
Abstract
Introduction:
Unsafe abortion is a significant cause of maternal morbidity and mortality in low- and middle-income countries. Female sex workers in Ethiopia are exposed to unwanted and unplanned pregnancy and subsequent abortion. In the absence of access to quality abortion care services, the chances of experiencing unsafe abortion are high. However, limited evidence is available on female sex workers’ experience with abortion services and their exposure to unsafe abortion.
Objective:
To explore the lived experiences of female sex workers who underwent unsafe abortion in Gedeo Zone, Southern Ethiopia.
Methods:
The study was conducted among female sex workers in Gedeo Zone, Southern Ethiopia, from April to June 2024. The study was employed among female sex workers who had a history of unsafe abortion in the past 2 years. Both establishment-based and street-based female sex workers were selected using the snowball sampling method. Face-to-face in-depth interviews were conducted with participants in locations of their preference to ensure privacy. Data saturation was achieved after interviewing 18 participants. The collected data were transcribed verbatim, translated into English, and analyzed thematically using the Open Code 4.03 software. Trustworthiness was ensured throughout the data analysis process.
Design:
A qualitative study with a phenomenological design was employed.
Results:
The findings of this study revealed that poor knowledge of safe abortion services and poor socioeconomic status are the main causes for seeking unsafe abortion services by commercial sex workers. Unsafe pregnancy terminations were mainly experienced using commercial medications from private pharmacies and using traditional practices through herbal and mechanical techniques. Sex workers resorted to traditional methods and self-induced medication abortions, leading to adverse health, psychosocial, and economic consequences.
Conclusion:
The study highlights the poor information literacy and limited access to abortion services for sex workers, leading to unsafe practices and subsequent physical and psychological suffering. Therefore, stakeholders should collaborate to increase female sex workers’ knowledge and access to safe abortion services.
Background
Globally, about 73 million abortions are performed each year, of which 45% are considered unsafe abortions.1,2 In developing countries, unsafe abortion contributes to 13% of maternal deaths. In Africa, more than 75% of abortions are considered unsafe.3–6 Globally, the prevalence of unintended pregnancy among female sex workers (FSWs) is high, which is around 37%.7,8 The term FSW refers specifically to women who engage in sexual services in exchange for money. Too frequent sexual contact, inconsistent contraceptive use, alcohol use, sexual intercourse in cities far from home, and sexual violence are supposed to cause unintended pregnancies among FSWs.8,9 Evidence indicates that unintended pregnancies among commercial sex workers result in decreases in their sexual customers, financial problems, and social and psychological crises; therefore, most pregnancies among FSWs have the potential to be terminated with induced abortions. 10
Abortion services are classified as safe and unsafe based on the level of safety. Safe abortions (with a trained provider using WHO recommended methods appropriate to pregnancy gestation), less safe abortions (trained provider not using recommended methods, or safe method used without the support of, or information from, a trained provider), and least safe abortions (untrained person using invasive and dangerous methods). The unsafe section includes both the less safe and least safe abortions.3,6,11
Studies showed that the rate of abortions is much higher among FSWs worldwide. A study conducted in China, Russia, and Iran reported that 50% of FSWs experienced induced abortion in their lifetime.8,12 Reports from Kenya revealed that 90% of commercial sex workers had at least one history of induced abortion. 8 There is also evidence showing that young FSWs aged 15–24 are more likely to have unsafe abortions. 13 In many countries where there are multicultural societies, sex workers use different methods to induce abortions at their homes. For example, they drink acoustic chemicals, use herbal medicines, and insert rubbers into their vaginas to induce abortions. Others also use illegal misoprostol to induce abortions at their homes. 14 These women who undergo unsafe abortions experience life-threatening conditions. Most girls experience life-threatening acute and chronic health problems that lead to death. Women fail to disclose whether they had an abortion because they might be considered naughty and criminals. 15
In countries with restrictive abortion laws and policies, including the criminalization of abortion, FSWs prefer to obtain unsafe abortion services. 16 Though unsafe abortion and its complications are preventable, the risk of morbidity and mortality continues to the present day.9,17 In different societies, FSWs are considered a threat to religious and cultural norms, which could result in difficulty in accessing healthcare services. For such reasons, FSWs’ desire to receive sexual and reproductive health (SRH) services from the public institutions is reduced. 18
Accessing safe abortion care for all women, adolescents, and high-risk marginalized women is also a humanitarian concern. Nowadays, abortion care is one of the key indicators of SRH services, and WHO has included comprehensive abortion care in the list of essential health services. The Ethiopian Ministry of Health allows safe abortion care in all healthcare units, but the proportion of women getting safe abortions is declining by 16% in the post-COVID-19 era.5,11
Assessing the practice of unsafe abortions and subsequent challenges would be significant in improving the uptake of safe abortion services among sex workers. Besides the availability of safe abortion services, Ethiopia maintains a semi-liberal abortion law, which was articulated in 2005 to permit termination under specific circumstances. According to Article 551 of the Penal Code of the Federal Democratic Republic of Ethiopia, abortion is legally permissible in cases where pregnancy results from rape or incest; when continuation poses a threat to the mother’s life; if the fetus is diagnosed with an incurable and severe anomaly; or when the pregnant woman, due to significant physical or mental disability, or because of her minority status, is deemed incapable of raising a child. Despite their vulnerability to reproductive health problems, there is no special consideration for FSWs in the Ethiopian abortion laws. 19 The experience of FSWs in connection with unsafe abortion was not well addressed. Therefore, this study aimed to explore the lived experience of unsafe abortion among commercial sex workers in the study setting.
