
Abstract
Background:
Violence against women is a serious human rights violation and a public health problem. In Peru, more than 55% of women have suffered intimate partner violence (IPV), which has a negative impact on their health and breastfeeding.
Objective:
To evaluate the association of IPV and early initiation of breastfeeding (EIBF) in Peruvian women.
Design:
Cross-sectional study.
Methods:
A secondary analysis was conducted using data from the Demographic and Family Health Survey (ENDES) of the period 2018–2022. The population included women of reproductive age (15–49 years). The outcome variable was the EIBF, and the main predictor variable was IPV. Crude prevalence ratios and adjusted prevalence ratios were estimated as a measure of association.
Results:
We analyzed a final sample of 30,482 women. The prevalence of IPV was 16.25%, while the prevalence of mothers who did not initiate early breastfeeding was 33.37%. It was found that partner violence was associated with a lower likelihood of complying with EIBF.
Conclusion:
We identified that women who experienced IPV were less likely to initiate early breastfeeding.
Plain language summary
Being a victim of intimate partner violence can have lasting negative effects on women’s health, including their breastfeeding practices. This study explores the relationship between partner violence and early initiation of breastfeeding among Peruvian women. Using data from the Demographic and Family Health Survey of Peru between 2018 and 2022, the experiences of over 30,000 women were analyzed to determine if partner violence was associated with the likelihood of early breastfeeding initiation. The study found that women who experienced partner violence were less likely to initiate breastfeeding early. Around 16% of women reported experiencing partner violence, and of these, a significant proportion did not start breastfeeding within the first hour after birth. Understanding this connection is crucial for developing interventions that support women in overcoming the effects of violence and promote healthy breastfeeding practices.
Introduction
Violence against women is a serious violation of human rights and a public health issue rooted in gender inequality. 1 Among its various forms, intimate partner violence (IPV) is the most common, 2 and is defined as “a behavior within an intimate relationship that causes physical, psychological, or sexual harm.” 3 Some women are subjected to multiple forms of IPV, including psychological, physical, and sexual violence. Exposure to two or more of these forms is referred to as polyvictimization. 4 According to the World Health Organization (WHO), in 2018, over 640 million women were subjected to IPV. 2
Peru is a middle-income country located in Latin America, characterized by notable geographic, ethnic, and socioeconomic diversity, as well as persistent gender inequalities. Despite national legislation and public campaigns against gender-based violence, IPV remains highly prevalent. The 2022 Peruvian Demographic and Family Health Survey (ENDES, by its Spanish acronym) reported that more than 55% of women had experienced violence from their partner or husband at some point in their lives. 5 In terms of maternal and child health, policies promoting breastfeeding have been implemented, yet disparities remain: early initiation of breastfeeding (EIBF) and exclusive breastfeeding (EBF) rates vary widely between urban and rural areas, and among different regions and income levels. According to ENDES 2020, less than half of postpartum women initiated EIBF, and around 70% of children under 6 months of age were breastfed. 6
It is important to differentiate between EIBF and EBF. EIBF, defined as the initiation of breastfeeding within the first hour after birth, is essential for neonatal survival due to the protective factors present in colostrum, which provide both passive and active immunity against infections.7,8 A systematic review found that, compared to infants who began breastfeeding within the first hour, those who initiated between 2 and 23 h after birth had a 33% higher risk of neonatal mortality, while those who began after 24 h had a 2.19 times higher risk. 9 EBF, on the other hand, refers to feeding the infant only breast milk, without water, other liquids, or solid foods, for the first 6 months of life. 8 Although both are critical for child health, they are distinct indicators and do not necessarily occur together. For example, a mother may initiate breastfeeding within the first hour but later supplement the infant’s diet with other liquids, thereby not meeting the definition of EBF. Analyzing both indicators independently allows for the capture of complementary dimensions of maternal behaviors. EIBF mainly reflects immediate factors associated with childbirth, the hospital environment, and perinatal care, 10 while EBF depends on social, psychological, and structural determinants that condition the continuity and sustainability of this practice over time. 11
Several studies have examined the relationship between IPV and breastfeeding practices. A population-based analysis of surveys from 51 low- and middle-income countries found that exposure to IPV was associated with a lower likelihood of EIBF, although the strength of the association varied by region and type of violence. 12 Other research has similarly found that IPV is linked to negative breastfeeding outcomes, such as delayed initiation, reduced intention to breastfeed, and shorter duration of EBF, particularly when multiple forms of violence are present.13,14
The link between IPV and breastfeeding practices could be explained from different perspectives. First, the social determinants of the health model suggest that structural conditions, such as poverty, gender inequality, and limited access to health care, shape both exposure to IPV and maternal health behaviors. 15 In the Peruvian context, women exposed to IPV often face reduced autonomy, limited decision-making power, and financial dependence, 16 which can hinder EIBF and EBF. Second, attachment theory helps explain how IPV disrupts emotional security, leading to impaired maternal–infant bonding. 17 IPV may cause psychological distress, depression, or anxiety,18,19 reducing a mother’s sensitivity and responsiveness to her newborn.20–22 Finally, Bronfenbrenner’s ecological model frames IPV as a phenomenon influenced by multiple levels, individual, interpersonal, community, and societal. 23 For instance, partner control and social norms that tolerate violence can limit a woman’s ability to access health services, whether through stigma, fear, or coercion, 24 reducing their maternal decision-making capacity and affecting neonatal health through prematurity or low birth weight, 25 which can delay or interrupt EBF.
