
Abstract
Background:
Fear of childbirth (FOC) is a significant psychological concern that can adversely affect maternal well-being and childbirth outcomes. While various factors influencing FOC have been investigated, the influence of sexual quality of life (SQOL) has not yet been sufficiently researched.
Objective:
This study aimed to examine the relationships among FOC, SQOL, and depression in pregnant women.
Design:
A descriptive, cross-sectional study.
Methods:
A cross-sectional study was conducted among 614 low-risk primiparous pregnant women aged 18–35 years in Kerman, Iran, between June 2022 and April 2023. Data were collected using the Wijma Delivery Expectancy/Experience Questionnaire Version A, the Edinburgh Postnatal Depression Scale, and the Female Sexual Quality of Life Questionnaire. A path analysis was conducted to examine the effects of SQOL, depression, and sociodemographic factors on FOC.
Results:
The average age of the mothers was 26.9 ± 4.5 years, and that of the spouses was 29.9 ± 4.2 years. The average gestational age was 35 weeks. SQOL was not significantly correlated to FOC. In contrast, FOC was positively associated with depression (p < 0.001) and the age of the spouse (p = 0.008). The mother’s age (p = 0.004) and the presence of chronic diseases (p < 0.001) were also significant negative predictors. In addition, maternal age was associated with better SQOL (p = 0.022), while depression (p < 0.001) and gestational age (p = 0.029) were significant negative predictors.
Conclusion:
Depression was a significant factor negatively related to both FOC and SQOL. Early detection and timely intervention for depression may reduce fear before labor and improve overall well-being during pregnancy.
Plain language summary
Fear of childbirth is a common concern for many women during pregnancy, especially those expecting their first child. In this study, more than 600 first-time mothers in Iran were surveyed to investigate whether depression and sexual quality of life were related to fear of childbirth. The results showed that women with depressive symptoms and women with older spouses were more likely to fear childbirth, while older women and women with chronic illnesses reported less fear of childbirth. Sexual quality of life was not related to fear of childbirth; however, it was influenced by other factors: older women reported better sexual quality of life, while depression and later stage of pregnancy were associated with poor sexual quality of life. These findings indicate the importance of early detection and timely intervention for depression in antenatal care to reduce fear of childbirth.
Highlights
Depression emerged as a stronger predictor of fear of childbirth.
Sexual quality of life was not found to be a predictor of fear of childbirth.
Fear of childbirth was significantly associated with maternal age, spouse’s age, and depression.
Introduction
Childbirth is a complex and multifaceted experience that is of great importance to women. Pregnancy and birth can be positive or negative and contain feelings of joy, hope, worry, fear, and anxiety. 1 Even nulliparous women (who have never given birth) are afraid of childbirth. 2 The reported prevalence of fear of childbirth (FOC) is between 20% and 80%, with about 10% of nulliparous women suffering from severe fear. 3
FOC, first described by Louis Victor Marcé in 1858 and defined in Swedish pregnant women in 1981, is characterized by severe anxiety that interferes with daily functioning. 4 There is a spectrum ranging from mild anxiety to phobic anxiety and from a normal worry to a complex psychological challenge for pregnant women. 5 Some women suffer from severe FOC or tokophobia, which is characterized by extreme anxiety and FOC. 6 Tokophobia (secondary) can arise from previous negative birth experiences. 7
FOC is not a constant construct and may vary during pregnancy. Researchers believe that the anxiety rate in pregnant women is high in the first trimester, decreases in the second trimester, but returns to its original level in the third trimester. The last trimester of pregnancy tends to be more stressful and anxiety-provoking. Around 33% of women suffer from anxiety and fear in the last trimester of pregnancy. 8
FOC, also known as tokophobia, can be so strong that some women may avoid becoming pregnant altogether, consider abortion, or request an elective cesarean section. 9 Women with severe FOC have an increased risk of medical complications during pregnancy, including prolonged labor, preterm delivery, a longer time to delivery, and an increased risk of cesarean section. 10
Studies in Iran have shown the prevalence of FOC ranges from 55.8% to 59%. 11 According to a recent study, the prevalence of FOC in Iran is estimated to be within the global range, but at a high percentage. This is due to concerns about pain, birth injuries, and harm to the baby. 12 Additionally, sociodemographic factors such as age, education, work status, economic status, pregnancy history, marital relationship, and mental health have an influence on FOC. 13
