
Abstract
Background:
One-third of U.S. women report experiencing intimate partner violence (IPV), which has been linked to negative mental health outcomes such as depression, anxiety, posttraumatic stress, and substance use problems. Sociocultural factors make women of color especially vulnerable to experiencing IPV and barriers to overcoming it; one particularly vulnerable group is Latinas. IPV-exposed Latinas who seek help may face language barriers, racism and discrimination, and a shortage of bilingual/bicultural mental health professionals. Digital tools, however, may be a useful alternative to face-to-face services for this population. Digital IPV interventions are scarce; they focus primarily on the prevention and reduction of IPV in English, leaving a wide gap for IPV-exposed Latinas whose journey out of abusive relationships and to recovery is complex.
Objective:
This study aimed to explore the psychoeducational content (the “what”) and digital formats and features (the “how”) of an online psychoeducation intervention that would suit the needs and preferences of IPV-exposed Latinas.
Design and Methods:
Virtual interviews with both IPV-exposed Latinas (n = 8) and providers who have worked with them (n = 7) were conducted. Interviews included questions about (1) lived experiences with IPV; (2) specific needs and disparities that IPV-exposed Latinas face; and (3) types of content and digital formats that should be included in a digital intervention for IPV-exposed Latinas in order to meet those needs.
Results:
Qualitative analysis of interview transcripts yielded three major themes: Identifying and Coping With IPV and its Mental Health Impact, Grounding in Latine Culture, and Ensuring a Positive Digital Experience. These themes provide preliminary evidence that represents the needs and values of IPV-exposed Latina women and can be used to inform intervention development.
Conclusion:
This is the first digital psychosocial intervention development study specifically for IPV-exposed Latina women. Results suggest further investigation of digital therapeutics for this at-risk population.
Keywords
Introduction
Despite a cultural shift toward egalitarianism in recent years, intimate partner violence (IPV) remains pervasive, with approximately one-third of women in the United States experiencing IPV in their lifetime. 1 Research suggests that rates of IPV are higher, and the impact of IPV is more severe among women of color (e.g., Latinas) who hold multiple marginalized identities.2,3 IPV risk and the impact of IPV is influenced by various factors, including disability status, 4 undocumented status, 5 and socioeconomic status. Compared to women with greater social capital, Latinas in the United States are more susceptible to IPV and its negative effects, which points to a critical need for targeted, culturally tailored interventions for IPV-exposed Latinas.
IPV-exposed Latinas have reported significantly higher trauma-related and depressive symptoms, lower self-esteem, and greater parenting stress despite reporting IPV at similar rates to non-Latina IPV survivors.6,2 Nonetheless, Latinas experience significant barriers to seeking IPV-related help (e.g., emergency shelter, restraining orders). 7 Between 2014 and 2019, nearly every state in the United States reported a decrease in the availability of mental health services for Spanish speakers despite a rise in the Hispanic/Latine population. 8 When IPV-exposed Latinas can access services, intersectional perspectives are crucial; researchers have deemed the integration of Latine values and awareness of the sociopolitical context of the Latine community essential.9,10 One study of IPV-exposed Latinas receiving community-based services indicated that cultural sensitivity was actually more impactful than trauma-informed practices. 11 When women hold multiple marginalized identities, their risk for IPV may be higher; their IPV experiences and their impact are influenced by their intersectionality—the inherent overlapping and interconnectedness of social identities which influence their experiences in the world, including oppression and privilege. 12 IPV-exposed Latinas urgently need culturally and linguistically sensitive IPV and mental health support that transcends the barriers they encounter associated with face-to-face services and considers their intersectional identities; digital tools may be a viable alternative to efficiently address the service gap for IPV-exposed Latinas.
Online interventions may offer a promising pathway to provide safe, culturally tailored, and accessible support to IPV-exposed Latinas. Researchers have emphasized the utility of digital interventions, given their potential to reduce per-person costs, access a wide range of populations and locations, and service under-resourced communities.10,11,13 Sabri et al. 14 noted that digital IPV interventions can increase the possibility of reaching immigrant survivors who may otherwise forgo traditional service engagement; Oliveira et al. 15 highlighted a critical need to develop and examine digital interventions for “hard-to-reach victims,” such as Latinas. Existing digital IPV interventions have several limitations that make them inadequate for IPV-exposed Latinas.
Research indicates that digital IPV interventions may lead to lower IPV risk/victimization and improved mental health outcomes for IPV-exposed women.16,17,18 These interventions tend to provide some combination of safety planning and prioritization assistance, psychoeducation about IPV, and resources.15,19,20,21 One example of the power of digital IPV interventions is isafe, a fully automated Internet-based safety decision tool for IPV-exposed women in New Zealand, which was found to reduce IPV risk in a randomized control trial; depressive symptoms were also significantly lower as a result of engaging with the isafe intervention. 19 Existing digital IPV interventions rely, however, on the assumption that leaving a relationship is the only or best option, which can, in itself, be culturally insensitive. For some IPV-exposed women, coping rather than leaving may be more realistic, as the desire to stay may be culturally bound, with some women valuing family unity highly enough to tolerate an unhealthy relationship dynamic (e.g., Latinas). 7 Rempel and colleagues 18 noted that most digital IPV interventions to date have lent insufficient attention to the aftermath of leaving an abusive relationship, as they have centered around “the act of leaving.” Existing IPV interventions understandably target IPV that is actively occurring and aim to reduce or eliminate IPV, but they neglect women with IPV histories that may still be impacted by those experiences, which is problematic given that IPV has long-term effects on women’s mental health. 22 There is a need for digital interventions that support IPV-exposed Latinas, regardless of their decision-making process or the recency of their IPV experiences. Further, existing digital IPV interventions tend only to be available in English, posing a barrier for monolingual Spanish-speaking Latinas.
For Latinas, digital tools present a unique opportunity to address a major gap in IPV interventions and access to needed mental healthcare. The importance of developing digital interventions that are tailored based on the cultural background and life circumstances of the recipient has been established, 13 but there are no digital IPV interventions to date that are designed specifically for Latinas, nor have existing digital IPV interventions been adapted for the Latine population. In fact, IPV-exposed Latinas’ needs and preferences with respect to digital IPV tools have not been studied. The current study aimed to address this gap by exploring the psychoeducational content (the “what”) and digital formats and features (the “how”) that would suit the needs and preferences of IPV-exposed Latinas. Because no digital IPV interventions specifically for Latinas exist, development of such an intervention should center the voices of Latinas as well as build upon previous research in this area; the methodology for this study was informed by a five-step process used to iteratively develop a digital psychoeducational intervention for people at risk for psychosis. 23 This model involves: (1) Identifying needs and framework(s) through literature review; (2) integrating technology for content and format development; (3) obtaining stakeholder feedback from the target population and professionals with relevant expertise (e.g., clinicians, researchers); (4) adapting the intervention following iterative thematic analysis of qualitative stakeholder feedback; and (5) feasibility testing. Steps 1 through 3 were completed as part of this study.