Even though the association between IPV and EIBF has been established globally, its expression and strength vary considerably by region, likely due to cultural, healthcare, and policy differences. 12 In Peru, IPV remains highly prevalent and has been consistently linked to poor maternal mental health outcomes. 16 These psychological consequences are well-known to interfere with maternal caregiving behaviors and breastfeeding practices.24,26,27 However, despite this documented burden, no recent national analyses have explored the relationship between IPV and EIBF using updated Peruvian data. Moreover, previous multicountry studies that included Peru rely on outdated surveys and fail to reflect the current policy landscape, including national efforts to promote optimal breastfeeding. 28 This lack of local evidence represents a critical gap, especially considering the persistent IPV rates and the suboptimal coverage of EIBF in the country. 29
Based on this evidence, we hypothesize that IPV, whether in any form (psychological, physical, sexual) or as polyvictimization, is associated with a lower probability of EIBF among Peruvian women. Therefore, this study aims to evaluate the association of IPV and EIBF in the Peruvian context, considering the specific forms of violence and polyvictimization. Additionally, as a secondary objective, we explore the association between IPV and EBF during the first 6 months of life.
Methods
Study design
This study is based on a secondary analysis of data collected by ENDES in Peru between 2018 and 2022. The ENDES is conducted annually by the National Institute of Statistics and Informatics of Peru (INEI). It includes three separate questionnaires (household, individual, and health), with the main objective of providing up-to-date information on the health indicators of the Peruvian population. For this study, we used all three questionnaires. 30
The ENDES uses a two-stage, stratified, probability sampling design, designed to ensure representativeness at the national and regional levels and by urban and rural areas. In the first stage, primary sampling units, which generally correspond to census clusters, are selected using a probability method proportional to population size. In the second stage, households within each primary sampling units are selected systematically and randomly. This process ensures a balanced and representative sampling, adapted to the population characteristics of each geographic domain (Metropolitan Lima, rest of the coast, highlands, and jungle). 30 The report of this study is in line with the STROBE statement (Supplementary Material). 31
Study population and sample
The population consisted of 103,924 women of reproductive age (WRA) between 15 and 49 years old. For this study, we considered WRA who were married or cohabitating, had at least one child aged 6 months or older at the time of the survey, and had been selected and interviewed for the domestic violence module of the individual questionnaire. Thus, women who only had children under 6 months of age (n = 7707) and who were neither married nor cohabiting (n = 15,701) were excluded from the analysis. On the other hand, women with missing information in the outcome variables (n = 33,572) or in relevant covariates (n = 16,462) were excluded. The effective sample size for our study consisted of 30,482 women, representing an expanded population of 2,575,975 (Figure 1). A statistical power analysis was conducted and indicated that the available sample size provided 100% power to detect statistically significant associations between IPV and EIBF, assuming an alpha of 0.05 and the observed effect size, which guarantees the ability to detect significant associations between IPV and the EIBF.

Flowchart of sample selection included in the study, ENDES 2018–2022.
Variables
Outcome variable
The outcome variables were EIBF and EBF, both treated as dichotomous (Yes/No) variables. In this study, EIBF was operationalized using the question: “How long after (NAME) was born did you start breastfeeding?” Following the WHO criteria, EIBF was defined as initiation of breastfeeding within the first hour after birth. 32 Responses indicating initiation within 1 h were coded as “Yes,” whereas initiation after 1 h was coded as “No.” Meanwhile, EBF was defined as EBF during the first 6 months, without any additional liquids or foods, and was generated using the question: “During the first 6 months of life, did (NAME) receive only breast milk, without including other foods or liquids?”
