within our sample.
Largely, decisions about their own health are made by women in tandem with their partners (64.9%, N = 74/114) or by themselves (23.7%, N = 27/114) with a small proportion having healthcare decisions made for them by their partners (5.3%, N = 6/114). However, 49.4% of women reported they felt they needed to seek permission to access healthcare compared to only 18.1% of women within the ENDES. 7
Eighty percent (80.3%, N = 94/117) of women reported using natural or traditional medicines when a member of their family was unwell. Many of respondents who use natural medicines learnt about plant-based medicine from their mothers (30.4%, N = 28/92) or grandparents (23.9%, N = 22/92). Accordingly, 95.6% (N = 87/91) have taught their children about traditional medicine. ENDES 2014 did not contain information about traditional medicine; however, this remained an important aspect of healthcare in the region.
General health
Self-reported health status was poor with the majority of women reporting ‘feeling slightly unwell’ (un poco mal) (47.6%) compared to only eight women feeling ‘very well’ (8.5%, N = 8/117). The most commonly reported health complaint within the survey sample was joint or back pain which was present in 55.2% of respondents; however, this was not reflected in care seeking behaviours. Of the women who had needed to seek care recently, the most common reasons included gynaecological complaints or pap smears (28.6%, N = 12/42), feeling generally unwell (19%, N = 8/42) and for dental work (11.9%, N = 5/42).
Sexual health
The median age of first sexual encounter was 16 years. Fifty of the 79 non-pregnant women of childbearing age who responded reported using contraception (65.7%). Of these 50 women, 45 used modern forms (90%) with the most commonly used form being the depot injection (N = 27/50, 60%). Five used traditional methods such as the rhythm method or withdrawal techniques. Twenty-two of the women surveyed reported being sexually active while not using any form of contraception and reporting they did not wish to currently become pregnant, or only wished to become pregnant in the future, leading to an unmet need for contraception in 24.1% of respondents of childbearing age. Of the respondents that answered, 66 out of 86 women (76.7%) of childbearing age reported receiving some form of information or education relating to family planning.
Maternal health and infant
The mean number of pregnancies for each woman was 5, with an average number of 4.6 births per woman in the 113 survey respondents who had ever been pregnant. A large proportion of women gave birth before their nineteenth birthday (N = 61/108, 56.5%) with very few women giving birth after the age of 25 years (N = 5/108, 4.6%). Eighty percent of reported deliveries (derived from information pertaining to the most recent delivery in survey respondents) occurred in the home (N = 87/109). Of the women who delivered at home, 20% (N = 17/87) reported no form of birth attendance, and 80% (N = 70/87) reported the presence of a traditional birth attendant. This differs from national ENDES data, which estimated that 91.6% of births were attended by a skilled attendant. 7 Some form of prenatal care was received by 64.5% (N = 69/107) of respondents and nearly all mother reported exclusively breastfeeding their children (98.2%, N = 107/109).
Breast cancer knowledge
Over two-thirds of women surveyed had ever heard of breast cancer (75.7%, N = 87/115) and 42.2% (N = 49/116) of women knew someone who has or has had breast cancer, but only half of respondents felt comfortable explaining what breast cancer is (50%, N = 58/116). Only 32% (N = 37/116) could identify one of the main symptoms. Accurate knowledge of early detection and treatment was limited. No respondents accurately identified measures for early detection of breast cancer (such as regular breast exams), and only 18 women identified the need to access health services when symptomatic (15.5%).