Among the predictors of FOC, prior research has emphasized the importance of social support and psychological well-being. Studies indicate that perceived social support, particularly from caregivers, can reduce stress and anxiety during pregnancy. For example, Buldum and Günér Emül reported a significant inverse relationship between perceived social support and FOC in adolescents, while Nulufer Erbil and Ozlem Akin found that greater support from attachment figures was associated with lower pregnancy stress.14,15 Similarly, Saisto et al. demonstrated that higher levels of anxiety, neuroticism, vulnerability, depression, low self-esteem, dissatisfaction with partnership, and lack of social support were associated with increased fear of vaginal delivery. In particular, it has been shown that dissatisfaction in intimate relationships increases FOC. 16
According to the conclusions, it is becoming increasingly clear that FOC is closely linked to impaired emotional well-being. Prenatal depression, characterized by persistent low mood and stress during pregnancy, has been consistently associated with higher levels of FOC. 17 This emphasizes the need to pay more attention to mental disorders during pregnancy, as depressive symptoms are not only common but also have a significant impact on maternal health. 18
In addition to depression, sexual quality of life (SQOL) is another important dimension of women’s psychological and relational well-being. SQOL is a multidimensional construct that encompasses psychological, relational, and physical aspects of sexual functioning. 19 Negative childbirth experiences have been shown to adversely affect SQOL. Emerging evidence indicates that anxiety and fear related to childbirth may also diminish women’s sexual well-being. 20
Although the reverse relationship between decreased SQOL and increased FOC has not yet been directly examined, the substantial overlap among sexual satisfaction, psychological distress, and FOC provides a strong theoretical rationale for examining SQOL as a predictor of FOC. This discrepancy is particularly noteworthy because women who report satisfying sexual relationships tend to have less anxiety and stress. In addition, partner support plays a central role in shaping pregnant women’s emotional responses and attitudes. 16 Despite this theoretical basis, the influence of SQOL alongside depression on FOC has been significantly under-researched in the literature.
We hypothesized that the SQOL of pregnant women may influence FOC, in addition to the impact of depression on both SQOL and FOC (Figure 1). This study aimed to investigate the relationship among SQOL, depression, and FOC. The findings may lead to educational interventions designed to reduce the negative consequences of FOC.

Conceptual framework illustrating the hypothesized relationships between sexual quality of life, depressive symptoms, and fear of childbirth.
Methods
Study design
The current study employed a cross-sectional design. When preparing this article, the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines were followed to ensure comprehensive and transparent reporting of the study findings. 21
Participants
The inclusion criteria of the study were as follows: Primigravida women aged between 18 and 35 years (childbearing age in Iran), gestational age between 28 and 40 weeks, basic literacy, and low-risk singleton pregnancy.
The exclusion criteria were as follows: a diagnosis of high-risk pregnancy (including multiple pregnancies, placenta previa, and preeclampsia), a history of infertility, a significant family history of stressful events, and any contraindications to vaginal delivery (causative factors that may affect FOC).
Participants were recruited between June 2022 and April 2023 at the prenatal units of 20 health centers affiliated with the Kerman University of Medical Sciences, Iran. A convenience sampling technique was used for recruitment. Participation was voluntary. A minimum sample size of 500 is recommended for observational studies with large populations to ensure accurate estimates of coefficients and Nagelkerke R 2 values. 22 After obtaining written informed consent, a total of 614 eligible pregnant women who met the inclusion criteria were included in this study.
The present study was designed and conducted in accordance with the ethical principles of the Declaration of Helsinki. Written informed consent was obtained from all participants prior to participation in the study, and they were explicitly informed of their right to withdraw from the study at any time without penalty. The research protocol was reviewed and approved by the Institutional Review Board of Kerman University of Medical Sciences.
Measures
In addition to a form designed to collect participant demographic information, three self-report questionnaires were administered: the Sexual Quality of Life-Female (SQOL-F) questionnaire, the Wijma Delivery Expectancy/Experience Questionnaire Version A (W-DEQ-A), and the Edinburgh Postnatal Depression Scale (EPDS).
Demographic characteristics evaluated included participants’ age, gestational age (in weeks), abortion history, chronic disease, employment status, level of education, spouse’s age, and spouse’s education.