Although both EIBF and EBF reflect important aspects of breastfeeding behavior, they represent conceptually and temporally distinct behaviors. EIBF reflects the EIBF and exclusive consumption of breast milk within the first hour after birth, capturing the mother’s ability to start breastfeeding promptly and provide early immunological protection to the newborn. EBF, in contrast, reflects the continuation of EBF for the first 6 months of life, assessing adherence to optimal feeding practices over a prolonged period. A mother may initiate breastfeeding early but introduce other liquids or foods before 6 months, and, conversely, a mother who delays initiation may still practice EBF later.
Predictor variables
The main predictor variable was IPV, which was categorized into four subtypes: (i) psychological, (ii) physical, (iii) sexual, and (iv) any type of IPV, defined as a positive response to any of these questions. Additionally, we considered a fifth variable, polyvictimization, defined as exposure to two or more types of IPV (4), and categorized into four groups: (i) No violence, (ii) Only one type of violence, (iii) Two types of violence, and (iv) Three types of violence.
Psychological violence was assessed using the following three questions:
Your (last) spouse (partner) ever:
D103A: Said or done things to humiliate you in front of others?
D103B: Threatened to hurt you or someone close to you?
D103C: Threatened to leave the house, take away your children or financial support?
Physical violence was evaluated through the following seven questions:
Your (last) spouse (partner) ever:
D105A: Pushed, shook, or threw anything at you?
D105B: Slapped you or twisted your arm?
D105C: Hit you with a fist or something that could hurt you?
D105D: Kicked or dragged you?
D105E: Tried to strangle or burn you?
D105F: Attacked/attacked you with a knife, gun, or other weapon?
D105G: Threatened you with a knife, gun, or other weapon?
Sexual violence was assessed with the following two questions:
Your (last) spouse (partner) ever:
D105H: Used physical force to force you to have sex even though you did not want to?
D105I: Forced you to perform sexual acts of which you do not approve?
Other variables
Additionally, other covariates were included as confounders based on previous studies, including maternal age (15–25, 26–35, and 36–49 years), maternal education level (complete elementary education or below, high school, non-university higher education, or university education), and marital status (live-in-partner only or married). Socioeconomic and contextual factors comprised wealth index (very poor, poor, medium, high, or very high), area of residence (urban or rural), geographical region of residency (Metropolitan Lima, rest of the coast, highlands, or jungle), and maternal ethnicity (mestizo, Quechua, Aymara, native of the Amazon, part of another people, Black/Brown/Zambo/Mulatto/Afro-Peruvian or Afro-descendant, White, and other races). Other covariates included health insurance coverage (yes or no), number of children (1, 2, 3, 4, or more), and partner alcohol consumption (yes or no).
Furthermore, delivery- and health service-related variables were included: antenatal care (inadequate or adequate), place of delivery (institutional or home delivery), type of delivery (vaginal or cesarean), and breastfeeding training (yes or no).
The specific ENDES questions used for each variable are detailed in Supplementary Material .
Statistical analysis
The ENDES database for the period between 2018 and 2022 was downloaded in SAV format and analyzed using STATA version 16.0 (StataCorp, College Station, TX, USA). All the analyses accounted for the complex sampling design of ENDES by applying the svy command, incorporating stratification, clustering, and sampling weights.
Categorical variables were described using absolute frequencies and weighted proportions. Maternal age, the only continuous variable, was summarized using the mean and 95% confidence intervals (95% CI). For the bivariate analysis, the Rao–Scott adjusted chi-square test (which corrects for complex survey design) was used to examine associations between IPV, both overall and by type (psychological, physical, sexual, and polyvictimization), and each of the two outcomes.
Subsequently, generalized linear regression models using a Poisson distribution were conducted to evaluate the association between IPV and each of the outcome variables (EIBF and EBF). This modeling approach was selected because it allows for the direct estimation of prevalence ratios, which are more appropriate than odds ratios when the outcome is common (i.e., prevalence exceeds 10%). For each analysis, both crude and adjusted prevalence ratios (aPRs) were calculated, along with their 95% CI and p-values. The adjusted models included the following covariates selected based on prior literature and theoretical relevance: maternal age, educational level, marital status, wealth index, area and region of residency, maternal ethnicity, number of children, and partner’s alcohol consumption. A p-value of less than 0.05 was considered statistically significant.
