
Abstract
Background:
Young refugee women face elevated sexual and reproductive health risks, but their family planning (FP) needs remain understudied.
Objectives:
This study aimed to assess FP awareness, contraceptive use and associated factors among young married Rohingya women aged 15–24 years in Cox’s Bazar refugee camps and to compare knowledge and use among women who report no desire for additional children.
Design:
A prospective cross-sectional survey was conducted between March and April 2023.
Methods:
A multistage random sample was used to select 541 married women across 8 refugee camps. Data were collected via interviewer-administered structured questionnaires. Descriptive statistics and multivariate logistic regression were used to identify sociodemographic, informational, and gender-power factors associated with current contraceptive use.
Results:
Among 541 participants, 84.7% reported general awareness of FP, but only 27.0% could name a contraceptive brand. Current contraceptive use was 44.9%, and 37.6% of women who wished to avoid pregnancy were not using any method. Factors positively associated with contraceptive use included older age, husband’s education, exposure to FP information (adjusted odds ratio (AOR): 1.74; 95% confidence interval (95% CI): 1.06–2.87), fieldworker visits (AOR: 2.00; 95% CI: 1.31–3.04) and awareness of FP centres (AOR: 5.18; 95% CI: 2.30–11.67). Husband-controlled FP decisions were negatively associated with use (AOR: 0.46; 95% CI: 0.30–0.73).
Conclusion:
Interventions are needed to enhance women’s empowerment, increase contraception use among young women and support local and international organisations in Bangladesh working with refugees by providing more targeted fieldworker visits for education and the delivery of FP services.
Introduction
Sexual and reproductive health (SRH) is a critical public health issue for refugees, whose displacement and precarious living conditions heighten their vulnerability to poor health outcomes. Family planning (FP), as a fundamental aspect of SRH, is identified by international humanitarian guidelines, particularly through the Minimum Initial Service Package (MISP), as a priority intervention aimed at addressing unmet contraceptive needs and reducing maternal and child morbidity and mortality during humanitarian crises.1,2 Despite this global recognition, the availability, acceptability and uptake of FP services remain inadequate in many humanitarian settings, particularly among young women, whose specific needs are often overlooked in aggregated data or sidelined in programmatic planning.3–7
The Rohingya, a stateless ethnic minority from Myanmar, has faced decades of systemic persecution, leading to one of the largest refugee crises in recent history. Since the outbreak of violence and genocide in Myanmar in 2017, more than 1 million Rohingya have sought refuge in neighbouring Bangladesh, primarily in Cox’s Bazar district, which is now home to the world’s largest refugee camp.8,9 While the Bangladesh government classifies them as ‘forcibly displaced Myanmar nationals (FDMNs)’, this population faces substantial health challenges, exacerbated by limited autonomy and entrenched patriarchal norms significantly impacting women and young girls, particularly regarding reproductive health and decision-making.10–12
FP services within Cox’s Bazar refugee camps, coordinated by the SRH Working Group led by UNFPA and supported by various international Non-Government Organisations (NGOs), offer a range of contraceptive methods, including injectables, oral contraceptives and condoms. 13 However, use remains low, due to irregular outreach, strong cultural resistance and pervasive male dominance in reproductive decisions.10,11,14,15 Systematic reviews focused on humanitarian settings consistently report low contraceptive use despite moderate awareness, emphasising sociocultural factors and male influence as primary barriers to FP utilisation among refugee populations, including the Rohingya.7,10 Previous studies reported that contraceptive use among Rohingya women of reproductive age 18–49 in Cox’s Bazar varies from approximately 34% to 51%, which is still lower than the national levels among Bangladeshi women.7,10
More than 30% of the Rohingya population are adolescents and youth, indicating a large cohort transitioning to adulthood in such a resource-constrained setting, and in 2024, 22% experienced difficulties accessing healthcare.16,17 Young Rohingya refugee women aged 15–24 are particularly vulnerable to poor reproductive outcomes due to early marriage, high fertility rates, insufficient spacing of pregnancies and gendered power imbalances that restrict their decision-making autonomy. 12 Only 29% of those aged 11–18 were enrolled, and girls are less likely to be enrolled after age 10 compared with boys, which limits their access to health information and life skills. 16 They also belong to the generation of women who have been growing up and coming of age in refugee camps (since their arrival in 2017); therefore, they fully rely on access to SRH education and FP services provided in this setting. 12 Indeed, SRH services in the camps may be their only source of reliable FP information. However, existing research has overwhelmingly treated Rohingya women as a monolithic reproductive-age group (15–49 years),14,15,18 overlooking the age-specific barriers and FP needs of younger women. 7 The only study that has thus far described young women had enrolled adolescents aged 10–19 years with experience of early marriage, 19 limiting our understanding of the specific FP needs and barriers faced by young women aged 15–24 years.
