
Abstract
Painful sexual intercourse among women, commonly referred to as female sexual pain, is a common and debilitating experience associated with decreased sexual frequency, dyadic maladjustment, reduction of the sexual repertoire, the development of sexual dysfunctions and psychological distress among its sufferers [1–6]. In premenopausal adult women prevalence figures range between 10 and 21% [7–11]. Among younger women (≤30 years), one of five reports recurrent sexual pain [12,13].
Sexual pain is one of the most common symptom of vulvodynia. Vulvodynia is defined by The International Society for the Study of Vulvovaginal Disease as vulvar pain occurring in the absence of relevant visible findings or a specific clinically identifiable, neurologic disorder. The pain might be provoked, unprovoked or mixed and may be provoked by sexual or nonsexual stimulation or by both. The diagnostic classification is further specified as localized or generalized [14]. From a psychological perspective, the diagnostic definitions regarding sexual pain have changed over time, and today, pain-related fear is given a central role in the Diagnostic and Statistical Manual of Mental Disorders, DSM-V [15]. During the last decade there has been an increased interest in the pain component within female sexual pain, emphasizing the similarities with other pain syndromes in terms of experiential, psychophysiological and neurological characteristics [16–22]. Sexual dysfunctions are gradually more regarded as multifactorial conditions from a biopsychosocial perspective both by clinicians and scientists [23]. This has also broadened the view on sexual pain including both physiological and psychosocial mechanisms involved in etiology and possible treatment interventions [24]. Although there seem to be similarities between persistent sexual pain and other chronic pain problems, there is an urgent need to understand the central mechanisms in the development of sexual pain. There is a lack of theoretical models describing the psychosocial mechanisms involved in the experience of sexual pain and in the development of chronic genital pain. Established pain models from other areas of pain might contribute to the understanding and treatment of female sexual pain.
To describe the psychological processes involved in the transition from acute to chronic pain in musculoskeletal disorders, Vlaeyen and Linton [25] developed the fear-avoidance (FA) model, shown in Figure 1. The central idea in the FA model is that catastrophic thoughts, fear, muscle tension and hypervigilance set the stage for avoiding situations which in turn threatens to result in disability, disuse and depression. The FA model is a good predictor of the development of persistent pain as well as poor treatment results for patients with musculoskeletal pain [26,27]. Central parts of the FA model also seem to be relevant in female genital pain. Pain catastrophizing has been reported among women with genital pain [18,22], showing similar levels as in other pain conditions [28] and associated with higher pain ratings and more negative experiences of intercourse [29,30]. In addition, women with genital pain report impaired sexual behavior in terms of avoidance [31] and higher levels of fear of pain [32], and pain-related fear is known to predict increased level of pain sensitivity in this group [29]. Avoidance behavior in pain typically develops and is governed by the distinct laws of learning. That is, the antecedent stimulus that commonly precedes sexual encounters will cognitively be paired with sex and may act as a stimulus that signals anticipation of pain. In this way, many women with vulvar pain over time report avoidance of physical intimacy in general, not just sexual behaviors [31].