Ethics approval and consent to participate
This study used publicly available data from the INEI website (http://iinei.inei.gob.pe/microdatos/). Participant confidentiality is ensured due to the absence of information that could identify them. In the original surveys, all the participants provided verbal informed consent. This consent included a statement outlining the purpose, procedures, and voluntary nature of participation in the survey. For individuals under 18, interviews were conducted only after obtaining verbal consent from the participant and approval from a parent or guardian present. As this is a secondary analysis of anonymized data, no additional ethical approval or new consent for participation was required for this study.
Results
Characteristics of the study population
The average age was 30.38 (30.28–30.48) years, with the majority aged between 26 and 35 years (50.46%). Of the participants, 49.76% received secondary education and 76.13% were cohabiting. Most women had health insurance coverage at 86.96% and lived in urban areas at 65.21%. Regarding socioeconomic status, 33.58% were classified as very poor. In terms of ethnicity, 43.74% identified as mestizo, and 34.50% resided in the Highlands. Adequate antenatal care was reported by 52.82% of participants, 92.13% delivered in a health institution, and 81.76% had a vaginal delivery. Breastfeeding training was reported by 73.75% of participants. The overall prevalence of IPV was 16.25%, with psychological, physical, and sexual violence reported by 11.99%, 9.71%, and 2.06% of participants, respectively. Additionally, 33.37% of women did not initiate EIBF and 28.87% did not adhere to EBF (Table 1).
General characteristics of the sample included in the analysis, ENDES 2018–2022 (n = 30,482; N = 2,575,975).

95% CI: 95% confidence intervals.
Weights and the design effect of the complex survey sampling were included.
Bivariate analysis according to IPV of any type
In the bivariate analysis, statistically significant differences were observed in both EIBF and EBF according to the occurrence of any type of IPV. Women exposed to IPV had a lower prevalence of EIBF (63.77% versus 67.18%) and EBF (67.12% versus 71.91%) compared with unexposed women (p < 0.001 for both). Regarding other covariates, women who experienced any type of IPV had a higher proportion of higher educational attainment compared with those who were not exposed (p < 0.001). In addition, a higher proportion of cohabiting women (p < 0.001) and women in the lowest wealth quintile (p < 0.001) were found among those who experienced IPV. Women exposed to IPV were also more likely to reside in the Highlands region (p = 0.013) and to belong to ethnic minority groups compared with unexposed women (p < 0.001). With respect to maternal healthcare and delivery-related variables, women who experienced IPV were less likely to have received adequate antenatal care (p < 0.001) and breastfeeding training (p < 0.001). Significant differences were also observed in place of delivery, with a higher proportion of institutional deliveries among IPV-exposed women (p = 0.002). No statistically significant differences were observed in type of delivery between women exposed and not exposed to IPV (p = 0.687). Finally, IPV exposure was significantly associated with health insurance coverage, number of children, and partner’s alcohol consumption (Table 2).
General characteristics of the sample included in the study according to the presence of intimate partner violence.

Weights and the design effect of the complex survey sampling were included.
Bold values indicate statistically significant differences (p < 0.05).
Refers to the statistical significance obtained from the comparison of the proportions between the categories of the variables considering the complex sampling of the survey.
Psychological and physical violence showed significant differences in the proportions of EIBF and EBF, with lower frequencies among exposed women, whereas sexual violence showed differences only for EBF but not for EIBF. Differences were also observed across several sociodemographic and obstetric characteristics, while no significant differences were found according to type of delivery ( Supplementary Material ).
Bivariate analysis according to early initiation of breastfeeding
In the bivariate analysis, EIBF was significantly associated with exposure to IPV, with a lower prevalence among women who experienced any type of IPV compared with those who did not (p < 0.001). Significant relationships were also observed for psychological and physical IPV, as well as polyvictimization. An inverse gradient was identified, whereby higher maternal age, educational level, and wealth index were associated with lower EIBF prevalence. Lower EIBF prevalence was also observed among women living in urban areas, particularly in Metropolitan Lima, those without health insurance, and those with only one child. Regarding healthcare- and delivery-related factors, EIBF prevalence was higher among women who delivered at home, had a vaginal delivery, and reported having received breastfeeding training, whereas no significant differences were observed according to antenatal care (Table 3).