Methods and materials
Study setting and design
The study was conducted in the Gedeo Zone, which is one of the administrative zones in Southern Ethiopia with an estimated total population of more than 820,000. Dilla is the capital city of the Gedeo Zone, located 364 km from Addis Ababa. Gedeo Zone is one of the cash crop areas in Southern Ethiopia where the Ethio-Kenyan long roads pass through. Gedeo Zone is one of the densely populated zones in Southern Ethiopia, known for its coffee product, which accounts for 28% of the total Ethiopian coffee output. 20 More than 1344 FSWs are estimated to be located in Gedeo Zones, with their work being based in streets, homes, hotels, bars, nightclubs, and Khat houses. In the Gedeo Zone, there are 38 health centers and four hospitals that can provide SRH services. A qualitative study with a phenomenological study design was implemented from April to June 2024. The basic rationale to use phenomenology is that FSWs are one of the marginalized population groups that carry untold SRH problems; therefore, phenomenology explores and reveals the experience lived by the study participants. The experience of unsafe abortion is the event (phenomenon) that FSWs have gone through.
Population, inclusion, and exclusion criteria
Participants were selected among all FSWs in the Gedeo Zone, Southern Ethiopia. Street-based and establishment-based (nightclub, shisha house, and hotel based) FSWs who had at least one history of unsafe abortion in the past 2 years were included in the study. FSWs aged 18 years and above were included in the study, as this is the minimum legal age for providing informed consent under Ethiopian law. FSWs who had an apparent mental or physical illness that restricted participants from having interviews were excluded from the study.
Participant selection and sampling techniques
FSWs engaged in commercial sex on streets, in bars/nightclubs, and in hookah houses (shisha bet) within the Gedeo Zone Administration were selected using the snowball sampling method. Participants with a history of unsafe abortion were specifically recruited through snowball chains. Prior to data collection, information was gathered about the locations (establishment sites) where FSWs were active in the sex market. The first participant was recruited through a systematic approach and subsequently referred her peers who had history of unsafe abortion. Each newly recruited participant identified additional FSWs, continuing the snowball process. The team of researchers approached the indicated sex workers individually. The snow ball referral chain and recruitment of participants was continued until saturation achieved. A total of 18 FSWs were interviewed, of whom the five were working on street-based type sex work and the 13 were establishment-based sex workers who were working in hookah houses and bars. Before conducting interviews, participants were informed about the purpose, risks, benefits, and rights of participants. Informed consent was obtained from participants.
Data collection methods and procedure
This study was carried out in accordance with the Ethical Principles of the Declaration of Helsinki. Ethics approval was obtained from the Institutional Review Board of Dilla University College of Health Sciences (ref. no. duchm/irb/059/2023). Before conducting in-depth interviews, the participants were told about the purpose of the study, risks, and benefits of participating in the study. After all, those who are willing to participate and voluntarily sign written consent were interviewed. The study was conducted and reported in accordance with the Consolidated criteria for reporting qualitative research (COREQ) statement. 21
Data were collected using face-to-face in-depth interviews with recruited FSWs. The interview guide was used to guide the in-depth interview. The interview guide was prepared in English and translated into the Amharic language. An interview guide was prepared by a team of researchers based on the scientific merit of the qualitative study and the objective of the study. Before conducting the actual data collection, a pilot interview (pretest) was conducted to test the interview guide. Two pilot interviews with the FSWs were conducted by the researchers, during which only minor adjustments were made. After these pilot interviews, minor changes such as rearranging the order of the interview questions, clarification, and elaboration of the interview questions were made. Participants were approached individually at a preferred time and place where they ensured their privacy. All responses of respondents were recorded using an audio recorder. Data were collected until saturation was maintained. Data were collected by a team of researchers who were MSc degree holders trained on qualitative data collection methods. Both male and female data collectors were involved in the study. Trainings were given for data collectors and field assistants prior to the actual data collection. The trained data collectors made the interviews under close supervision of the facilitators/field assistants.
Data processing and analysis
The analysis of the data was started simultaneously with the data collection, and thematic analysis was used. The audio/video recordings of individual interviews were transcribed and translated verbatim from Amharic to English. The translation versions were checked for consistencies with the original language. Data analysis was supported by the Open Code 4.03 qualitative software. Translated files were exported into the open-code software, and inductive coding was applied. Initially, the researchers engaged in an in-depth reading of the scripts to develop a comprehensive understanding of the underlying ideas. Subsequently, each text was carefully examined, and codes were generated to represent specific segments of the texts and paragraphs. These codes were systematically documented in a codebook and further refined to ensure accuracy and clarity in their representation. The final, refined codes were defined and clustered to form branches (subthemes). Then, the more related subthemes were looked for broader patterns forming a theme, which finalizes the thematic structure (Table 1). Finally, the researchers wrote up the description of the results presented to the final themes.
List of themes and sub themes.

Rigor/trustworthiness
To ensure trustworthiness, the criteria of credibility, transferability, dependability, and conformability were considered in each step of data analysis. Credibility was ensured through prolonged engagement with the data and building trust with participants. Field notes were taken in each step of data collection, and peer debriefing was made to confirm valid findings that can improve quality. Transferability was ensured through thick descriptions of findings gained from respondents with sufficient details. Dependability was considered to ensure the study procedure replicated with consistent results. Careful data collection techniques were implemented, and an audit trail from the outside reviewer was considered. Confirmability was ensured by following scientific data collection, analysis, and reporting procedures to make the process free of bias. To minimize bias and subjectivity arising from the researchers’ attitudes and profiles, reflexivity was ensured through self-reflection and peer debriefing.