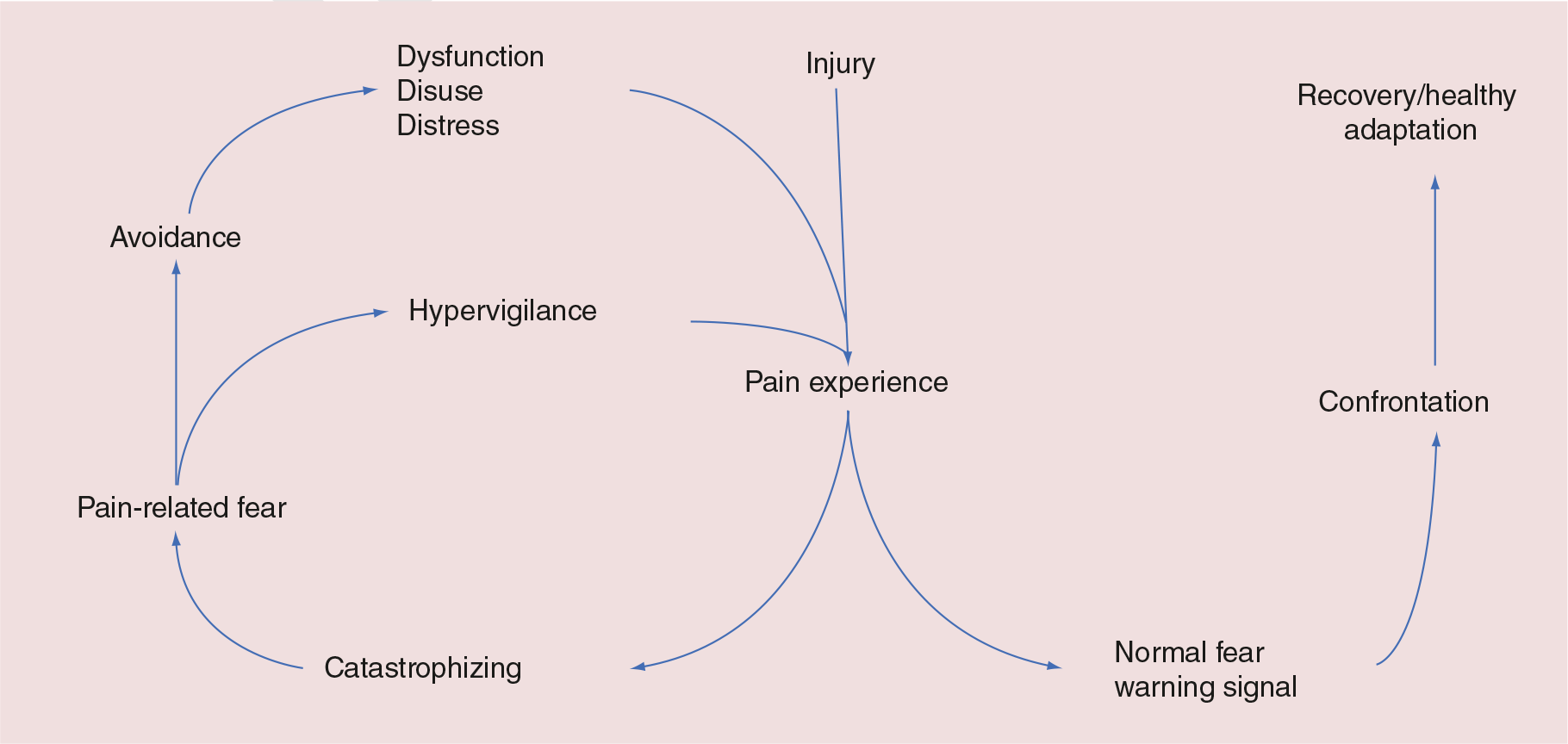
The fear-avoidance model of pain.
In a recent review on psychological factors in genital pain, results show sufficient concordance with the FA model to merits its use [33]. However, there is still a lack of empirical studies examining both the role of avoidance and pain catastrophizing in female sexual pain and to relate these factors to anxiety, depression and specific behavior patterns regarding intimate relationships.
The aim of the study is to examine fear avoidance (beliefs and behaviors), pain catastrophizing, and symptoms of depression and anxiety among women reporting intercourse pain. Part of the aim was to address a general female population with a liberal inclusion criteria regarding pain duration in order to examine the variation in and the association among the psychological components in the experience of painful intercourse, regardless of the etiology of pain. Thereby the study does not focus specifically on chronic pain. To our knowledge this is one of the first studies with a specific focus on avoidance behavior. Due to the lack of previous knowledge on these components in sexual pain, the need for cross-sectional data seems essential.
Methods
Design
The study was cross-sectional using a questionnaire that was both distributed in paper format and published as a web-based survey.
Participants & setting
The study used a convenience sampling method and included a mixed sample of 133 women, 18–35 years (mean: 24.5, SD: 3.8) both with and without sexual intercourse pain. Most participants were university students (94), and a third (49 women) were invited to take part through a webpage regarding sexual information/sexual pain. The sample included both women living as singles and women living in relationships. Intercourse pain may well take place although there is no stable sexual relationship and therefore this is not a factor that should exclude participants when examining sexual pain.