Methods
Study procedures
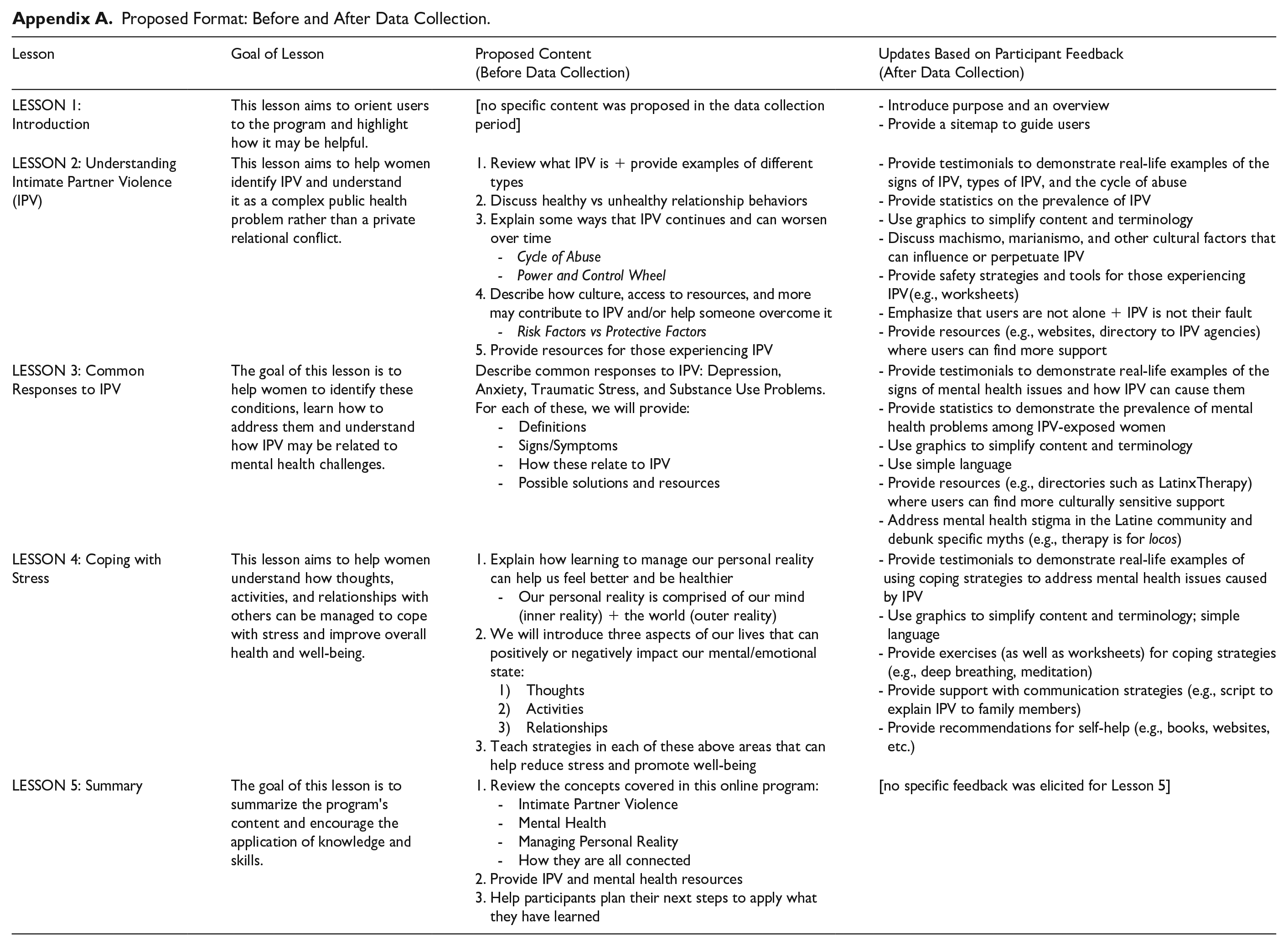
In accordance with the BEGIN model above, the first author (AA) conducted a needs assessment via literature review (Step 1) and drafted an outline of content to include in a digital psychoeducational intervention for IPV-exposed Latinas (Step 2; Appendix A). The study procedures below describe Step 3: obtaining feedback on the content outline from IPV-exposed Latinas and IPV providers in preparation for intervention development. The COREQ guidelines were used during preparation of this manuscript (see Supplemental Materials). 24 This study received ethical approval from the Palo Alto University Institutional Review Board (protocol no. #2023-032).
All study procedures were conducted online during a 10-month period (August 2023 and May 2024). Participants were recruited via an Instagram flyer available in English and Spanish that included an eligibility survey link. Prospective participants completed the brief online eligibility survey to confirm they were over 18 years and residing in the United States, and either an IPV-exposed Latina or a provider who worked with IPV-exposed Latinas; purposive sampling was employed. Seventy-three people visited the study eligibility survey. A majority (95%) of clicks resulted in at least partial completion of the eligibility survey. Many were considered ineligible due to residing outside of the United States (6.8%) or not being a Latina exposed to IPV or a provider (9.6%), while others did not provide sufficient information to determine eligibility (8.2%). Sixteen people (21.9%) were considered eligible but did not consent to participate. Thirty-eight (52.1%) people consented to participate, and a total of 18 completed the study procedures and were compensated. Twenty failed to complete a study interview or focus group; of these, four did not provide contact information, two withdrew from this study (reason unknown), 11 scheduled interviews but were lost to follow up, and three never scheduled an interview. Excluded from analyses were three participants who completed study procedures but did not consent to their interview audio file being converted into a transcript for data analysis. The final sample consisted of 15 participants, comprising seven providers who currently or previously worked with IPV-exposed Latinas and eight IPV-exposed Latinas. Among these 15 participants, four were both providers and IPV-exposed Latinas; these participants were counted only as IPV-exposed Latinas for the purposes of this study. Previous qualitative research with IPV-exposed women suggests that a sample size of 15 to 20 participants is sufficient to reach data saturation.25,26
Informed consent was obtained at the end of the eligibility survey via an electronic digital signature; the study consent form indicated that the research team would safeguard identifiable information via a secure password-protected database (i.e., the Box platform) and that participants would be notified immediately in the unlikely event of a data breach. Consented participants completed an online demographic questionnaire, which also assessed their experiences with and knowledge about IPV, mental health, and technology (see Supplemental Materials). Several efforts were made to minimize attrition and prevent non-response bias, including flexible participation options, e-mail reminders for study interviews, and follow-up contacts by the research team. For example, at the end of the online demographic questionnaire, participants self-scheduled via Calendly for either a group interview (via Zoom) or a one-on-one interview (via Zoom or phone). Those who failed to schedule an interview, canceled an interview, or did not attend their scheduled interview were contacted by the study team via email or phone up to six times. While the authors intended to solely conduct focus groups, most participants selected one-on-one interviews; only two providers opted for a group and were thus interviewed together.