Results
Socio demographic characteristics of participants
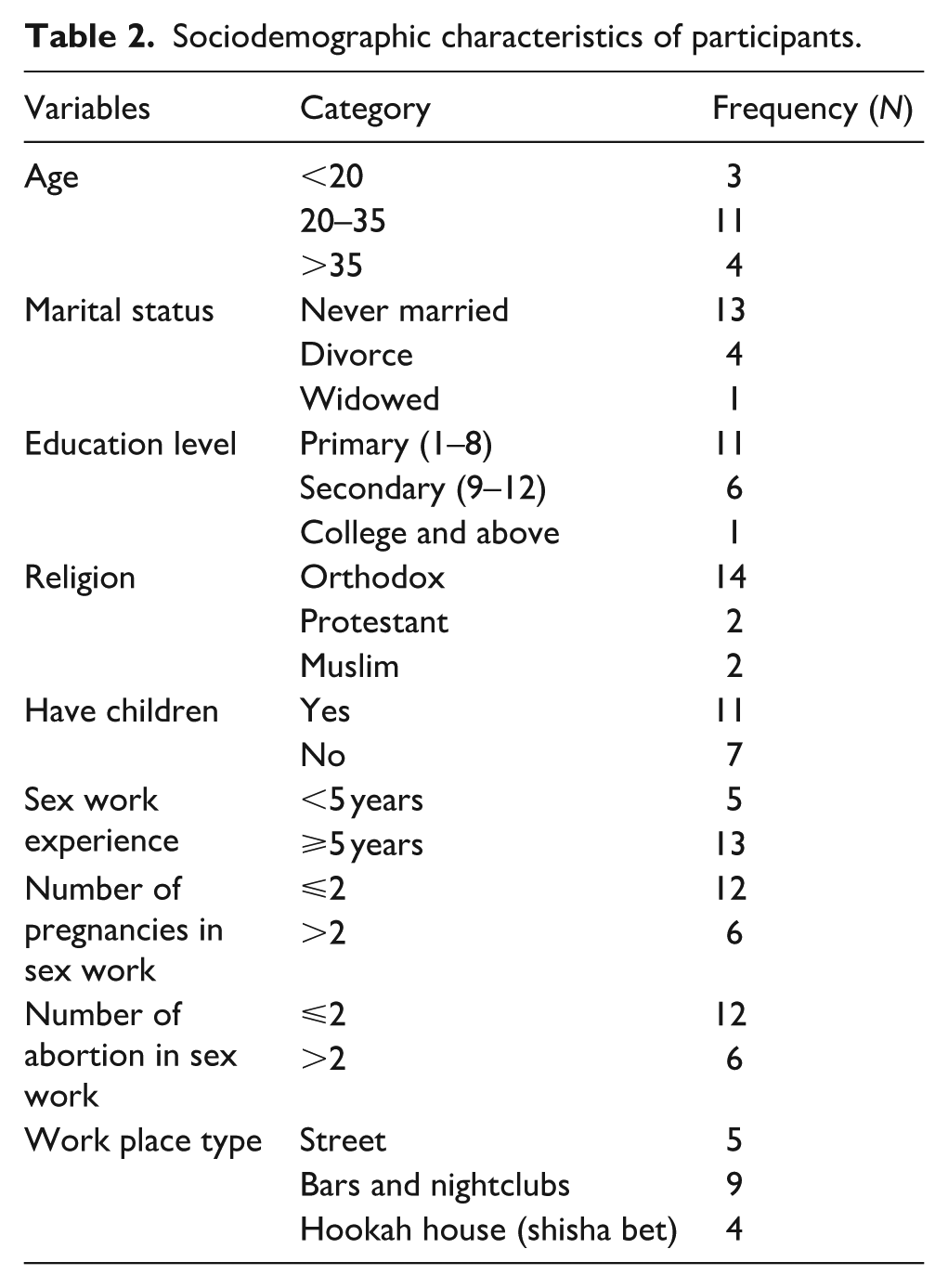
A total of 18 FSWs were interviewed. Most had not completed primary school (eighth grade or lower) and had never been married. The majority had at least one child. The age of the respondents ranged from 18 to 40 years old, and their experience in sex work ranged from 2 to 18 years (Table 2).
Sociodemographic characteristics of participants.
The final result of the thematic analysis was categorized into six themes, namely, history of female sex work engagement, pregnancy in sex work, experiences of unsafe abortion services, psychosocial influences of unsafe abortion, attitudes to unsafe abortion services, and information on abortion. The first two themes were highlighting the pre-abortion sex work experiences of the FSWs.
Theme 1: History of sex work engagement
The sex workers in this study come from different backgrounds. Engagement in sex work was associated with different reasons. Factors such as extreme poverty, lack of family support, conflict with families, domestic violence, lack of job access, and peer pressure were factors driving women into the sex industry. As reported by participants, their poor socioeconomic condition and inability to take care of children and families forced them to engage in sex work.
After my divorce from my husband, life seriously challenged me; I was not able to feed my children. I started working as a mobile maid in such a way that I wash clothes and bake Injera at their home. However, after some time, I didn’t get even this labor. To sustain the lives of my children, I decided to sacrifice myself and engage in sex work. (a 31 year FSW) I was living with my husband and had one child, but after some time he left me alone. I was working as a bed-maker in hotels and pensions. I suffer a lot from financial crises, which I discussed with my friend. My friend told me why you always complain about problems: you can get more money with your pussy. She advised me to have sex work and overcome financial problems. I agreed with her idea and engaged in sex work. (a 30-year-old Muslim FSW)
Girls who lacked family support due to death of parents in childhood faced numerous obstacles in life, which ultimately lead them to engage in sex work. They grew up in labor-intensive, unsatisfying employment, and sex work is the last occupation they have.