Women were recruited from multiple sources in order to maximize the number of participants and sought to include sexually active women with experiences of painful intercourse, not necessarily diagnosed with specific pain conditions or with chronic pain.
Measures
The questionnaire was carefully designed to include women as having dyspareunia when they had such experiences of at least 1 month's duration during the past 12 months although they presently did not have to be in a stable relationship.
To measure intercourse pain, participants were asked if they had experienced vulvar pain during sexual intercourse (minimum 1 month's duration) during the past 12 months with response options ranging from 0 to 4 (never, seldom, sometimes, often, always). Pain intensity was measured on a visual analogue scale (VAS) scale where participants were asked to indicate their pain intensity when the pain was at its worst. Women with pain were also asked during what additional activities (apart for vaginal intercourse) that they experienced pain (e.g., biking, horse riding, wearing tight clothes, during stress, gynecological exams), given the same response options as for intercourse pain above. In addition questions on how long pain commonly remained after the pain provoking situation (e.g., sexual intercourse) had been terminated, was included, with response options (pain subsides directly, remains 0–4 h, remains 4–12 h, remains for 12–24 h, constant pain).
Sexual frequency was measured both in terms of vaginal intercourse, nonpenetrative sex and sex without a partner (masturbation). Participants were asked to indicate separately for each type of sexual behavior how often they engaged in sex with response options ranging from 0 and 4 (less than once a month, one-to-four-times a month, one-to-two-times/week, twice or more/week).
Fear-avoidance beliefs were measured using The Fear-Avoidance Beliefs Questionnaire (FABQ), which consists of 15 items and in its original form focused on the individual's beliefs about how work and physical activity affect his/her lower back pain [34]. In the present study, the FABQ was adjusted to measure the woman's beliefs about how sexual activity affects her intercourse pain (e.g., ‘sexual activity may damage my genitals’, ‘I don't think I will ever be able to have penetrating intercourse'). The respondents are asked to what extent they agree with the statement on a four-point scale (0 = strongly disagree to 4 = strongly agree). The questionnaire has shown good validity and reliability [34]. Since the FABQ has not previously been used in a vulvar-pain sample psychometric characteristics of the instrument for this population is still lacking. The revised version of the FABQ showed a good internal consistency with Cronbachs α = 0.87.
To further measure avoidance behavior among women with pain, a couple of items that commonly are paired with sex among most women were selected. These questions were included to capture avoidance in a more general sense (not just sexual avoidance) in terms of physical intimacy which by many patients is described as (over time) becoming affected with fear, anxiety and associated negative emotions. Participants were asked to indicate to what degree they agree with the following statement; ‘Because of pain… I avoid physical intimacy that may lead to sexual intimacy’. To measure avoidance behavior among women not involved in a relationship, two statements were added: ‘Because of pain… I do not initiate love relationships’, and ‘I avoid sexual contacts’. Response options for these questions followed the FABQ using a four-point scale (0 = strongly disagree to 4 = strongly agree). Temporal sexual contacts were distinguished from love relationships in order to include a broader definition of relational settings in which sexual intercourse may be present.
Pain catastrophizing was measured with the Pain Catastrophizing Scale (PCS) [35], designed to assess various dimensions of catastrophizing about pain. The PCS consists of 13 items describing various thoughts and feelings about pain (e.g., ‘I keep thinking how badly I want the pain to stop’, ‘There is nothing I can do to stop the intensity of the pain’). Respondents were asked to rank each statement on a five-point scale, with respect to the degree to which they have these thoughts and feelings when they are in pain (0 = not at all; 4 = all the time). In the present study, all women answered the PCS regarding their thoughts of pain in general; that is, how they tend to react on pain, regardless of what kind of pain they were experiencing. The PCS has been used in similar ways to measure catastrophizing in genital pain [20]. Cronbachs a for PCS in the present sample was 0.92.