All participant interviews (N = 15) were conducted between September and October 2023; interviews were audio-recorded for transcription and coding; the authors utilized an artificial intelligence (AI) transcription program, OtterAI, to convert interview audio files to written transcripts. Transcripts were not returned to participants, as the interview marked the completion of their participation. Members of the research team conducted the 90-minute semi-structured interviews using a script developed by the first author (AA). Nine interviews were conducted by AA, a doctoral candidate in clinical psychology, while six interviews were completed by a doctoral-level research assistant. At the start of the interviews, participants were reminded that the research study was being conducted as part of a dissertation study. Interview questions targeted relevant areas for the development of an online psychoeducational intervention for IPV-exposed Latinas, including barriers and facilitators to engagement in mental healthcare, IPV-related services (e.g., case management, shelter), and online IPV interventions areas of needed support concerning emotional well-being during IPV exposure and recovery, and content and format preferences for a digital IPV intervention (see Supplemental Materials). As part of the interview script and procedures, interviewers presented participants with an overview of the outline of content to include in a digital psychoeducational intervention for IPV-exposed Latinas and participants were invited to provide feedback. Interviewers developed field notes after interviews if new potential themes emerged. Participants were compensated with a $35 e-gift card at the completion of the interviews; interviews were not repeated.
The research team was composed of three female, bilingual Latinas. The first author (A.A.) completed this study as part of her doctoral dissertation research, under the supervision of her faculty advisor (A.Z.B.). The first author conducted an undergraduate honors thesis using thematic analysis and served as a research assistant in a psychosis risk lab, where she was trained in thematic analysis and contributed to manuscript development. The research assistants—a doctoral student and a master’s student in clinical psychology—had completed coursework in research methods and had background research and clinical experiences with IPV-exposed women.
Participants
There are two samples in this study: the IPV-exposed Latinas group and the providers group. IPV exposure was operationalized as having ever experienced physical, psychological, emotional, verbal, sexual, and/or economic abuse or exploitation by an intimate partner. IPV providers were operationalized as service professionals (e.g., therapists, caseworkers) who have worked with IPV-exposed Latinas.
IPV-exposed Latinas sample
IPV-exposed Latinas (n = 8) were on average 30.25 (SD = 2.86) years. One participant identified as Afro-Latina and all but one completed the study in English (87.5%). Participants were predominantly U.S.-born (75%) and U.S. citizens (87.5%). IPV-exposed Latinas were highly educated; two participants had obtained a master’s degree (25%), and four obtained a doctorate (50%). See Table 1 for more demographic information. All IPV-exposed Latina (n = 8) participants endorsed past, but not current, exposure to IPV. The most common types of IPV endorsed included emotional/psychological abuse and sexual abuse (Table 2). When asked about the degree to which being a Latina woman had influenced their experience of accessing help to deal with or overcome IPV, 50% of IPV-exposed Latinas selected “very much,” while the rest selected “somewhat.” Of those who reported accessing help/resources for IPV (n = 6), one-third (n = 2) endorsed a “mostly positive” experience, while one-third endorsed a “somewhat negative” experience. The IPV-exposed Latinas in this study endorsed several barriers to receiving help for IPV-related issues, including self-blame for their partner’s behaviors (100%) and a lack of financial resources (62.5%). Half of the IPV-exposed Latinas (n = 4) reported that fear of retaliation, not knowing where to search for help, feeling discouraged from past attempts to get help, little to no support from family or friends, and the cultural belief that women should be submissive were barriers to help-seeking. Half of this sub-sample reported receiving mental health services presently or in the past. Descriptive information about their technology preferences and mental health/IPV experiences can be found in Table 2.
IPV-exposed Latinas’ demographics (n = 8).

IPV, intimate partner violence.
Participants could choose multiple options.
Participants wrote in their spiritual/religious affiliation; one participant identified as “raised catholic, but not practicing.”
IPV-exposed Latinas’ mental health, IPV, and technology experiences (n = 8).

IPV, intimate partner violence.
Participants could choose multiple options.
Provider sample
IPV providers (n = 7) were on average 30.29 years old (SD = 7.81). Five reported that their work with IPV-exposed Latinas was in the past (71.4%), while two were actively working with this population. The level of involvement with IPV-exposed Latinas was mostly weekly (42.9%). Occupations included case manager (n = 2), counselor (n = 1), psychotherapist (n = 2), victim advocate (n = 1), and pediatric nurse practitioner (n = 1; see Table 3). All providers participated in English and were at minimum college-educated. Most identified as Hispanic/Latina (85.7%). They reported working with IPV-exposed Latinas between 6 months (n = 2) to 10+ years (n = 1). Nearly all providers reported that their workplace provided Spanish-language services to IPV-exposed Latinas (85.7%). Most providers reported speaking to IPV-exposed Latinas about their mental or emotional well-being (85.7%) and/or recommending mental health services (85.7%). Some providers reported using Internet searches (e.g., Google; 42.9%) and domestic violence websites (57.1%) when working with IPV-exposed Latinas; none reported using social media for this purpose. Descriptive information about IPV providers’ technology preferences and mental health and IPV-related professional involvement can be found in Table 4.
Providers’ demographics (n = 7).

IPV, intimate partner violence.
Participants could choose multiple options.
Providers’ mental health, IPV, and technology experiences (n = 7).

IPV, intimate partner violence.
Participants could choose multiple options.