I had no family alive who supported me, and I was living alone. No one supported me. I tried some jobs, like tea and coffee works but it was not effective, life was not going well, so my choice was to engage in sex work. I have worked for four years as a sex worker. (a 25-year-old FSW) I have never known my mother. Along with my father, I endured a lot of hardships, including a lack of food for daily consumption. I was a student and continued until grade 5. I often skipped school classes due to hunger. When I was in sixth grade, I started working as a glass washer at a hotel. While I was working in the hotel, one of my friends advised me to join the sex market. She told me that sex work was productive and that I could earn more money. I was a virgin when I joined the sex market at the age of fifteen. (an 18-year-old FSW)
Participants in our study described how domestic violence has contributed to their engagement in sex work. Some participants were survivors of domestic violence by their stepfathers in their adolescent years.
Domestic violence forced me to enter into sex work. While my mother was out of the country, I lived with my stepfather for a long time. He harshly abused me a lot. He allowed me to stop school in the fifth grade. He committed sexual violence against me repeatedly. I tried to resist a lot when he was having sex with me, but he injected me with an IV drug to desensitize me. He took my virginity, and I experienced repeated sexual assaults from him. To hide his misdeeds, he told my mother that I was rude and that I was experiencing drug addictions. He misleads my mother about me, and she also detests me. I left out of their home at the age of 17 and joined the sex workers. (a 24-year-old FSW) My father died early when I was a child, and we were living with my mother and stepfather. My stepfather mistreats me a lot, in such a way that he usually hits and beates me repeatedly. In addition, my stepfather needs to have sex with me. My mother wouldn’t trust me if I told her the case, so I kept it secret. I discussed the case with my friend, who lived alone in a rented house. She advised me to leave the city and migrate to another city together. In the city to which we moved, we work as waitresses. While we were working as waitresses, we decided to engage in sexual work because the job was not as satisfactory as intended. (a 20-year-old FSW)
Theme 2: Pregnancy in sex work
Prevention of unwanted pregnancy in the sex work
Sex workers have used different techniques to prevent pregnancy as they could not have capacities to give birth and rear children. Most sex workers experienced the use of modern contraceptives, but inconsistency of the contraceptive use and dropouts were reported by many participants. Condoms were considered a definitive contraceptive option among commercial sex workers. In combination with condoms, sex workers experienced the use of pills and injectables contraceptive alternatives in the past. Many sex workers were currently using injectables, oral pills, post pills, and implants as a method of contraception. For the fear of the side effects of other modern contraceptives, some women are using condoms only for the prevention of pregnancy.
I was using a contraceptive injection, but the injection disturbed my periodic cycle. My period was delayed for a prolonged period, and I was concerned about my health status when the period was delayed, so I stopped using injectables. Currently, I am using an implant that is placed under the arm. I have used it for 6 years. (a 35-year-old FSW) I have been performing intercourse with high precautions to prevent pregnancy. I don’t perform risky sexual intercourse. I have never used modern contraceptives other than condoms because I feel they could harm my health; for example, they could cause hypertension. (a 40-year-old FSW)
Exposure to unintended pregnancy
Due to the risky nature of the sex market, many sex workers suffered from unwanted pregnancies throughout their lives. The study’s participants elucidated how various behavioral factors had exposed them to unintended pregnancies in the sex industry. Condom rupture, high-paying clients, alcohol use, unprotected sex with boyfriends and long-term clients, and aggression by sex clients are the most frequent causes of pregnancy among sex workers. Many sex workers have intimate partners whom they consider faithful boyfriends. Sex workers had unprotected sex with these intimate friends, resulting in pregnancies. Similarly, many women have long-term sexual clients whom they consider their definitive customers. These long-term sex clients seek intercourse without condoms.
I knew a sex client who talked to me and contacted me frequently. One day, he told me to chill out overnight. We relaxed, drank a lot, and had sex without a condom, resulting in my pregnancy. (a 20-year-old FSW) My first pregnancy at sex work was from my customer, who visited me frequently and gave me much more money. At that time, I was not aware of any subsequent risks; however, he continuously gave me money and had sex without a condom, resulting in a pregnancy. (a 35-year-old FSW)
Condom rupture was one of the most frequently occurring events among sex workers. Participants explained that condom rupture during intercourse exposed them to unwanted pregnancies. Although there are instances where condoms burst for unknown reasons, drunken sexual acts are typically the culprit.
I had an unintended pregnancy once before two years. The condom ruptured while I was having sex with an older man, but at that time I didn’t notice what had happened. He told me that the condom ruptured; however, I didn’t pay attention to the event. But after some point, the symptoms of pregnancy became noticeable in my body. (An 18-year-old FSW)
FSWs deal with a variety of clients who exhibit violent and abusive tendencies. The men usually force the women to have sex without condoms; however, those women who refuse the men’s request will experience harsh physical violence. As some participants described, they got pregnant after forceful sexual violence committed by their clients.
My first pregnancy resulted from having sex with an intoxicated man. We drank alcohol together, but he was more intoxicated. He wanted to have intercourse without a condom, but I declined; despite this, he forcefully defeated me. At that time, I was more afraid of diseases than of pregnancy. After two months, I became amenorrhic and tested positive for pregnancy. On another occasion, I got pregnant for the second time as a result of sexual violence at work. My second pregnancy was prompted by the sexual violence I encountered in the sex industry. One day, a sex client allowed me to go to bed and forced me to have unsafe sex, which I refused. He beat me brutally when I refused to do as he wanted. He threw me out of bed. He performed terrible risky intercourse on me. Even after he had sex, he did not pay me. (a 37-year-old FSW)
Theme 3: Experience of unsafe abortion in sex work
Reason for unsafe abortion service
For variety of reasons, FSWs preferred unsafe measures to terminate pregnancies. Participants in our study reported that a lack of awareness of abortion services, a lack of money to provide safe abortion services, privacy and confidentiality concerns, and discouraging bureaucracies among government health facilities were all common factors driving sex workers to unsafe abortion care.
