
Abstract
The prevention of intimate partner violence continues to be a high priority for health practitioners and researchers around the world. Screening practices and intervention efforts utilized within high- and/or middle-income areas may not translate effectively to low-resource areas due to differences in financial, social, and physical context. However, little is known about the evidence-base of intervention efforts in such areas. Using the Arksey and O’Malley framework for scoping reviews, the purpose of this review was to synthesize what is known about intimate partner violence screening, management, and treatment in low-resource areas. A total of 31 programs reported across 34 articles were included in this scoping review. The programs incorporated a range of intervention activities, including group-based education and skill-development combined with microfinance to screening and referral to community resources. Slightly less than half of the studies (n = 14) were randomized controlled trials or clustered randomized controlled trials. Many barriers were common across the programs, including limited financial support, lack of community support, and lack of coordination across programs. Despite considerable barriers related to the limited available resources, the literature base had many strengths, such as strong evaluation methodologies, inclusion of a theoretical or conceptual framework to guide the intervention, and community engagement before and during the intervention implementation. However, insufficient statistical power and barriers related to cultural differences or inadequate cultural sensitivity were also common. With a variety of barriers to program implementation noted within the articles, it is important for researchers and practitioners to consider the geographic, social, cultural, and economic contexts when implementing intimate partner violence programs in low-resource areas. Given the significant differences in context across low-resource areas, additional research to establish effective protocols for tailoring and implementing evidence-based programs using a community-engaged framework would be beneficial to future research and practice.
Worldwide, nearly 30% of all women experience physical and/or sexual violence by an intimate partner. 1 The reported lifetime prevalence of intimate partner violence (IPV) is highest among women in low- to middle-income regions that include Africa, the Eastern Mediterranean, and South-East Asia with prevalence rates of 36.6%, 37.0%, and 37.7%, respectively. 1 Comparatively, the high-income regions (including over 20 countries such as Australia, Canada, France, Japan, South Korea, United Kingdom of Great Britain, and the United States of America) and the low- to middle-income regions of Europe and Western Pacific experience IPV prevalence rates of 23.2%, 25.4%, and 24.6%, respectively. 1 A substantial number of physical and psychological outcomes are associated with IPV victimization among women. 2 Beyond the physical health issues directly associated with the experience of violence, 3 IPV victimization may result in poor overall health 4 and specific physical and psychological health conditions.5–9 IPV victimization may also cause significant disability or death. 1 Due to the high prevalence and significant consequences, the prevention of IPV continues to be a high priority for health practitioners and researchers around the world. 10
In light of the high prevalence of IPV across the world, multiple United States-based organizations11,12 have recommended universal screening to assess for the occurrence of IPV, as a way to ultimately reduce violence and improve women’s health. In contrast, the World Health Organization (WHO) acknowledges the wide variation across regions in the prevalence of IPV, laws to protect women, and resources available for prevention and intervention efforts. 13 As such, WHO does not recommend universal screening for IPV at all healthcare encounters and encourages a case-finding approach.