General characteristics of the sample included in the study according to exclusive breastfeeding compliance.

Weights and the design effect of the complex survey sampling were included.
Bold values indicate statistically significant differences (p < 0.05).
Refers to the statistical significance obtained from the comparison of the proportions between the categories of the variables considering the complex sampling of the survey.
Similarly, EBF was significantly associated with exposure to any type of IPV, as well as psychological, physical, and sexual violence (p < 0.001 for all). The prevalence of EBF decreased with increasing levels of polyvictimization, from 71.9% among women with no IPV exposure to 63.6% among those exposed to all three types (p < 0.001). Regarding sociodemographic factors, lower EBF prevalence was observed among older women, those with higher educational level, higher wealth index, urban residence (particularly in Metropolitan Lima), and among women without health insurance. In addition, EBF prevalence was lower among women with fewer children. With respect to healthcare- and delivery- related factors, EBF prevalence was higher among women who delivered at home, had vaginal delivery, and reported having received breastfeeding training (Table 3).
Association between intimate partner violence and early initiation of breastfeeding
In the multivariate analysis, exposure to any type of IPV was associated with a lower prevalence of EIBF (aPR: 0.93; 95% CI: 0.90–0.96; p < 0.001). Similarly, psychological violence (aPR: 0.94; 95% CI: 0.91–0.97; p < 0.001) and physical violence (aPR: 0.91; 95% CI: 0.88–0.94; p < 0.001) were significantly associated with a lower prevalence of EIBF. No statistically significant association was observed between sexual violence and EIBF after adjustment. Regarding polyvictimization, exposure to one or two types of IPV was associated with a lower prevalence of EIBF, whereas exposure to all three types of violence was not statistically significant in the adjusted model (Table 4).
Crude and adjusted regression models to evaluate the association between intimate partner violence and early initiation of breastfeeding in the sample included in the analysis.

PR: prevalence ratio; 95% CI: 95% confidence intervals.
Bold values indicate statistical significance (p < 0.05).
A generalized linear model of the Poisson family with a log link was made considering the effect of the design and the weights of the complex sampling of the survey.
Adjusted for age, education level, current marital status, wealth index, area of residence, geographic region of residency, maternal ethnicity, number of children, and partner’s alcohol consumption.
Association between IPV and exclusive breastfeeding
Regarding EBF, the multivariate analysis showed that exposure to any type of IPV was associated with a lower prevalence of EBF (aPR: 0.92; 95% CI: 0.90–0.95; p < 0.001). Similar associations were observed for psychological violence (aPR: 0.92; 95% CI: 0.89–0.95; p < 0.001), physical violence (aPR: 0.93; 95% CI: 0.90–0.97; p < 0.001), and sexual violence (aPR: 0.90; 95% CI: 0.83–0.96; p = 0.003). With respect to polyvictimization, compared with women who experienced no IPV, those exposed to one type of violence (aPR: 0.92; 95% CI: 0.89–0.96; p < 0.001), two types of violence (aPR: 0.94; 95% CI: 0.90–0.98; p = 0.006), and all three types of violence (aPR: 0.85; 95% CI: 0.77–0.94; p = 0.002) had a lower prevalence of EBF (Table 5).
Crude and adjusted regression models to evaluate the association between intimate partner violence and exclusive breastfeeding in Peruvian women.