Cervical cancer knowledge
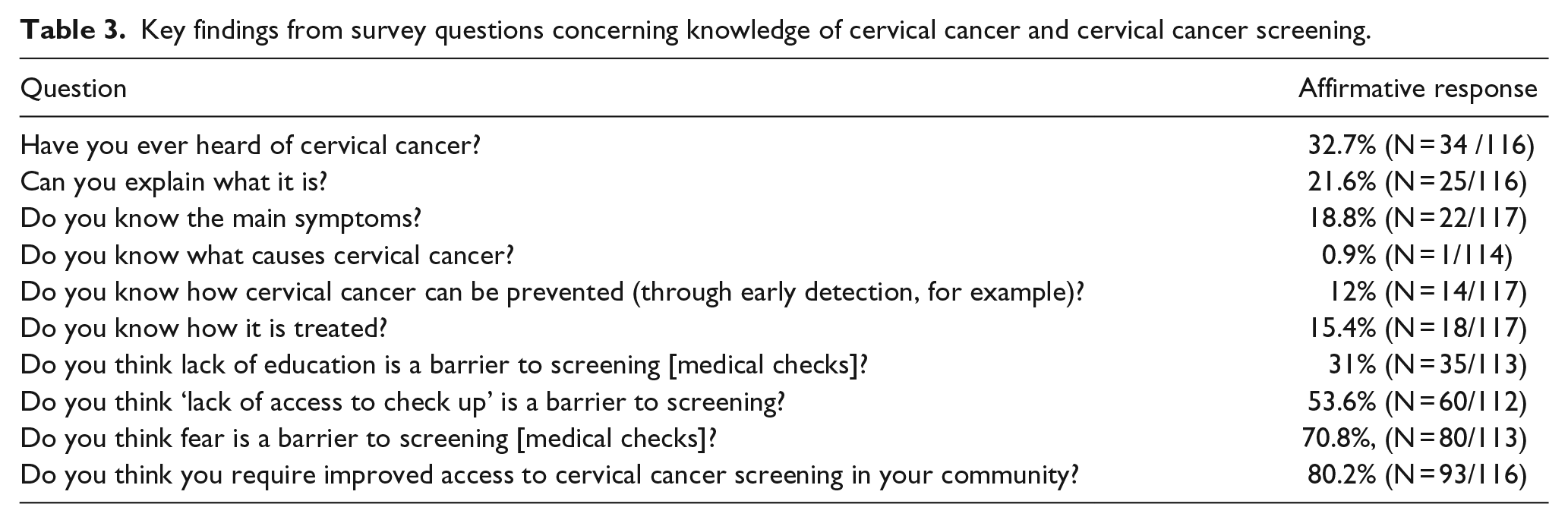
Table 3 shows the responses to survey questions surrounding cervical cancer. Less than a third of women had ever heard of cervical cancer (32.7%, N = 34/116) with just over a fifth who felt they could explain what cervical cancer is (22%, N = 25/116). Across the respondents 20% reported knowing someone who had been diagnosed with cervical cancer (N = 23/115). Only seven women (6%) identified routine pap smears as a preventive measure and only 18 (15.5%) indicated that if symptomatic they should access health services for assessment and treatment. The most common barriers to cervical cancer screening was fear surrounding the screening process (70.8%, N = 80/113) and lack of access to services (53.6%, N = 60/112). A vast majority of women expressed a need for cervical cancer screening programmes in their communities (80.2%).
Key findings from survey questions concerning knowledge of cervical cancer and cervical cancer screening.
Discussion
The aims of this study were twofold: to explore the health, health practices and access to healthcare for women living in the Lower Napo River communities and to assess women’s knowledge surrounding cervical cancer and the need for appropriate services within these communities. We found that women living in these communities face considerable barriers to accessing healthcare largely due to their socio-economic status and the area’s remote geography. Furthermore, we highlighted the considerable difference between data collected from women within these communities and the national Peruvian ENDES survey data, highlighting substantial inequality spanning both social-economic outcomes (literacy, years of formal schooling) and health outcomes (access to healthcare and maternal and sexual health).