Using private pharmacies to get abortion medications is more confidential and keeps our privacy. Public hospitals had a long bureaucracy; they requested to come with a male partner who impregnated me which was unlikely. The nurses working in public hospitals are not as confidential as intended. (a 23-year-old FSW) I went to the clinic for abortion services, but they refused to do so. They told me that they couldn’t kill souls. I told my friend, and she advised me to take medication from a veterinarian. (a 25-year-old FSW)
In the early stages of their sex work, many women lacked sufficient knowledge and awareness about abortion services. Participants mentioned that they were primarily focused on earning money, and their decisions were not made with full awareness at the beginning of their involvement in sex work.
I had no prior knowledge or awareness since I had no prior exposure to pregnancy, so I preferred not to go to the clinics. My friend who is also a sex worker did a urine test at home to confirm my pregnancy. I discussed the cases with my friends (sex workers) and they brought me a yellow abortion medication to be drunk with Coca-Cola. (a 30-year-old FSW)
Pregnancy termination practices
Self-induced abortion experiences
Many women terminate pregnancies at home by themselves using a variety of practices. Most sex workers bought drugs from private pharmacies and apply by themselves. This study revealed that some women experienced unsafe abortions by taking any form of medication at hand. The medications could be antibiotics, antimalarial, or iron tablets; even some women took veterinary drugs like albendazole.
I took the seven non-hormonal tablets (irons) attached to a contraceptive pill. I took all seven tablets at once, along with Coca-Cola. At night, bleeding started to pass through my vagina, and I drank Coca-Cola. I suffered the expulsion of a blood clot for 7 consecutive days. (a 28-year-old FSW) My friend advised me to take medication from veterinary pharmacies to have an abortion since she has used it before. I paid 50 birr to a veterinary pharmacy and bought green tablets (Albendazole) that are used to treat sheep and goats. I dilute two tablets with water, drink, and sleep. After 20 minutes, it began to burn my heart and my entire body. After twenty minutes of sleep, I went to the restroom, but the abortus had been completely removed. (a 25-year-old FSW)
FSWs have reported purchasing abortion-inducing medications, such as misoprostol, from private pharmacies. Even though the medication was authorized, they did not seek early medical help for post-abortion complications, leading to significant challenges following these induced abortions.
I went to the private clinic and consulted a professional about abortion. I paid 450 birr and received an abortion-inducing medication from the private clinic. I took one tablet orally, and after 30 minutes of feeling lower abdominal pain, I placed a half tablet into my vagina. After taking the medication vaginally, I had abdominal pain. I inserted another dose through my vagina after one hour of abdominal pain. The pain persisted for long hours, and I started sweating all day and night. The next morning, about 6 a.m., the watery fluid drained away, and bleeding began. It was a 4-month conception, the bleeding persisted; I was collapsed and unable to control myself. (a 28-year-old FSW) I went to a private clinic for a pregnancy test, and I told the care provider that I had to terminate my pregnancy because I didn’t want that pregnancy. He directly prescribed the drug and allowed me to buy it from the pharmacy. I paid 950 birr, and the dispenser instructed me to take one tablet orally soon and to insert the remainder vaginally after the third day. Immediately, I took the first tab orally, and abdominal pain started. Then I inserted the tablet through my vagina, and I felt low back pain with a pushing-down sensation. After some time, it bleeds and expels. After the abortion, I suffered from heavy bleeding and dizziness, which was unpleasant. (a 25-year-old FSW)
Some FSWs induced abortions by themselves at their home by taking home prepared local mixtures. They prepared mixtures to be drunk that allow the conception to be destabilized and ending in abortion.
When I was with my family, I heard that “Mustard” can cause abortion. I smashed and powdered the mustard seed, then diluted it with water. I drank a glass of mustard solution. After I drank, lower abdomen pain and vaginal bleeding began. Because the abortion occurred in the first few weeks of pregnancy, there was not much bleeding. (a 40-year-old FSW)
Abortion induced with assistance
There were a group of women who sought assistance to terminate pregnancies; mainly they visited traditional abortion services providers. Sex workers used leaf-extracted herbal drugs ordered by the traditional providers or assisted with mechanical termination techniques.
I went to the residence of the traditional abortion service provider woman with my friend. The woman massaged my abdomen and gave me a plant leaf to drink. She gave me a KOSSO (Hagenia abyssinica) plant leaf to squeeze and ordered me to drink the liquid extraction from the squeezed leaf. My friend extracted the leaf and gave me a cup of drugs to drink. I drank the extracted liquid drug with an empty gastric at 6:00 am. In the afternoon, I felt abdominal pain and I became sweaty and lethargic. The pain and bleeding persisted for 3 days resulting in loss of energy. (An 18-year-old FSW)
Beyond giving herbal medicines, traditional abortion service providers apply mechanical inductions to make abortions for sex workers. As the participant explained, the traditional woman inserted tubes through the vagina and allow destabilizing the entire conception.
I dealt with my friend and she told me to go to the traditional abortion provider woman. I went to the home of a traditional woman for an abortion service and she inserted a tube through my vagina to the length of the uterus. Once the tube reached my uterus she disturbed the entire uterus with the glucose tube. It was painful, it started to bleed and she told me it could be completely expelled at home and returned to my home. Initially, the bleeding was minimal but continued to bleed for one week. It is completed at the end of the week. She didn’t give any other drug other than mechanically disturbing the entire conception. I paid 800 birr for the service. (a 26-year-old FSW)
Complications experienced with unsafe abortion
Sex workers have experienced various complications associated with unsafe abortions. Unsafe abortion has challenged sex workers with acute and long-term health consequences. Most sexual workers have had life-threatening encounters with unsafe abortions. According to this study, FSWs who lived with unsafe abortions frequently suffered severe pain, heavy bleeding, and prolonged bleeding, which resulted in severe deterioration and collapse. Some participants reported that they were critically ill and reached the door of death. On the contrary, some participants faced only minimal complications.