Symptoms of depression and anxiety were measured with a Swedish version of The Hospital Anxiety and Depression Scale (HADS). The HADS was originally developed to measure anxiety and depression among patients not in psychiatric care. The HADS includes 14 items, 7 relating to anxiety and 7 to depression [36]. HADS has shown good validity and reliability when used in both clinical and general populations [36,37]. Cronbachs a for the anxiety subscale was 0.84 and for the depression subscale 0.83 in the present sample.
Procedure
The data gathering was conducted via internet and by direct recruitment in a university population. The main strategy was to administer paper-questionnaires in four university courses by classroom visits where spoken information about the study was given and students were asked to take part in the study. Participants received additional written information and after giving their consent to take part in the study they were asked to fill in the questionnaire. To increase the number of participants, the questionnaire was also published on a student webpage regarding sexual information. All participants were volunteers and answered the questionnaire anonymously, confidentiality was emphasized. The study followed the ethical principles for research involving human subjects as defined by the Declaration of Helsinki as well as Ethical Guidelines for Pain Research in Humans (IASP).
Statistical analysis
Mean differences on psychological variables were calculated for women reporting intercourse pain and for the group who did not report pain. In addition, correlation analyses were performed for psychological variables (pain catastrophizing, fear-avoidance beliefs), avoidance behavior and pain intensity. In the last part of the analysis, regression models were built for intercourse pain and for pain intensity. A logistic regression model for intercourse pain included pain catastrophizing, fear-avoidance beliefs, symptoms of anxiety and depression as potential predictors to explain the variance in intercourse pain. A multiple linear regression including the same variables was conducted in order to explain the variance in pain intensity among those women reporting intercourse pain. The explanatory models were built using a stepwise regression in order to closely follow the unique contribution of each of the variables. The order in which the variables were inserted into the model was based on the strength of the correlation with the outcome in the previous analysis.
Results
Of the total sample (n = 133), 27.8% (n = 37) reported pain often/always and was thus categorized as having (frequent) sexual pain. Those women reporting pain only occasionally was not included in the group ‘women with pain’. Mean duration of pain was 4.4 years (ranging between 2 months and 16 years). A majority of women with sexual pain (85.7%) reported that pain commonly remained even after sexual intercourse was terminated. Half of the sample, 51.1% (n = 68), had a stable sexual relationship with a partner.
Differences between women with intercourse pain & women without pain on fear avoidance, pain catastrophizing & symptoms of depression & anxiety
As shown in Table 1, there were significant differences between women with pain compared with pain-free women on all psychological variables, with women with intercourse pain reporting higher levels of fear-avoidance beliefs, pain catastrophizing, symptoms of depression and anxiety. For pain catastrophizing and fear-avoidance beliefs, women with pain in the present sample reported similar levels as in previous pain populations. However, for depression and anxiety, the scores did not reach clinical levels.
Differences in mean between women with and without pain on fear-avoidance beliefs, pain catastrophizing, anxiety and depression (n = 133).

Standard deviation is displayed in brackets.
M diff.: Mean difference; W: Pain-free women; WP: Women with pain.
Correlations between psychological factors, avoidance behavior, frequency of sexual intercourse & pain intensity
As seen in Tab le 2, fear-avoidance beliefs showed a moderate positive correlation with frequency of sexual intercourse and were strongly and positively correlated with reports of actively avoiding sexual contacts/relationships. Although fear-avoidance beliefs and pain catastrophizing showed a positive correlation, the PCS was uncorrelated to frequency of sexual intercourse and avoidance behavior, but showed a moderate positive correlation to pain intensity. Pain intensity was also positively correlated with the FABQ. Finally, not surprisingly, the different types of avoidance behaviors showed strong positive correlations with one another and, except for avoidance of physical intimacy, were negatively associated with frequency of sexual intercourse.
