
Abstract
Background:
Premenstrual tension (PMT) syndrome is a combination of a disruptive set of physical and emotional symptoms that women experience cyclically before the start of each menstrual period. It may impede day-to-day activities and can vary in severity.
Objectives:
This study aims to investigate the factors associated with PMT and explore their influences, along with family support, on the academic performance of female university students in Bangladesh.
Design:
This study used a cross-sectional design.
Methods:
This study is based on primary data collected from 765 female students of Jahangirnagar University, Bangladesh. A well-structured questionnaire, having sociodemographic information, PMT rating scale, and APGAR family function scale. Descriptive statistics, the chi-square test, Monte Carlo approximation test, multivariable logistic regression, and structural equation modeling (SEM) were employed for data analysis.
Results:
The findings revealed that 115 (15.03%) respondents demonstrated significant PMT symptoms, of which 54% reported that PMT had an impact on their academic performance, and 67% reported experiencing physical issues. This study also found that family support negatively influences PMT (standardized path coefficient = −0.23). The SEM path analysis indicates that all hypothesized relationships are statistically significant at the 5% level, leading to the rejection of the corresponding null hypotheses. PMT is positively associated with academic performance and is statistically significant (β = 0.505, p < 0.001). Moreover, family support is positively related to academic performance, exhibiting a weak but significant effect (β = 0.083, p = 0.045). Students with PMT were 53% less likely to belong to lower dysfunctional families (adjusted odds ratio (AOR) = 0.47, 95% confidence interval (CI): 0.33–0.66, p < 0.01). Students with chronic illnesses were less likely to belong to lower dysfunctional families (AOR = 0.53, 95% CI: 0.33–0.87).
Conclusion:
The findings indicate that strong family support can help alleviate PMT, potentially benefiting students’ academic performance. PMT is also associated with family dysfunction and chronic illness. Overall, family care and health awareness play an important role in supporting students’ academic success and overall well-being.
Introduction
Premenstrual tension (PMT) syndrome is a prevalent condition that impacts women during their menstrual cycle. Premenstrual syndrome (PMS) and premenstrual dysphoric disorder (PMDD) are included in PMT. 1 PMS is a collection of physical, behavioral, and emotional symptoms unrelated to any organic disease that start 5 days before menstruation and then subside during the luteal phase of the female menstrual cycle. 2 Adolescence significantly impacts physiological and psychological systems, primarily due to the monthly menstrual cycle, which typically occurs between 8 and 14 years after puberty. 3 The American College of Obstetricians and Gynecologists defined PMS as a clinical condition characterized by the cyclic occurrence of physical and emotional symptoms unrelated to any organic disease that appear during the 5 days before menses and end 4 days after the onset of menses in three consecutive cycles with sufficient severity that interferes with normal activity. 4 The International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD-10) defines PMS as a condition characterized by one premenstrual symptom during the luteal phase of the menstrual cycle, ending when menstrual flow begins. 5 In the mid-1980s, a severe form of PMS was called PMDD. 6 Mild PMS, often misunderstood by women, is characterized by three physical or mental symptoms, with severe symptoms linked to psychological dominance and extreme mood swings, which can either intensify or lessen preexisting symptoms. PMS can be attributed to hormonal, genetic, environmental, and sociocultural factors. 7
Family systems interact autonomously, and changes in a woman’s behavioral patterns and personal traits have been linked to severe PMS. 8 The World Health Organization estimates that 20%–31% of female university students globally suffer from at least one menstruation-related mental illness. 5 Academic stress, often perceived as a chronic stressor, is linked to physical sickness and sadness, potentially affecting premenstrual symptoms in female college students. 9 The ovarian cycle and the menstrual cycle are the two primary cycles that occur simultaneously during the monthly reproductive cycle experienced by menstruating females. Hormone directly impacts brain function, affecting a woman’s affective and cognitive state, and are believed to cause mood swings and cognitive processes.10,11 Physical symptoms caused by PMS include abdominal pain, uncomfortable breast tenderness, weight gain, headaches, back pain, nausea, acne, and psychotic symptoms, including depression, anxiety, lethargy, irritability, mood swings, changes in sleep patterns, and changes in appetite, along with women’s social and professional environments. 12 The American College of Medicine’s diagnostic criteria are used to identify premenstrual diseases, with over 150 identified symptoms. 13