Bleeding started after four hours of taking the tablet. The heavy bleeding continued to flow, which was not stoppable. It flows overnight and continues for up to 15 days. After 15 days, I lost my energy, became lethargic, and could not take food, so my friends took me to the clinic. I felt tenderness in my uterus and was unable to lean forward or lean down. I was dying, but God healed me. I recovered after I visited the clinic. (a 30-year-old FSW) After we inserted the medication vaginally, the discharge passed out on the second day. I bleed a lot. It was very painful and I hated myself. It pierced my womb. I was not standing alone and my friends were ambulating me for the bathroom. I suffered a lot for 15 days. (an 18-year-old FSW)
Sex workers who experienced unsafe abortions suffered from acute and chronic gynecologic problems. Many women complain of chronic pelvic pain, painful intercourse, and genitourinary infections. Sex workers believe that these problems were not present before their unsafe abortions.
I have developed chronic pelvic pain after having that abortion. Still, now, I feel pain in my uterus during sex. I feel low back pain while washing clothes. (a 28-year-old FSW) The abortion has caused me recurrent genital infection which is manifested by urinary urgency and pain during intercourse. This infection was not present before the abortion. I use treatments for recurrent infections. (a 30-year-old FSW)
In this study, some women believed that the drugs they used to induce abortions had caused chronic medical problems. Chronic gastritis, anemia, and chronic heart problems were among the medical problems reported by sex workers associated with abortion drugs.
I have been suffering from a heart problem, which I believe is related to the abortion. I visited the clinic for it and asked the physicians whether it could be associated with abortion drugs. He also informed me that the abortion medicine could rarely cause heart failure. (a 24-year-old FSW) The mustard is powerful; it affects the gastric and it is prohibited for pregnant women. The drug has damaged my gastric wall and; I have been suffering from gastritis since my abortion. (a 40-year-old FSW)
Theme 4: Psychosocial influences of unsafe abortion
Sex workers who had abortion histories experienced a wide range of psychological, social, and economic burdens. Participants explained that they were emotional victims of their abortion stories. Many women considered themselves criminals and sinful. Following their abortions, women experienced isolation and insults from their partners. Additionally, sex workers experienced financial hardship during the times when they stopped working because of their abortions.
I am not morally free in my abortion; I feel as if the fetus’ soul is accusing me. I am still concerned about that practice. I regret not giving birth; I sinned. (a 25-year-old FSW) When I think about it, my emotions are unsteady. Seeing the house where I slept during an abortion brings back the pain. My friend, who urged me to have an abortion, attacked me after we disagreed. She considered me hopeless because I had a black history. (an 18-year-old FSW)
In contrast, there were participants who did not experience any significant health or psychosocial influence in relation with their abortion.
Except for the financial cost, there was no long term health or social impact on me as a result of the unsafe abortion. (a 25-year-old FSW)
Theme 5: Attitudes to unsafe abortion services and future preferences
Attitudes to unsafe abortion services
Participants were asked about their attitudes toward unsafe abortion practices and their upcoming choices. Most participants were not comfortable with the past practices. Many participants have a negative attitude toward unsafe abortions and regret their past actions. Sex workers explained that they would not repeat that practice again. They stated that unsafe abortion was risky and lethal.
I have bad attitude for abortion. It has no comfort, I regret. I feel anxious of that woman; what a cruel woman she was aborting me with that technique. I recommend others to go clinics and have to take safety measures. (a 26-year-old FSW) I regret for my past action. I will go to clinic if it happens in the future, I don’t prefer the traditional one. My friends use misoprostol which is relatively safe. Some women drink herbal drug privately and dies. If someone consulted me I will support her to have medical abortion. (a 30-year-old FSW)
Future service preferences
Many FSWs who encountered harsh experiences associated with unsafe abortion were promised not to consider the unsafe practices as their service of choice. They prefer to visit the modern clinics to have safe abortion care.
I recall what I went through during my previous abortion, which brought me back from the dead. If comparable incidents occur again, I will visit the clinic and receive modern care. (a 36-year-old FSW)
In contrast, there are women who prefer such unsafe practices to terminate pregnancies for the sake of their privacy and confidentiality concerns. These participants reported that medication abortion from commercial pharmacies is preferable even in their future events.
Relatively, having an abortion at a private pharmacy is more comfortable than having it at a public hospital. I felt comfortable having an abortion. I don’t know whether it will happen next or not. If I become pregnant in the future, I will have no other alternative except to have an abortion. For abortion, I will prefer the method I used before, which was taking medications from private pharmacies. (a 25-year-old FSW) I will do the same fashion as the previous if it happens next. Using private pharmacies to get abortion medications is more confidential and keeps privacy. (a 23-year-old FSW)
Theme 6: Information on abortion in sex work
Participants were asked about their exposure to information about abortion services. Most responded that they had no access to information on abortion services. Participants also revealed that there was no access to safe abortion services in the governmental health institutions. Most FSWs share information from peer experiences. Those FSWs who receive any form of abortion service were the ultimate source of information. Most respondents explained that no organizational body came to us to discuss abortion. A few participants mentioned that organizations and professionals occasionally provided health education on sexually transmitted infections and contraceptive methods, but not on abortion services.
Nobody tells us organized information about abortion services; however, sex workers with abortion histories are the ultimate information sources. (a 25-year-old FSW) There are some health professionals who provide information at our work place like in shisha house by considering themselves as customers to communicate information. They didn’t tell as there were health professionals but they negotiate talks about reproductive issues and share information in between. (a 26-year-old FSW)
Discussion
This study explores the experience of FSWs who encountered unsafe abortion along with pre-abortion sex work experiences. The findings of this study entail that FSWs suffer from unwanted pregnancies resulting from inconsistent contraceptive use, violent sexual practices, and unprotected sex for extra money benefits. Unsafe pregnancy termination was experienced by many FSWs due to poor information literacy, partially liberal abortion laws, and privacy concerns. FSWs who underwent unsafe abortions suffered from medical, socioeconomic, and psychological problems.