Data analysis
Data analysis was completed in a 5-month period. Descriptive analyses were conducted in SPSS using data obtained from online questionnaires completed before the virtual interviews. Iterative thematic analysis was conducted using transcripts from completed IPV-exposed Latinas’ and providers’ interviews. Iterative thematic analysis consists of four phases represented by the acronym ABLE: “assessing initial beliefs as themes [which] examines the researcher’s preconceptions; building new beliefs during data collection [which] develops content of existing themes; listing tentative themes [which] produces a provisional statement of final themes; evaluating themes through coding [which] ensures that the themes are appropriate”. 27 Before data collection, the research team developed an a priori list of expected themes, based on their personal, clinical, and academic experiences with IPV-exposed women (see Supplemental Materials). After data collection was completed, the research team revised the list of expected themes based on the interviews conducted, drawing upon their field notes. Some expected themes did not emerge from the data collection and were removed from the list (e.g., negative perceptions about a digital intervention); new potential themes were identified to be confirmed via coding. A codebook based on the revised list of expected themes was developed by the first author. This codebook and de-identified interview transcripts were loaded into Dedoose, a cloud-based research application for data organization and research, 28 and each interview transcript was individually coded by tagging sections of the transcript with certain themes/subthemes. New patterns were iteratively identified and added to the codebook in Dedoose. After initial coding was completed, the frequency of each code was reviewed; if a theme was endorsed by 75% of the sample, it was included in the final list of themes. A total of 13 final themes were endorsed (see Figure 1) and reviewed one final time to identify what IPV-exposed Latinas need in an online psychoeducational intervention and how to meet those needs. The first author determined that the 13 themes fit into three categories (i.e., Identifying and Coping with IPV and its Mental Health Impact, Grounding in Latine Culture, Ensuring a Positive Digital Experience), thus making them better represented as sub-themes of three overarching themes. A.Z.B. supervised the development of the final list of themes. Following data analysis, the research team updated the previously created outline of the proposed online IPV intervention (see Appendix A).

Coding tree for a digital IPV intervention for Latinas.
Results
Three central themes related to program content, cultural considerations, and online program characteristics were identified. The frequency of themes endorsed by IPV-exposed Latinas versus Providers is described in Table 5. Sub-themes are represented in the coding tree (Figure 1) and described below.
Theme and code frequency for IPV-exposed Latinas and providers.

IPV, intimate partner violence.
Identifying and coping With IPV and its mental health impact
Identifying IPV and mental health awareness
Participants in both groups endorsed the importance of including content to learn how to identify IPV and mental health issues (e.g., depression, PTSD, anxiety, addiction) in an online psychoeducational intervention for IPV-exposed Latinas. Participants’ specific suggestions included sharing “warning signs” of IPV, symptoms of common mental health disorders, IPV and mental health prevalence rates, and the relationship between IPV and mental health. All participants endorsed a need to describe the signs and symptoms of mental health issues.
“I think. . .giving examples of what domestic violence is. Again, it's not just physical. . .When you enter a domestic violent relationship, it's not, like, abusive right away, or we don't think it's abusive, right?. . . I'm starting to learn more, like, the love bombing stage.” (age 33, IPV-exposed Latina)
Most participants (4/8 IPV-exposed Latinas and 4/7 providers) mentioned how IPV-related stress and mental health issues can manifest as physical symptoms, noting the importance of making this link explicit in an online IPV intervention for Latinas. One participant explained it this way:
“Something that is common is associating physical symptoms. . .when there might be mental symptoms. . .Latinos tend to say, ‘Oh, my stomach hurts,’ but it’s actually anxiety or things like that. So drawing a connection between physical symptoms and mental health symptoms would be key.” (Former domestic violence case manager, provider)
Coping
All participants were invested in ensuring that an online intervention empowers IPV-exposed Latinas with action steps for both IPV and mental health issues; they expressed a need for safety planning support for those actively experiencing IPV and coping strategies (e.g., meditation, breathing techniques, activities list) for all IPV-exposed women, regardless of their current IPV status. IPV-exposed Latinas recalled how they have coped and made distinct suggestions for recommendations to include in an online intervention, such as books, podcasts, and reconnecting with interests. Reflecting on what helped the IPV-exposed women they have worked with, one provider suggested including:
“how to deal with a person, like, if they’re still in that situation. . .How to be safe. . .Maybe if you want to prepare to leave from the situation, what would be the steps to take?. . .that exit strategy.” (Pediatric nurse practitioner and researcher)
Self-esteem
Participants' feedback also pointed to another important aspect of the mental health impact of IPV: self-esteem. All IPV-exposed Latinas and most providers (5/7) mentioned lower self-esteem as a major impact of IPV:
“. . .it affected my self-esteem a lot. And even though it’s been years, I just feel like I’m still feeling insecure in a lot of areas of my life. . .” (age 30, IPV-exposed Latina)
Overall, participants in this study highlighted critical questions to include in intervention content: What is IPV? What does it look like for Latinas? What is mental health? What are some mental health conditions associated with IPV? What are the signs and symptoms? How common are these problems (both IPV and mental health conditions)? What can Latinas do to support their mental health and deal with current IPV and/or the impact of past IPV experiences?
Grounding in Latine culture
Participants underscored the need to ground an online IPV intervention in Latine culture in various ways. They recommended addressing the harmful effects of stigma and extreme gender roles, as well as incorporating positive cultural values such as collectivism and personalism. They provided suggestions that showcased the importance of representation, including design elements and language preferences.
Stigma
In accordance with the research team’s a priori expectations about this population, participants in this study mentioned stigma as an important cultural consideration (8/8 IPV-exposed Latinas and 6/7 providers). When asked about making the online intervention applicable to Latinas, participants mentioned addressing stigma within the Latine community related to IPV and mental health, emphasizing the need to use stories, statistics, and psychoeducation for this purpose. To explain how stigma manifests in the Latine community, one participant shared:
“I think as a Latina, I - I've experienced it. . .we don't know what our emotions are. We don't know what depression is. We don't know what anxiety is. We don't know what our feelings are. . .And it's because it's not talked about in our culture, right? It's not talked about, like, our parents don't talk about it if you're feeling sad, like, let's be honest. . .if we tell a parent, like, ‘I'm feeling depressed.’ Like, they'll tell you in Spanish, like, ‘ay, eso no es nada.’ Like, that's not - there's no such thing, right? It's no such thing as depression. ‘Oh you’re anxious? Ponte a limpiar.’” (age 33, IPV-exposed Latina)
Gender roles
Gender roles were also mentioned by most participants as a cultural consideration for an online IPV intervention for Latinas (8/8 IPV-exposed Latinas and 5/7 providers). The cultural values of machismo and marianismo were mentioned directly and indirectly by participants as factors that contributed to IPV victimization and staying in abusive relationships. Most importantly, participants mentioned that these values and how they can impact relationships should be considered for this online intervention:
“Taking into consideration the. . .different or potential roles of women in the culture. . .So, like, if they’re a mother, then they might be more like, ‘No, I don’t want to leave because of my kids. . .’ or maybe even, like, the way, like, womanhood or being a woman is seen in the culture. . .this idea that women should, like, keep the family together. . .I feel like that would be helpful and, like, figuring out other ways to be mindful of that, but also helping them as well.” (age 27, IPV-exposed Latina)
IPV-exposed Latinas and providers shared the view that strict gender norms can be dangerous for women who face IPV or delay their safe exit due to the normalization of abuse and expectations of tolerance for women.