The most severe type of PMS, PMDD, requires diagnosis of at least one mood symptom (marked affective lability, irritability, depressed mood, anxiety, or tension) is required in a group of five symptoms. 14 Epidemiologic studies show irritability is the most common symptom of PMS, with 3%–8% of women meeting PMDD criteria and 15%–20% meeting risk criteria. 15 Around the world, 47.8% of people have PMS. 16 A recent 2022 analysis shows that global prevalence fluctuates between 10% and 98%. 17 In recent times, rage has emerged as a significant issue that complicates living for people with PMDD. 18 The prevalence of PMT among female university students varies across countries, ranging from low in Australia (33%–41%) and the USA (20%–40%) to high in Turkey (72%–91.8%) and South Korea (89.5%).19,20 The geographical variation in PMT prevalence could be attributed to variations in the genetic, nutritional, and lifestyle characteristics of the young adult females under study. 19 A study pointed out that 90% of women experience PMS symptoms during their cycles, with 20% regularly experiencing behavioral, emotional, or physical symptoms during their reproductive years. 6 PMS and PMDD have been found to negatively impact relationships, productivity, work attendance, and healthcare consumption and expenses. 21 PMT negatively impacts women’s sleep quality, leading to frequent school absences, poor grades, and disengagement from education, particularly among teenage girls.22,23
PMT symptoms, such as emotional instability, irritability, difficulty concentrating, and fatigue, can significantly impair students’ cognitive abilities and result in lower academic performance because they make it difficult to concentrate during lectures, prepare for tests, and complete assignments.1,24,25 Their capacity to function academically may be further impacted by the additional strain of PMS, which can increase stress and anxiety. Attending courses regularly, actively participating in practical sessions, and working on group projects may be difficult for students. 26 Researchers concluded that PMS can affect students’ quality of life and academic performance.27–29 Additionally, PMS’s physical symptoms, such as headaches, sore muscles, and overall discomfort, may lead to absenteeism, which limits the time available for learning and developing critical skills. 30 PMS was linked to several issues in educational activities, including low scores, poor individual and collaborative task performance, and a lack of focus and enthusiasm. 31 Psychological disorders, such as sadness and mood swings, can also lower self-esteem and motivation, making it more difficult for students to maintain high academic standards. 32 Moreover, for students suffering from PMT syndrome, family support is essential since it can lessen the detrimental effects on academic performance, including problems with focus, involvement, and absence. To help students manage their symptoms and focus on their schoolwork, families can provide physical support, emotional encouragement, and a supportive environment.
Poor academic performance among university students may increase psychological stress, potentially worsening PMDD and PMS symptoms. 33 PMS-afflicted women report severe relationship problems and decreased productivity at work. 34 According to a prior study conducted in the United Arab Emirates, PMT has a considerable impact on the academic performance of female university students. 1 However, research has primarily focused on prevalence and severity, while overlooking understanding and perception, and there is a notable lack of literature on this topic in Bangladesh. This lack of knowledge makes it difficult to take the necessary steps to overcome these challenges. Despite its importance in the lives of female students, certain gaps remain. To our knowledge, no other studies have examined the impact of PMT and family support on academic success in the context of Bangladesh. Therefore, this study aims to focus on female students who have experienced PMT to explore the association between several factors and PMT among Bangladeshi university students. This study also aims to understand the impact of PMT and family support on academic performance, particularly among female university students in Bangladesh. The findings of this study may offer new insights into the impact of PMT and family function on academic performance.
Methods
Study design, area, and period
A quantitative approach was adopted to examine the severity of PMT syndrome and its impact on the day-to-day life of Bangladeshi female university students. Primary data for this cross-sectional study were gathered from Jahangirnagar University in Bangladesh between February 18 and April 1, 2025. Of the 17,212 students enrolled at the university, 8606 are female. Female university students from their first year to their master’s degree were the subjects of this study. The reporting of this study conforms to the STROBE statement. 35 The ethical approval for this study and its procedures was obtained from the Biosafety, Biosecurity, and Ethical Committee of Jahangirnagar University, with approval reference number BBEC, JU/M 2025/02 (196), dated February 17, 2025. Moreover, prior to the commencement of the survey, the study’s objectives were explained to participants, and they were asked whether they had given consent. Written informed consent was obtained from all participants prior to data collection. Participants below 18 years of age provided written informed consent for participation and for publication, obtained from the parents or legally authorized guardians of the minors.
Study population
All female students currently studying at Jahangirnagar University are considered the study population.
Inclusion and exclusion criteria
Participants were considered eligible for inclusion if they provided informed consent to participate in the study. Students with chronic medical conditions or who were pregnant were excluded. Additionally, students who were absent from the university on the day of data collection, those who were too ill to sign informed consent, and those with visual or hearing impairments were also excluded from the study.