To date, no study has specifically examined FP among married Rohingya women aged 15–24 years using a representative, probability-based design, nor has prior work adequately analysed gender-power dynamics and exposure to services as potential determinants of contraceptive use in this age group. Therefore, this study seeks to examine the FP awareness and use of contraception among young married Rohingya refugee women aged 15–24 years residing in refugee camps in Cox’s Bazar, Bangladesh. Specifically, we aimed to assess their FP awareness and current contraceptive use, compare knowledge and use among women who wish to avoid further childbearing, and identify determinants of current use aligned with the socio-ecological framework.
Methods
Study design
This cross-sectional quantitative survey was conducted in the refugee camps of Cox’s Bazar in Bangladesh between March and April 2023. The study focused on assessing SRH issues, including FP. We adhered to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist for cross-sectional studies (Supplementary Table 1). 20 The study employed a representative multistage random sampling design.
Population and setting
We used the UN definition of young people and targeted young Rohingya women aged 15–24 years. 21 At the time of data collection, more than 968,981 Rohingya refugees resided in 34 refugee camps in Cox’s Bazaar and were distributed across 208 blocks, with an average of 892 households per block.9,22 Included in this study were currently married, sexually active Rohingya women aged 15–24 years residing in the selected camps. Unmarried women and those outside the target age range were not eligible to participate.
Sample size and sampling technique
The minimum required sample size for this cross-sectional survey (n = 384) was calculated using Fisher’s formula 23 based on the following assumptions: an estimated 50% prevalence of key SRH indicators (current contraceptive knowledge, use and practice) derived from previous research 18 ; a standard normal deviation value corresponding to a 95% confidence level; a significance level of α = 0.05; and a margin of error of 5% (d = 0.05). To account for the multistage sampling design, a design effect of 1.3 and an anticipated 10% non-response rate were applied, resulting in a target sample size of 541 with sufficient statistical power (⩾80%) for multivariate logistic regression.
To achieve the desired sample size, we employed multistage random sampling. We randomly selected 8 camps out of 34 and intended to randomly select 68 households per each (541 households in total). Due to the lack of a complete household list or identification numbers within the camps, we took the following recruitment approach: A residence of Majhi (community leader) was identified in each camp to serve as a central point. 24 Households were randomly selected by walking away from each side of Majhi’s residence and stopping every 10 steps in front of a household tent. In each household, one young married woman was invited to participate in the survey. If there was more than one eligible young woman, the eldest woman within the specified age group (15–24) was invited. This approach has been used in prior humanitarian surveys where sampling frames are unavailable and yields approximate spatial randomisation around a known landmark. 24
Data collection and measures
Data were collected using a face-to-face, interviewer-administered survey via a structured paper-and-pencil questionnaire. The survey collected information about SRH literacy (including FP and contraception), sociodemographic characteristics, personal health and lifestyle factors, sexual partnerships, behaviour and sexual self-efficacy, awareness and use of SRH health services, contraception and condoms. It was developed based on DHS questions.25,26 We used the Adolescent Sexual and Reproductive Health Toolkit for humanitarian crisis situations as a guideline. 27 The questionnaire was pretested with 20 young married Rohingya women, and adjustments were made to ensure the questions were culturally and contextually appropriate for the refugee setting. Participants provided written informed consent; for participants under 18 years, written assent was obtained along with parental/guardian consent. For illiterate participants, the consent form was read aloud, and a thumbprint was obtained. The respondents were informed that participation was voluntary and that they had the right to refuse to answer any questions or withdraw at any time during data collection.
Upon completion of data collection, the data were promptly entered into REDCap, 28 a secure online data collection platform. A team of 10 local women, all fluent in the Rohingya language and experienced in data collection for various international organisations, were trained and served as interviewers. The data were stored in accordance with the policies of the University of Sydney, Australia.
We focused on measuring contraceptive use. Guided by the intersectional socio-ecological framework, 29 we propose that contraceptive use is shaped by three domains: (i) sociodemographic characteristics, (ii) exposure to FP information and services and (iii) household gender-power dynamics. Our outcomes of interest were ever use of contraceptive methods and current use of contraception – both measured as binary variables (yes/no). We selected three groups of independent factors. Sociodemographic characteristics were selected to allow comparison with findings from previous research in similar settings. They included age in years (categorised as 22–24 versus 18–21 and 15–17), women’s education (literate/illiterate), women’s employment status (household work/work outside the home), husband’s education (literate/illiterate), husband’s employment status (unemployed/ employed), current number of children, the expected number of children and woman having a desire for more children (have another child/no more).
Exposure to FP information was measured using a set of questions asking whether they had received any FP information from various sources, such as radio, TV, social media, newspapers, health workers, peers, religious leaders and family members (yes versus no for each) in the last 6 months. Given limited mass media access in the camps, this composite primarily captures interpersonal and community channels (e.g. health workers, family and community members, peers, religious leaders) and media channels (e.g. radio, television, newspapers, posters, mobile messages, social media).