The SQOL-F questionnaire is a self-report instrument designed to assess sexual self-esteem, and emotional and relationship issues. It comprises 18 items, each rated on a 6-point Likert scale ranging from “completely agree” to “completely disagree.” Responses are scored from 1 to 6, yielding a total score between 18 and 108, with higher scores indicating a better SQOL. The psychometric properties of the Persian version of the SQOL-F were evaluated and confirmed by Maasoumi et al. 19
The W-DEQ-A used in this study contains 33 questions, with responses ranging from 0 (indicating no FOC at all) to 5 (indicating the most severe FOC). The total score ranges from 0 to 165, with scores above 85 indicating clinical FOC. The Persian version of the W-DEQ-A has been validated and shown to be reliable for measuring the fear of birth in Iranian women. 23
The Persian version of the EPDS, specifically designed for determining depression in pregnant women, was utilized, which has been evaluated for its reliability and validity in a previous study. The EPDS is a 10-item self-rating tool developed by Cox et al. Each item is scored on a scale of 0–3, and the total instrument score ranges from 0 to 30, with 0 indicating the absence of depressive symptoms and 30 denoting probable severe depression. Acquiring a score of 12 and above is considered a possible/probable depression. 24
EPDS gives clinically meaningful results as a psychological screening tool and is used both extensively in research and practice to screen for depression in perinatal women in both primary care and midwifery centers. 25
In this study, the reliability of each measure was assessed using Cronbach’s alpha. The coefficient was 0.87 for SQOL-F, 0.76 for W-DEQ, and 0.80 for EPDS.
Statistical analysis
Descriptive statistics were employed to calculate the mean and standard deviation of the variables of interest. A path analysis was conducted to examine the direct and indirect effects of sociodemographic and psychological variables on FOC. The model specified depression and SQOL as potential mediators. Model parameters were estimated using the maximum likelihood with robust standard error method with 1000 bootstrap resamples to compute bias-corrected 95% confidence intervals (CI). Standardized and unstandardized coefficients, standard errors, 95% CI, and p values were reported. Model fit was evaluated using the comparative fit index (CFI), Tucker–Lewis index (TLI), root mean square error of approximation (RMSEA), and standardized root mean square residual (SRMR). Path analysis model was conducted in R software (version 4.3.1, R Foundation).
Results
Participants
The average age of the participants was 26.9 years, and the average age of the spouses was 3 years older (29.9 years). The average gestational age was 35.1 weeks, close to full term. For the psychological variables, the mean of the depression score was 8.2, the SQOL average was 92.5, and the FOC average during pregnancy (W-DEQ score) was 79.0. Overall, 29.2% of the women experienced FOC. The majority of participants (67.9%) held a bachelor’s degree or higher. In terms of occupation, 69.7% were housewives, while 30.3% were employed. Among spouses, 63.5% had attained a bachelor’s degree or higher, whereas 36.5% had less than a bachelor’s degree. The most common occupation among spouses was freelance or blue-collar work (65%), followed by white-collar employment (35%). Regarding reproductive history, most participants (84.0%) reported no history of miscarriage, while 16.0% reported a history of miscarriage. With respect to chronic disease, 76.9% of participants reported no such condition, whereas 16.0% reported having one chronic disease (Table 1).
The characteristics of pregnant people.

A path analysis results
A path analysis was conducted to examine the direct and indirect effects of depression, sociodemographic factors, and health characteristics on FOC and SQOL (summarized in Figure 2). The hypothesized model (Figure 1) demonstrated a good fit to the data with scaled χ²(6) = 6.22, p = 0.400, robust CFI = 0.998, robust TLI = 0.992, robust RMSEA = 0.007 (90% CI: 0.000–0.052), and SRMR = 0.011.