Collectivism and connection
An emphasis on the cultural value of collectivism and connection was evident throughout participant interviews. Both IPV-exposed Latinas (7/8) and providers (6/7) mentioned social connections, referring to family, friends, children, and even new partners post-IPV when discussing; they highlighted the need for communication strategies and reconnection post-abuse.
Family was an important component in the lives of the IPV-exposed Latinas in this study; they encouraged the research team to consider this when developing this online intervention. Nearly all IPV-exposed Latinas (7/8) reported that reconnecting with friends and family after being isolated during their IPV experiences has been critical for their healing and many recommended that connection should be encouraged in the online intervention.
“Community is something that, like, a Latina might value, and kind of incorporating something with, like, maybe getting more involved with their community, or their family, or kind of strengthening those like interpersonal, like, relationships.” (IPV-exposed Latina, age 27)
Personalismo
The cultural value of personalismo primarily manifested as participants’ suggestion to include testimonios (testimonials), or stories, of survivors’ lived experiences to help them identify with the content and reflect on their own lives. Most providers (6/7) and all IPV-exposed Latinas (8/8) suggested including stories and testimonials. Participants were interested in hearing the stories of actual survivors, but they also mentioned the utility of including success stories.
“We don't remember, like definitions, but we remember stories. Those stories remind us of ourselves or someone close that we know.” (age 27, IPV-exposed Latina)
Another specific way that participants emphasized personalism was through their suggestions to include avatars or characters that users can see/engage with throughout the intervention. Participants were adamant about using testimonials to help IPV-exposed Latinas feel less alone, identify their own patterns, and foster hope:
“Maybe having, like, one person throughout the whole, like, if this is a module or something, having one person throughout the whole module, and this is a Latina person. And just, like, showing her going through these different examples of how to mediate stress would be really cool.” (age 27, IPV-exposed Latina)
Representation
Participants in this study (12/15) expressed a need for Latine representation to be apparent throughout the intervention—seven of eight IPV-exposed Latinas and five of seven providers endorsed this sentiment. They provided tangible ways to integrate Latine culture into the design of the online intervention through images (e.g., of people), vibrant colors, names, artwork, graphics, and more. Participants underscored their need to feel seen when seeking IPV-related support to facilitate their trust and engagement; they commented on the diversity within the Latine community:
“Whatever graphics are used, obviously make it representative of the population. And, like, by that, I also mean, like, not just, like, White-passing Latinos. . .we come in all colors and hair textures. . .” (age 31, IPV-exposed Latina)
Ensuring a positive digital experience
Interactive
All participants endorsed a need for an online IPV intervention to be interactive. When asked about specific media, participants suggested a multi-media approach, integrating video, graphics, text, audio clips, and—as mentioned previously—self-report questions (e.g., screening questionnaires). The features participants suggested and the frequency with which they were endorsed can be found in Table 6. One example of the interactive approach participants endorsed came from an IPV-exposed Latina (age 27) who described ways to incorporate interactive coping activities into the intervention: “maybe like a relaxation activity or something like that, then maybe providing. . .a guided either video or, or like a script. . .to kind of, like, allow them to practice it while they’re doing the lesson.”
Intervention features recommended by participant group.
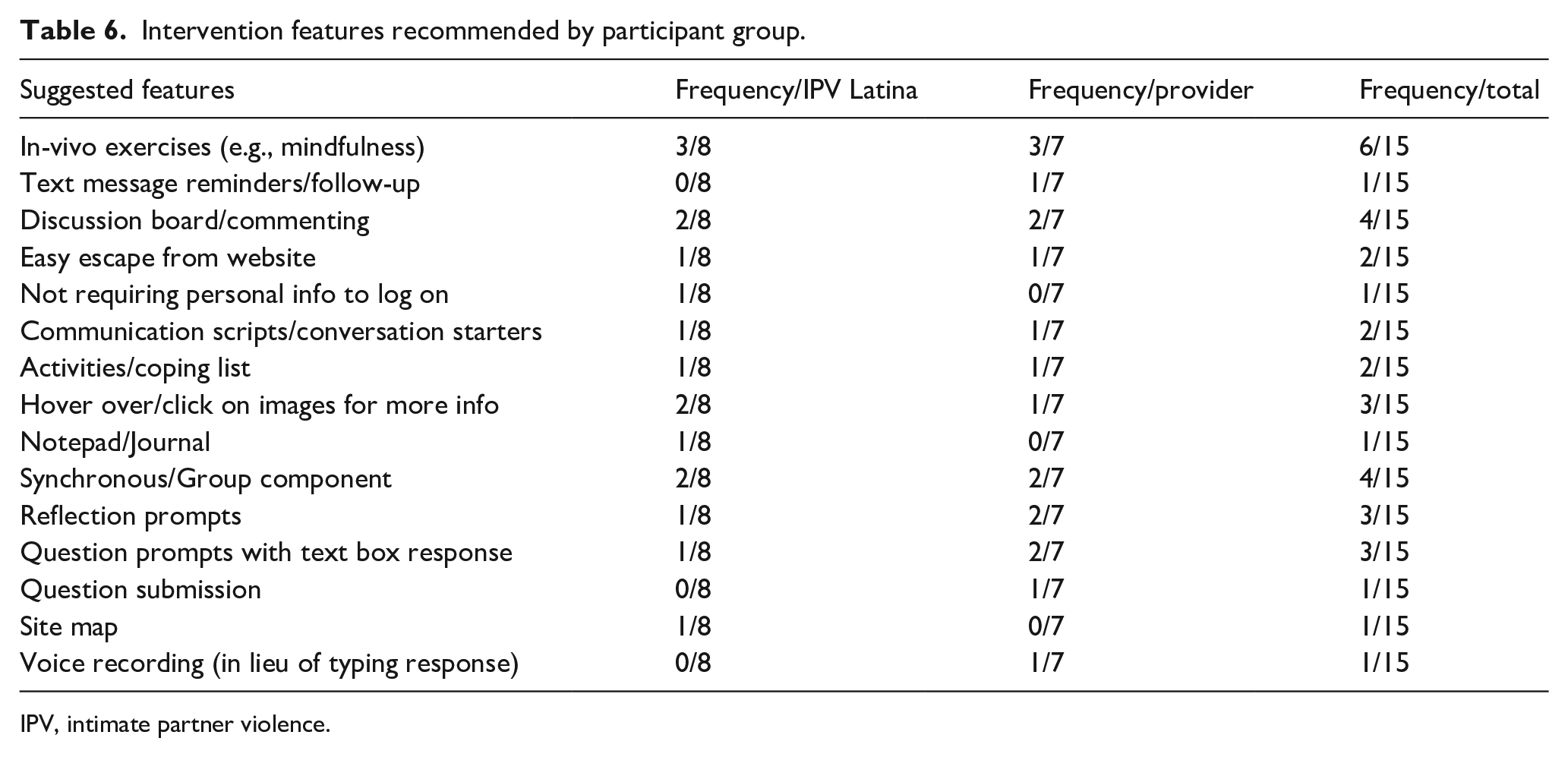
IPV, intimate partner violence.