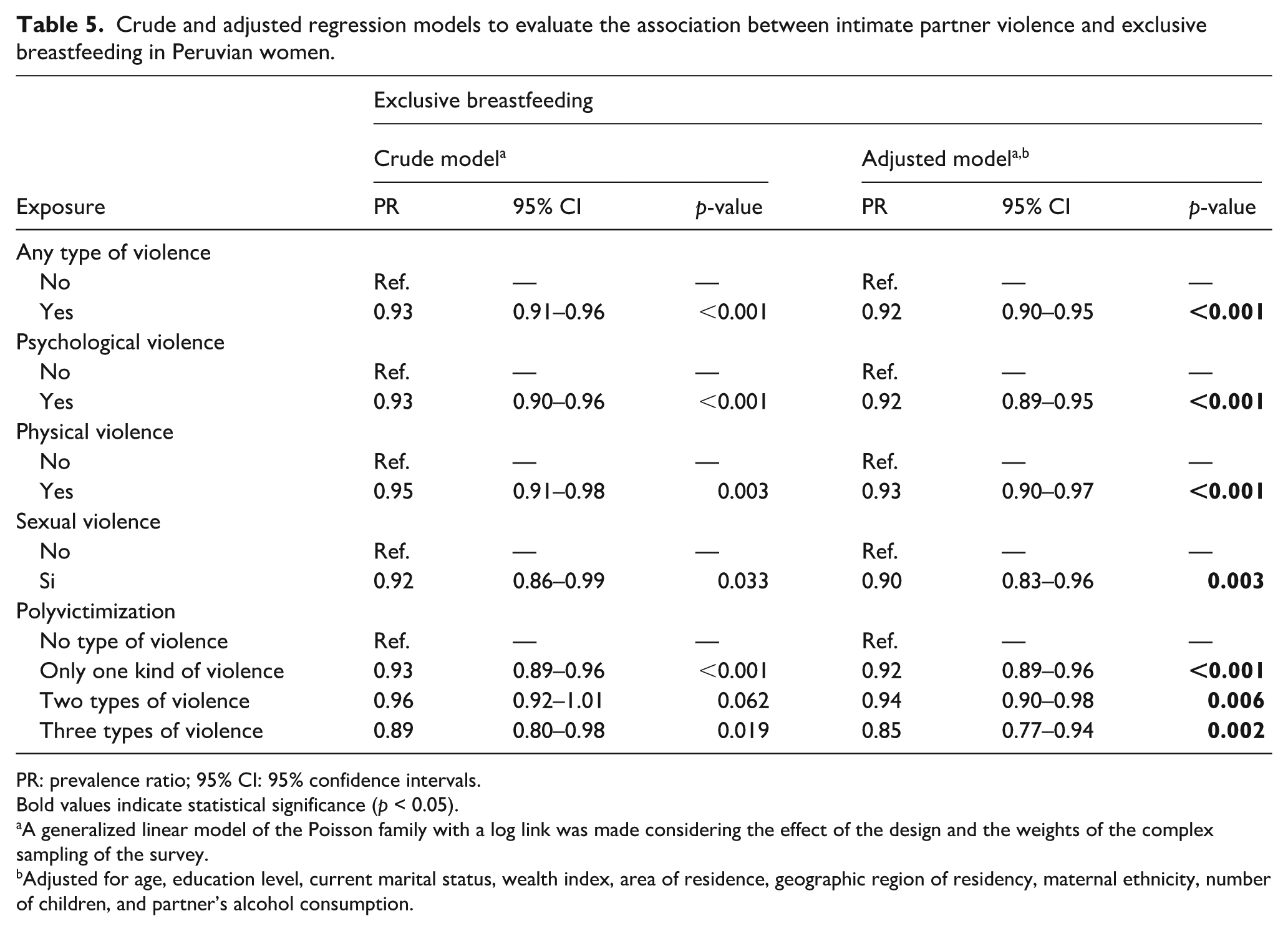
PR: prevalence ratio; 95% CI: 95% confidence intervals.
Bold values indicate statistical significance (p < 0.05).
A generalized linear model of the Poisson family with a log link was made considering the effect of the design and the weights of the complex sampling of the survey.
Adjusted for age, education level, current marital status, wealth index, area of residence, geographic region of residency, maternal ethnicity, number of children, and partner’s alcohol consumption.
Discussion
Main findings
Our main findings indicate that exposure to IPV was associated with a lower prevalence of EIBF. Specifically, IPV of any type, as well as psychological and physical violence, was significantly associated with a lower prevalence of EIBF after adjustment. In contrast, no statistically significant association was observed between sexual violence and EIBF. For polyvictimization, reduced EIBF prevalence was evident among women exposed to one or two IPV types, whereas this association was not observed among those exposed to all three types of violence.
In contrast, EBF showed a more consistent pattern. Exposure to any type of IPV, its specific forms (psychological, physical, and sexual violence), and polyvictimization were all significantly associated with a lower prevalence of EBF. These findings suggest that IPV may exert a stronger influence on the continuity of breastfeeding over time than on the EIBF after birth.