We intended to assess whether participants had clear knowledge of FP methods and asked them to name specific brand names. It is possible that some participants who use FP methods lack detailed knowledge about FP. Knowledge about modern FP methods (‘knowledge about FP’ henceforth) was measured based on the recognition of at least one contraceptive brand name. Awareness about the existence of FP service centres in the camps (‘awareness about FP service centre’ henceforward, yes/no), receiving any fieldworker visits for FP in the last 6 months (talked/gave method/both/no) and exposure to FP information were recorded.
To assess the decision-making dynamics as to contraceptive use, we asked young married Rohingya women about who, in their relationship, had made a decision to use contraception (mainly husband, mainly women, joint decision). We also asked about the preference of expanding family (yes versus no) and asked each woman if they had ever refused having sex with their husband (yes versus no). We also compared FP knowledge and use in the overall sample with the subgroup of women who reported no desire for any more children, to identify gaps in meeting contraceptive needs.
Statistical analysis
Sample characteristics were assessed using descriptive statistics (means with standard deviations (SD) and frequencies with percentages, as appropriate). Comparisons of groups were investigated using Pearson’s χ2 test for independence or a t-test, depending on the nature of the variables; where expected cell counts were <5, Fisher’s exact test was used. A p-value of 0.05 was used as a cut-off for the determination of statistical significance.
To approximate the unmet need for contraception among married young Rohingya refugee women, we assessed the knowledge and use of modern contraception methods in the entire sample and in a subsample of women who did not want to have any more children.
To identify factors associated with the current use of contraception, we used logistic regression. Regression models were built using a forward stepwise model-building technique. The final model included the following variables: woman’s age, her husband’s education, exposure to FP, awareness about FP service centres, receiving any fieldworker visits for FP in the last 6 months, having ever refused to have sex with her husband, husband controlling the decision-making about contraceptive use and woman having no desire to have more children. Model fit was evaluated using the Hosmer-Lemeshow goodness-of-fit test and a pseudo-R² statistic. We report unadjusted and adjusted odds ratios (ORs and AORs, respectively) with the corresponding 95% confidence intervals (95% CIs). All the statistical analyses were performed using Stata (version 14.0; StataCorp, College Station, TX, USA).
Results
We enrolled 541 young married Rohingya women aged 15–24 years. Their characteristics, FP awareness and contraceptive use are presented in Table 1. The mean age of the participants was 21.4 years (SD: 2.3 years). The sample included 35 (6.5%) women aged 15–17 years, 192 (35.5%) aged 18–21 years and 314 (58%) aged 22–24 years. The mean age of their husbands was 26.1 years (SD: 4.6 years). In this sample, 541 (100%) women were married; 293 (54.2%) were illiterate; 522 (96.5%) were engaged in household work; and only 19 (3.5%) worked outside the household. Among their husbands, 264 (48.8%) were illiterate and 459 (84.8%) were engaged in income-generating activities such as day labourers.
Sociodemographic characteristics, FP awareness and contraceptive use of the sample: married Rohingya refugee women aged 15–24 years (n = 541).

FP: family planning; SD: standard deviation.
The average number of children per woman was 1.7 (SD: 1.1). The desired number of children was 3.7 (SD: 1.3), and 416 of 541 participants (76.9%) wanted to have another child, while 125 (23.1%) did not.
Table 1 also presents the knowledge and use of contraception among those who desired no more children. In the entire sample (n = 451), 458 women (84.7%) reported knowing about FP, 68 (12.6%) knew about the emergency contraception pill and 44 (8.1%) knew about the ‘lactational pill’ (progestin-only contraceptives). A quarter of the participants (n = 146, 27%) could identify specific FP brand names. A substantial proportion (n = 458, 84.7%) reported awareness of the FP service centre.
One-third of the participants (n = 180, 33.3%) reported receiving fieldworker visits to their home for FP in the last 6 months, including 29 (5.4% who received only one visit) and the remaining 140 women (25.9%) receiving multiple visits, but none of these women reported receiving visits every 2 weeks, as recommended. Participants reported that 356 (65.8%) visited health service centres for various reasons, such as FP, immunisation, antenatal care, vitamin A for children, monitoring child growth and pregnancy-related care. About 134 (24.8%) received FP-related services and counselling from the health service centre in the 3 months before the survey. Overall, 380 (70.2%) reported exposure to FP information from any source including 376 (69.5%) through interpersonal and community-based channels (e.g. health workers, religious leaders, peers, family and community members) and 4 (0.7%) via media channels (radio, TV, social media and newspapers) in the last 6 months. As to contraceptive use, 299 (55.3%) reported ever using contraceptive methods, whereas 243 (44.9%) reported current use. The ever use of condoms was relatively low (n = 34, 6.3%).