Accessibility
Another important factor for participants was accessibility; they advocated for accessible language (6/8 IPV-exposed Latinas, 4/7 providers), almost always mentioning the need for the intervention to be available in Spanish. Some also reported that indigenous languages and varying dialects within the Latine community should be considered, too. Thinking of those with limited literacy and/or education, participants also stated that simple, basic language was key:
“. . .not everyone is as educated. . .in the English language. Or even that can read, just very simple, simply worded because I know that I’ve come across other women where, you know, they go to a website, and it’s just overwhelming.” (age 32, IPV-exposed Latina)
Providers and IPV-exposed Latinas alike believed that the intervention should be user-friendly, even for those with limited technological savvy. When not using the term “user-friendly” explicitly, participants gave specific suggestions, such as a site map “helping them navigate the website” (provider who worked with survivors of violent crimes). One provider even mentioned acknowledged potential technology barriers that IPV-exposed Latinas may face and suggested that the intervention be accessible on mobile devices.
Resources
All participants suggested that resources be a key component of an online IPV intervention for Latinas. One IPV-exposed Latina participant (age 33) suggested a comprehensive approach to resource provision; she said the following:
“just putting every single resource you can find. . . . shelters. A lot of like agencies, right, they do education, so like. . .the names of the agencies, obviously like the hotlines. . .I use, like, Instagram a lot to where there’s a lot of like Latina therapists, so finding a lot of, like, Latino/Latina therapists, you know, like just putting their names out there today, especially if you see people who focus in domestic violence. . .”
Some participants also suggested including in the resources lists of, and as relevant, links to books, videos, and podcasts from IPV/mental health professionals and IPV-exposed women. Overall, participants mentioned resources in a wide range of domains, including the following: IPV (e.g., shelters, hotlines), mental health (e.g., hotlines, therapy directories [e.g., Latinx therapy]), legal, parenting, financial, employment, housing, and English language learning (for monolingual Spanish speakers).
Discussion
We conducted 15 interviews with IPV-exposed Latinas (n = 8) and providers who work with them (n = 7) to explore the content (“the what”) and format (“the how”) preferences that may inform the preliminary development of an online psychoeducational intervention specifically for IPV-exposed Latinas. Qualitative analysis revealed three distinct themes: (1) Identifying and Coping With IPV and its Mental Health Impact, (2) Grounding in Latine Culture, and (3) Ensuring a Positive Digital Experience. Both IPV-exposed Latinas and providers in this study emphasized a need to integrate education about IPV and its mental health impact, as well as coping skills into an online IPV intervention for Latinas. In terms of how to do so effectively, participants highlighted the needs to ground all content and formatting in Latine cultural values and address stigma present in the Latine community. Finally, participants provided concrete suggestions to ensure that the intervention format and delivery results in a positive user experience. These findings point to IPV-exposed Latinas’ priorities and needs with respect to IPV services and recovery and provide critical insights into ways to use technology to address the challenges that IPV-exposed Latinas face when seeking support for safe exit from abusive relationships and/or their mental health.
The results of this study provide important lessons learned to help bridge the major service gap that exists for IPV-exposed Latinas. First, face-to-face and online interventions for IPV-exposed Latinas must address the impact of IPV, especially its mental health impact, over and above the outcome of their abusive relationship(s). IPV-exposed Latinas in this study were still affected by the abuse years later, consistent with previous research, 29 and could benefit from using an online tool to support their recovery. Understandably, digital IPV tools tend to focus on getting women out of abusive relationships by providing safety planning and resource connection, 15 but our findings highlight that women with past IPV exposure are a neglected group. Therefore, there is a critical need for a shift in IPV interventions; insufficient attention has been given to women recovering from IPV experiences, and digital tools may be used to support them. This study extends the priorities of IPV interventions to include psychoeducation about mental health and its relationship to IPV, as well as ways to cope; this is in line with research suggesting that digital tools could supplement face-to-face services to better treat mental health problems associated with IPV.15,16,17 Once out of abusive relationships, IPV-exposed Latinas are typically on their own to manage subsequent anxiety, depression, PTSD, and/or addictive behaviors as well as the resulting challenges in other areas of their lives (e.g., childrearing, employment, housing) due to isolation and loneliness, which are associated with IPV. 30 When services for IPV-exposed women are inaccessible or culturally insensitive, they are alone or lean on informal support (i.e., friends) not equipped to adequately support their mental health and overall well-being. IPV-exposed Latinas need affordable, accessible support options even long after they have left an abusive relationship; online interventions can leverage technology to provide necessary psychoeducation and support and link IPV-exposed Latinas to more intensive service options—filling a wide gap for this population.