Regardless of using a universal or selected approach, screening is only the first step to addressing IPV victimization. There is little evidence to suggest that screening without referral to resources or programs reduces IPV victimization or improves women’s health and well-being. 14 When support services and/or legal rights for women are limited, screening may actually cause harm. 14 As a result, it may only be appropriate to screen for IPV when evidence-based programs or resources are available. 13 In addition, screening practices and intervention efforts utilized within high- and/or middle-income areas, which represent the majority of the current literature, 14 may not translate effectively to low-resource areas. Thus, it is imperative to understand what screening, management, and treatment efforts are evidence-based and appropriate for low-resource areas worldwide. To the best of our knowledge, there are no existing reviews of screening and intervention efforts focused on IPV victimization in low-resource areas. To address that gap, the purpose of this review is to synthesize what is known about IPV screening, management, and treatment in low-resource areas. The guiding question for this review is, “What screening, management, and treatment programs focused on reducing IPV, including risk and protective factors or related sequela, have been implemented and evaluated in areas with limited resources?”. Several types of reviews were considered to answer this question, including systematic, mapping, qualitative, and scoping reviews. Systematic reviews address a well-defined research question using an exhaustive, comprehensive search framework. To effectively conduct a systematic review, it is necessary to have a sufficient number of high-quality, similar studies in the literature. Mapping reviews focus on broadly categorizing the existing literature around a specific topic, while qualitative reviews highlight themes or constructs from across the literature, frequently focusing on qualitative or mixed-method studies. 15
Scoping reviews focus on the extent, range, and nature of research in the topic area for the purpose of summarizing and disseminating findings, evaluating the feasibility of conducting a systematic review, or identifying gaps in the literature. 16 Scoping reviews include a complete, but not exhaustive, search framework that may include results from both peer-reviewed, empirical research and the gray literature, which includes white papers, evaluation or project reports, government documents, and other sources of information about projects that are not published through traditional commercial or academic processes.15,16 This type of review may include a quality assessment but articles are not excluded as a result of insufficient quality. Scoping reviews are ideal for topics with emerging evidence where it would be difficult to complete a systematic review or meta-analysis. 16
Methods
This review followed the Arksey and O’Malley 17 framework for scoping reviews. First, we identified the specific research question with a focus on determining the aspects of the research question that were most important for the search parameters, including study population and outcome. Next, we identified relevant studies through a systematic search of the literature. Because scoping reviews often include both published and unpublished findings, we searched Google Scholar, a web search engine that indexes scholarly literature across a wide