Sample size and sampling technique
To obtain the maximum sample size, it is assumed that 50% of respondents have sufficient knowledge and experience with PMT syndrome, with a 95% confidence level. 36 A sample size of 384 has been determined using a formula suitable for finite populations. The following formula was used to determine the sample size:

In this case, the estimated prevalence
Data collection tools and procedures
The data were collected using a brief, well-structured, and pretested questionnaire. Thirty individuals from the target audience participated in pilot research to assess the acceptability and transparency of the questionnaire. These data were excluded from the final analysis. The survey consists of simple, self-explanatory questions. Of the 794 data collected, 29 were missing and excluded from the primary analysis. Data collection was conducted through face-to-face interviews. A few trained team members, who understood the study’s importance and goals, as well as the confidentiality of information, participant rights, and consent, were responsible for gathering the primary data. Additionally, a professor supervises the data collection process. The questionnaire has three parts. The first section provides sociodemographic information. The revised PMT syndrome rating scale, which aligns with the DSM-5 criteria for PMDD, was used in the second section of the survey. The third section assesses family function using the APGAR score questionnaire of Smilkstein. 38
Measurement variable
Sociodemographic information included age, age of menarche in years, year of study, and several other variables. This part also included PMT symptoms that affected the participant’s academic performance, including attendance, participation in physical activities, timely completion of assignments, exam performance, involvement in extracurricular activities, and attentiveness in class. 1
This study evaluated 11 symptom dimensions using a self-rated scale similar to the observed PMT symptoms. These domains included physical symptoms, eating and sleeping patterns, emotional instability, irritability and hostility, depression, anxiety and tension, and others. On a scale of 0–4, respondents scored their symptoms in the nine categories: no symptoms, mild, moderate, and severe. The final two domains received scores ranging from 0 to 2, signifying no symptoms or slight or noticeable alterations. The maximum possible total score was 40. 38 In this study, Cronbach’s alpha was recorded at 0.89. The total scores were divided into four different categories: normal (0–10), mild (11–18), moderate (19–27), and severe (⩾28). 1
The family function, being a dependent variable, is evaluated using Smilkstein’s APGAR score questionnaire. These inquiries enable the evaluation of a person’s contentment with the way their family functions, based on APGAR, an abbreviation for “essential in the family unit,” which assesses the functional elements of resolve, growth, partnership, adaptability, and affection. The APGAR questionnaire consists of five questions about the elements of family function. Students select one of three options, which are worth “almost always (2 points), some of the time (1 point), or hardly ever (0 points).” The total score ranges from 0 to 10. In this study, Cronbach’s alpha was 0.81. The participants were divided into two groups using the median family function score for statistical analysis: A higher Dysfunctional group (⩾9) and a lower Dysfunctional group (<9). 38
Statistical analysis
Descriptive statistics, including percentages and frequencies, the Chi-square test, and Monte Carlo approximation for association and bivariate analysis, were employed. Monte Carlo approximation was used for the chi-square test when expected frequencies were below 5. The authors examined the significance using a 5% level of significance. PMT syndrome was transformed into a binary variable, where “yes” denoted moderate and severe cases and “no” denoted normal or mild symptoms. We then applied structural equation modeling (SEM) to investigate the effects of PMT and family activities on students’ academic performance. We used the Python programming language (Python 3.11.7 version, Python Software Foundation, Available at http://www.python.org), SPSS AMOS, and Kobo Toolbox for data input, cleaning, and exploratory data analysis.
Results
Table 1 displays the sociodemographic details of 765 respondents. Of the respondents, 81% are between the ages of 20 and 23, and the majority experienced menarche between the ages of 13 and 15 years, and were first-year students. The majority of students in mathematical and physical sciences are 31% and live in urban areas. Additionally, 74.51% of female students reported residing in university residence halls, while 97% were single. Moreover, Muslim students comprised the majority of the student body at 89%. Regarding parental education, only 9.15% of fathers were illiterate, and 58.04% had at least a higher secondary education. Just 12.68% of the participants’ mothers were illiterate, whereas 38.41% of the mothers had completed higher secondary education or more. Only 2.88% of students came from wealthy households based on the family wealth index, whereas 81% belonged to middle-class families. Furthermore, menstruation typically lasts between 3 and 7 days in 90% of cases. Additionally, 95% of female university students refrain from smoking. Similarly, about 75% of students drink coffee for various reasons. Meanwhile, 74% of college students stay up late, leading to different struggles. Lastly, 87% of female students do not have chronic illnesses. Menstruation is regular for 82% of students, most are of normal weight (62%), and only 3% are obese.
Frequency distribution of the sociodemographic characteristics of the respondents.