Second, we found that integrating Latine values and awareness of the sociopolitical context of the Latine community into online IPV interventions is critical, supporting the notion that intersectionality must be considered in intervention development for IPV-exposed Latinas.9,31 Research has shown that ethnic minorities, as well as immigrants, tend to underutilize IPV services 32 and that IPV-exposed Latinas utilized mental health services less than IPV-exposed women from other racial groups (specifically White and African-American). 33 Despite Latinas’ disproportionate victimization, 2 they remain underserved due to various barriers. 34 It is important for intervention development to consider Latinas’ overlapping marginalized identities as ethnic minority women and consider other demographic variables such as socioeconomic status, education, and immigration status which influence their lived experiences and IPV risk. Research has shown that culture can influence help-seeking, risk factors, and IPV experiences;7,34 therefore, interventions must be culturally informed. After experiencing violations of their person and rights within the context of intimate relationships, IPV-exposed Latinas may also experience racism and discrimination in their pursuit of services to overcome the effects of IPV.7,35 Our findings suggest that IPV-exposed Latinas may benefit services that prioritize cultural values such as personalism, collectivism, and familism while also addressing stigma and harmful gender norms (i.e., machismo and marianismo) that are prevalent in the Latine community. Specifically, participants’ emphasis on the usefulness of testimonials is a manifestation of personalismo, a well-documented cultural value of the Latine community, which prioritizes relationships and friendliness, trust, and warmth practiced through small talk (charla), self-disclosure, and socializing. 36 IPV-exposed Latinas in the United States are forced to navigate individualistic systems with countless barriers to seeking support. 34 Our findings provide a pathway to leverage technology to connect IPV-exposed Latinas with each other—through testimonials and an overall design that is culturally and linguistically tailored. Machismo and marianismo have been related to IPV in previous studies;7,37,38 the former is characterized by sexist attitudes and behaviors of Latino men toward women, often offset by the responsibility of provision and protection for the family. 39 Marianismo is an ideal inculcated into Latina girls and women which emphasizes proximity to the Virgin Mary, promoting self-sacrifice and submissiveness.37,40 These cultural norms, in turn, can make identifying IPV and seeking support extremely difficult. This points to a need to use culturally specific examples to educate Latinas on how to identify IPV and mental health problems as well as debunk harmful gender norms to prevent revictimization. Our results underscore that a Spanish-language translation of an existing IPV intervention would not be sufficient; instead, this may do a disservice to IPV-exposed Latinas. While cultural adaptations are meant to make interventions applicable to a cultural group’s values 41 and are often more successful than non-adapted interventions, we propose that centering Latinas’ experiences and voices in intervention development promotes healing, community, and social justice. 42
This study adds a new element to the world of online IPV interventions: representation. Our findings suggest that, in order to best serve IPV-exposed Latinas, digital interventions should integrate diversity in language, nationality, literacy, education, and economic resources among Latinas and cultivate belonging and cultural sensitivity through design. Specifically, names, colors, and images can be used to the benefit of this population—in contrast to widely available resources online, which fail to represent Latinas. Participants in this study made suggestions that are in line with the Ecological Validity Framework,43,44 which outlined eight aspects of culture to consider when developing culturally sensitive interventions for the Latine population, including language, cultural values, and symbols. Latine ethnical/racial identity has been positively associated with mental health; that is, identifying with the Latine community is protective. 45 For IPV-exposed Latinas at large, acknowledging and incorporating their ethnic/racial identity in interventions may support their mental health. Our results suggest that a lack of representation may contribute to feelings of isolation and “otherness,” which could deter help-seeking for IPV and/or mental health services. 46 Overall, our results lend support to the use of digital tools to address IPV service gaps for Latinas and provide insight into how to culturally tailor such tools.
Limitations and future directions
A meaningful limitation of this study is the small sample size recruited; the sociodemographic characteristics of the sample limit the generalizability of the results to IPV-exposed Latinas only. The IPV-exposed Latinas in this sample were highly educated, mostly U.S. citizens, and had no children; only one participant was a monolingual Spanish speaker. Data collected in 2021 by the Latino Data Hub 47 show that 20% of Latinas over 25 have a bachelor’s degree or higher; educated Latinas were overrepresented in this study, likely due to social media recruitment of the PI’s professional account on which content about academia is predominantly shared. Social media algorithms tend to connect users with similar interests, and likely demographics, 48 leading to the possibility of a high rate of educated Latinas viewing the study recruitment flier. Future research should target IPV-exposed Latinas from more diverse educational and socioeconomic backgrounds, as the development of digital interventions for this population must include the voices of the most marginalized. No IPV-exposed Latina participants were actively experiencing IPV at the time of their participation in this study; the data derived from this study relied on retrospective accounts, which may limit the accuracy and generalizability of IPV-exposed participants’ feedback. Future research on the needs and preferences of IPV-exposed Latinas with respect to digital interventions should include the perspectives of those actively engaged in IPV services (e.g., shelters).
While data collection and preliminary development of themes were completed by the entire study team, the coding of qualitative data and the refinement of study themes were conducted only by the first author, which may have resulted in bias. 49 Finally, the first author also developed the outline of the proposed intervention content and presented it to study participants for feedback (Appendix A); this likely influenced participants’ responses, as they were left to agree or disagree with the proposed content rather than spontaneously suggest content for inclusion, which may have contributed to bias in the results.50,51 Future research may consider excluding an a priori intervention description or format to elicit IPV-exposed Latinas’ organic needs and preferences for a digital program. Additionally, this study explored the needs of IPV-exposed Latinas broadly, without limiting its scope to actively occurring IPV or past IPV. Future research may consider multiple user experience options to facilitate tailored content (i.e., content for those experiencing IPV, survivor of past IPV, co-parenting after IPV, etc.). Further research is also needed to ascertain whether IPV-exposed Latinas prefer a multi-lesson online IPV intervention, a mobile application, and/or a synchronous component such as a drop-in virtual support groups or live clinician support. As technological advancements continue, continued research can provide insight into whether features such as AI should be integrated into online IPV interventions for Latinas. Overall, future research is recommended to develop and beta test an online psychoeducational intervention for IPV-exposed Latinas. One approach is human-centered design, which considers the user throughout the entire process; this approach has been used to develop previous digital mental health tools. 52 We recommend human-centered design methods such as participatory design and co-design, which involve the target population in every step of the intervention design process.
Implications
A fully developed and empirically examined online IPV intervention for Latinas may serve as an accessible tool to assist a vulnerable population in their recovery from abusive relationships and/or a safe exit from an abusive relationship. Digital tools may provide a culturally and linguistically sensitive option for IPV-exposed Latinas who face various barriers to help-seeking (e.g., language, stigma). Receiving psychoeducation in an online, self-paced format may support IPV-exposed Latinas in self-identifying mental health problems linked to their IPV experiences, which may prompt them to seek more formal services (e.g., psychotherapy). If formal mental health services are not an option for IPV-exposed Latinas, they can begin to work toward wellness using the coping strategies and resources presented in an online IPV intervention. Digital health tools such as online psychoeducational intervention for IPV-exposed Latinas may be integrated in healthcare settings as a supplemental tool for mental health and women’s health professionals interfacing with women who are not yet ready to exit an abusive relationship or speak directly to their providers about IPV. While digital tools are increasingly being used, IPV providers may be hesitant to integrate technology into their practice; 53 our findings point to a critical need to establish buy-in with IPV providers to effectively integrate technology-based interventions for IPV. Dissemination of an online IPV interventions for Latinas may be achieved in a variety of ways, including collaboration with domestic violence and gender-based violence agencies nationwide (e.g., RAINN), community partnerships (i.e., in churches), through social media advertisement, and women’s and mental health provider recommendations. While our findings offer preliminary insights that can inform the development of the first ever online IPV intervention for Latinas, funding is a critical consideration. Further research on digital IPV interventions can inform policy changes that may result in insurance coverage or provider reimbursement for these tools, if proven effective. 16 Policymakers and funding agencies should consider the costs of current healthcare disparities for IPV-exposed Latinas, which may be addressed using novel approaches such as culturally tailored digital interventions.