Our research demonstrates prominent within-country disparities in both women’s health and socio-economic indicators in Peru and highlights the importance of the social and structural determinants of health in geographically remote and impoverished river communities of the Amazon. The creation of SIS insurance programme in 2002 and widespread health sector reform in 2009, aimed at improving health service equity, has led to a considerable increase in health insurance coverage for poorer members of Peruvian society. 5 This was supported by our findings, as only 5.9% of women reported being uninsured with a clear majority insured under the SIS scheme. Concerningly, we found that lacking money for treatment remained the leading barrier to accessing care in this population, supporting recent similar findings across both female and male populations across this region.3,4 Opportunity costs associated with seeking healthcare are significant, with women from low income households spending a higher proportion of personal income on care seeking than those from higher income backgrounds. 13 Despite high national coverage of health insurance, out of pocket expenditure continues to make-up a considerable proportion of health funding within Peru, inhibiting national goals of achieving universal health coverage (UHC). 14 Opportunity costs associated with care seeking are fundamental barriers to access within the LNR. Those wishing to access care face up to a 12-hour journey by boat from the LNR communities to Iquitos, where the nearest health facilities are situated, costing a large proportion of annual income. Respondents to our survey clearly highlighted that care seeking was also hampered by issues surrounding childcare with many women unable to find help to care for their children when they needed to access services. We found that even when women can make the journey to the city, they continue to face financial barriers through out of pocket expenditure for services and medications despite qualifying for free care; similar findings were reported by Kristiansson and colleagues 15 who explored care seeking for children within the Peruvian Amazon.
Despite poor health indicators from the Amazon states in Peru, significant progress has been made nationally in health metrics. Following widespread social sector reform across Latin America in the 1980s and Peruvian health system reforms centred around UHC, key health indicators such as life expectancy at birth, 16 under five mortality 16 and maternal mortality 17 all significantly improved between 1990 and 2015. However, inequalities driven by an individual’s gender, 9 ethnicity18,19 and region of residence 7 persist. Total government health expenditure is lower than similar-sized nations within the region, 5 in part contributing to supply side gaps in both health infrastructure and workforce numbers. 5 Due to persistent challenges to incentivize an already depleted healthcare workforce to practice in rural communities, 20 inhabitants of communities such as the LNR face further marginalization.
Novel responses to service delivery and mechanisms to ensure sustained financial protection are key to improving coverage and reduce barriers to access. The work of local and international non-governmental organizations (NGOs) remains important in improving health in the region. Our findings support that costly and lengthy journeys down river inhibit women’s willingness to seek care. Furthermore, fluctuant seasonal water levels can, for certain portions of the year, make the journey itself increasingly difficult. Projects like the Vine Trust’s Amazon Hope improve coverage of health services through using boat clinics staffed with local medical professionals and international volunteers to traverse the river, bringing care to communities. 21 A sustainable and community-focused solution is being led by DB Peru who are working to upskill promotores to ensure they can provide local basic healthcare within communities and importantly to identify clinical need for referral to larger healthcare centres. Globally, Community Health Workers have become pivotal in improving coverage of key health services in low- and middle-income countries (LMICs) 22 and are effective in ensuring improvement of access to essential services for women’s health. 23
Importantly, we found that women surveyed were considerably less likely to access key maternal health services than women surveyed within the most recent ENDES survey. The average number of deliveries per women in our sample was high at 4.6 and with a large majority of women not delivering in health facilities or receiving any form of skilled birth attendance. Furthermore, the coverage of prenatal care delivered by a trained healthcare professional was 20% lower than the national average. 7 These indicators, as risk factors for preventable maternal mortality, 24 highlight the significant risks associated with pregnancy and birth in this region. High fertility and parity is likely driven by a considerable unmet need for family planning within this population, which we found to be 24.1%, triple recent national estimates. 7 Despite considerable global investment in maternal health, inequities between and within countries such as Peru are persistent within key indicators, including access to and coverage of essential services. 25 Investment in improving maternal health must be rooted in equity and health system strengthening to reduce the considerable barriers marginalized women face within access to care.26,27
Women’s limited access to health services and health education is reflected in the low level of health literacy regarding cervical and breast cancer within this population. With a focus on cervical cancer, our findings show women have limited knowledge of behavioural risk factors that may contribute to development of the disease and are largely unaware of the need to undergo regular screening or to seek medical treatment for suspected cases. Barriers to undertaking screening are extensive, driven mainly by fear of the screening process and an identified lack of accessible services. Over 80% of respondents highlighted the need for accessible screening services within their communities. DB Peru has worked to understand the logistical barriers compounding the issue of high cervical cancer incidence. While screening services do exist within Loreto, in the city of Iquitos, a number of challenges to preventive care surrounding cervical cancer were evident. Previously, screening involving cytology testing through a pap smear which was ineffective for women within LNR communities. The process of undertaking screening and returning to the city for results collection is incredibly time-intensive and costly leading to significant loss to follow-up compounded by ineffective processing of results at local health facilities delaying results.