When compared to the entire sample, women who had no desire to have more children (n = 125) were more likely to be aware about FP (92.0% versus 84.7%), know a contraceptive brand name (35.2% versus 27.0%), receive any fieldworker visits at home for FP in the last 6 months (40.8% versus 33.3%) and use any contraceptive, ever (72.8% versus 55.3%) or currently (62.4% versus 44.9%). Still, 47 of 125 women (37.6%) who desired no more children were not using any contraception at the time of the survey, and condom use in this group was low at 9.6%.
Table 2 compares current contraceptive users and nonusers among Rohingya refugee women aged 15–24 years. Compared with nonusers, contraceptive users were, in general, older (66.7% versus 51.0% were aged 22–24 years, respectively; p < 0.001) and more likely to report that their husbands were literate (86.4% versus 83.6%, p = 0.004). Contraceptive users and nonusers did not differ in terms of their own education (59.7% versus 49.7%, p = 0.020), occupation (96.3% versus 96.6%, p = 0.827) or husband’s occupation (86.4% versus 83.6%, p = 0.356).
Comparison between the sociodemographic and other characteristics of contraceptive users and nonusers: married Rohingya refugee women aged 15–24 years (n = 541).

p-Values are from Pearson’s χ² unless indicated. FP: family planning.
Fisher’s exact test used due to sparse cells (Fisher-Freeman-Halton for r × c).
Contraceptive users were more likely to report exposure to FP information (81.9% versus 60.7%, p < 0.001), knowing a contraceptive brand name (59.3% versus 0.7%, p < 0.001), being aware about the FP service centre (93.4% versus 78.2%, p < 0.001), having received any fieldworker visits at home for FP (44.4% versus 24.2%, p < 0.001), reporting that they had ever refused having sex with their husband (57.2% versus 32.2%, p < 0.001) and reporting that their husband controlled decision-making about FP (62.6% versus 78.9%, p < 0.001). Among women who did not desire additional children, contraceptive use was higher than in those who wanted more children (67.9% versus 84.2%, p < 0.001). Where expected cell counts were <5, Fisher’s exact test was applied.
Table 3 presents the results of the unadjusted and adjusted analyses of the associations between selected independent variables and the use of contraceptives. In the multivariate logistic regression model, women were more likely to use contraceptives if they were aged 22–24 years (AOR = 1.76; 95% CI: 1.19–2.61) than the younger women (aged 15–21 years). Women whose husbands were literate were approximately 1.5 times more likely to use contraceptives than those whose husbands were illiterate (AOR = 1.47; 95% CI: 1.00–2.17).
Factors associated with the use of contraception among Rohingya refugee women aged 15–24 years (n = 541).
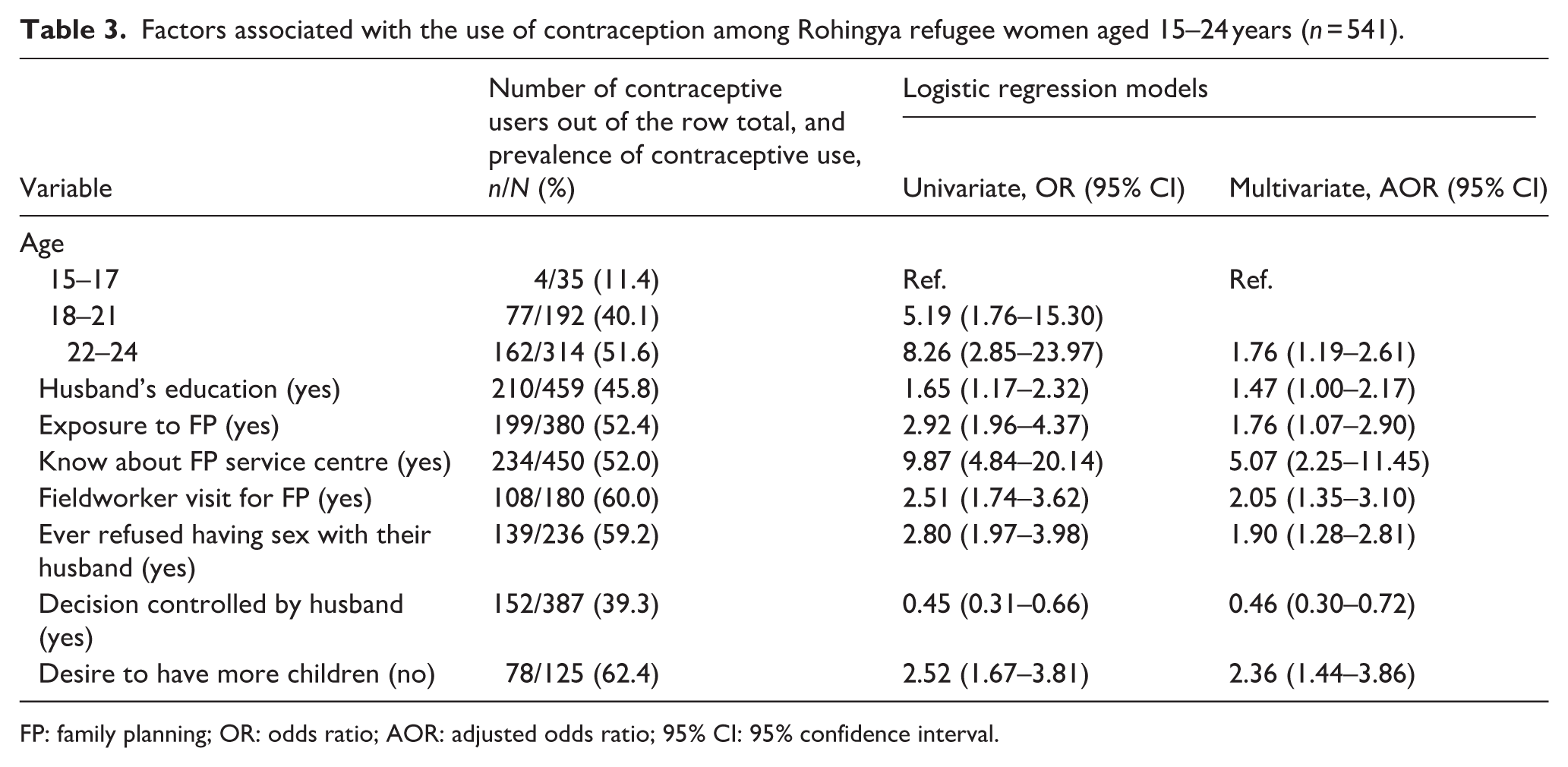
FP: family planning; OR: odds ratio; AOR: adjusted odds ratio; 95% CI: 95% confidence interval.
Higher likelihood of contraceptive use was associated with exposure to FP information (AOR = 1.76; 95% CI: 1.07–2.90), awareness about the FP service centre (AOR = 5.07; 95% CI: 2.25–11.45), having fieldworker visits at home for FP (AOR = 2.05; 95% CI: 1.35–3.10), having ever refused having sex with their husband (AOR = 1.90; 95% CI: 1.28–2.81) and having a desire to have no more children (AOR = 2.36; 95% CI: 1.44–3.86). The only factor associated with lower likelihood of women reporting contraceptive use was their husband’s control over decision-making regarding FP (AOR = 0.46; 95% CI: 0.30–0.72).