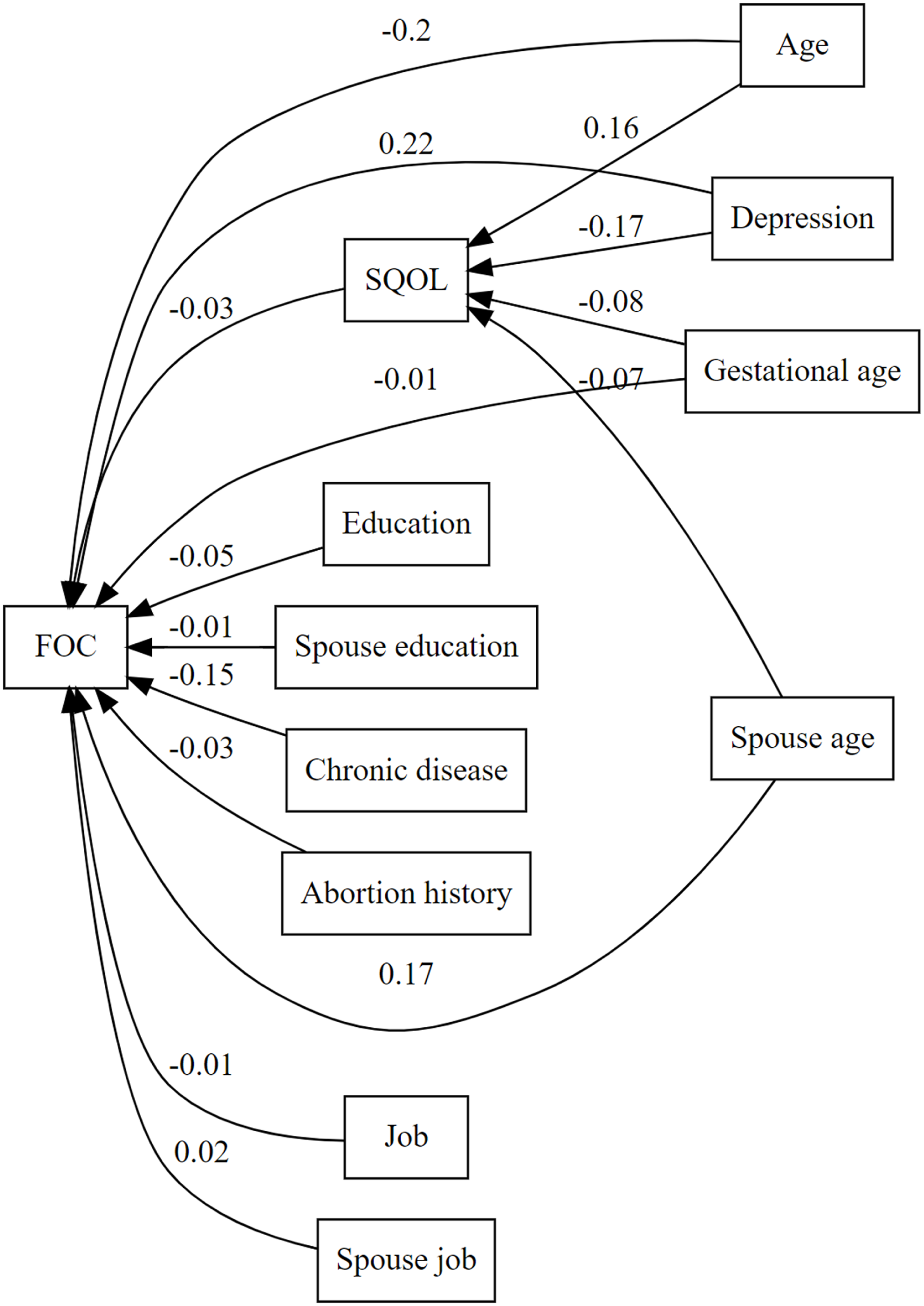
Path diagram showing the among FOC, depression, SQOL, and other variables.
Predictors of fear of childbirth
FOC was significantly and positively associated with depression (standardized coefficient (β) = 0.225, p < 0.001) and age of spouse (β = 0.171, p = 0.008). Age (β = −0.200, p = 0.004) and chronic diseases (β = −0.153, p < 0.001) were significant negative predictors. Other predictors, including education, spouse’s education, abortion history, gestational age, occupation, and spouse’s occupation, were not significant (Table 2).
Standardized direct, indirect, and total effects in the path model.

Significant predictors are bolded. SE: standard error; β: standardized coefficient; FOC: fear of childbirth; SQOL: sexual quality of life; CI: confidence interval.
Predictors of sexual quality of life
Older age was associated with better SQOL (β = 0.157, p = 0.022), while depression (β = −0.170, p < 0.001) and gestational age (β = −0.085, p = 0.029) were significant negative predictors. The age of the spouse was not significantly associated with SQOL (Table 2).
Indirect and total effects
The indirect effect of depression on FOC via SQOL was small and nonsignificant (β = 0.006, p = 0.404). The total effect of depression on FOC, combining direct and indirect pathways, was significant (β = 0.231, p < 0.001; Table 2).