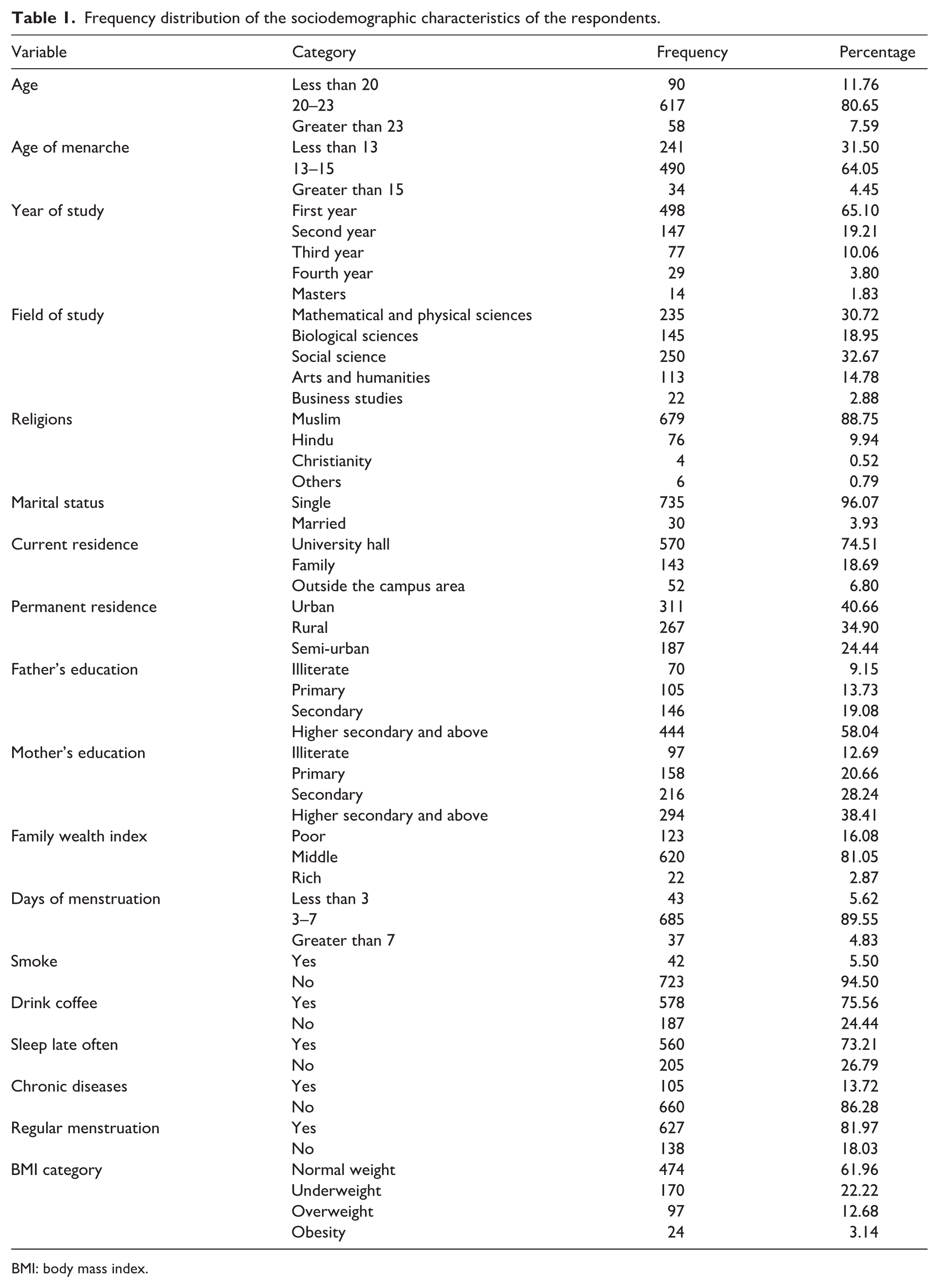
BMI: body mass index.
Association between sociodemographic factors and PMT syndrome
The association between sociodemographic factors and PMT syndrome among university girls is presented in Table 2. The demographic variables age, age of menarche, year of study, field of study, religion, area of permanent residence, area of current residence, family wealth index, and mother’s education, the habits of smoking, consuming coffee, sleeping late, and chronic disease are all significantly associated with p < 0.05 for PMT syndrome. Girls who had their menstruation before 13 years (19.09%) had more severe PMS tension than those who had their menstruation between the ages of 13 and 15 years (13.67%) and after 15 years (5.88%). The severe PMT syndrome for girls living in university residential halls, living with family, and living off-campus were 16.32%, 11.19%, and 11.54%, respectively. The majority of girls (15.45%) who were from poor families faced severe PMS, more than among middle-class and rich families (15.16% and 9.09%, respectively). There was more severe premenstrual stress among girls who do not frequently drink coffee (19.79%) compared to those who consume coffee frequently. The prevalence of severe premenstrual stress syndrome is higher among girls who sleep late (16.25%) than among those who sleep early (11.71%). Additionally, girls who were overweight (18.56%) experienced typical normal PMT syndrome in contrast to those who were underweight (17.65%), normal weight (13.29%), or obese (16.67%). Furthermore, there is no significant association between PMS and marital status, religion, father’s education, days of menstruation, or regular menstruation.
Results of bivariate analysis and chi-square test among factors associated with premenstrual tension syndrome (PMTS) among university students.