range of formats and disciplines, PsychInfo, and PubMed. Google Scholar included a substantial number of reports, books, and other articles that are less likely to be indexed in archives that focus on peer-reviewed literature. We did not restrict the time span for the search, nor the language. However, the search terms were in English so primarily English language results were returned (Table 1). We also did not restrict the search to male-perpetrated violence against women but found no articles about same-sex IPV. After compiling all studies identified through Google Scholar, PsychInfo, and PubMed, we conducted a multi-stage review of the relevant studies (Figure 1). First, we excluded all duplicate articles. Next, we reviewed the title and abstract to eliminate studies that did not include an intervention and/or evaluation, along with studies that did not include any mention of IPV in the title or abstract. During the second stage, we reviewed the full-text of the articles to eliminate studies that (1) did not include IPV perpetration or victimization, risk or protective factors for IPV perpetration or victimization, or related sequela as an outcome, (2) were not identified by the authors as having been conducted in a limited-resource area, and (3) did not meet the first stage criteria upon closer review (i.e. did not include intervention/evaluation or not relevant to any aspect of IPV). After identifying the relevant articles, we reviewed the bibliographies of the 23 articles that met the inclusion criteria and 27 other articles that were relevant to the topic but did not meet the inclusion criteria (e.g. commentary or study of prevalence of IPV in low-resource area). The 27 articles that did not meet the inclusion criteria were only included in the bibliography search and were not included in the review.
Inclusion criteria and search string.

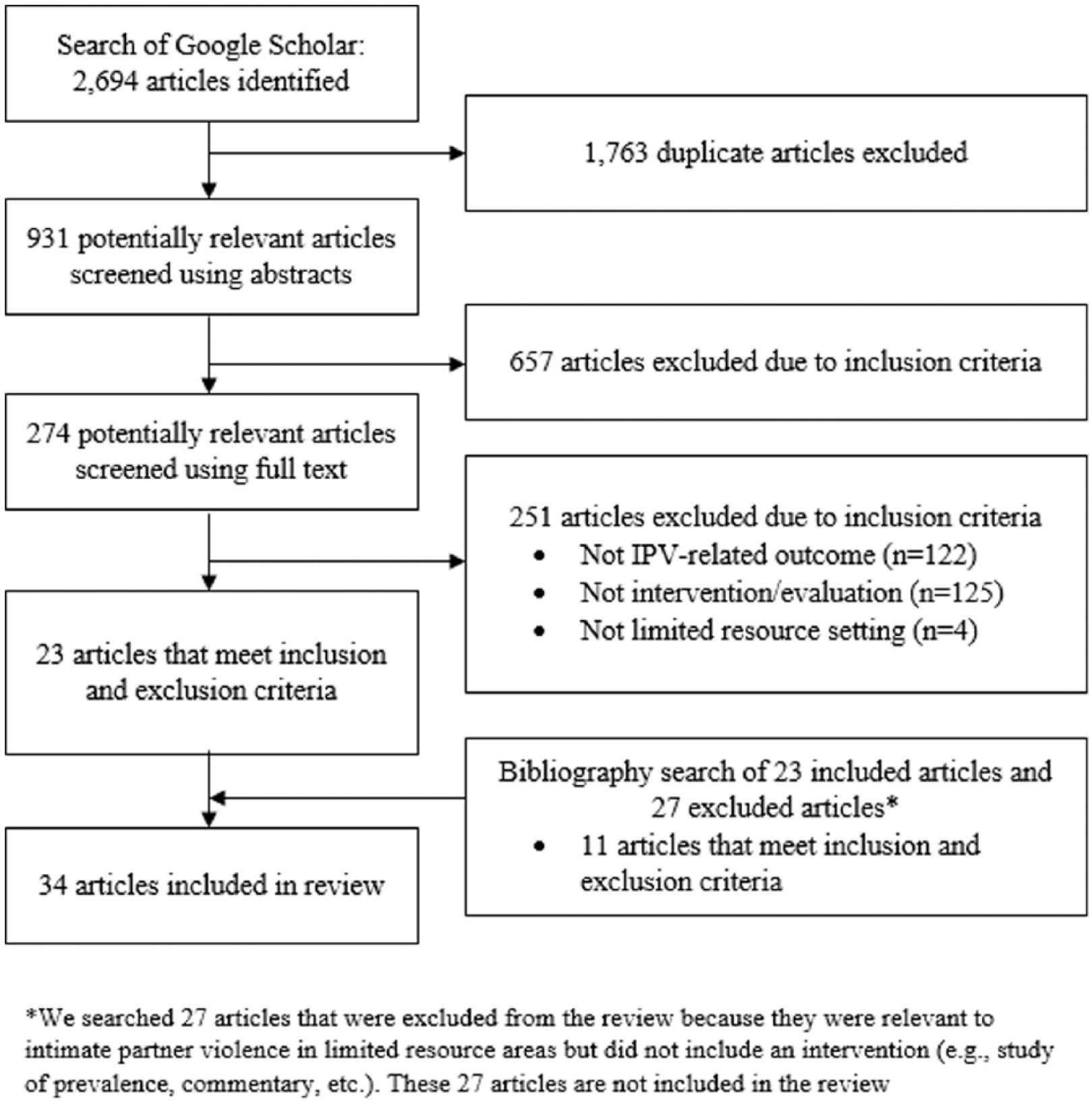
Search process and results.
Next, key information from the 34 articles was charted, with a focus on the type of screening, management, or treatment intervention, study activities, study findings, and important contextual factors. We recorded the following information in Microsoft Excel: authors; year; title of article; intervention sample and location; research/evaluation design; type of intervention; program name; theoretical/conceptual framework; details of the program; targeted outcomes; results; and important contextual factors.
Finally, we used the information collected during the charting stage to provide an overview of the studies relevant to this scoping review. Specifically, we created tables and figures to allow for easy identification of the geographical distribution of the studies (Figure 2), the types of research studies, the theoretical or conceptual framework, sample size, targeted outcomes, and primary intervention activities (Table 2), details for each study, including first author, year, study/intervention sample, brief details of the program, and violence-related outcomes (Table 3), and the violence-related outcomes and the context-specific barriers reported by the authors (Table 4). In the narrative, we provided additional information regarding the program details, results, and important contextual factors.

Geographic distribution of studies included in the review.
Characteristics of studies included in review.

Program details of studies included in the review.

Findings of completed evaluations and barriers to program implementation.