Intimate partner violence and early initiation of breastfeeding: comparison with other studies
We found that IPV affects EIBF. Similar to our findings, other studies have reported comparable conclusions related to the association between IPV and EIBF. One study evaluated demographic and health surveys conducted in 51 low- and middle-income countries, over half of which were from African nations and only two (Peru and Colombia) were from the Western Pacific region. 12 Their findings indicate that mothers experiencing IPV were less likely to present EIBF compared to mothers not exposed to any type of IPV. 12
Because IPV encompasses various types that can independently influence EIBF or occur concurrently, some studies have evaluated their association with EIBF. For instance, in the study that included 51 low- and middle-income countries, all types of IPV were linked to lower likelihood of EIBF. 12 In contrast, a study in Cameroon found that emotional and sexual violence were significantly associated with lower probabilities of EIBF but not physical violence. 33 Additionally, another investigation in India found no association between IPV and EIBF. 34
The results may be influenced by factors associated with EIBF, such as history of cesarean sections, birth weight, birth order, and economic status.35,36 Additionally, cultural factors that vary across different regions within the same country may affect this association based on the region of residence, 36 which we evaluated collectively. Another aspect to consider is that we excluded from our analysis pregnant women who did not report data on partner violence or breastfeeding practices, as they may have been more likely to engage in non-recommended breastfeeding practices and marginally more likely to be exposed to any type of IPV, which could limit the analysis of this association.
Intimate partner violence and exclusive breastfeeding: comparison with other studies
Our findings indicate that any form of IPV, including psychological, physical, and sexual violence, as well as polyvictimization, was associated with a lower prevalence of EBF. This suggests that IPV may have a stronger influence on the continuation of breastfeeding rather than on its early initiation, particularly when multiple forms of violence coexist. This interpretation is supported by previous evidence. A systematic review that included 12 observational studies (mostly cross-sectional) found that women exposed to emotional, physical, or sexual IPV were more likely to report lower breastfeeding intention, delayed initiation, and early cessation of EBF before 6 months of age, despite heterogeneity in measurement approaches. 13 Similarly, another review that synthesized 16 studies similarly found that IPV exposure was associated with reduced breastfeeding duration and early termination of EBF in a substantial proportion of studies. 14 Despite variability in methodological quality, these studies consistently indicate a negative association between IPV exposure and sustained breastfeeding practices, in line with our results.
Interpretation of results
The associations observed in this study may be partly explained by psychosocial and health service-related pathways. In our analysis, women exposed to IPV were less likely to receive adequate antenatal care and breastfeeding training, suggesting reduced engagement with maternal health services. This pattern is consistent with evidence indicating that women experiencing IPV often face social isolation, limited family support, and strained interactions with healthcare providers, which may hinder access to timely and effective prenatal care.37–40 Given that prenatal care represents a critical opportunity for breastfeeding counseling, these barriers may contribute to suboptimal breastfeeding practices. In addition, the lower prevalence of EBF among women exposed to IPV may reflect the emotional and psychological consequences of violence. There is evidence in Peru that IPV is associated with depressive symptoms, which are independently linked to the ability to continue breastfeeding.41,42 Moreover, IPV affects a mother’s self-esteem and confidence, which are also associated with lower probabilities of initiating breastfeeding. This can undermine the emotional bond between the mother and child, further complicating the initiation of breastfeeding. 33 Together, these findings suggest that the impact of IPV on breastfeeding operates through intertwined social, emotional, and health system pathways, reinforcing the importance of addressing IPV within maternal and child health services.
Implications
Our findings may have important public health implications and suggest the potential value of implementing interventions to reduce IPV, although these should be considered with caution given the observational nature of the study. In this regard, there is evidence of the effectiveness of community interventions that significantly reduce IPV, with participants also reporting lower probabilities of endorsing IPV after engaging in community-based violence prevention initiatives. 43 These programs often operate through mechanisms such as improved communication, conflict resolution, reflection on harmful gender norms, and awareness of the adverse consequences of partner violence and violence against children. 44 Therapeutic programs for women and children exposed to partner violence have facilitated participation in trauma-related discussions, increased awareness of the effects of partner violence, and promoted avoidance of unhealthy relationships. 44 Furthermore, there is evidence of the effectiveness of digital interventions to mitigate IPV as a complement to traditional modalities, employing a coordinated response strategy. 45 In Peru, regulatory documents from the Ministry of Health (MINSA), such as the “Technical Guide for the Mental Health Care of Women Experiencing Violence from a Partner or Ex-Partner,” published in 2021, reflect efforts to strengthen mental health services for women experiencing partner violence and have incorporated several of these recommended approaches. 46
Limitations
Our study has several limitations. First, the study’s cross-sectional design makes it impossible to establish causal relationships between IPV and EIBF. Second, since the data were based on participants’ recollections, memory bias may have occurred, and, due to the sensitive nature of IPV, responses may have been influenced by social desirability. Third, the use of self-reported information, while valuable for understanding personal experiences, may underestimate the true prevalence of violence due to fear, stigma, or omission of certain facts. Fourth, the study did not consider the severity of IPV, which may have excluded women exposed to more severe forms of violence, and relied on a secondary database that, although robust, did not include all relevant determinants of EIBF. Finally, it is important to acknowledge the absence of some clinical, obstetric, and contextual variables, such as maternal mental health, autonomy, resilience, and women’s access to health information and services, which may have influenced the associations observed. Future research should address these issues to achieve a more comprehensive understanding of the complex relationship between IPV and breastfeeding practices.