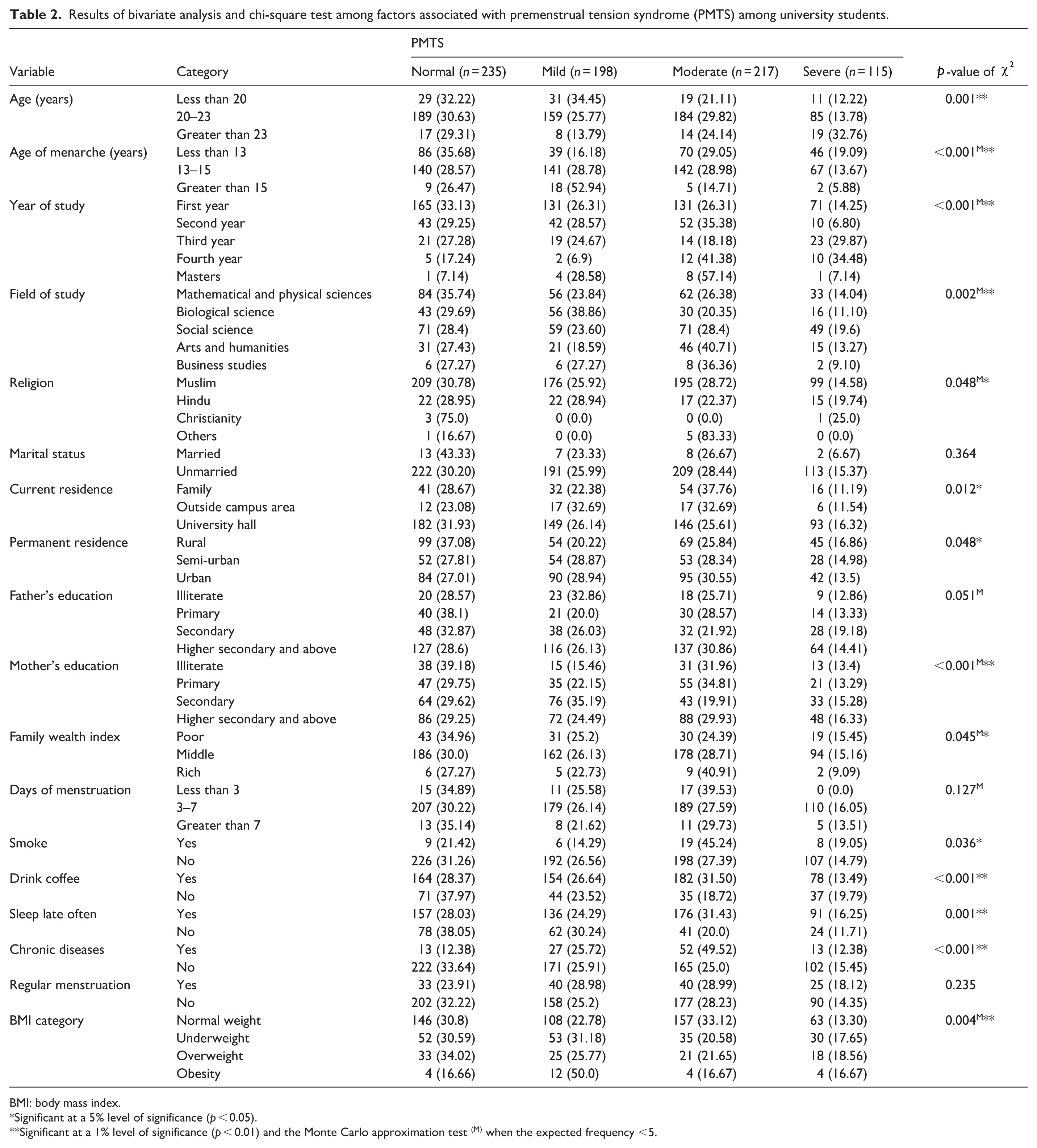
BMI: body mass index.
Significant at a 5% level of significance (p < 0.05).
Significant at a 1% level of significance (p < 0.01) and the Monte Carlo approximation test (M) when the expected frequency <5.