Associations between fear avoidance, intercourse pain & pain intensity
Based on the bivariate analyses, two models were built to examine possible predictors to intercourse pain. In the first model, depression, anxiety, pain catastrophizing and fear-avoidance beliefs were included and associations with intercourse pain (yes/no) were examined. Using a stepwise analysis, the first block identified symptoms of depression as associated with intercourse pain, while this effect disappeared in the final version of the model where only fear-avoidance beliefs and pain catastrophizing remained as predictors. The model explained 73% (Nagelkerke R2) of the variance in intercourse pain (see Table 3). Symptoms of anxiety were not associated with intercourse pain.
Correlations between fear avoidance, pain catastrophizing, avoidance behavior, frequency of sexual intercourse and pain intensity among women with frequent sexual pain (n = 37).

p < 0.05
p < 0.01
p < 0.001.
Exact p-values are displayed in brackets.
FABQ: Fear-Avoidance Beliefs Questionnaire; NA: Not applicable; PCS: Pain Catastrophizing Scale.
Associations between pain catastrophizing, fear-avoidance beliefs, depression, anxiety and intercourse pain among all women (n =133).

Nagelkerke R2.
p < 0.05
p < 0.001.
B: Unstandardized Beta CI: Confidence interval; FABQ: Fear-Avoidance Beliefs Questionnaire; HADS: The Hospital Anxiety and Depression Scale; PCS: Pain Catastrophizing Scale; SE: Standard error.
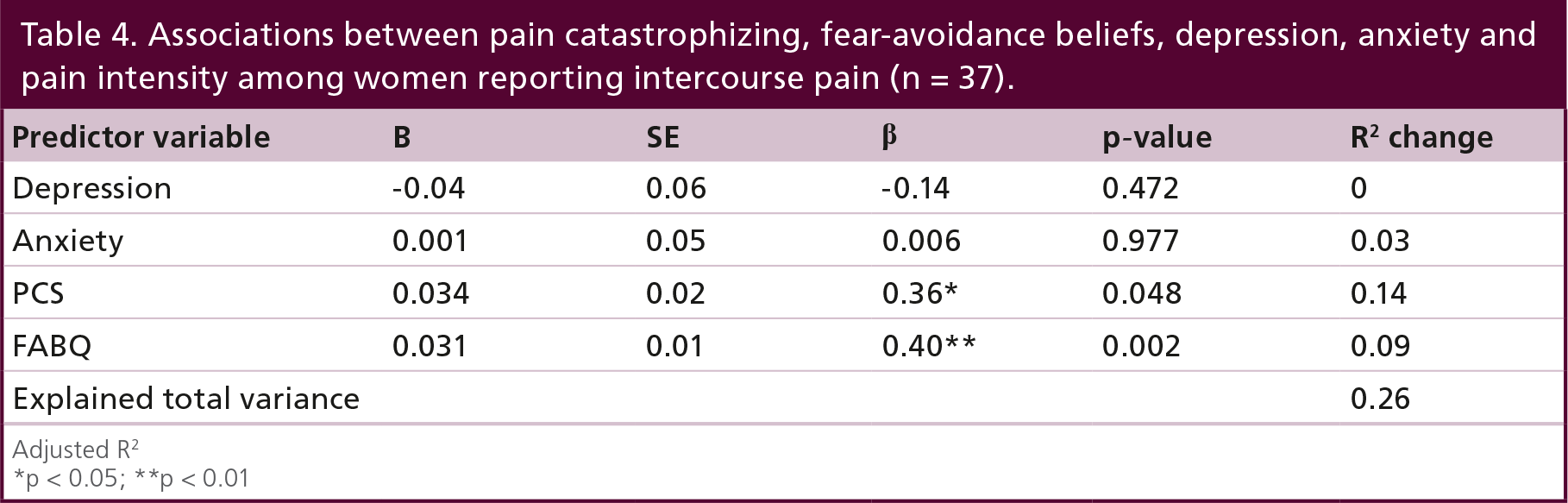
Finally, a second model was built to examine predictors for pain intensity among those women reporting frequent (often/always) sexual pain. The same variables were included as in the model to explain sexual pain overall. A similar pattern emerged in this model with fear-avoidance beliefs and pain catastrophizing being weakly associated with pain intensity while no effects were found for symptoms of depression and anxiety. The final model explained 26% (Nagelkerke R2) of the variation in pain intensity (see Table 4).