We conducted a sensitivity analysis that combined ages 15–17 and 18–21 into a single category (15–21 years). The direction and statistical significance of the age effect were unchanged, with older age associated with higher odds of current use. The final multivariate model showed good fit (Hosmer-Lemeshow test: χ2(8) = 11.96, p = 0.153), and its explanatory power was moderate for contraceptive use (McFadden R2 = 0.184; Cox-Snell R2 = 0.224; Nagelkerke R2 = 0.299).
Discussion
This study revealed several key findings regarding the FP awareness and use of contraception among young married Rohingya women residing in refugee camps in Bangladesh. First, awareness of FP methods was moderate. A significant proportion of women have been exposed to FP information, yet detailed and comprehensive knowledge of contraceptive methods remains limited. Second, the observed prevalence of contraceptive use was low on the backdrop of women’s desire for a larger family size. Third, the decision-making process regarding contraceptive use has remained primarily patriarchal, with a significant majority reporting that the decision was made by their husbands. Fourth, a significant proportion of women who had unmet need for FP were not using any contraceptive methods. Finally, factors associated with the higher likelihood of contraceptive use included older age, husband’s education, exposure to FP information, awareness of the FP service centre, fieldworker visits at home, having ever refused to have sex with their husband and having desire to have no more children, while the husband’s control of decision-making about FP was associated with lower likelihood of contraceptive use.
Awareness of FP methods among young married Rohingya women in refugee camps in Bangladesh is moderate. A significant proportion reported knowing about FP in general (84.7%), which is somewhat higher than that reported in previous studies in similar settings. Zakaria et al. reported that 58.3% were well informed about the benefits of contraception. 14 This suggests that efforts to disseminate FP information within the camps have reached a considerable proportion of the population. However, this general awareness does not extend to detailed and comprehensive knowledge about modern contraceptive methods, which remains notably low, as a large proportion of women (73%) could not name specific contraceptive brands or methods they were using. Only 1 in 10 women had heard about the emergency contraception pill, and even fewer knew about progestin-only contraception, probably because these methods had not been promoted in the camps. These findings align with the FP communication setting, mainly involving face-to-face counselling and fieldworker messaging, where awareness of contraceptive brand names might be limited despite frequent use of depo injections. The gap in detailed knowledge about contraceptive methods limits the ability of young women to make fully informed decisions about their reproductive health. Without a clear understanding of the different contraceptive methods, their benefits and potential side effects, women may be hesitant to adopt any method, thereby perpetuating low interest in FP and poor contraceptive use.