Association between sociodemographic factors and family function among university students
The association between sociodemographic factors and family function among university girls is presented in Supplemental Table 1. The bivariate table shows that the age of menarche, year of study, field of study, permanent residence, father’s education, smoking, sleeping late often, chronic diseases, and regular menstruation are all significantly associated (p < 0.05) with family function. Compared to girls who menstruated for more than 15 years (44.12%) and fewer than 13 years (48.13%), those who menstruated between 13 and 15 years (69.8%) belong to more dysfunctional households. The study shows that students in their third year (88.31%) and fourth year (82.76%) are more prone to come from dysfunctional families, whereas only 35.71% of master’s students show an inclination to come from dysfunctional families. Students of mathematical and physical sciences (65.96%) and biological sciences (75.86%) have a higher affiliation with dysfunctional families than those from social sciences (50.4%) and business studies (54.55%). The study found that 68.91% and 61.5% of students from rural and semi-urban areas, respectively, came from higher dysfunctional families, while only 55.95% of students from urban areas came from higher dysfunctional households. 76.03% of students whose fathers had secondary-level education show an association with higher dysfunctional families compared to those whose fathers had primary (59.05%) and higher secondary and above (58.33%) education 78.5% of students who smoke exhibit more affiliation with higher dysfunctional households as opposed to 60.86% of students who don’t. Furthermore, 58.04% of students who sleep late often belong to higher dysfunctional families, and 41.96% are from lower dysfunctional families. Additionally, 44.76% of students who suffer from chronic diseases came from higher dysfunctional families, while 55.24% belong to the lower dysfunctional families. Lastly, 59.97% of students who experience regular menstruation belong to higher dysfunctional families compared to 40.03% of students who are from lower dysfunctional families.
Figure 1 illustrates only a significant association between the PMT symptoms on respondents’ academic performance; therefore 54% of respondents said PTM syndrome had an impact on their academic performance, with physical activities (68%), focus in class (60%), involvement in extracurricular activities (58%), exam performance (46%), attendance (36%), and meeting deadlines for assignments (26%), being the most affected areas.

PMT syndrome affects various facets of the respondents’ academic performance.
Factors associated with PMT syndrome with demographic variables
Only significant variables (p < 0.05) from the bivariate analysis were entered into the regression analysis. The odds of having to experience PMT (adjusted odds ratio (AOR): 1.69, 95% confidence interval (CI): 1.00–2.84) were nearly 1.7 times higher among students aged less than 20 than those aged 20–23. Likewise, students who menarched beyond the age of 15 had a significantly higher likelihood of suffering PMT syndrome (AOR: 3.15, 95% CI: 1.28–7.77) than those who menarched between the ages of 13 and 15. Similarly, the odds of experiencing PMT (AOR: 0.16, 95% CI: 0.06–0.43) are 0.16 times lower for female university students in their fourth year compared to those in their first year. The odds of having experienced PMT (AOR:1.75, 95% CI: 1.07–2.87) were 1.75 times more likely for those in mathematical and physical sciences than for those who had arts and humanities. The odds of experiencing PMT were 2.22 times higher among students of biological science compared to those in arts and humanities. Those who sleep often late are 0.65 times less likely to experience PMT syndrome compared to those who don’t. Individuals with chronic disease have 0.53 times lower odds of experiencing PMT compared to those without chronic disease. Lastly, individuals experiencing PMT (AOR = 0.46, 95% CI: 0.33 – 0.65) had .46 times lower odds of highly functional families than those from dysfunctional families (Table 3).
Results of logistic regression to examine the factors associated with PMTS and family function, considering demographic variables among university students.

PMT: premenstrual tension; AOR: adjusted odds ratio; CI: confidence interval.
Significant at a 5% level of significance (p < 0.05).
Significant at a 1% level of significant (p < 0.01).
Factors associated with the family function demographic variables
Family function is significantly impacted by several factors, including age of menarche, year of study, study field, father’s educational background, smoking status, chronic disease, and PMS. The odds of experiencing menarche before the age of 13 are 0.36 times lower for respondents from less dysfunctional households (AOR: 0.36, 95% CI: 0.25–0.52) than for those between the ages of 13 and 15. Once more, their chances of reaching menarche after 15 years old are 0.26 times lower than those of those between the ages of 13 and 15. For respondents from less dysfunctional homes, the likelihood of pursuing a social science degree (AOR: 0.45, 95% CI: 0.27–0.75) is 0.45 times less than that of studying arts and humanities, respectively. Those whose fathers only have a secondary education are 2.36 times more likely to come from lower dysfunctional households than people whose fathers have higher secondary education or above. Respondents with chronic illnesses have 0.53 times lower odds of originating from lower dysfunctional households than those without, whereas smokers have significantly 3.6 times higher odds of coming from lower dysfunctional homes compared to nonsmokers. Additionally, the odds of experiencing PMT symptoms (AOR: 0.47, 95% CI: 0.33–0.66) are 0.47 times lower for people from lower dysfunctional homes compared to those who do not (Table 3).
Structural equation modeling
Hypothesis statement
The authors consider the following hypotheses:
H1: There is a significant relationship between premenstrual tension and academic performance.
H2: There is a significant relationship between family function and academic performance.