Results
A total of 31 programs reported across 34 articles were included in this scoping review.18–51 These programs targeted low-resource areas across the world, with the majority in Africa (Figure 2). Slightly less than half of the programs (n = 14; 45%) included a randomized controlled trial or clustered randomized controlled trial (Table 2).19,21,22,24,25,28,33,35,36,40,44–47,49–51 Most of the remaining studies were qualitative evaluations26,27,30,37–39,43 or mixed-methods evaluations,18,31,34 and some used a community-based participatory research approach.20,32 The other evaluation designs included quasi-experimental designs, pre/posttest designs, and other non-randomized quantitative designs.23,29,41,42,48 As described by authors of the articles, the majority of interventions were guided by at least one underlying theoretical or conceptual framework or model. Economic theories,23,45,49,50 the social-ecological framework,18,29,40 cognitive-behavioral theories,27,33,34 and participatory frameworks20,36,47 were mentioned by the developers of three programs. The transtheoretical model was used by two program developers.35,44,51 Many other frameworks were mentioned,18,20,24,26,28–30,32,36,43,46–50 including diffusion of innovation, 18 social norm theory, 46 the WHO engagement framework, 34 and feminist theory. 43 Nearly half of all articles did not have a theoretical or conceptual framework specified;19,21,22,25,31,37–39,41,42 although, a framework may have been included in the development of the intervention but not reported in the article. Among studies with available sample sizes (n = 29), there was substantial variability (Table 2). The smallest evaluation was a case study, 32 while the largest included a population-based survey of over 150,000 households. 41 Approximately one-third (n = 10) of the studies had a sample size smaller than 100,20,23,26,27,30,32,37–39,43 while five studies had a sample size larger than 1500.35,40,41,45,47
An equal number of programs had a singular focus on IPV victimization or pereptration,18–20,27–29,32,34,37,38,39,44,46 and a focus on IPV and an additional health issue,21–26,30,31,33,41,42,45 such as reproductive health,24,26 general well-being,21–23,30 and food insecurity. 25 Approximately one-quarter of the studies included a combined focus on IPV victimization, perpetration, risk or protective factors, or sequela and HIV/AIDS.35,36,40,43,47–51 A variety of intervention activities were included in the reviewed studies. Group-based skill-development or education was the most common intervention activity (n = 14, 41.9%).18,24,29,33,35,36,40,42–44,46–50 Screening,19,30,34,35,38,39,51 referral to community resources,19,28,30,31,34,39 and financial or resource support21,22,25,41,44,45,49,50 were also common (n = 6, 19.4% for each activity). Screening and referral activities were commonly conducted in healthcare settings, such as perinatal care clinics34,38 and outpatient care clinics.30,39 The financial or resource interventions took two main forms. In some instances, the government provided cash unconditionally or provided cash based on the completion of certain behaviors. 41 In others, organizations facilitated savings and loans programs44,49,50 or provided an animal that could be raised, bred, and sold.21,22,25 Further details of the location, characteristics, and outcomes of the programs may be found in Table 3.
Overall, many authors reported positive outcomes related to reducing IPV victimization, perpetration, risk or protective factors, or the related sequela (Table 4). Many of the interventions had positive effects on at least one of the identified primary outcomes.20–22,24,26,27,29,31,34,35,37,40,42,43,46,48,51 Some programs had clear, strong impacts on the occurrence of IPV victimization or perpetration. For example, Pigs for Peace, a microfinance program that loaned and supported raising a piglet, showed consistent decreases in IPV rates among intervention households compared with control households.21,22 The Intervention with Microfinance for AIDS and Gender Equality (IMAGE), another microfinance program combined with a gender-focused training and discussion group, showed similar significant decreases in IPV among intervention participants.49,50 Other programs, such as Asociacion de Organizacions por lo Eomocional (ACOPLE), needed additional evaluation to be considered an evidence-based program. 27 ACOPLE used a qualitative evaluation design to examine the perceptions of program effectiveness among providers and found that providers view family violence victimization as a common part of life in the area. At the time of publishing, a quantitative evaluation was on-going, which may provide additional support for the use of the program to reduce trauma symptoms following IPV victimization. Many of the programs, however, had no effect or a combination of positive and negative effects on one or more of their primary outcomes.19,23,30,32,38,39,41,43–47 For example, Bobonis et al. 41 found that the effects of conditional cash transfer on IPV were dependent upon the education of the women’s partners, with increased IPV victimization occurring if the partner’s education was equal to or greater than her partner’s.