Discussion
Childbirth is known to be a stressful experience that can make some mothers vulnerable to developing affective disorders, including perinatal anxiety and depression. Importantly, this emotional distress affects both women and men, with a common manifestation being FOC during pregnancy. 26
Our results showed that higher depression scores were significantly associated with both lower SQOL and higher FOC, consistent with previous studies linking depressive symptoms to childbirth-related anxiety. 23 These findings suggest that depression may play a dual role: It directly increases anxiety about childbirth and is simultaneously associated with lower SQOL. Although the indirect pathway from depression to FOC via SQOL was not statistically significant, the observed co-occurrence of decreased SQOL and increased FOC in women with depressive symptoms emphasizes the importance of considering the psychological dimension of well-being during pregnancy.
Depression has been identified as a significant factor influencing both SQOL and FOC. Research has shown that this mood disorder plays a critical role in the development and severity of FOC. 18 A study in Sweden found a significant association between FOC and a high comorbidity of depressive symptoms in women. 27 Another study in the United Kingdom found that 27% of women with severe FOC suffered from depression. 17
In addition, we found that younger maternal age was a significant predictor of FOC. This is consistent with the findings of previous studies from China and Iran, both of which reported that younger women experience higher levels of FOC.11,28 Conversely, our results showed that the age of the spouse was positively associated with FOC. Although less reported in the literature, this relationship could be explained by relationship and support dynamics. Increased age of the spouse could be associated with lower emotional congruence or less effective communication, which could reduce perceived support and increase FOC. 29 Alternatively, this association could also reflect sociodemographic factors in our sample, such as cultural expectations or socioeconomic norms regarding older partners.
Our results showed that a history of chronic diseases was associated with lower FOC, although unexpected, the results of a qualitative study by Tyer-Viola et al. showed that pregnant women with chronic illnesses may view pregnancy as a return to normality. The women described pregnancy as a balancing act between the fantasy of being normal and the reality of having a chronic illness, as the increased vigilance regarding health status could alleviate anxiety. 29 In addition, pregnancies in women with chronic illnesses are often more carefully planned and better monitored, fostering a sense of preparation that may buffer against fear. 30
In the analysis of predictors of SQOL, higher levels of depression were negatively associated with SQOL, which is consistent with the previous literature showing that depressive symptoms negatively impact sexual well-being and decrease overall SQOL. 31 Moreover, older gestational age was identified as a significant negative predictor, indicating that SQOL tends to decline as pregnancy progresses. This decline is likely attributable to the well-documented physiological, hormonal, and psychosocial changes occurring in later stages of pregnancy that interfere with sexual function and satisfaction. 20 However, older age was found to be a positive predictor, suggesting that older age is associated with better SQOL. This finding is consistent with the results of the perspective study, which suggests that age has a positive relationship with SQOL and that older adults’ SQOL is differentially influenced by the quality rather than the quantity of sex. Aging may be associated with the acquisition of skills and strategies that can mitigate age-related declines in SQOL. 32
Research shows that poor SQOL is consistently associated with higher levels of anxiety in pregnant women. 33 Additionally, various interventions such as cognitive-behavioral counseling, psychoeducation, and structured couples therapy have been shown to significantly enhance intimacy, sexual function, and perinatal mental health. 34 For instance, a randomized controlled trial conducted in Iran found that virtual cognitive-behavioral sexual counseling significantly enhanced both sexual function and intimacy among pregnant women. 35 A prospective study also indicated that poor partner relationships were associated with higher levels of state and trait anxiety, emphasizing the importance of emotional and communicative dimensions for sexual well-being. 36 Despite these findings, our study did not find a statistically significant association between FOC and SQOL.
Socio-cultural factors significantly influence both SQOL and FOC. In contexts such as Iran, cultural elements strongly shape women’s perceptions, experiences, and decision-making related to childbirth. Factors including stigmatization, gender roles, and religious beliefs contribute to fears surrounding childbirth and affect how women approach this experience.37,38 Societal expectations of childbirth and motherhood can increase feelings of inadequacy or fear in younger women, particularly those with little knowledge or experience. 39 These cross-cultural differences highlight the need for culturally sensitive approaches to antenatal care that address mental and sexual health in a supportive, non-judgmental manner. 40 Although this study did not capture cultural context, comparisons with findings from other regions suggest the need for future research to examine cultural expectations, gender norms, and partner support in different countries.