Associations between pain catastrophizing, fear-avoidance beliefs, depression, anxiety and pain intensity among women reporting intercourse pain (n = 37).
Adjusted R2.
p < 0.05
p < 0.01.
Discussion
Our results suggest that the main psychological factors of the FA model may be involved in the experience of intercourse pain. The exact role of these concepts in the context of sexual pain cannot be determined based on the present data. However, the principal pattern indicates that cognitive and effective factors together with the behavior patterns described by the FA model might be as essential to the experience of intercourse pain as to, for example, sustained musculoskeletal pain conditions [38].
Fear-avoidance beliefs were identified as a central factor associated with both the presence of sexual pain overall and with pain intensity among those women with pain. These beliefs could be viewed as mirroring an overarching belief that ‘hurt equals harm’, and are thought to play a vital role in the development of a chronic pain condition [25]. Evidence supports that fear-avoidance beliefs are significant predictors of future disability in patients suffering from acute back-pain [39, 40]. Also within sexual pain, research has shown that compared with no-pain controls, women with sexual pain report more fear of pain [41], and pain-related fear has also been identified as a significant factor associated with increased pain sensitivity in this group [29]. In the present study, fear-avoidance beliefs were reported with similar levels as in previous studies on persistent pain populations [34,39], and showed a negative correlation with sexual frequency and positively correlated with avoidance of sexual activities. In women suffering from sexual pain, sexual activity will be associated with negative emotions of shame, guilt and emotional distress, and many women and their partners describe that sexual activities are avoided, resulting in poorer sexual function [34], and decreased sexual satisfaction [42]. Unfortunately the present study only comprises cross-sectional data and could not outline any causal associations. However, according to the pain literature, fear-avoidance beliefs should not primarily be described as causing pain. Instead previous studies suggest a maintaining role for fear-avoidance beliefs. That is, pain may definitely result in pain-related fear/avoidance, but these behavior patterns in turn play a central role in maintaining the vicious circle of fear, avoidance, disuse/dysfunction and further pain experience.
Women who suffered from painful intercourse also showed elevated levels of pain catastrophizing, similar to levels reported by individuals with other chronic pan problems [35,43]. This factor was also associated with sexual pain and pain intensity in the explanatory models. Catastrophizing about pain has been described as a common negative mental set present during actual or anticipated painful experience [43], and thought to increase both fear of pain and hypervigilance for pain-related sensations and is thereby a path to avoidance behavior. The tendency to engage in pain catastrophizing has previously been associated with sexual pain [22,44], and related to increased pain ratings [34]. Pain catastrophizing is also found to negatively impact the experience of intercourse [30]. Among women with sexual pain, catastrophic thinking has been identified within several areas such as the intimate relationship, the value as a woman and the ability to become pregnant [45,46].
Taken together, although several aspects of the model were not examined in the present study (hypervigilance, physiological dysfunction/disuse), the results are in line with the central psychological aspects of the model. An important contribution made by the present study is the specific focus on fear-avoidance beliefs and avoidance behavior which has not been thoroughly examined within sexual pain previously. Avoidance of actual/anticipated pain is a powerful mechanism in the development of pain-related fear since safe situation (pain-free sex/intimacy) will also be avoided; thereby hindering the acquisition of learned experienced where sex is not conditioned to pain. However, in sexual pain among women, avoidance behavior is not just described as stop having sex. Many women continue having sexual intercourse despite of pain [47–49], to confirm their value as a woman and to satisfy their partners’ needs [45,50]. Thereby the overt behavior of engaging in sexual intercourse despite of pain may be described as illustrating a function of avoidance in terms of dysfunctional emotion regulation. Engaging in sexual intercourse among women with dyspareunia has the function of avoiding negative emotional consequences (shame, guilt) of saying no to sexual penetration. The behavior of ignoring and suppressing pain while activities are assumed, despite a worsening of symptoms, has been described within other pain populations as endurance coping [51]. To continue having intercourse despite of present pain might increase the risk of prolonged pain due to disrupted physiological and psychological sexual arousal (e.g., lack of lubrication) and friction during sexual penetration. Thereby, endurance of sexual penetrative activities despite of pain will contribute to maintenance of fear, catastrophizing and avoidance. Continued studies are needed on the specific function of fear, avoidance and endurance in the course of intercourse pain to understand the significance of pain catastrophizing and how it is linked to strategies for handling pain.