The use of contraception among young married Rohingya refugee women in Bangladesh is low, with less than half of married women currently using contraceptives. This prevalence is generally in agreement with previous literature on the topic. For example, the rate is slightly lower than the 50.9% reported by Khan et al. 15 but somewhat higher than the 34% reported by both Chowdhury et al. and Ainul et al. among married Rohingya women.30,31 Only a small portion of couples (6.3%) have ever used condoms as a contraceptive method. In contrast, national Bangladeshi data show higher uptake among similarly aged women, with 48% of married adolescents and up to 64% of young women using any FP method. 32 We found that about two-thirds of participants in our study planned to expand their families, and only half of the married young Rohingya women intended to use contraceptives in the future. This low rate of contraceptive use, despite moderate awareness, is understandable in the population of young women who are still building their families. However, we found that levels of current contraceptive use are also insufficient among women who have reached their desired family size and want no more children. More than a third of this group were not using any FP despite having a need for contraception. Indeed, the unmet FP need may be much higher, because contraceptive use is also recommended for healthy birth spacing, which was reportedly not used by many Rohingya refugee women. 15 Unfortunately, we did not have sufficient information to measure the use of contraception for birth spacing. This gap indicates missed opportunities for counselling, method mix optimisation and timely follow-up.
We also found that the average desired family size among young married Rohingya refugee women in Bangladesh was high at 3.7 children per woman, which is consistent with the 3.96 children per Rohingya refugee woman of reproductive age reported by Zakaria et al. 14 This desired family size is notably higher than the government-recommended limit of two children per family for local Bangladeshi women. The government of Bangladesh actively promotes this smaller family size through its FP campaigns, contributing to the decline in the population growth rate from 2.64% to 1.37%. 33 Underlying this large desired number of children is a complex interplay of several factors.
Previous studies have reported a cultural preference for larger families among Rohingya.18,30 Having many children is not only common among Rohingya refugees in Bangladesh but may also be valued within this community. In traditional societies such as the Rohingya, larger family sizes are often associated with economic security, social status and the fulfilment of cultural or religious expectations.14,18,31 The larger number of children may also be perceived as a matter of social security by Rohingya refugee families in Bangladesh. These norms and perceptions have the potential to influence reproductive behaviour, making the adoption of contraceptive methods less likely, even when these methods are available and known.
Therefore, preferences for higher number of children in Rohingya refugee families cannot be overcome by simply providing information and access to contraceptive methods. Programmes need to focus on changing norms, perceptions, and attitudes, and the best way of dealing with this is by addressing the root causes and targeting influential community members and decision-makers. That is, engaging the religious and community leaders, as well as men in general. This can best be done by generating and demonstrating evidence of a negative impact of family size and a lack of the use of contraception on community development, access to resources, and the health and well-being of children, women and all family members. By engaging religious and community leaders and promoting the health benefits of smaller families.15,31 FP programmes can gradually shift these norms while respecting community values.
Our study found that only 6.5% of young girls were married before the age of 18. Most of the young women lacked formal education and were primarily engaged in household work. Limited educational and economic opportunities for women continue exacerbating vulnerabilities related to SRH.14,18 The combination of poor education, early marriage, large family size, as well as preference for sons reported by previous authors, suggests a traditional societal structure that may limit the knowledge of and access to FP.14,19,31,34
Our study found that contraceptive use among young Rohingya refugee women was predominantly influenced by patriarchal decision-making, with a significant majority reporting that the decision to use or not use contraception was made by husbands. This highlights the deeply rooted patriarchal gender dynamics within the Rohingya community, where men often exert substantial control over reproductive decisions. Many women are conditioned to accept their husbands’ authority over reproductive decisions, reflecting broader societal norms that prioritise male authority and female subordination. 14 In such settings, women’s autonomy over their reproductive health is severely constrained, which may contribute to the low prevalence of contraceptive use despite the moderate level of awareness and access to FP information. This finding aligns with broader evidence from previous studies among Rohingya refugees and other refugees in similar settings, where patriarchal norms have been shown to impede women’s access to and use of FP services. In many cases, men’s approval or consent is required for women to access contraceptives, effectively placing the control of fertility in the hands of men.14,15,18,35 This can lead to unmet contraceptive needs, unintended pregnancies, and larger family sizes than desired by the women themselves.