Measurement model
Confirmatory factor analysis revealed three main latent constructs in this study: PMT, academic performance, and family functioning. Here, items PMT1–PMT9 were used as indicators of PMT, AT1–AT7 were used as indicators of academic performance, and FE1 and FE4 were used as indicators of family functioning. The factor loadings of these items primarily indicate their relationships with the latent constructs, highlighting how strongly each construct is reflected in them, as shown in Supplemental Figure 1. Components with factor loadings less than 0.5 were removed from the model to improve construct validity, reliability, and model fit. 39
Structural model
An investigation using SEM was conducted to evaluate the study model shown in Figure 2. The SEM results showed a satisfactory fit to the data (χ2/df = 4.55, CFI = 0.917, IFI = 0.918, RMSEA = 0.068, SRMR = 0.062), as presented in Table 4. The model appears to accurately reflect the underlying properties of the data, as indicated by these statistical indicators. Tables 4 and 5 summarize the results of the SEM.

Structural equation model.
Model fit indices.

Results of hypothesis tests based on the SEM model.

SEM: structural equation modeling.
p < 0.05. ***p < 0.001.
SEM path coefficient analysis showed that all null hypotheses of the model were statistically rejected. First, hypothesis H1 (PMT is positively related to a student’s academic performance) had an acceptable strength (β = 0.505, p < 0.001) and a positive direction. Second, hypothesis H2 (PMT is positively related to a student’s academic performance) shows an acceptable, weak but significant relationship (β = 0.083, p = 0.045) with a positive direction (Table 5).
The model indicates that family function has a negative influence on PMT (standardized path coefficient = −0.23), suggesting that better family support is associated with lower premenstrual symptoms. Family function also has a small, positive, though weak, direct effect on academic performance. PMT, in turn, has a moderate positive effect on academic performance. Measurement indicators for each latent construct exhibit strong loadings, confirming the reliability of the scales: all factor loadings for family function, PMT, and academic performance exceed 0.66. For instance, the indicator loadings for academic performance range from 0.58 to 0.84, indicating that the latent construct is well represented by its observed variables (Figure 2).
Discussion
The present study examined the impact of PMT syndrome and family function among female Bangladeshi university students on academic performance. Our findings specifically highlight that female students with PMT experience both physical and emotional challenges, which may interfere with their academic performance. Moreover, body mass index (BMI), age of menarche, chronic disease, and family dysfunction were found to have a significant association with PMT symptoms. According to an Iranian research study, common symptoms include intolerance, irritability, fatigue, increased sensitivity, unfavorable attitudes toward others, and a desire to be alone. Our study found that several demographic factors influence PMT symptoms, such as smokers having a 1.9 times higher risk of developing PMT syndrome. Additionally, age, year, and field of study all significantly affect the likelihood of having PMT syndrome in a binary logistic regression model. 46 A prior study on obesity and PMT syndrome discovered a strong linear relationship between higher BMI and PMT syndrome. Our findings align with this, showing that respondents’ BMI has a significant influence on PMT syndrome. Moreover, underweight or overweight respondents are more likely to come from households with higher dysfunction, which can be explained by the influence of body weight on hormonal balance and stress levels that may, in turn, affect both the physical and psychological symptoms of PMT. 47 Our study’s bivariate analysis results demonstrate that consuming coffee has an impact on PMT syndrome since various mechanisms support this. Research indicates caffeine and coffee consumption can worsen PMT symptoms by inhibiting adenosine, leading to vasoconstriction and increased progesterone levels. However, a prospective study found no compelling evidence linking high caffeine or coffee consumption to the development of PMT syndrome. 48 We found that students who slept late were 0.65 times less likely to have PMT syndrome (AOR: 0.65, 95% CI: 0.45–0.95), indicating a protective association. The findings were contradictory to other surveys of female university students, which generally reported increased PMT syndrome risk from late sleeping. The discrepancy may be due to differences in caffeine consumption, study habits, or other lifestyle factors. 49 The results of our study showed that both PMT and family functioning were positively associated with students’ academic performance. A study conducted in the United Arab Emirates found that PMT was statistically significantly associated with academic performance, which is consistent with our study. 1
Again, females with PMT syndrome report mood swings, depression, anxiety, and difficulty concentrating. University students frequently experience these issues during menstruation, with 46% reporting problems attending exams and nearly 55% reporting problems with academic performance, such as paying attention in class or doing extracurricular work, which affects their academic performance. However, a study conducted at the University of Jordan’s School of Nursing discovered no significant difference in Grade Point Average (GPA) grades or levels of participation among students with PMT syndrome. This emphasizes the necessity of understanding and managing PMT syndrome among university students. 33 A Brazilian study found that females with PMT syndrome experience physical symptoms like sensitive breasts, headaches, muscle or joint discomfort, swelling, weight gain, overeating, food cravings, tearfulness, anxiety, and anger. 50 These symptoms disrupt academic, family, and social activities. Based on these symptoms, this study found that 25% of respondents had mild PMT syndrome, 28% had moderate PMT syndrome, and 15% had severe PMT syndrome. These symptoms prevent 67% of respondents from participating in physical activities, in contrast to a study of college students in Gujarat, which found no significant connection. However, regular exercise might be beneficial for maintaining a healthy lifestyle. 