This needs assessment was conducted as part of the larger ABCS Project, a community-based approach to cervical cancer prevention. The crux of the approach involves bringing screening and treatment to women, rather than them needing to travel to town or to a clinic, thus overcoming barriers to access and reducing the disease burden. Furthermore, the project aims to shift focus towards prevention and away from treatment, which is more expensive and often occurs too late in the progression of the disease. Cervical cancer remains the most prevalent form of female cancer in LMICs, with 90% of mortality focused in low resource settings. 28 Peruvian cancer statistics reflect this with a cumulative risk of women developing cervical and breast cancer before the age of 75 years as 4.3% and 2.4%, respectively. 29 Cervical cancer incidence in the LNR populations is compounded by the high proportion of high-risk HPV subtypes within the Loreto region 30 and limited knowledge of HPV transmission and its contributory role in cervical cancer across the country. 31
Indigenous communities’ experience of cancer screening programmes varies significantly between populations in regard to knowledge, practices and beliefs, 32 suggesting a need for programmes appropriately tailored to the needs of communities. National screening programmes that fail to account for cultural and geographic disparities between indigenous and non-indigenous populations may be unsuccessful in delivering effective coverage of screening programmes. 33 The ABCS project is hinged upon a community-based approach and works in line with World Health Organization (WHO) guidance to deliver a screen and treat programme based on visual inspection of the cervix with acetic acid (VIA) and immediate cryotherapy of identified lesions where clinically indicated. 34 This process is recommended in low resource settings due the limited practicality of traditional screening which is hindered by lacking human resources, long waits for results and referral pathways meaning women would need to make long journeys to receive treatment.34,35
Our study had a number of limitations. Data were collected from a relatively small number of respondents within the LNR region, with participation limited to 55%–83% of eligible community members at the time of the survey. We were unable to survey any women under the age of 21 years, likely due to these women’s schooling or employment commitments. These factors could have introduced selection bias into the results and limited the generalizabilty of the results. For many women, this was their first experience of ever participating in a ‘survey’. This posed challenges where many women had difficulty in articulating their opinion and could possibly have introduced recall bias when reporting medical history. This was overcome by providing in-depth group explanations of the survey process and providing education to each woman as needed. We also opened-up discussions around breast and cervical cancer, performed all interviews in a safe and culturally appropriate manner, and maintained dialogue and communication with all community members.
Conclusion
While significant progress has been made at improving health within Peru, gains have not been experienced equitably across the population. We have found marked inequities between the women living in communities across the LNR and national ENDES data. As well as identifying the extent to which these women were socially marginalized and experienced health inequalities, we identified a significant unmet need for health education, preventive and curative interventions for prevalent issues of women’s health within this region, particularly for cervical cancer.
Supplemental Material
DB_Peru_Encuesta_de_Demografiia_General_y__Cuidados_Baisicos_de_Salud_supplementary_material – Supplemental material for A descriptive analysis of health practices, barriers to healthcare and the unmet need for cervical cancer screening in the Lower Napo River region of the Peruvian Amazon
Supplemental material, DB_Peru_Encuesta_de_Demografiia_General_y__Cuidados_Baisicos_de_Salud_supplementary_material for A descriptive analysis of health practices, barriers to healthcare and the unmet need for cervical cancer screening in the Lower Napo River region of the Peruvian Amazon by Joseph H Collins, Diana Bowie and Geordan Shannon in Women’s Health
Footnotes
Acknowledgements
The authors acknowledge the health workers of the Lower Napo River (LNR) communities who helped facilitate this project, the team of DB Peru volunteers, and Circo and Pilar Petite who provided local care and guidance.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The ABCS Project was funded by a Dining for Women grant.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.