Conclusion
This qualitative study provides preliminary evidence that an online psychoeducational intervention for IPV-exposed Latinas should aim to help survivors identify and cope with IPV and its mental health impact. Grounding in Latine culture and a positive digital experience should be prioritized in digital intervention development, according to IPV-exposed Latinas and providers who work with this population. Although this study relied on retrospective data and its generalizability is limited, results can inform preliminary development of the first ever online psychoeducational intervention specifically for IPV-exposed Latinas.
Supplemental Material
sj-pdf-1-whe-10.1177_17455057251329638 – Supplemental material for Developing a brief online psychoeducational intervention for Latina survivors of intimate partner violence
Supplemental material, sj-pdf-1-whe-10.1177_17455057251329638 for Developing a brief online psychoeducational intervention for Latina survivors of intimate partner violence by Aeriell Armas, Kitzia Corona and Alinne Z. Barrera in Women’s Health
Supplemental Material
sj-pdf-2-whe-10.1177_17455057251329638 – Supplemental material for Developing a brief online psychoeducational intervention for Latina survivors of intimate partner violence
Supplemental material, sj-pdf-2-whe-10.1177_17455057251329638 for Developing a brief online psychoeducational intervention for Latina survivors of intimate partner violence by Aeriell Armas, Kitzia Corona and Alinne Z. Barrera in Women’s Health
Supplemental Material
sj-pdf-3-whe-10.1177_17455057251329638 – Supplemental material for Developing a brief online psychoeducational intervention for Latina survivors of intimate partner violence
Supplemental material, sj-pdf-3-whe-10.1177_17455057251329638 for Developing a brief online psychoeducational intervention for Latina survivors of intimate partner violence by Aeriell Armas, Kitzia Corona and Alinne Z. Barrera in Women’s Health
Supplemental Material
sj-pdf-4-whe-10.1177_17455057251329638 – Supplemental material for Developing a brief online psychoeducational intervention for Latina survivors of intimate partner violence
Supplemental material, sj-pdf-4-whe-10.1177_17455057251329638 for Developing a brief online psychoeducational intervention for Latina survivors of intimate partner violence by Aeriell Armas, Kitzia Corona and Alinne Z. Barrera in Women’s Health
Footnotes
Appendix
Proposed Format: Before and After Data Collection.
| Lesson | Goal of Lesson | Proposed Content |
Updates Based on Participant Feedback |
|---|---|---|---|
| LESSON 1: Introduction | This lesson aims to orient users to the program and highlight how it may be helpful. | [no specific content was proposed in the data collection period] | - Introduce purpose and an overview - Provide a sitemap to guide users |
| LESSON 2: Understanding Intimate Partner Violence (IPV) | This lesson aims to help women identify IPV and understand it as a complex public health problem rather than a private relational conflict. | 1. Review what IPV is + provide examples of different types 2. Discuss healthy vs unhealthy relationship behaviors 3. Explain some ways that IPV continues and can worsen over time - Cycle of Abuse - Power and Control Wheel 4. Describe how culture, access to resources, and more may contribute to IPV and/or help someone overcome it - Risk Factors vs Protective Factors 5. Provide resources for those experiencing IPV |
- Provide testimonials to demonstrate real-life examples of the signs of IPV, types of IPV, and the cycle of abuse - Provide statistics on the prevalence of IPV - Use graphics to simplify content and terminology - Discuss machismo, marianismo, and other cultural factors that can influence or perpetuate IPV - Provide safety strategies and tools for those experiencing IPV(e.g., worksheets) - Emphasize that users are not alone + IPV is not their fault - Provide resources (e.g., websites, directory to IPV agencies) where users can find more support |
| LESSON 3: Common Responses to IPV | The goal of this lesson is to help women to identify these conditions, learn how to address them and understand how IPV may be related to mental health challenges. | Describe common responses to IPV: Depression, Anxiety, Traumatic Stress, and Substance Use Problems. For each of these, we will provide: - Definitions - Signs/Symptoms - How these relate to IPV - Possible solutions and resources |
- Provide testimonials to demonstrate real-life examples of the signs of mental health issues and how IPV can cause them - Provide statistics to demonstrate the prevalence of mental health problems among IPV-exposed women - Use graphics to simplify content and terminology - Use simple language - Provide resources (e.g., directories such as LatinxTherapy) where users can find more culturally sensitive support - Address mental health stigma in the Latine community and debunk specific myths (e.g., therapy is for locos) |
| LESSON 4: Coping with Stress | This lesson aims to help women understand how thoughts, activities, and relationships with others can be managed to cope with stress and improve overall health and well-being. | 1. Explain how learning to manage our personal reality can help us feel better and be healthier - Our personal reality is comprised of our mind (inner reality) + the world (outer reality) 2. We will introduce three aspects of our lives that can positively or negatively impact our mental/emotional state: 1) Thoughts 2) Activities 3) Relationships 3. Teach strategies in each of these above areas that can help reduce stress and promote well-being |
- Provide testimonials to demonstrate real-life examples of using coping strategies to address mental health issues caused by IPV - Use graphics to simplify content and terminology; simple language - Provide exercises (as well as worksheets) for coping strategies (e.g., deep breathing, meditation) - Provide support with communication strategies (e.g., script to explain IPV to family members) - Provide recommendations for self-help (e.g., books, websites, etc.) |
| LESSON 5: Summary | The goal of this lesson is to summarize the program's content and encourage the application of knowledge and skills. | 1. Review the concepts covered in this online program: - Intimate Partner Violence - Mental Health - Managing Personal Reality - How they are all connected 2. Provide IPV and mental health resources 3. Help participants plan their next steps to apply what they have learned |
[no specific feedback was elicited for Lesson 5] |
Acknowledgements
The authors thank Dr. Matthew Yalch and Dr. Joyce Chu, dissertation committee members for A.A., who took the time to review and provide feedback on this study. A special thanks to Ashley Mullin, one of the research assistants on this project. The authors thank TRACC and CTBH for their support of A.A. during the development and completion of this study. The authors also thank the participants who completed the study activities for this project.
Authors’ Note
Alinne Z. Barrera, PhD is now at the National Institute of Mental Health (NIMH). This manuscript was prepared while at Palo Alto University and accomplished in their personal capacity. The opinions expressed in this article are the author’s own and do not reflect the view of the National Institutes of Health, the Department of Health and Human Services, or the United States government.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.