Implications for practice and policy
The findings in this study highlight the importance of integrated models of care that embed psychological screening within routine prenatal services. Early recognition of FOC and depressive symptoms by healthcare providers is crucial for delivering timely, targeted interventions, including cognitive-behavioral therapy and psychoeducational support. 41 Equally important is the involvement of spouses in couples’ pregnancy education and counseling to strengthen emotional intimacy and create a protective buffer against prenatal stressors. 42 Policy makers should consider investing in multidisciplinary perinatal care service models, and community-based interventions should be prioritized to ensure comprehensive, equitable maternal health strategies.
Limitation
It is important to recognize the limitations of this study. Due to the use of self-report and the cross-sectional design, it is limited in its ability to establish causality or capture change over time. In addition, the fact that only primiparous and low-risk pregnant women in Iranian health centers were included may limit the generalizability of the results to other populations. In addition, the study did not collect data on other potential moderating variables, such as cultural norms and partner support, which could have a significant impact on FOC. We suggest that future research should use larger, more diverse samples and conduct longitudinal or cohort studies to examine how FOC and SQOL evolve during pregnancy and postpartum. In addition, an in-depth examination of psychosocial factors, including cultural expectations and the role of partner support, could provide valuable insights into the mechanisms underlying FOC and enable the development of culturally sensitive and targeted interventions to support women at this critical time.
Conclusion
This study emphasizes the multifactorial nature of FOC in primiparous women. Depression was found to be a significant predictor, associated with both greater FOC and lower SQOL. Younger maternal age and older spouse age were identified as significant predictors of FOC, while the presence of a chronic illness appeared to buffer against FOC. In addition, SQOL did not show a significant association with FOC. It was influenced by depression, maternal age, and gestational age. These findings emphasize the importance of integrating routine mental health screening, targeted interventions for depressive symptoms, and contextualized partner support into antenatal care. Future longitudinal and cross-cultural studies are needed to develop tailored strategies to improve maternal well-being.
Supplemental Material
sj-doc-3-whe-10.1177_17455057261426800 – Supplemental material for Relationship among fear of childbirth, sexual quality of life, and depression during pregnancy: A cross-sectional study
Supplemental material, sj-doc-3-whe-10.1177_17455057261426800 for Relationship among fear of childbirth, sexual quality of life, and depression during pregnancy: A cross-sectional study by Farzaneh Ashrafinia, Julie Jomeen, Saiedeh Haji-Maghsoudi, Hui Chen, Erika L. Kelley, Omolbanin Heydari and Zeinab Mirzaee in Women's Health
Supplemental Material
sj-pdf-1-whe-10.1177_17455057261426800 – Supplemental material for Relationship among fear of childbirth, sexual quality of life, and depression during pregnancy: A cross-sectional study
Supplemental material, sj-pdf-1-whe-10.1177_17455057261426800 for Relationship among fear of childbirth, sexual quality of life, and depression during pregnancy: A cross-sectional study by Farzaneh Ashrafinia, Julie Jomeen, Saiedeh Haji-Maghsoudi, Hui Chen, Erika L. Kelley, Omolbanin Heydari and Zeinab Mirzaee in Women's Health
Supplemental Material
sj-pdf-2-whe-10.1177_17455057261426800 – Supplemental material for Relationship among fear of childbirth, sexual quality of life, and depression during pregnancy: A cross-sectional study
Supplemental material, sj-pdf-2-whe-10.1177_17455057261426800 for Relationship among fear of childbirth, sexual quality of life, and depression during pregnancy: A cross-sectional study by Farzaneh Ashrafinia, Julie Jomeen, Saiedeh Haji-Maghsoudi, Hui Chen, Erika L. Kelley, Omolbanin Heydari and Zeinab Mirzaee in Women's Health
Footnotes
Acknowledgements
We would like to express our sincere gratitude to all the pregnant women who participated in this study. In addition, we would also like to thank the staff of Kerman Medical University of Sciences for their support and assistance throughout the duration of this study. Their dedication and expertise greatly facilitated the smooth conduct of the research process.
Ethical Considerations
This study was reviewed and approved by the Research Ethics Committee of Kerman University of Medical Sciences (approval number: IR.KMU.REC.1402.315). All the procedures complied with the ethical standards of the institutional and/or national research committee and were in accordance with the ethical principles of the Declaration of Helsinki.
Consent to participate
Informed written consent was obtained from all the participants before participating in the study.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.