Conclusion
In conclusion, our results suggest that experiencing any type of IPV is associated with a lower likelihood of EIBF. This highlights the importance of addressing IPV in interventions aimed at promoting maternal and infant health. Reducing IPV could mitigate delays in EIBF, which, in turn, may help lower child mortality rates.
Supplemental Material
sj-docx-1-whe-10.1177_17455057261424821 – Supplemental material for Intimate Partner Violence and Early Initiation of Breastfeeding: Evidence from the Peruvian Demographic and Family Health Survey
Supplemental material, sj-docx-1-whe-10.1177_17455057261424821 for Intimate Partner Violence and Early Initiation of Breastfeeding: Evidence from the Peruvian Demographic and Family Health Survey by Jennyfher R. Toro-Vera, Jerry K. Benites-Meza, Christopher J. Alarcón-Toro, Andrea A. Aldea-García, Liseth Pinedo-Castillo, Carlos J. Zumaran-Nuñez, Percy Herrera-Añazco and Vicente A. Benites-Zapata in Women's Health
Supplemental Material
sj-docx-2-whe-10.1177_17455057261424821 – Supplemental material for Intimate Partner Violence and Early Initiation of Breastfeeding: Evidence from the Peruvian Demographic and Family Health Survey
Supplemental material, sj-docx-2-whe-10.1177_17455057261424821 for Intimate Partner Violence and Early Initiation of Breastfeeding: Evidence from the Peruvian Demographic and Family Health Survey by Jennyfher R. Toro-Vera, Jerry K. Benites-Meza, Christopher J. Alarcón-Toro, Andrea A. Aldea-García, Liseth Pinedo-Castillo, Carlos J. Zumaran-Nuñez, Percy Herrera-Añazco and Vicente A. Benites-Zapata in Women's Health
Supplemental Material
sj-docx-3-whe-10.1177_17455057261424821 – Supplemental material for Intimate Partner Violence and Early Initiation of Breastfeeding: Evidence from the Peruvian Demographic and Family Health Survey
Supplemental material, sj-docx-3-whe-10.1177_17455057261424821 for Intimate Partner Violence and Early Initiation of Breastfeeding: Evidence from the Peruvian Demographic and Family Health Survey by Jennyfher R. Toro-Vera, Jerry K. Benites-Meza, Christopher J. Alarcón-Toro, Andrea A. Aldea-García, Liseth Pinedo-Castillo, Carlos J. Zumaran-Nuñez, Percy Herrera-Añazco and Vicente A. Benites-Zapata in Women's Health
Footnotes
Acknowledgements
None.
ORCID iDs
Ethical considerations
This study was based on publicly available, anonymized data obtained from the INEI website (![]() ). The database does not contain any information that allows identification of participants, thereby ensuring confidentiality and privacy. As this research involved secondary analysis of de-identified data, no additional ethical approval was required according to national regulations and institutional policies governing research using publicly accessible datasets.
). The database does not contain any information that allows identification of participants, thereby ensuring confidentiality and privacy. As this research involved secondary analysis of de-identified data, no additional ethical approval was required according to national regulations and institutional policies governing research using publicly accessible datasets.
Consent to participate
In the original surveys conducted by INEI, verbal informed consent was obtained from all participants prior to data collection. The consent process included an explanation of the study objectives, procedures, and the voluntary nature of participation. For individuals younger than 18 years, interviews were conducted only after obtaining verbal assent from the participant and authorization from a parent or legal guardian who was present at the time of the interview. Given that the present study is a secondary analysis of anonymized data, no new consent to participate was required.
Consent for publication
Not applicable.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.