Our study identified several factors, including age, husband’s education, exposure to FP information, knowledge of the FP service centre, fieldworker visits, women’s refusal to have sex with their husbands and desire to have no more children, that were significantly associated with the higher likelihood of contraceptive use among young Rohingya refugee women in Bangladesh. With increasing age, women were more likely to use contraceptives. This trend may suggest that with age, marriage and having children, women are increasingly exposed to information about FP, along with a heightened desire to space or limit pregnancies as they are nearing their desired family size. Additionally, the education level of husbands appeared to be an important factor, with higher educational attainment among husbands associated with greater contraceptive use reported by their wives. Among Rohingya, reproductive health decisions are heavily influenced by male partners, and men typically hold substantial decision-making power regarding FP. Our finding as to FP decision-making highlights the need for targeted FP education and the engagement of men in reproductive health dialogues, including training for male and female Rohingya volunteers to work closely with health services.
Exposure to FP information was positively associated with contraceptive use, as was knowledge of FP service centres. Women exposed to FP information were significantly more likely to use contraception. This highlights the important role of FP education in influencing contraceptive behaviours. Women who were aware about an FP service centre in the camp were nearly five times more likely to use contraceptives. Our results clearly show that access to knowledge is strongly associated with contraceptive use, which is in agreement with evidence from previous research on refugee populations. 14
Fieldworker visits were also strongly associated with higher likelihood of contraceptive use. Women who received fieldworker visits were more likely to use contraceptives than those who did not have such visits. It is noteworthy that in our study, none of these women reported receiving fortnightly fieldworker visits in the last 6 months as recommended. 15 Mass media channels have limited reach and are often not accessible in the camps; therefore, exposure to FP information likely reflects the FP education provided by community-based sources, especially community health workers, particularly during their home visits. Findings indicate that only one quarter of the participants receive FP counselling and services from the health care service centre. Our findings also highlight the importance of exposure to FP information and services and suggest that expanding outreach services and ensuring regular fieldworker visits could improve contraceptive use. This underscores the importance of direct community-based interventions, where health workers engage women in their homes, providing FP information and addressing misconceptions. Regular fieldworker visits could be an effective strategy to increase contraceptive use, particularly in conservative communities like the Rohingya, where women may have limited mobility and access to health services.
The ability of women to refuse having sex with their husbands was also associated with higher contraceptive use. This suggests that women with greater autonomy within their marital relationships are more empowered to make informed decisions about their reproductive health. Enhancing women’s agency and decision-making power within their marital relationships could be critical in improving SRH outcomes. The dominance of male decision-making in contraceptive use underscores the need for FP interventions that engage both men and women. Promoting spousal communication and shared decision-making could help shift these entrenched power dynamics, allowing women more say as to their reproductive choices. Educational initiatives targeting men, along with efforts to empower women through increased access to education and economic opportunities, are crucial for fostering a more gender-equitable approach to FP.14,19
This study contributes to the literature on SRH among young Rohingya refugees by highlighting the interplay of sociocultural norms, gender dynamics and access to information on FP practices. To improve contraceptive use, a multifaceted approach is needed, one that includes enhancing access to accurate FP information, improving male engagement and empowering young women through education and community-based programmes. This approach should also include providing comprehensive, evidence-based education and counselling to ensure informed contraceptive choices.14,36 Culturally sensitive outreach efforts that improve access to condoms and promote their use as part of a comprehensive FP programme are essential for addressing SRH needs.31,37 Such strategies are already used by local and international organisations working in refugee camps in Bangladesh and providing SRH services, which tirelessly work to improve the SRH of refugees. However, better coordinated, supported and resourced, they could further significantly improve SRH outcomes for Rohingya refugee women in Bangladesh.
Examples from other refugee settings highlight the success of multifaceted approaches in improving contraception use. In Jordan, programmes for Syrian refugees combined education on contraceptive options, community health worker outreach, and gender-based violence support, leading to increased contraceptive use and awareness.38,39 Similarly, in Uganda, engaging South Sudanese male community leaders and offering youth-friendly services enhanced contraceptive use among young women.40,41 In the Democratic Republic of Congo, integrating FP services with maternal health programmes and community outreach significantly increased contraceptive use among displaced populations.40,42 These examples highlight that a comprehensive approach addressing both supply-side (service delivery) and demand-side (community engagement and education) barriers can be effective and can improve SRH outcomes among Rohingya refugees in Bangladesh.