In this study, women mentioned different reasons to engage in commercial sex work. Economic need and financial sufferings, followed by the inability to feed children and cover school fees, forced many participants to engage in sex work. Findings from previous studies also revealed that highly impoverished women engage in commercial sex work to fulfill their basic needs.22,23 Women who were raised in unstable family environments and experienced the loss of parents during their childhood often ended up turning to sex work. Participants in this study stated that lack of support from parents and families forced them to engage in sex selling. As supported by previous studies conducted abroad, children who have lost their parents and family tend to experience labor-intensive, unsatisfying jobs, and may eventually turn to sex work.24,25 Some participants in this study explained that repeated domestic violence by their families pushed them to migrate to sex work. Some girls who grew up with stepfathers were victims of harsh treatment and sexual violence. These repeated violence attempts forced girls to prefer to leave home and join the sex industry. A previous study also supported the evidence of childhood neglect and abuse as drivers into sex work. 26
FSWs have employed various contraceptive methods to avoid pregnancy, as they may not have the means to bear and raise children. The findings of this study indicated that condoms were the predominant form of protection used by many FSWs; however, a significant number of FSWs reported inconsistent condom use. This inconsistency in condom use could be attributed to the awareness levels of FSWs, their sexual debut, alcohol consumption, and the diversity of their clients.27–29 Some women were using condoms as the only method of pregnancy prevention due to the fear of side effects of other contraceptives. While many sex female workers have tried modern contraceptives such as implants, pills, and injectables, a significant number reported inconsistencies in use and instances of discontinuation. The reasons for skipping contraceptive use varied, including alcohol intoxication affecting their ability to remember to take pills, inconvenience in accessing healthcare services in their area of residence, and discontinuation due to experiencing side effects.30–33
Many participants in the study mentioned that condom rupture during intercourse was a common cause of their pregnancies. Women in the sex work industry frequently encounter both intentional and unintentional condom ruptures and slippages, leading to unintended pregnancies. The instances of slippages and condom rupture were attributed to engaging in intercourse under the influence of alcohol, improper condom use, or forceful thrusting during sexual activity. Additionally, there are instances of male clients intentionally breaking condoms during intercourse to prioritize their own satisfaction, disregarding the risks associated with unsafe sex.34,35 All these implies, due to the risky nature of the sex market, many sex workers suffered from unwanted pregnancies throughout their lives. Inconsistent and inappropriate contraceptive uses, along with various behavioral factors, are contributing to the risk of unintended pregnancies among FSWs.
The participants in the study expressed that their sex clients had a significant influence on their exposure to unintended pregnancy. FSWs often experienced unintended pregnancies from their regular clients, who sometimes acted as intimate boyfriends. These male clients would negotiate unprotected sexual intercourse with the FSWs, leading to pregnancies. On days when sex workers met with their regular clients, they frequently skipped using contraception.30,36 According to this study, FSWs became pregnant as a result of having intercourse with high-paying clients who sought out unprotected sex and gave them additional cash. FSW frequently negotiated for good relations with sex clients that provided extra money. Similar to this study, a previous study carried out in Tanzania revealed that FSWs waived condom use to gain higher payment, which could result in pregnancy.33,37 FSWs deal with a variety of clients who exhibit violent and aggressive tendencies. Some participants described becoming pregnant as a result of sexual violence inflicted by aggressive sex clients. Some sex clients initially negotiate peacefully with women and proceed to bed, but then forcefully prohibit the use of condoms. As a result of sexual violence by sex clients, FSWs became pregnant. This suggests that women did not consider using alternative modern contraceptives in situations where condom use was not possible.38–40 Stakeholders should take initiatives to increase awareness toward modern contraceptive use among high-risk populations. FSW-focused information and behavioral change communications strategies for SRH services need to be strengthened to reduce the burden of unintended pregnancy.
Many pregnancies that happened to sex workers ended with abortions. FSWs tend to seek various abortion services to terminate their pregnancies. This study found that many sex workers opt for unsafe abortion services due to a variety of reasons. Women who are new to sex work often lack knowledge about where to access safe abortion services and instead rely on the experiences and recommendations of their peers.41,42 Women aimed to keep their abortions private and undisclosed, so they avoided public health facilities and opted for unsafe private procedures or self-induction. Women expressed concerns that seeking care at public health facilities could compromise their privacy and confidentiality due to a lack of trust in health professionals.43,44 FSWs stated that the bureaucratic processes at public health institutions deter them from seeking care. Participants expressed that the legal requirements for abortion services at government institutions are lengthy and off-putting. Additionally, the sex workers noted that health providers did not treat them nicely, particularly when they knew they were sex workers. A previous study carried out among Indian FSWs reported the stigmatizing behavior of healthcare providers when sought for abortion services, resulting in the loss of intention to access medical abortion services and ending up with using home abortion remedies. 45 Consistent with this study, a previous finding from northern Ethiopia revealed the uncooperative characteristics of the abortion care providers. 46 These findings would have implications for the national policies and abortion laws, including abortion service providers’ legal duties in providing safe abortion services. The Ethiopian abortion laws are semi-liberal in such a way that legal abortion would be permitted if there was rape or incest, severe congenital anomalies, severe maternal medical and mental deterioration from giving birth, or maternal life-threatening pregnancies. 19 As the legal abortion laws would have an impact on harmonizing the service needs of the FSWs, the need to expand awareness of abortion service availability and legality was revealed in prior research.43,47
In this study, sex workers used various methods to end their pregnancies. The majority obtained commercial abortion drugs from private pharmacies and performed self-induction. Many sex workers are familiar with commercial misoprostol and often purchase it. However, the practices employed by sex workers to terminate their pregnancies were found to be unsafe. Some women used abortion medications with inappropriate solvents, employed improper vaginal insertions, or failed to promptly respond to the raised complications.48–50 Although there is an emerging liberalization of self-management of medical abortion, there is no adequate evidence on how much women are effectively experiencing it.51,52
FSWs who lacked the financial means to access modern health care often opted for self-induced abortions using local herbal products at home or sought assistance from traditional abortion care providers. These traditional providers would either administer herbal drugs or conduct invasive mechanical procedures to terminate the pregnancy. Some traditional healers would insert plastic tubes and wires through the vagina to disrupt the conception, leading to severe pain and life-threatening bleeding for the women involved.14,43,49,50 There were also FSWs who took any medication at hand to terminate pregnancies. These included women ingesting high-dose pills, antibiotics, antimalarial, iron tablets, and even veterinary medications to terminate their pregnancies.53,54 Although there has been a shift from traditional abortion methods to medication-based abortion, there are women who continue to resort to unsafe and illegal practices to terminate pregnancies. Therefore, policy goals and interventions should prioritize improving the uptake of safe abortion services, particularly among marginalized populations.