Women who reported intercourse pain also showed elevated levels of depressive symptoms and anxiety when compared with women free of intercourse pain. However, these factors did not reach clinical levels and could not explain intercourse pain or pain intensity in the predictive models. It is well known that women with sexual pain are more psychologically distressed than women without this type of pain [3,4], with depressive symptoms being associated with more severe pain reports [52]. A recent study using case–control pairs of women with and without vulvodynia demonstrated that DSM-IV-diagnosed antecedent depression and anxiety disorders influence the risk of vulvodynia and that vulvodynia increases the risk of both new and recurrent onset of psychopathology [5]. The failure to identify these factors as predictors of sexual pain in the present study might indicate that the type of emotional distress relevant for sexual pain is better conceptualized in some other way. When addressing female sexual pain from a fear-avoidance perspective it has been proposed that emotional distress might be better described in terms of shame, guilt and fear, and not primarily as depression [33]. These findings indicate the need for further studies using prospective designs on the experience of sexual pain and different measures of emotional distress.
In sum, our results are in line with the central psychological aspects of the FA model and support the importance of fear-avoidance beliefs and avoidance behavior as well as pain catastrophizing in the experience of intercourse pain among women. These findings should be integrated with physiological aspects of female genital pain in terms of increased innervations of the vulvar area, pelvic floor muscle dysfunction and the increased risk of female fungal infections [53].
Limitations
The main problem with the present study deals with generalizibility. By using a convenience sample the results of the present study might not be illustrative of the general population or a strictly defined clinical population, and the inclusion criterion was not set to address a chronic pain population. However, the association between fear and avoidance is similar to patterns identified within several other pain populations and indicates that fear avoidance and pain catastrophizing might be central mechanisms in intercourse pain among women. In addition, the amount of women reporting sexual pain often/always was similar to previous studies, although the definition here was based on frequency and not duration of symptoms. This might explain the somewhat higher prevalence in sexual pain reported here as compared with previous studies. However, the exact role of fear avoidance and pain catastrophizing remains to be studied and demands a more-controlled sampling procedure regarding randomization and predefined inclusion criteria for sexual pain. In addition, since pain intensity was only reported for pain at its worst, the mean pain intensity might be lower and in some cases pain might be of short duration (1 month). Therefore, the results have to be considered with restraint.
The questionnaire included instruments regarding pain in general and also items specifically adjusted or developed for the specific aim of sexual pain. For FABQ the items were adjusted to intercourse pain while the PCS were kept in its original version. Future studies should examine the validity of instruments based on the FA model adjusted to sexual pain. In addition, to further examine different types of avoidance in detail women in stable sexual relationships and those who where singles may be given separate questions regarding avoidance behavior. For example, the present study might have failed to identify a valid control group since single women who did not report intercourse pain may in fact actively avoid sexual intercourse and thereby not experience the problem with pain.
In order to examine the role of the social context in sexual pain, data on relationship status would be of interest. Unfortunately differences in relationship status among those with and without pain could not be reliably calculated since there was a high amount of missing data on this item among pain-free women in the present sample. Therefore, this factor was not included in the analysis. It is plausible that relationship status might interfere both with pain, emotional reactions such as fear, shame and avoidance behavior, and such patterns are essential to look into in future studies to give a valid picture of the experience of sexual pain among women.
Using a cross sectional design, conclusions regarding the predictive power among the variables of interest cannot be determined which is clearly relevant when examining a model such as the FA model in sexual pain. The results presented here only indicate that fear-avoidance beliefs, fear-avoidance behavior and pain catastrophizing are linked to sexual pain. The active mechanisms involved in the development of pain over time cannot be defined and it is therefore plausible that pain might result in these factors as well as describing them as active in the development of pain.