34 Furthermore, our study found a significant correlation between PMT symptoms and family dysfunction, with girls with PMT syndrome being 53% times more likely to come from higher dysfunctional households. This finding is consistent with an Egyptian study that reported a similar association between family support and PMT symptoms. Factors such as poor communication, emotional neglect, and unsolved conflict in a dysfunctional family environment can increase stress and disrupt the body’s hormonal balance, which can make PMT symptoms more severe. In contrast, where open communication, mutual empathy, and effective stress management strategies exist among family members, such as a supportive environment, it helps to reduce these negative effects by increasing emotional stability and reducing feelings of stress, 38 also there are positively significant relationship between family and academic performance, suggesting that students from well-functioning families generally perform relatively well academic performance. The supportive role of the family positively influences mental well-being and motivation, leading to improved academic performance among students. On the other hand, previous studies have shown that family support is positively associated with academic performance. 51
Limitations of the study
This study has a few limitations. One of them is that we did not focus on how females suffering from PMT syndrome deal with it or if they are receiving therapy for it, as we know that these symptoms might interfere with their everyday lives. The symptoms of PMT are subjective to the female students themselves and may be perceived differently in different cultures. The female students’ performance was collected based on their own self-assessment, which was not verified by GPA or other specific criteria. Furthermore, since this study was cross-sectional, it is not possible to establish a cause-and-effect relationship, and there is a possibility of recall bias during data collection. Data were collected over a 6-week period, which may not accurately reflect seasonal or academic changes. Still, the period was adequate for exploring general patterns. Future studies could use a longer duration. Moreover, because our study is primarily focused on university students, we do not know how these symptoms affect young schoolchildren or married women after delivering a child. The findings of this article may help society better understand women’s experiences and challenges, enabling it to be more sensitive to these issues. Additionally, it would assist healthcare providers in delivering services and educating women on how to manage their condition, thereby enhancing their self-esteem. Furthermore, parents should exercise caution when dealing with their child, as this might have a substantial impact on PMT syndrome.
Conclusion
The study shows that PMT syndrome and family support have significant negative effects on academic performance among female university students in Bangladesh. This research demonstrates that strong family support reduces PMT, which has a positive impact on academic outcomes. In contrast, PMT exhibits a moderate positive association with performance, as some of its symptoms pose obstacles to day-to-day life in a moderate-to-severe manner. The study emphasizes the importance of incorporating PMT into standard medical treatment for women and calls for healthcare providers to be aware of the issue and provide comprehensive services to university students. It also suggests raising students’ awareness of the problem and available coping techniques. Despite adopting a healthy lifestyle, women should consult with health professionals to manage PMT symptoms. Furthermore, parents must be more aware when dealing with their daughters and openly discuss these issues; they can also teach their sons to be more sympathetic to individuals experiencing these symptoms. Finally, the government can organize health promotion campaigns to raise awareness and encourage individuals to address these symptoms.
Supplemental Material
sj-docx-1-whe-10.1177_17455057261429272 – Supplemental material for Exploring the factors of premenstrual tension syndrome and their influence on academic performance among female university students in Bangladesh: A cross-sectional study
Supplemental material, sj-docx-1-whe-10.1177_17455057261429272 for Exploring the factors of premenstrual tension syndrome and their influence on academic performance among female university students in Bangladesh: A cross-sectional study by Md. Rayhan Kabir, Moinur Rahman, Afrida Tasnim, Niha Rani Debi, Maria Tasnim, Syeda Nujhat Nowshin and Md. Moyazzem Hossain in Women's Health
Footnotes
Acknowledgements
The authors are grateful to the participants for providing the information and consent to publish the survey results, which have been anonymized to protect their identities.
Ethical considerations
The ethical approval for this study and its procedures was obtained from the Biosafety, Biosecurity, and Ethical Committee of Jahangirnagar University, with approval reference number BBEC, JU/M 2025/02 (196), dated February 17, 2025.
Consent to participate
Written informed consent was obtained from all participants prior to data collection. Participants below 18 years of age provided written informed consent for participation and for publication, obtained from the parents or legally authorized guardians of the minors. Moreover, prior to the commencement of the survey, the study’s objectives were explained to participants, and they were asked whether they had given consent. If they agreed, the survey proceeded. Respondents were adequately informed that their information would be confidential and that no identifiable information would be disclosed. Furthermore, participants were assured that they could withdraw from the survey at any point.
Consent for publication
Not applicable.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data will be made available upon reasonable request by the first author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.