Because of the limited resources available for program implementation, many barriers were common across the programs (Table 4). Lack of community support, either as stigma related to receiving services or as community acceptance or ambivalence regarding IPV, was cited as a barrier to implementation in 15 of the programs. In healthcare-based programs, there was some resistance to treating IPV within that system. In some areas, victimization was so common that it was regarded as normal or outside the scope of healthcare practice.23,28,30 In others, there was resistance to discussing IPV or attempting to make change because IPV was consider a private, family issue 49 or part of men’s rights within the family. 43 Several authors reported that lack of logistical support and infrastructure was significant challenges.19,22,26,32,38,39 Lack of coordination across programs, limited financial support for program implementation, and limited availability of existing services for victims were also common. For example, interventions designed to increase screening efforts often encountered barriers with the availability of resources for participants who screened positive for IPV.37–39 It was also frequently difficult for women to follow-up with services after screening due to issues with transportation, time away from work, or stigma associated with being seen by a social worker or in a specific clinic.37–39 Other barriers to implementation included a lack of data to support the need for an intervention, safety and security issues for researchers, response to services that exceeded program capacity, political disturbances, and others.
Discussion
In this scoping review, we assessed what was known about IPV screening, management, and treatment in low-resource areas. The 31 programs (across 34 articles) included in the review represented a variety of interventions, ranging from psychosocial education and discussion groups to microfinance programs and communication campaigns. Despite considerable barriers related to the limited available resources, the literature base had many strengths. First, many of the interventions used strong evaluation methodologies, such as clustered randomized controlled trials and mixed-methods evaluations. This methodological rigor was striking, especially given the likely limited resources available for intervention and evaluation in these areas. However, several of these studies involved well-funded, international partners so rigorous evaluation may have been a requirement for the funding. For example, SASA! 40 was supported by Irish Aid, the Sigrid Rausing Trust, 3ie, an anonymous donor, AusAID, the Stephen Lewis Foundation, American Jewish World Service, HIVOS, and the NoVO Foundation. While SHARE35,51 was supported by the Bill & Melinda Gates Foundation, US National Institutes of Health, WHO, President’s Emergency Plan for AIDS Relief, and the Fogarty International Center. It is unlikely these, and other studies funded by international agencies, represent feasible programs for those working in low-resource areas without well-funded international partners. Finally, several of the interventions explicitly focused on community engagement before and during the intervention implementation, which may have reduced obstacles related to cultural differences between community members and researchers.18,32,34–36,40,43,47,51
Despite the many strengths, there were also several challenges identified in the current literature. Some of the randomized controlled trials potentially lacked sufficient power to detect significant differences between the intervention and control groups. Other programs used evaluation designs that did not allow for clear identification of the effects of the program on the target outcomes. Due to this issue, few of the interventions had clear, strong evidence of effectiveness. Future evaluations in low-resource areas could include mixed-methods components to facilitate better understanding of the underlying processes and changes when insufficient statistical power may be a barrier to the evaluation.
Additionally, several interventions encountered barriers related to cultural differences or inadequate cultural sensitivity. In one instance, all participants at a specific location dropped out of the program in protest of the perceived lack of cultural sensitivity. This event highlighted the importance of community-engaged research and suggests there may be benefit to utilizing a participatory approach where researchers and community members function as partners. This type of approach involves community members, researchers, and program staff in all aspects of the research process in order to allow all partners to contribute expert knowledge and share in the decision-making and implementation of the intervention.
Implications for research and practice
Given the variety of barriers to program implementation noted within the articles included in this review, it may be important for researchers and practitioners to consider the geographic, social, cultural, and economic contexts when implementing IPV programs in low-resource areas. Several articles provided a framework that could be used to develop or adapt interventions to account for the unique physical, cultural, and financial context of various areas around the world. The SHARE intervention in Uganda, for example, used a five-phase approach to tailoring the intervention focused on extended community assessment, raising awareness within the community, networking, intervention implementation, and transfer of intervention activities to community members.35,51 Similarly, an intervention in rural Kenya used a four-stage engagement process that focused on building partnerships, training and engagement of local staff and community leaders, pilot-testing the intervention, and assessing and refining the approach. 34 Although the specific activities of these programs may not be appropriate for other low-resource areas, these community-engaged approaches could be incorporated into other efforts to reduce some implementation barriers, such as community acceptance of the program, researcher safety within the community, and insufficient understanding of the community need for services. Given the substantial differences in facilitating factors and barriers across low-resource areas around the world, additional research to establish effective protocols for tailoring and implementing evidence-based programs would be beneficial.