Implications & future needs
There is an immediate need for studies in the field to take on a prospective approach in order to examine the development of female sexual pain and possible maintaining mechanisms from a biopsychosocial perspective. In addition, there is a true need to address these mechanisms also in the clinic. Treatment programs built on cognitive behavior therapy based on the main parts of the FA model have been evaluated in a small number of studies and findings seem to indicate that these interventions may affect pain severity and sexual function [54,55], and that avoidance, pain catastrophizing and self-efficacy predict treatment outcome [56]. In addition, a number of studies using exposure interventions for intercourse pain have shown promising effects in terms of decreased avoidance and lowered fear of penetration [57–59]. However, there is still a lack of controlled treatment studies where specific interventions are implemented and evaluated within the sexual pain disorders.
In the FA model shown in Figure 1, the right-side loop describes a functional adaption to the injury where fear is confronted and no longer hinders the development of functional behaviors [25]. This has been illustrated in treatment studies were exposure interventions have resulted in decreased pain, fear of pain and increased function [60]. Similar results have been obtained in sexual-pain treatment where gradual exposures for fear of pain result in decreased avoidance and increase of intercourse [57]. Such interventions may be criticized in terms of being overly focused on penetrative sexual behavior and not working on adapting the sexual situation to the woman's needs and interests. An important development would be to not focus primarily on interventions aiming at exposure for fear and emotional distress in order to decrease avoidance, but to develop and strengthen a general sexual competence in terms of sexual desire/arousal of the women and alternative sexual behaviors. This might be the most adaptive strategy in the context of sexual pain where sex is neither avoided nor endured, but kept as an intimate, affectionate interaction.
The need for future resources in the field of female sexual pain cannot be overemphasized. Although showing high figures in prevalence estimates, only 60% of women suffering from these disorders seek professional care and of these only 40% receive a formal diagnosis [11]. This clearly mirrors two challenges for professionals: many women suffer in silence, probably due to shame, guilt and lack of knowledge on where to consult, and professional healthcare expertise in the female sexual pain disorders is still lacking.
Conclusion & future perspective
The over-representation of women in pain problems and in mental ill-health will hopefully result in strategies for increasing knowledge on how to prevent these often co-occurring health problems to develop into chronic conditions. Sexual and genital pain has only received a fraction of interest from clinicians and researchers as compared with the musculoskeletal pain conditions, which will change as the health of women will have to become a prioritized area. However, this demands that the health of men and women is viewed in equal terms in society, a development that will not take place in the nearest future.
Following the results of additional studies on the development of sexual pain, this condition will increasingly be viewed as a multifactorial problem resulting in the development of alternative and combined treatment interventions and in additional research interest. This will add further knowledge to the clinical setting regarding how pain is viewed and administered from a biopsychosocial perspective and how to combine physiological and psychological interventions. Theoretical models including both the physiological aspects of sexual arousal as well as cognitive–emotional components will receive further acceptance.
The importance of the development of individual sexual confidence and self-knowledge will be further stressed in sex education and the shame associated with sexual dysfunctions will be further diminished.
Executive summary
Between 20 and 25% of women under the age of 35 years report recurrent sexual pain.
There is accumulating evidence that cognitive, emotional and behavior aspects may be central in sexual pain just as in any other long-term conditions.
Women with sexual pain report elevated levels of fear-avoidance beliefs, sexual avoidance behavior and pain catastrophizing as well as lower sexual satisfaction than their pain-free counterparts.
Fear avoidance in the present study showed a negative correlation with sexual frequency and positively correlated with avoidance of sexual activities.
Women with pain engage in sexual avoidance behaviors even if not in a sexual relationship.
Fear-avoidance beliefs and pain catastrophizing are associated with sexual pain and the level of pain intensity among women with pain.
There is additional support for the application of the fear-avoidance model in female sexual pain.
There is an immediate need for prospective studies examining the role of fear, avoidance and pain catastrophizing in the development of female sexual pain.
Footnotes
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.