FSWs who had unsafe abortions suffer from acute and long-term complications. Some participants explained that they were severely collapsed and were near death. Mild to life-threatening pain, heavy bleeding, infection, collapse, and hospitalization were acute complications experienced after the unsafe abortion. Some FSWs explained that they live with chronic gynecologic and medical problems associated with their history of unsafe abortion.48,50 All these imply that unsafe practices and poor responses to post-abortion complications caused sex workers to experience life-threatening morbidities. FSWs with a history of abortion faced significant psychological, social, and economic challenges. FSWs who undergo abortion face financial difficulties as they are unable to work for days or even months. Participants reported emotional suffering as well as feelings of guilt and regret. These emotions were linked to the violation of religious norms and a sense of committing a sin against God. Additionally, FSWs whose abortion stories were revealed faced a significant level of stigma. House renters and friends mocked and gossiped about them for their abortions, which could lead to social isolation. These findings are confirming a previous study carried out in Ethiopia that has revealed the community-level stigma occurred among women who underwent induced abortions. It is also indicated that community interventions would improve abortion knowledge and decreased abortion stigma.46,55,56
Many participants have a negative attitude toward unsafe abortions and regret their past actions. Those who experienced life-threatening complications were promised not to repeat the unsafe alternatives. They stated that self-induction of abortion was risky and lethal.50,57 In contrast, there are women who are comfortable with self-induced abortions for the sake of their privacy and confidentiality concerns. These participants reported that medication abortion from commercial pharmacies will also be their future preference. 55 These findings would imply the preferences of medication abortion along with service centers. To bring about meaningful changes at both national and regional levels, it is essential to identify the centers most frequently utilized by FSWs for abortion services and to strengthen the quality of care in these facilities, ensuring that services are relatively safe, easily accessible, and provided in a manner that upholds women’s comfort and dignity.
Poor information access to sexual and reproductive services was also reported by FSWs. Most sex workers share information from friends and peer experiences. Those sex workers who receive any form of abortion service were the ultimate source of information. Lack of sufficient information about safe abortion services, including where and when to access them, has affected women’s decision making.41,49 These findings would have revealed the gap in reproductive healthcare information provision for all social classes; in particular, the national care provision and information dissemination could not address the marginalized and hidden populations such as FSWs. This study supports a previous study conducted on eight countries also revealed the need for comprehensive reproductive health services for vulnerable population. 18
Strength and limitations
This phenomenological qualitative study pioneers the study setting by exploring the experiences of FSWs, who are poorly addressed marginalized populations. Since this is a qualitative study, there might be generalizability doubts due to the small sample size and non-randomized samples. There might be recall bias, as many sex workers frequently use alcohol, and due to the sensitive nature of sex work, social desirability bias could be present.
Conclusion
The study highlighted that many sex workers were experiencing unsafe abortion practices due to poor information literacy and limited access to safe abortion services, leading to severe medical, psychosocial, and economic consequences. Therefore, enhancing women’s awareness and health literacy would significantly reduce morbidity, mortality, and the psychosocial burden of unsafe abortion among sex workers. In addition, scaling up comprehensive health education and behavior change communication, along with advocating for policy measures that expand access to safe and affordable reproductive health services are critical to preventing unsafe abortion practices among FSWs and safeguarding their overall well-being.
Footnotes
Acknowledgements
Our deepest gratitude goes to the Guttmacher institute in collaboration with St. Paul Institute for Reproductive Health and Rights (SPIRHR) for providing the financial support to conduct this research. Next, great thank goes to Dilla University for acknowledging this task and provide ethics approval for the study. Lastly, we would like to acknowledge the data collectors, supervisors, and study participants for their support in conducting this study.
Ethical considerations
This study was carried out in accordance with Ethical Principles of Declaration of Helsinki. Ethics approval was obtained from the Institutional Review Board of Dilla University College of Health Sciences (ref. no. duchm/irb/059/2023; protocol unique no. duirb/059/18-12).
Consent to participate
The participants were informed about the purpose of the study, risks, and benefits of participating in the study. After all, those who were willing to participate and voluntarily sign the written consent were interviewed informed written consent was obtained from each participants. The privacy and confidentiality of participants was assured. The data obtained from respondents were kept safe and used for this study purpose only.
Consent for publication
Not applicable.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by St. Paul Institute for Reproductive Health and Rights in collaboration with Guttmacher Institute.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data pertinent to the findings of this study are available from the corresponding author upon reasonable request.