Researchers and practitioners in the area of IPV may also find it beneficial to work with collaborators in other fields. Many of the interventions in this review targeted IPV in combination with other health issues. For example, HIV/AIDS and IPV frequently co-occur and several interventions used in Africa, such as IMAGE49,50 and SASA!, 40 focused on reducing both health issues in a single intervention, which has the benefit of improving multiple aspects of women’s health while sharing resources. Although it has been particularly effective to combine IPV and HIV/AIDS interventions, other communities may find different local health issues are a priority, and that these health issues are also amenable to combined intervention approaches. If multiple health outcomes are targeted, it is necessary to confirm the intervention does effectively reduce both issues.
Finally, researchers and practitioners in many low-resource areas encountered obstacles to effective intervention implementation as a result of cultural acceptance or ambivalence toward violence against women. As a result, changes to social norms and beliefs may be necessary before substantive individual-level change occurs. The National Center for Injury Prevention and Control at the Centers for Disease Control and Prevention and the Department of Violence and Injury Prevention and Disability of the World Health Organization released a five-prong framework for preventing violence in developing countries. 52 First, an action plan should be developed with objectives, priorities, strategies, and responsibilities. As part of this action plan, a lead organization that has the capacity to engage multiple sectors in the strategy should be identified. Second, local systems for data collection should be identified and, when necessary, enhanced so that data on key indicators are reliably available in the area. Third, specific programs may be implemented and evaluated after the identification of key stakeholders and the development of an action plan. Fourth, health, social, and legal systems to support the victims of violence must be available to reduce the consequences of victimization. Finally, it is critical to engage individuals and agencies across social sectors, including health, criminal justice, and social services, because “the success of violence prevention efforts depend substantially on these sectors being able to cooperate (p. 198).” 52
Limitations
This review had several limitations. First, our review may have missed important articles that were not published in English. Although articles written in languages other than English would have been considered for the review, the English language search terms substantially reduced the number of returned articles in languages other than English. This limitation is common among reviews conducted by researchers from majority native English-speaking countries; yet, it may be particularly problematic in this instance due to the focus of the review. Nearly all articles found through the search process used in this review were published in English, and despite the interventions being carried out in low-resource areas, the majority of articles were written by academic partners from high-income countries, including the United States and the United Kingdom, rather than local researchers and practitioners. Thus, it was likely that all possible relevant articles were not noted in this review, and that the programs reported in this review were not representative of programs conducted by locals who did not have the resources or English language proficiency to publish findings. Second, it was possible to define low- and limited-resource settings in various ways. We relied on the authors of each article or of other commentaries or reviews to indicate whether the intervention applied to individuals residing in low-resource areas. Other definitions could result in a somewhat different literature base for review. A definition focused on specific geographical areas or low- to middle-income countries may be an alternate way to assess low- or limited-resource settings. However, resource allocation is rarely homogeneous across countries. For example, India is classified as a lower middle-income country by the World Bank, 53 but there are substantial disparities in resources, such as availability of education 54 and access to healthcare, 55 across geographical region and urbanicity. As such, a focus on specific geographical areas or low- to middle-income countries would likely result in the inclusion of programs implemented in areas with sufficient resources. Finally, the intentionally broad search framework resulted in the inclusion of a variety of intervention outcomes and research designs, which prevented comparisons of effectiveness across studies. However, as previously noted, the purpose of a scoping review is to survey the landscape and provide a summary of information on the extent, range, and nature of research with respect to a focused topic, as well as to identify gaps in the literature. As also noted, scoping reviews are ideal for topics with emerging evidence, such as the implementation and evaluation of screening, management, and treatment programs focused on IPV prevention or intervention in low-resource areas.
Conclusion
The results of this scoping review provided an overview of the characteristics of screening, management, and treatment activities conducted in low- or limited-resource areas around the world. Many of these programs have been evaluated using a rigorous research design, although statistical power to detect effects was often limited. Additional research into the development of culturally sensitive, community-engaged intervention processes may allow the existing evidence-based interventions to be appropriately tailored to other low- or limited-resource areas around the world.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.