Limitations
The strength of our study lies in the direct collection of first-hand data from young Rohingya refugee women, providing their perspective on FP practices. The data were gathered voluntarily using their native language within familiar camp settings, fostering candid responses and enhancing reliability. Unlike previous studies that relied on convenience sampling, our study is the first in Cox-Bazaar to employ random sampling across multiple camps, ensuring a broad cross-section of the Rohingya population and increasing the generalisability of our findings. Our sample of 541 participants provided sufficient power for multivariate analyses of factors associated with contraceptive use. However, our study has several limitations. This was a cross-sectional survey; our findings establish associations but cannot infer causal relationships. This study did not collect data related to certain potentially important confounding factors, such as the perspectives of husbands and other influential family and community members, previous contraceptive use by women and use of contraception for birth spacing. All the information was self-reported in the context of an interviewer-administered survey, so there may be a potential for socially desirable answers, as well as reporting and recall bias. The interviewer-administered survey approach was necessary because most Rohingya refugee women are illiterate or have low literacy and could not complete the questionnaire on their own. However, the interviewers avoided probing and validation to minimise information bias. They also conducted interviews in the Rohingya language and were well trained to deliver the interviews to minimise any potential misreporting and bias. Despite these constraints, our research yields valuable insights into the SRH of young Rohingya refugee women in Bangladesh and adds to the already available evidence about the SRH of Rohingya refugees by focusing on young women and their needs.
Conclusion
The SRH of refugee populations, particularly those residing in low-income countries, remains a critical area of concern within the global public health landscape. Our findings reveal that while general awareness of FP is relatively high, detailed and actionable knowledge about modern contraceptive methods remains limited, and overall contraceptive use is insufficient to meet the needs of young women, especially those wishing to limit or space births. Persistent patriarchal decision-making and gender norms continue to constrain women’s reproductive autonomy, resulting in substantial unmet need and suboptimal SRH outcomes.
Our findings underscore critical policy implications aligned with international humanitarian FP guidelines, particularly the MISP. Enhancing FP awareness and detailed contraceptive knowledge among young refugee women is essential, necessitating intensified community-based outreach and educational initiatives. Furthermore, addressing gender dynamics through engaging husbands and community leaders in FP education is crucial to shifting patriarchal norms and fostering women’s reproductive autonomy. Therefore, targeted humanitarian interventions that include youth-friendly FP services, culturally sensitive education campaigns and robust community outreach are urgently needed. These strategies are not only applicable to the Rohingya context but also provide valuable insights for addressing FP needs in similar humanitarian crises globally.
Future research should explore the effectiveness of these interventions and identify additional strategies to enhance the SRH of young Rohingya women. Humanitarian FP programmes should prioritise comprehensive, age-specific and gender-sensitive approaches to effectively meet the reproductive health needs of young refugee women, thus fulfilling international commitments to reproductive health rights and ensuring equitable access to FP in crisis-affected populations.
Supplemental Material
sj-pdf-1-whe-10.1177_17455057261416251 – Supplemental material for Family planning awareness and contraceptive use among young Rohingya refugee women: A representative cross-sectional study in Cox’s Bazaar, Bangladesh
Supplemental material, sj-pdf-1-whe-10.1177_17455057261416251 for Family planning awareness and contraceptive use among young Rohingya refugee women: A representative cross-sectional study in Cox’s Bazaar, Bangladesh by Muhammad Anwar Hossain and Iryna Zablotska-Manos in Women's Health
Footnotes
Acknowledgements
We acknowledge the support of the Postgraduate Program in Sexual and Reproductive Health, Westmead Clinical School, Faculty of Medicine and Health, The University of Sydney, Australia, Office of the Refugee Relief & Repatriation Commissioner, Cox’s Bazar, Bangladesh, and the Department of Sociology, Begum Rokeya University, Rangpur, Bangladesh.
Ethical considerations
The study received ethics approval from the National Research Ethics Committee under the Bangladesh Medical Research Council (registration number 52324012023). Permission to conduct the research in the Rohingya refugee camps was also obtained from the local authorities, including the Office of the Refugee Relief and Repatriation Commissioner (RRRC), Bangladesh. All procedures adhered to the Declaration of Helsinki and WHO ethical guidelines for research with displaced populations.
Consent to participate
All participants provided written informed consent. For participants aged 15–17, written assent was obtained alongside parental/guardian consent, emphasising voluntary participation and withdrawal rights. For illiterate participants, the consent form was read aloud, and a thumbprint was obtained.
Consent procedures explicitly covered: (1) study objectives, (2) anonymisation measures, (3) voluntary participation and the right to decline to answer questions or withdraw at any time without consequences and (4) data storage protocols. We put strong measures in place to protect privacy and confidentiality. All interviews were conducted in a private setting within the camps, such as quiet tented areas or offices, where conversations could not be overheard. Participants received no monetary compensation or gifts; Participation was entirely voluntary. Personal identifiers were removed from all datasets. All identifying information was anonymised, and unique IDs were assigned (e.g. ID001). All consent forms, data and study-related materials were stored securely and accessed only by authorised members of the research team.
Consent for publication
Not applicable.
Author contributions
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Data availability statement
The data that support the findings of this study are available on request from the corresponding author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.